
New Effective Intraoperative Techniques for the Prevention of Coronal Imbalance after Circumferential Minimally Invasive Correction Surgery for Adult Spinal Deformity
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
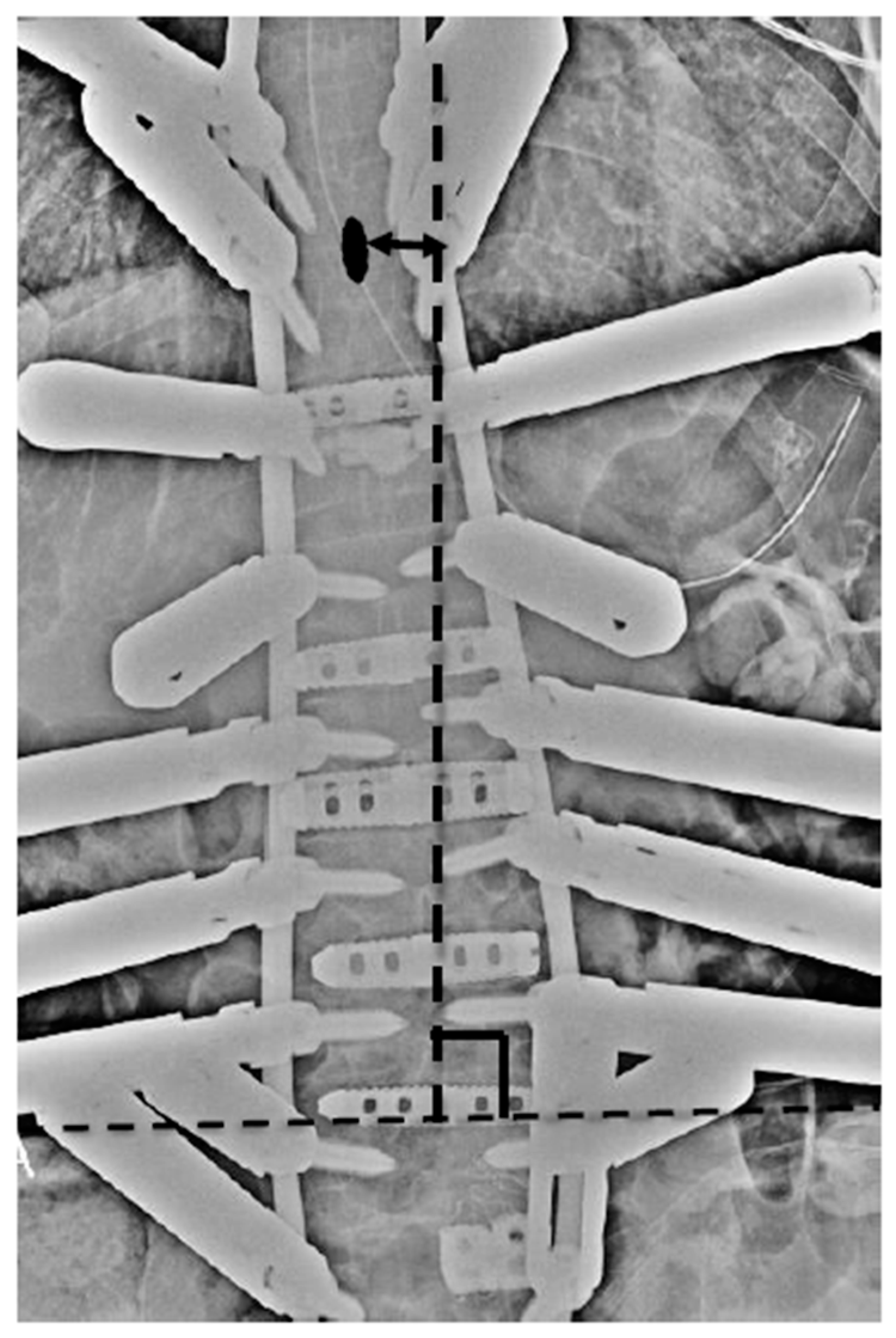
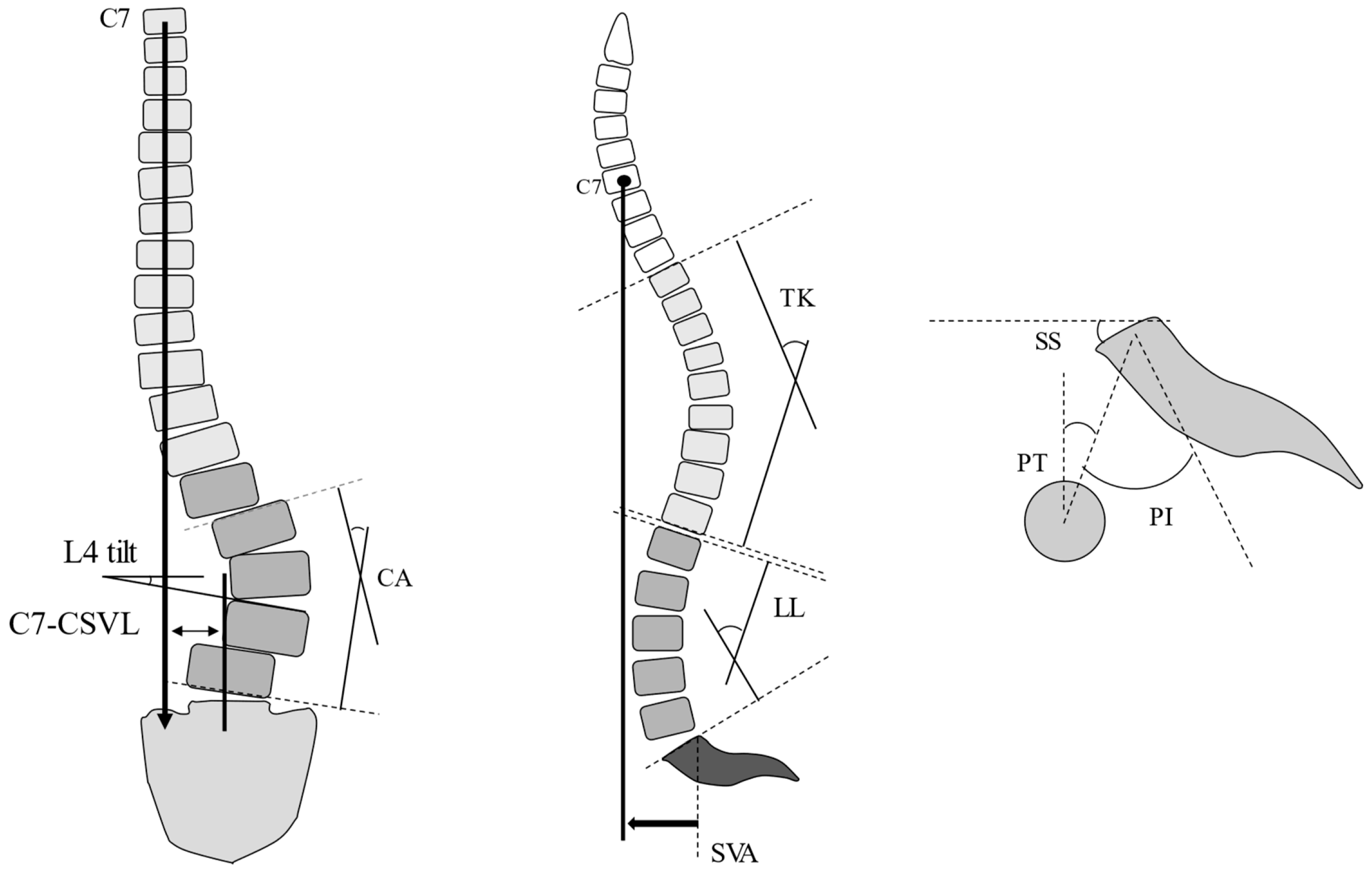
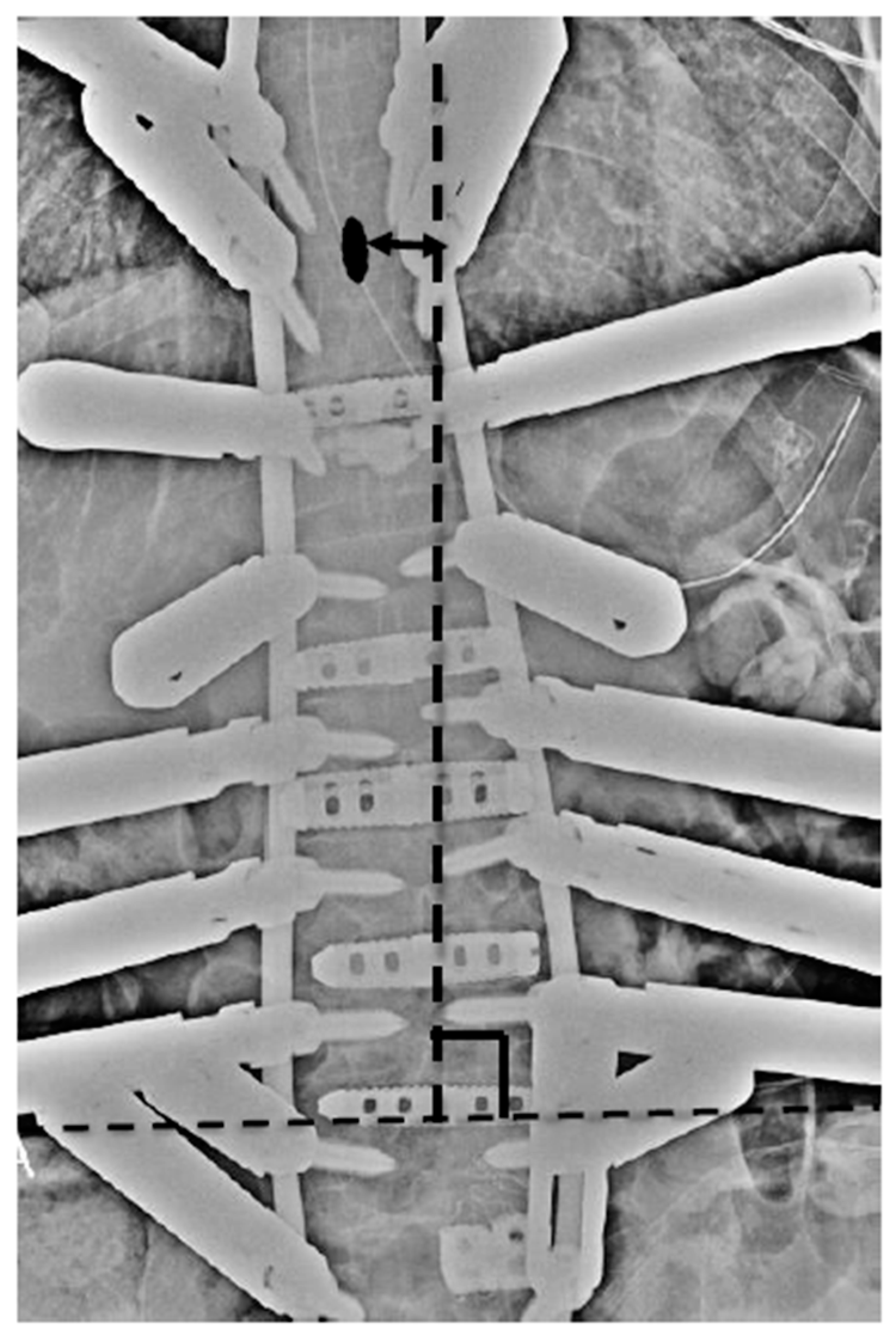
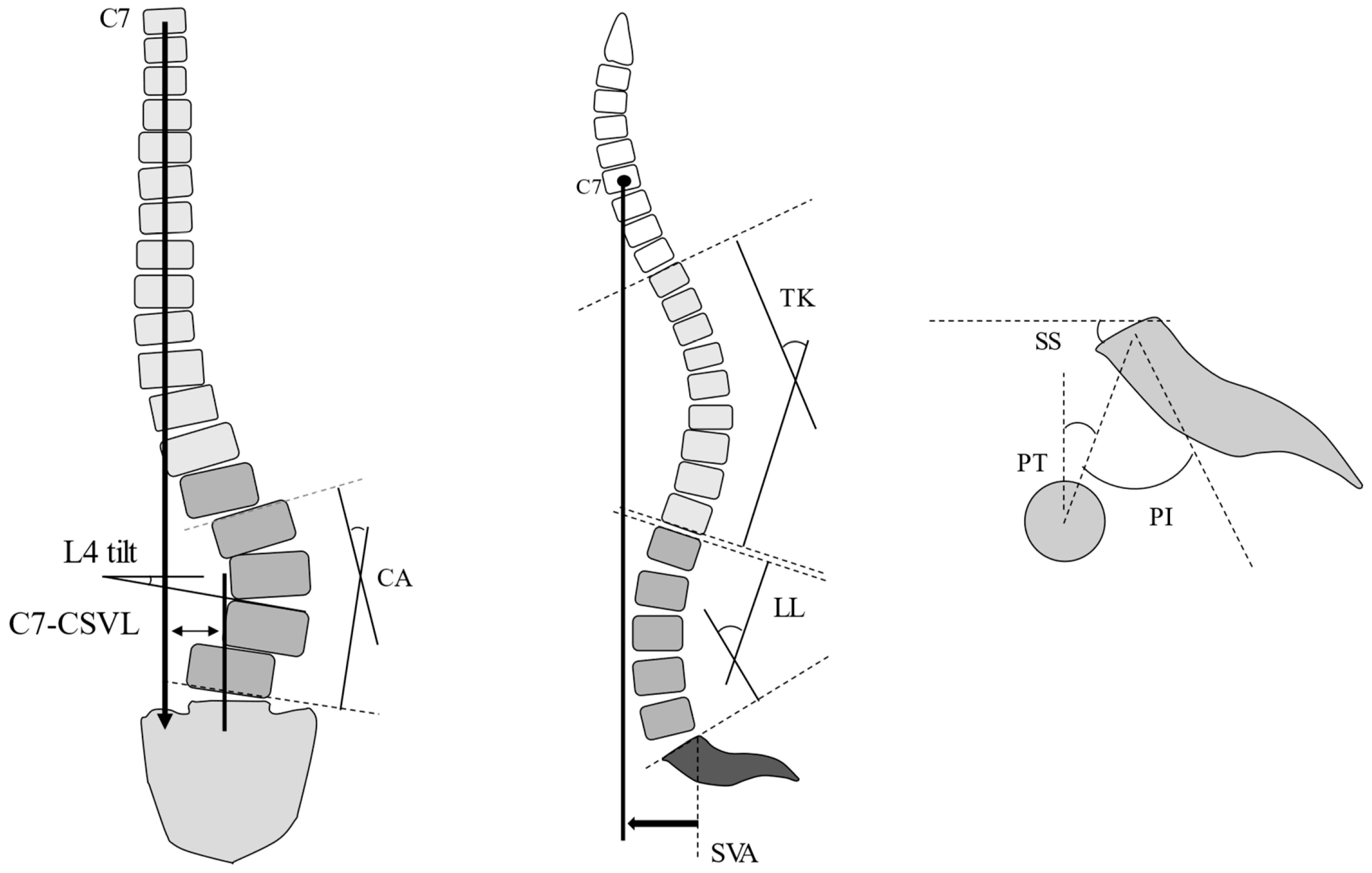
2.1. Radiological Evaluation
2.2. Statistical Analysis
3. Results
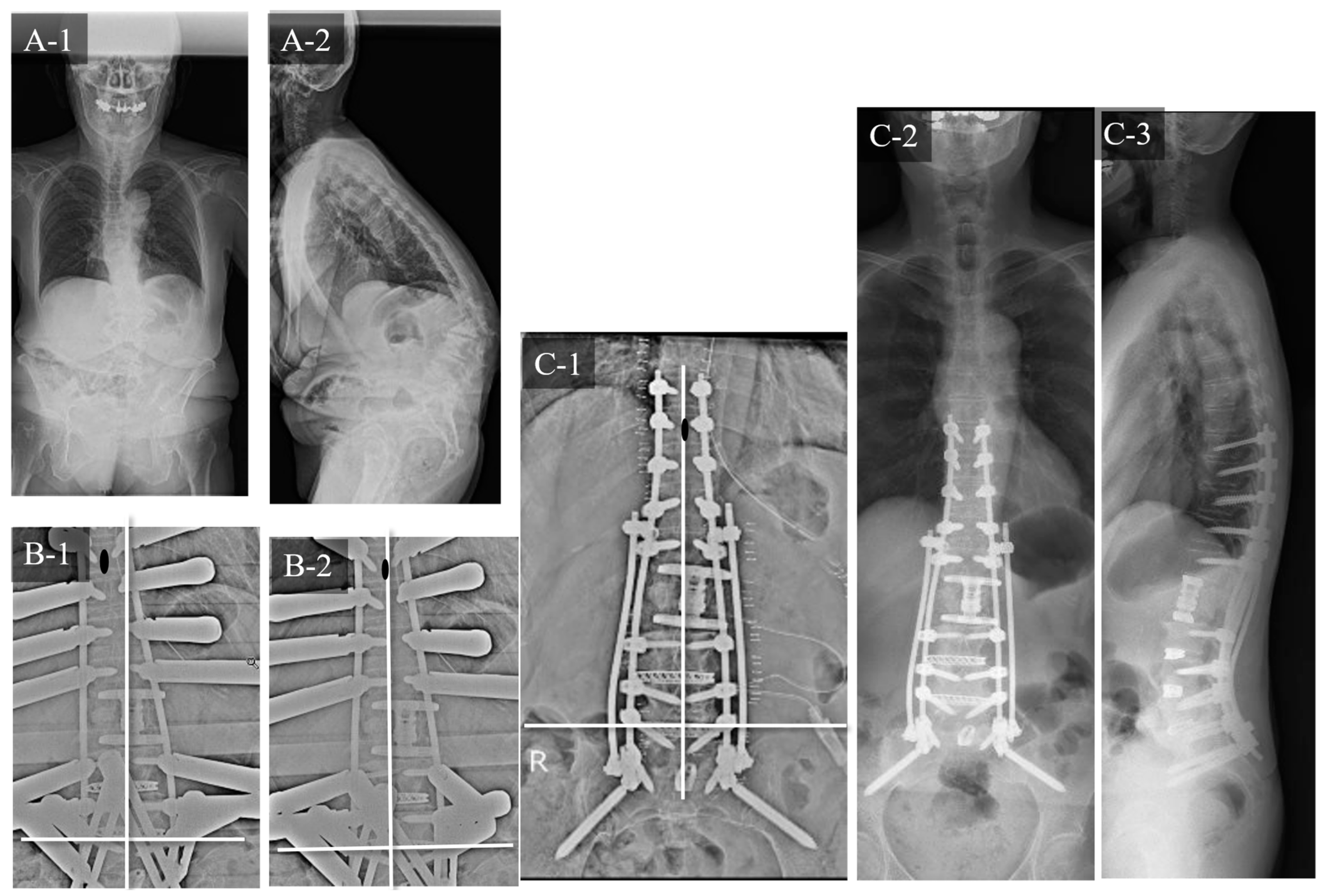
3.1. Case Study 1: RR
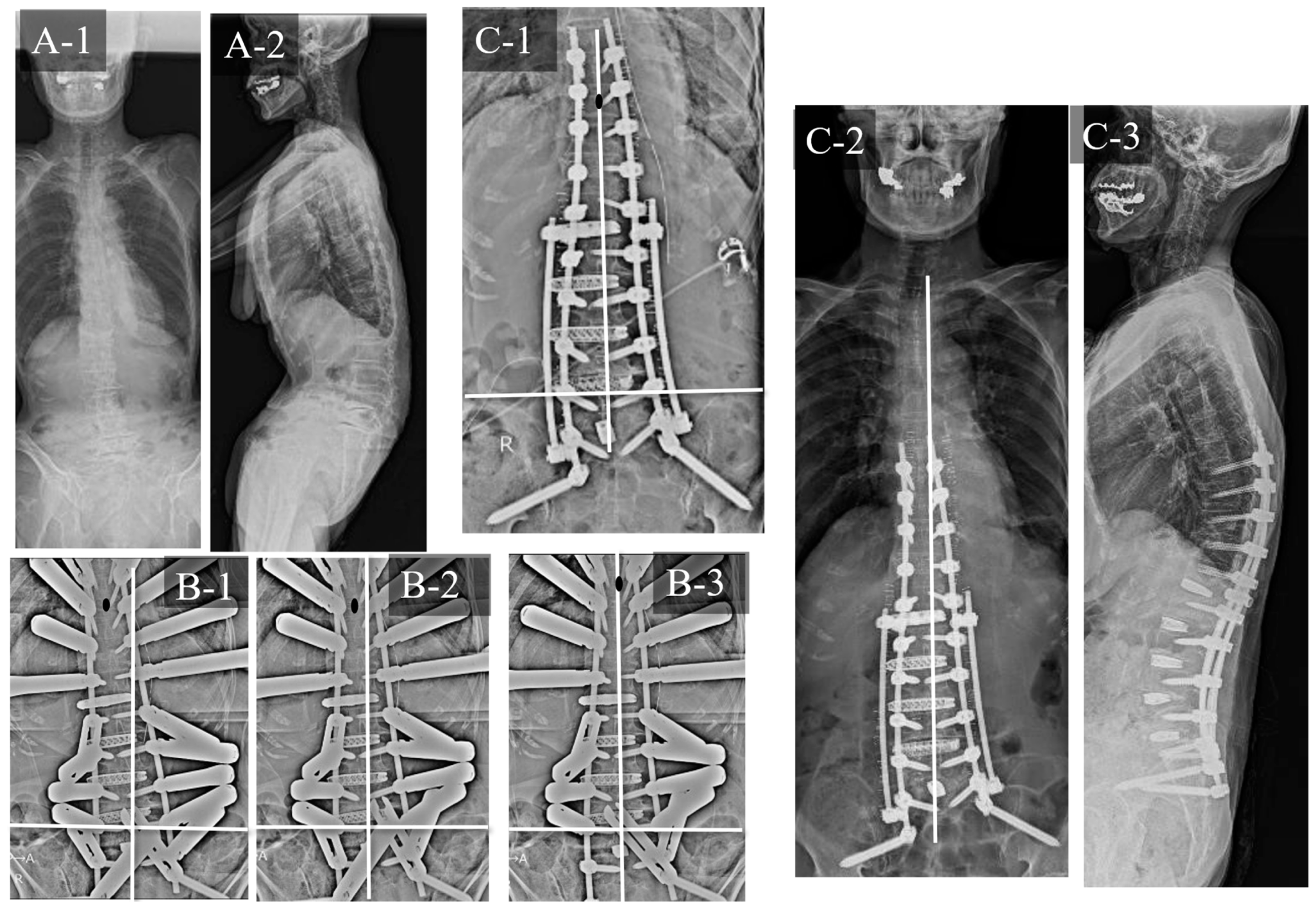
3.2. Case Study 2: RR and SD
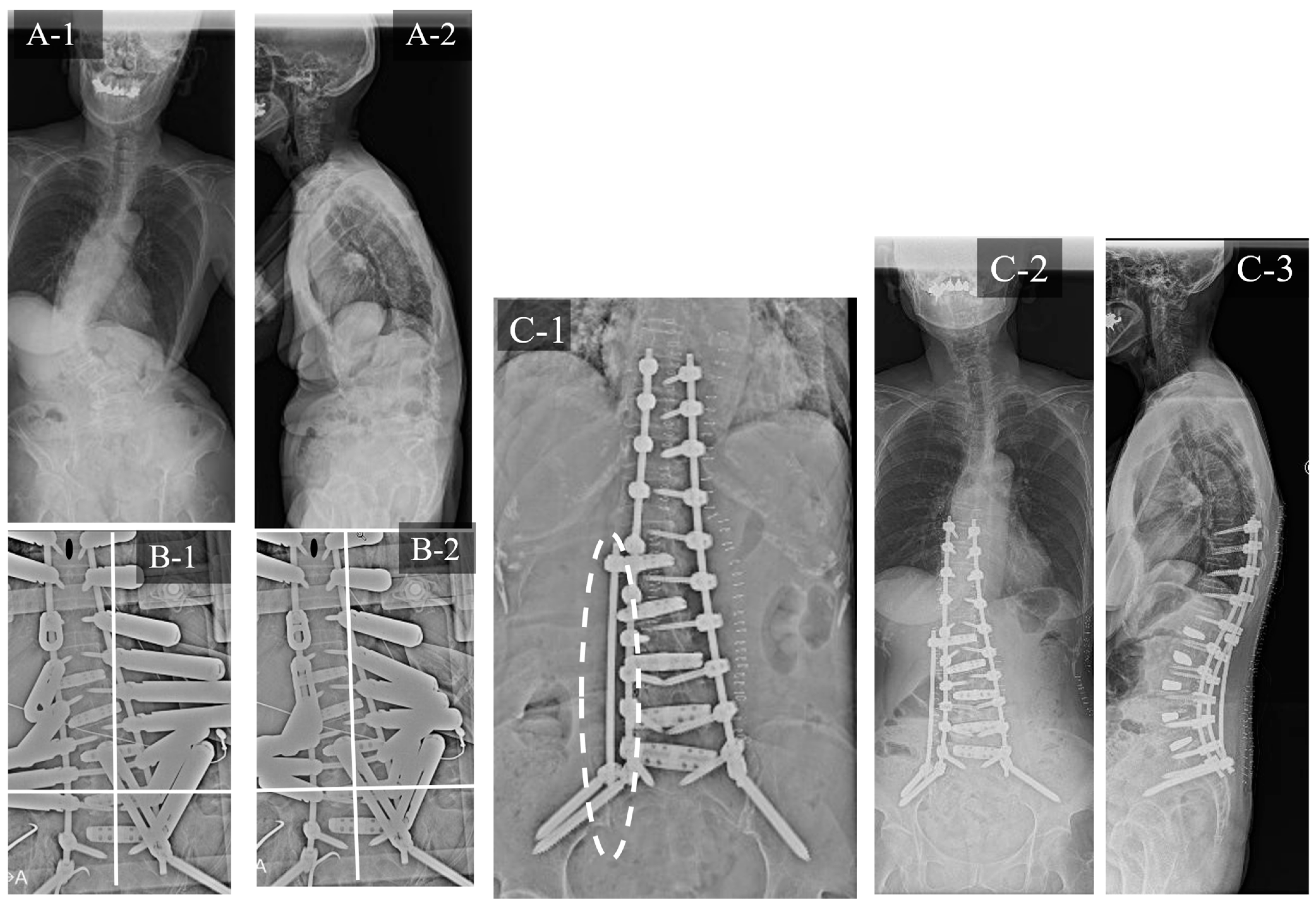
3.3. Case Study 3: RR and KR
4. Discussion
4.1. Risk Factors for CI
4.2. Measures for CI
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bess, S.; Protopsaltis, T.S.; Lafage, V.; Lafage, R.; Ames, C.P.; Errico, T.; Smith, J.S. Clinical and radiographic evaluation of adult spinal deformity. Clin. Spine Surg. 2016, 29, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Bess, S.; Line, B.; Fu, K.M.; McCarthy, I.; Lafage, V.; Schwab, F.; Shaffrey, C.; Ames, C.; Akbarnia, B.; Jo, H.; et al. The health impact of symptomatic adult spinal deformity: Comparison of deformity types to united states population norms and chronic diseases. Spine 2016, 41, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Ohba, T.; Koyama, K.; Oba, H.; Oda, K.; Tanaka, N.; Haro, H. Clinical importance, incidence and risk factors for the development of postoperative ileus following adult spinal deformity surgery. Glob. Spine J. 2022, 12, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Acaroglu, E.; Yavuz, A.C.; Guler, U.O.; Yuksel, S.; Yavuz, Y.; Domingo-Sabat, M.; Pellise, F.; Alanay, A.; Perez