
Maternal SARS-CoV-2 Infection at Delivery Increases IL-6 Concentration in Umbilical Cord Blood
 ,
,  , ,
, , 
Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
4.1. Maternal IL-6 Levels in Women Infected with SARS-CoV-2
4.2. Amniotic Fluid and Umbilical Cord IL-6 Levels in Women Infected with SARS-CoV-2
4.3. Relation between Maternal Blood, Umbilical Cord Blood, and Amniotic Fluid IL-6 Levels
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar]
- Galang, R.R.; Newton, S.M.; Woodworth, K.R.; Griffin, I.; Oduyebo, T.; Sancken, C.L.; Olsen, O.O.; Aveni, K.; Wingate, H.; Shephard, H.; et al. Risk Factors for Illness Severity Among Pregnant Women with Confirmed Severe Acute Respiratory Syndrome Coronavirus 2 Infection-Surveillance for Emerging Threats to Mothers and Babies Network, 22 State, Local, and Territorial Health Departments, 29 March 2020–5 March 2021. Clin. Infect. Dis. 2021, 73, S17–S23. [Google Scholar]
- Jamieson, D.J.; Rasmussen, S.A. An update on COVID-19 and pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.Q.; Bilodeau-Bertrand, M.; Liu, S.; Auger, N. The impact of COVID-19 on pregnancy outcomes: A systematic review and meta-analysis. CMAJ 2021, 193, E540–E548. [Google Scholar] [CrossRef]
- Balachandren, N.; Davies, M.C.; Hall, J.A.; Stephenson, J.M.; David, A.L.; Barrett, G.; O’Neill, H.C.; Ploubidis, G.B.; Yasmin, E.; Mavrelos, D. SARS-CoV-2 infection in the first trimester and the risk of early miscarriage: A UK population-based prospective cohort study of 3041 pregnancies conceived during the pandemic. Hum. Reprod. 2022, 37, 1126–1133. [Google Scholar] [CrossRef]
- Saito, S. Cytokine network at the feto-maternal interface. J. Reprod. Immunol. 2000, 47, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Tosun, M.; Celik, H.; Avci, B.; Yavuz, E.; Alper, T.; Malatyalioǧlu, E. Maternal and umbilical serum levels of interleukin-6, interleukin-8, and tumor necrosis factor-alpha in normal pregnancies and in pregnancies complicated by preeclampsia. J. Matern. Fetal Neonatal Med. 2010, 23, 880–886. [Google Scholar] [CrossRef] [PubMed]
- De Jongh, R.F.; Puylaert, M.; Bosmans, E.; Ombelet, W.; Maes, M.; Heylen, R. The fetomaternal dependency of cord blood interleukin-6. Am. J. Perinatol. 1999, 16, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine Storm in COVID-19: The Current Evidence and Treatment Strategies. Front. Immunol. 2020, 11, 1708. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2021, 93, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Caparros-Gonzalez, R.A.; Pérez-Morente, M.A.; Hueso-Montoro, C.; Álvarez-Serrano, M.A.; de la Torre-Luque, A. Congenital, Intrapartum and Postnatal Maternal-Fetal-Neonatal SARS-CoV-2 Infections: A Narrative Review. Nutrients 2020, 12, 3570. [Google Scholar] [CrossRef] [PubMed]