Grueso, F.S.; Kleinstück, F.; et al. A decision analysis to identify the ideal treatment for adult spinal deformity: Is surgery better than non-surgical treatment in improving health-related quality of life and decreasing the disease burden. Eur. Spine J. 2016, 25, 2390–2400. [Google Scholar] [CrossRef]
- Djurasovic, M.; Glassman, S.D. Correlation of radiographic and clinical findings in spinal deformities. Neurosurg. Clin. N. Am. 2007, 18, 223–227. [Google Scholar] [CrossRef]
- Gum, J.L.; Glassman, S.D.; Douglas, L.R.; Carreon, L.Y. Correlation between cervical spine sagittal alignment and clinical outcome after anterior cervical discectomy and fusion. Am. J. Orthop. 2012, 41, E81–E84. [Google Scholar] [PubMed]
- Lenke, L.G.; Fehlings, M.G.; Shaffrey, C.I.; Cheung, K.M.; Carreon, L.; Dekutoski, M.B.; Schwab, F.J.; Boachie-Adjei, O.; Kebaish, K.M.; Ames, C.P.; et al. Neurologic outcomes of complex adult spinal deformity surgery: Results of the prospective, multicenter Scoli-RISK-1 Study. Spine 2016, 41, 204–212. [Google Scholar] [CrossRef]
- Kothari, P.; Lee, N.J.; Leven, D.M.; Lakomkin, N.; Shin, J.I.; Skovrlj, B.; Steinberger, J.; Guzman, J.Z.; Cho, S.K. Impact of gender on 30-day complications after adult spinal deformity surgery. Spine 2016, 41, 1133–1138. [Google Scholar] [CrossRef]
- Maruo, K.; Ha, Y.; Inoue, S.; Samuel, S.; Okada, E.; Hu, S.S.; Deviren, V.; Burch, S.; William, S.; Ames, C.P.; et al. Predictive factors for proximal junctional kyphosis in long fusions to the sacrum in adult spinal deformity. Spine 2013, 38, E1469–E1476. [Google Scholar] [CrossRef]
- Mok, J.M.; Cloyd, J.M.; Bradford, D.S.; Hu, S.S.; Deviren, V.; Smith, J.A.; Tay, B.; Berven, S.H. Reoperation after primary fusion for adult spinal deformity: Rate, reason, and timing. Spine 2009, 34, 832–839. [Google Scholar] [CrossRef]
- Pichelmann, M.A.; Lenke, L.G.; Bridwell, K.H.; Good, C.R.; O’Leary, P.T.; Sides, B.A. Revision rates following primary adult spinal deformity surgery: Six hundred forty-three consecutive patients followed-up to twenty-two years postoperative. Spine 2010, 35, 219–226. [Google Scholar] [CrossRef]
- Ozgur, B.M.; Aryan, H.E.; Pimenta, L.; Taylor, W.R. Extreme lateral interbody fusion (XLIF): A novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006, 6, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Park, P.; Fu, K.M.; Wang, M.Y.; Nguyen, S.; Lafage, V.; Uribe, J.S.; Ziewacz, J.; Terran, J.; Okonkwo, D.O.; et al. Does minimally invasive percutaneous posterior instrumentation reduce risk of proximal junctional kyphosis in adult spinal deformity surgery? A propensity-matched cohort analysis. Neurosurgery 2016, 78, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.M.; Mundis, G.M.; Ahmed, Y.; El Ahmadieh, T.Y.; Wang, M.Y.; Mummaneni, P.V.; Uribe, J.S.; Okonkwo, D.O.; Eastlack, R.K.; Anand, N.; et al. Comparison of radiographic results after minimally invasive, hybrid, and open surgery for adult spinal deformity: A multicenter study of 184 patients. Neurosurg. Focus 2014, 36, E13. [Google Scholar] [CrossRef]
- Ishihara, M.; Taniguchi, S.; Adachi, T.; Tani, Y.; Paku, M.; Ando, M.; Saito, T. Conditions for achieving postoperative pelvic incidence-lumbar lordosis < 10° in circumferential minimally invasive surgery for adult spinal deformity. J. Clin. Med. 2022, 11, 1586. [Google Scholar] [CrossRef]