- Kyle, M.H.; Glassman, M.E.; Khan, A.; Fernández, C.R.; Hanft, E.; Emeruwa, U.N.; Scripps, T.; Walzer, L.; Liao, G.V.; Saslaw, M.; et al. A review of newborn outcomes during the COVID-19 pandemic. Semin. Perinatol. 2020, 44, 151286. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.; Li, W.; Kang, Q.; Xiong, Z.; Wang, S.; Lin, X.; Liu, Y.; Xiao, J.; Liu, H.; Deng, D.; et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: A retrospective, single-centre, descriptive study. Lancet Infect. Dis. 2020, 20, 559–564. [Google Scholar] [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef]
- Melekoglu, R.; Yilmaz, E.; Ciftci, O.; Kafadar, Y.T.; Celik, E. Associations between second-trimester amniotic fluid levels of ADAMTS4, ADAMTS5, IL-6, and TNF-α and spontaneous preterm delivery in singleton pregnancies. J. Perinat. Med. 2019, 47, 304–310. [Google Scholar] [CrossRef]
- Lu-Culligan, A.; Chavan, A.R.; Vijayakumar, P.; Irshaid, L.; Courchaine, E.M.; Milano, K.M.; Tang, Z.; Pope, S.D.; Song, E.; Vogels, C.B.F.; et al. Maternal respiratory SARS-CoV-2 infection in pregnancy is associated with a robust inflammatory response at the maternal-fetal interface. Med 2021, 2, 591–610.e10. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Wang, K.; Chen, W.; Zhang, Z.; Deng, Y.; Lian, J.Q.; Du, P.; Wei, D.; Zhang, Y.; Sun, X.-X.; Gong, L.; et al. CD147-spike protein is a novel route for SARS-CoV-2 infection to host cells. Signal Transduct. Target. Ther. 2020, 5, 283. [Google Scholar] [CrossRef]
- Wender-Ozegowska, E.; Bomba-Opoń, D.; Brazert, J.; Celewicz, Z.; Czajkowski, K.; Gutaj, P.; Malinowska-Polubiec, A.; Zawiejska, A.; Wielgoś, M. Standards of Polish Society of Gynecologists and Obstetricians in management of women with diabetes. Ginekol. Pol. 2018, 89, 341–350. [Google Scholar] [CrossRef]
- Brancaccio, M.; Mennitti, C.; Calvanese, M.; Gentile, A.; Musto, R.; Gaudiello, G.; Scamardella, G.; Terracciano, D.; Frisso, G.; Pero, R.; et al. Diagnostic and Therapeutic Potential for HNP-1, HBD-1 and HBD-4 in Pregnant Women with COVID-19. Int. J. Mol. Sci. 2022, 23, 3450. [Google Scholar] [CrossRef]
- Rubio, R.; Aguilar, R.; Bustamante, M.; Muñoz, E.; Vázquez-Santiago, M.; Santano, R.; Vidal, M.; Melero, N.R.; Parras, D.; Serra, P.; et al. Maternal and neonatal immune response to SARS-CoV-2, IgG transplacental transfer and cytokine profile. Front. Immunol. 2022, 13, 999136. [Google Scholar] [CrossRef]
- Raj, R.S.; Bonney, E.A.; Phillippe, M. Influenza, immune system, and pregnancy. Reprod. Sci. 2014, 21, 1434–1451. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Avila, C.; Santhanam, U.; Sehgal, P.B. Amniotic fluid interleukin 6 in preterm labor. Association with infection. J. Clin. Investig. 1990, 85, 1392–1400. [Google Scholar] [CrossRef]
- Santhanam, U.; Avila, C.; Romero, R.; Viguet, H.; Ida, N.; Sakurai, S.; Sehgal, P.B. Cytokines in normal and abnormal parturition: Elevated amniotic fluid interleukin-6 levels in women with premature rupture of membranes associated with intrauterine infection. Cytokine 1991, 3, 155–163. [Google Scholar] [CrossRef]
- Taglauer, E.S.; Dhole, Y.; Boateng, J.; Snyder-Cappione, J.; Parker, S.E.; Clarke, K.; Juttukonda, L.; Devera, J.; Hunnewell, J.; Barnett, E.; et al. Evaluation of maternal-infant dyad inflammatory cytokines in pregnancies affected by maternal SARS-CoV-2 infection in early and late gestation. J. Perinatol. 2022, 42, 1319–1327. [Google Scholar] [CrossRef] [PubMed]
- Bermick, J.; Watson, S.; Lueschow, S.; McElroy, S.J. The fetal response to maternal inflammation is dependent upon maternal IL-6 in a murine model. Cytokine 2023, 167, 156210. [Google Scholar] [CrossRef]
- Zaretsky, M.V.; Alexander, J.M.; Byrd, W.; Bawdon, R.E. Transfer of inflammatory cytokines across the placenta. Obstet. Gynecol. 2004, 103, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Merchant, P.; Walker, C.R.; Kryworuchko, M.; Diaz-Mitoma, F. Interleukin-6 expression in cord blood of patients with clinical chorioamnionitis. Pediatr. Res. 1996, 39, 976–979. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yockey, L.J.; Iwasaki, A. Interferons and Proinflammatory Cytokines in Pregnancy and Fetal Development. Immunity 2018, 49, 397–412. [Google Scholar] [CrossRef]
- Prins, J.R.; Gomez-Lopez, N.; Robertson, S.A. Interleukin-6 in pregnancy and gestational disorders. J. Reprod. Immunol. 2012, 95, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Küçük, M.; Sezer, S.D.; Yenisey, Ç.; Yüksel, H.; Odabaşi, A.R. Comparison of interleukin-6 levels in maternal and umbilical cord blood in early- and late-onset preeclampsia. Gynecol. Endocrinol. 2012, 28, 640–643. [Google Scholar] [CrossRef] [PubMed]