- Ishihara, M.; Taniguchi, S.; Kawashima, K.; Adachi, T.; Paku, M.; Tani, Y.; Ando, M.; Saito, T. Bone fusion morphology after circumferential minimally invasive spine surgery using lateral lumbar interbody fusion and percutaneous pedicle screws without bone grafting in the thoracic spine: A retrospective study. Medicina 2022, 58, 496. [Google Scholar] [CrossRef]
- Ishihara, M.; Taniguchi, S.; Adachi, T.; Tani, Y.; Paku, M.; Ando, M.; Kotani, Y.; Saito, T. Analysis of measures against mechanical complications in circumferential minimally invasive surgery for adult spinal deformity. Mini-Invasive Surg. 2022, 6, 35. [Google Scholar] [CrossRef]
- Ishihara, M.; Taniguchi, S.; Adachi, T.; Tani, Y.; Paku, M.; Ando, M.; Saito, T. Surgical approaches and short-term results of Circumferential minimally invasive correction surgery for adult idiopathic scoliosis. World Neurosurg. 2023, 178, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, A.; Namikawa, T.; Kato, M.; Hori, Y.; Hidaka, N.; Nakamura, H. Factors related to postoperative coronal imbalance in adult lumbar scoliosis. J. Neurosurg. Spine 2020, 34, 66–72. [Google Scholar] [CrossRef]
- Lewis, S.J.; Keshen, S.G.; Kato, S.; Dear, T.E.; Gazendam, A.M. Risk factors for postoperative coronal balance in adult spinal deformity surgery. Glob. Spine J. 2018, 8, 690–697. [Google Scholar] [CrossRef]
- Obeid, I.; Berjano, P.; Lamartina, C.; Chopin, D.; Boissière, L.; Bourghli, A. Classification of coronal imbalance in adult scoliosis and spine deformity: A treatment-oriented guideline. Eur. Spine J. 2019, 28, 94–113. [Google Scholar] [CrossRef]
- Makhni, M.C.; Cerpa, M.; Lin, J.D.; Park, P.J.; Lenke, L.G. The “Kickstand Rod” technique for correction of coronal imbalance in patients with adult spinal deformity: Theory and technical considerations. J. Spine Surg. 2018, 4, 798–802. [Google Scholar] [CrossRef] [PubMed]
- Glattes, R.C.; Bridwell, K.H.; Lenke, L.G.; Kim, Y.J.; Rinella, A.; Edwards, C. Proximal junctional kyphosis in adult spinal deformity following long instrumented posterior spinal fusion: Incidence, outcomes, and risk factor analysis. Spine 2005, 30, 1643–1649. [Google Scholar] [CrossRef]
- Tanaka, N.; Ebata, S.; Oda, K.; Oba, H.; Haro, H.; Ohba, T. Predictors and clinical importance of postoperative coronal malalignment after surgery to correct adult spinal deformity. Clin. Spine Surg. 2020, 33, E337–E341. [Google Scholar] [CrossRef]
- Redaelli, A.; Langella, F.; Dziubak, M.; Cecchinato, R.; Damilano, M.; Peretti, G.; Berjano, P.; Lamartina, C. Useful and innovative methods for the treatment of postoperative coronal malalignment in adult scoliosis: The “kickstand rod” and “tie rod” procedures. Eur. Spine J. 2020, 29, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Ploumis, A.; Simpson, A.K.; Cha, T.D.; Herzog, J.P.; Wood, K.B. Coronal spinal balance in adult spine deformity patients with long spinal fusions: A minimum 2- to 5-year follow-up study. J. Spinal Disord. Tech. 2015, 28, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Berjano, P.; Lamartina, C. Classification of degenerative segment disease in adults with deformity of the lumbar or thoracolumbar spine. Eur. Spine J. 2014, 23, 1815–1824. [Google Scholar] [CrossRef]
- Cecchinato, R.; Berjano, P.; Aguirre, M.F.; Lamartina, C. Asymmetrical pedicle subtraction osteotomy in the lumbar spine in combined coronal and sagittal imbalance. Eur. Spine J. 2015, 24 (Suppl. S1), S66–S71. [Google Scholar] [CrossRef] [PubMed]