- Mirabella, F.; Desiato, G.; Mancinelli, S.; Fossati, G.; Rasile, M.; Morini, R.; Markicevic, M.; Grimm, C.; Amegandjin, C.; Termanini, A.; et al. Prenatal interleukin 6 elevation increases glutamatergic synapse density and disrupts hippocampal connectivity in offspring. Immunity 2021, 54, 2611–2631.e8. [Google Scholar] [CrossRef]
- Estes, M.L.; McAllister, A.K. Maternal immune activation: Implications for neuropsychiatric disorders. Science 2016, 353, 772–777. [Google Scholar] [CrossRef] [PubMed]
- González-Mesa, E.; García-Fuentes, E.; Carvia-Pontiasec, R.; Lavado-Fernández, A.I.; Cuenca-Marín, C.; Suárez-Arana, M.; Blasco-Alonso, M.; Benítez-Lara, B.; Mozas-Benítez, L.; González-Cazorla, A.; et al. Transmitted Fetal Immune Response in Cases of SARS-CoV-2 Infections during Pregnancy. Diagnostics 2022, 12, 245. [Google Scholar] [CrossRef] [PubMed]
- Treviño-Garza, C.; Villarreal-Martínez, L.; Estrada-Zúñiga, C.M.; Leal-Treviño, M.; Rodríguez-Balderrama, I.; Nieto-Sanjuanero, A.; Castillo, B.C.-D.; Montes-Tapia, F.F.; de la O-Cavazos, M. Leptin, IL-6 and TNF-α levels in umbilical cord blood of healthy term newborns in relation to mode of delivery. J. Obstet. Gynaecol. 2016, 36, 719–721. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SARS-CoV-2 Positive N = 48 | SARS-CoV-2 Negative N = 42 | ||
|---|---|---|---|
| Median (Interquartile Range) | Median (Interquartile Range) | p | |
| Women | |||
| Age (years) | 32 (31–37) | 33 (31–35.5) | 1 |
| BMI (kg/m2) | 27.5 (25.5–33.4) | 28 (26.4–30.3) | 0.8 |
| SARS-CoV-2 vaccination * | 25 (52.1) | 33 (78.6) | 0.02 |
| COVID-19 treated with oxygen supply * | 2 (4.2) | - | |
| COVID-19 pneumonia | 0 | - | |
| CPAP | 0 | - | |
| Mechanical ventilation | 0 | - | |
| Primiparous * | 18 (37.5) | 18 (42.9) | 0.6 |
| Chronic hypertension * | 2 (4.2) | 1 (2.4) | 0.8 |
| Gestational hypertension/preeclampsia * | 6 (12.5) | 1 (2.4) | 0.1 |
| SGA * | 5 (10.4) | 4 (9.5) | 0.9 |
| Gestational diabetes mellitus * | 3 (6.3) | 4 (9.5) | 0.8 |
| Nicotinism in pregnancy * | 3 (6.3) | 0 | 0.1 |
| Gestational age at delivery (weeks) | 38 (37–39) | 39 (38–39.25) | 0.3 |
| Preterm delivery * | 7 (14.5) | 2 (4.8) | 0.2 |
| Newborns | |||
| Birthweight (g) | 3375 (3110–3910) | 3510 (3092–3742) | 0.7 |
| Apgar < 8 * | 0 | 0 | 1 |
| NICU admission * | 6 (12.5) | 0 | 0.046 |
| CPAP * | 6 (12.5) | 0 | 0.046 |