- Moal, B.; Schwab, F.; Ames, C.P.; Smith, J.S.; Ryan, D.; Mummaneni, P.V.; Mundis, G.M.; Terran, J.S.; Klineberg, E.; Hart, R.A.; et al. Radiographic outcomes of adult spinal deformity correction: A critical analysis of variability and failures across deformity patterns. Spine Deform. 2014, 2, 219–225. [Google Scholar] [CrossRef]
- Bao, H.; Yan, P.; Qiu, Y.; Liu, Z.; Zhu, F. Coronal imbalance in degenerative lumbar scoliosis: Prevalence and influence on surgical decision-making for spinal osteotomy. Bone Jt. J. 2016, 98-B, 1227–1233. [Google Scholar] [CrossRef]
- Daubs, M.D.; Lenke, L.G.; Bridwell, K.H.; Kim, Y.J.; Hung, M.; Cheh, G.; Koester, L.A. Does correction of preoperative coronal imbalance make a difference in outcomes of adult patients with deformity? Spine 2013, 38, 476–483. [Google Scholar] [CrossRef]
- Cho, W.; Mason, J.R.; Smith, J.S.; Shimer, A.L.; Wilson, A.S.; Shaffrey, C.I.; Shen, F.H.; Novicoff, W.M.; Fu, K.M.; Heller, J.E.; et al. Failure of lumbopelvic fixation after long construct fusions in patients with adult spinal deformity: Clinical and radiographic risk factors: Clinical article. J. Neurosurg. Spine 2013, 19, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Buell, T.J.; Shaffrey, C.I.; Kim, H.J.; Klineberg, E.O.; Lafage, V.; Lafage, R.; Protopsaltis, T.S.; Passias, P.G.; Mundis, G.M., Jr.; Eastlack, R.K.; et al. Global coronal decompensation and adult spinal deformity surgery: Comparison of upper-thoracic versus lower-thoracic proximal fixation for long fusions. J. Neurosurg. Spine 2021, 35, 761–773. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Z.; Chi, P.; Chi, C. Orientation of L4 coronal tilt relative to C7 plumb line as a predictor for postoperative coronal imbalance in patients with degenerative lumbar scoliosis. Sci. Rep. 2020, 10, 16148. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Song, K.; Wu, B.; Chi, P.; Wang, Z.; Wang, Z. Coronal imbalance in adult spinal deformity following posterior spinal fusion with instrument: A related parameters analysis. Spine 2019, 44, 550–557. [Google Scholar] [CrossRef]
- Kurra, S.; Metkar, U.; Yirenkyi, H.; Tallarico, R.A.; Lavelle, W.F. Assessment of coronal spinal alignment for adult spine deformity cases after intraoperative T square shaped use. Spine Deform. 2018, 6, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Buell, T.J.; Christiansen, P.A.; Nguyen, J.H.; Chen, C.J.; Yen, C.P.; Shaffrey, C.I.; Smith, J.S. Coronal correction using kickstand rods for adult thoracolumbar/lumbar scoliosis: Case series with analysis of early outcomes and complications. Oper. Neurosurg. 2020, 19, 403–413. [Google Scholar] [CrossRef]
- Fiani, B.; Jarrah, R.M. The “Kickstand Rod” technique for coronal imbalance in patients with spinal deformity: A case report with review of literature. Cureus 2020, 12, e11876. [Google Scholar] [CrossRef] [PubMed]
- Makhni, M.C.; Zhang, Y.; Park, P.J.; Cerpa, M.; Yang, M.; Pham, M.H.; Sielatycki, J.A.; Beauchamp, E.C.; Lenke, L.G. The “kickstand rod” technique for correction of coronal imbalance in patients with adult spinal deformity: Initial case series. J. Neurosurg. Spine 2019, 32, 415–422. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group P (n = 50) | Group G (n = 65) | p Value (Group P vs. Group G) | |
|---|---|---|---|---|
| Age (years) | 73.3 ± 6.9 | 73.0 ± 7.7 | 0.762 | |
| Rate of women (%) | 80.8 | 78.1 | 0.859 | |