| Mechanical ventilation * | 1 (2.1) | 0 | 0.9 |
| IVH * | 0 | 0 | 1 |
| SARS-CoV-2 Positive N = 48 | SARS-CoV-2 Negative N = 42 | |||
|---|---|---|---|---|
| Median (Interquartile Range) | Median (Interquartile Range) | p | ||
| Maternal blood | WBC (103/μL) | 9.4 (6.7–11.3) | 9.1 (8–10.6) | 0.9 |
| CRP (mg/L) | 6.9 (2.6–15.6) | 2.8 (1.5–3.9) | 0.06 | |
| PCT (ng/mL) | 0.07 (0.04–0.1) | 0.04 (0.01–0.07) | 1 | |
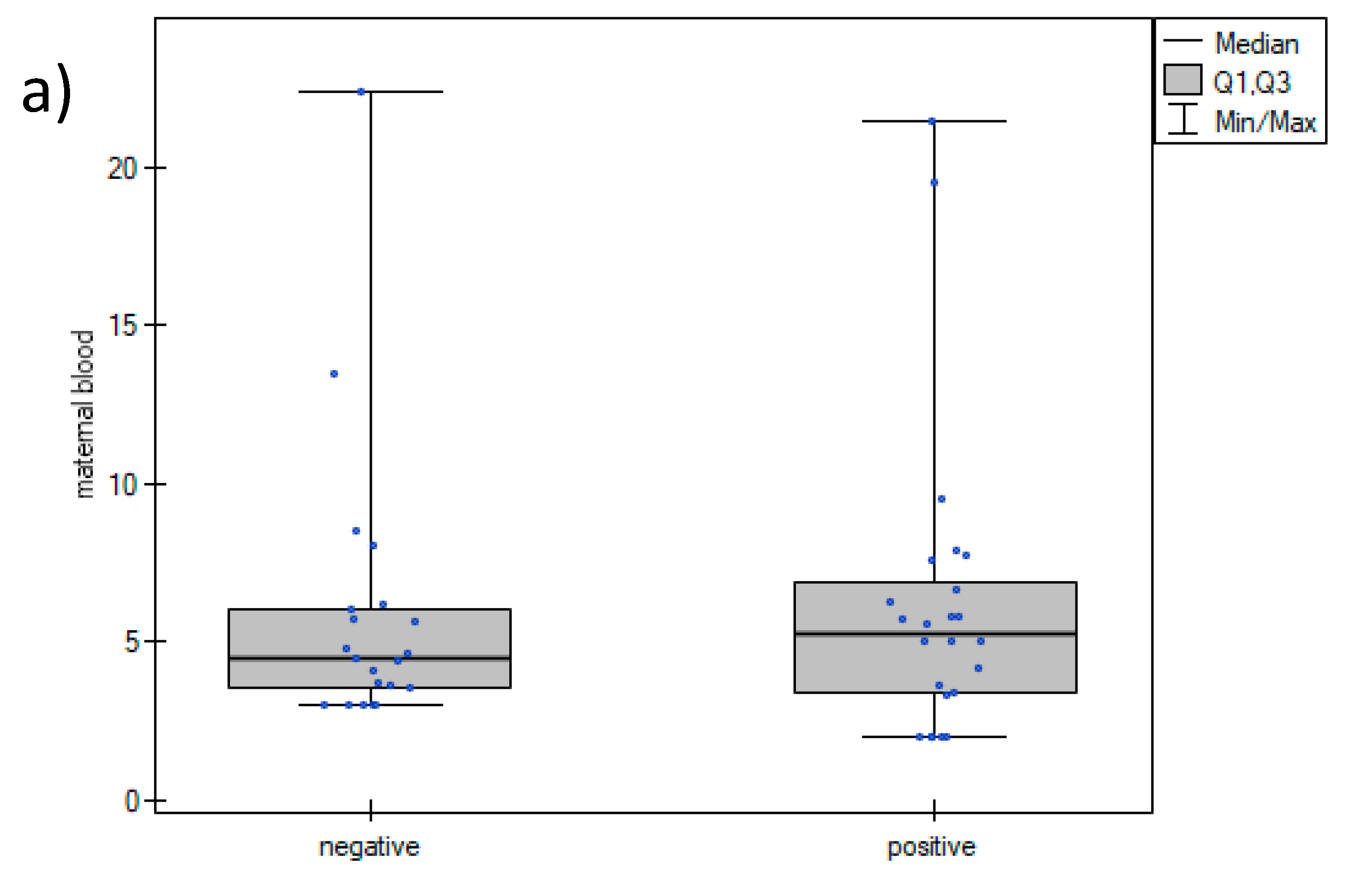
| IL-6 (pg/mL) | 5.3 (3.4–7.1) | 4.4 (3–5.9) | 0.6 | |
| Amniotic fluid | IL-6 (pg/mL) | 511 (259–880.5) | 514 (310–770.5) | 0.9 |
| Umbilical cord blood | IL-6 (pg/mL) | 6.2 (4.3–8.3) | 4.2 (2.6–4.9) | 0.02 |
| Composite Neonatal Morbidity | No Composite Neonatal Morbidity | ||
|---|---|---|---|
| IL-6 (pg/mL) | Median (Interquartile Range) | Median (Interquartile Range) | p |
| Maternal blood | 5.1 (4.14–9.64) | 4.5 (3.38–7.34) | 0.4 |
| Amniotic fluid | 294 (168–733) | 524 (323–860) | 0.4 |
| Umbilical cord blood | 7.6 (5.02–9.54) | 4.6 (3–6.22) | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosińska-Kaczyńska, K.; Rebizant, B.; Czeszko-Paprocka, H.; Bojdo, A.; Przybylski, M.; Chaberek, K.; Lewandowska, A.; Szymusik, I.; Brawura-Biskupski-Samaha, R. Maternal SARS-CoV-2 Infection at Delivery Increases IL-6 Concentration in Umbilical Cord Blood. J. Clin. Med. 2023, 12, 5672. https://doi.org/10.3390/jcm12175672
Kosińska-Kaczyńska K, Rebizant B, Czeszko-Paprocka H, Bojdo A, Przybylski M, Chaberek K, Lewandowska A, Szymusik I, Brawura-Biskupski-Samaha R. Maternal SARS-CoV-2 Infection at Delivery Increases IL-6 Concentration in Umbilical Cord Blood. Journal of Clinical Medicine. 2023; 12(17):5672. https://doi.org/10.3390/jcm12175672
Chicago/Turabian StyleKosińska-Kaczyńska, Katarzyna, Beata Rebizant, Hanna Czeszko-Paprocka, Agata Bojdo, Maciej Przybylski, Katarzyna Chaberek, Agnieszka Lewandowska, Iwona Szymusik, and Robert Brawura-Biskupski-Samaha. 2023. "Maternal SARS-CoV-2 Infection at Delivery Increases IL-6 Concentration in Umbilical Cord Blood" Journal of Clinical Medicine 12, no. 17: 5672. https://doi.org/10.3390/jcm12175672
APA StyleKosińska-Kaczyńska, K., Rebizant, B., Czeszko-Paprocka, H., Bojdo, A., Przybylski, M., Chaberek, K., Lewandowska, A., Szymusik, I., & Brawura-Biskupski-Samaha, R. (2023). Maternal SARS-CoV-2 Infection at Delivery Increases IL-6 Concentration in Umbilical Cord Blood. Journal of Clinical Medicine, 12(17), 5672. https://doi.org/10.3390/jcm12175672