| Period of follow-up (months) | 40.7 ± 6.3 | 40.6 ± 6.2 | 0.792 | |
| Rod diameter/number in construct | 5.5 mm/2 rods | 20 | 25 | 0.509 |
| 6 mm/2 rods | 10 | 13 | ||
| 5.5 mm/3 rods | 20 | 27 | ||
| Number of levels fused | 10.3 ± 0.5 | 10.4 ± 0.5 | 0.721 | |
| Number of LLIF | 4.0 ± 0.3 | 4.1 ± 0.5 | 0.692 | |
| UIV (case) | T8 | 2 | 0 | 0.185 |
| T9 | 15 | 16 | ||
| T10 | 33 | 49 | ||
| Operative time (min) | Anterior (first surgery) | 112.4 ± 40.2 | 100.8 ± 26.5 | 0.613 |
| Posterior (second surgery) | 233.2 ± 52.1 ** | 233.0 ± 47.7 ** | 0.752 | |
| Blood loss (mL) | Anterior (first surgery) | 117.7 ± 152.4 | 63.0 ± 75.1 | 0.316 |
| Posterior (second surgery) | 488.6 ± 290.9 ** | 528.1 ± 350.9 ** | 0.263 | |
| ODI | before surgery | 41.3 ± 6.2 | 40.1 ± 5.1 | 0.425 |
| Final | 24.8 ± 5.8 * | 25.9 ± 2.6 * | 0.501 | |
| Complications | PJK | 12% | 15% | 0.679 |
| RF | 9% | 13% | 0.498 | |
| Type of CI | Total (n = 115) | Group P (n = 50) | Group G (n = 65) | p Value (Concave CI vs. Convex CI) | ||
|---|---|---|---|---|---|---|
| Preop | Non-CI (case) | 72 (63%) | 26 | 46 | 0.031 * | |
| CI (case) | 43 (37%) | 24 | 19 | |||
| CI | Concave CI (case) | 23 (20%) | 10 | 14 | 0.036 * | |
| Convex CI (case) | 20 (17%) | 14 | 5 | |||
| Postop | Non-CI (case) | 110 (96%) | 47 | 63 | 0.377 | |
| CI (case) | 5 (4%) | 3 | 2 | |||
| CI | Concave CI (case) | 2 (1%) | 0 | 2 | 0.100 | |
| Convex CI (case) | 3 (3%) | 3 | 0 | |||
| Group P (n = 50) | Group G (n = 65) | p Value | |
|---|---|---|---|
| PI (°) | 43.1 ± 10.5 | 46.5 ± 10.8 | 0.071 |
| Preop LL (°) | 9.2 ± 16.1 | 13.0 ± 15.8 | 0.258 |
| Postop LL (°) | 46.2 ± 10.2 | 48.8 ± 10.6 | 0.253 |
| Preop PI-LL (°) | 33.9 ± 17.9 | 38.5 ± 18.1 | 0.186 |
| Postop PI-LL (°) | 1.2 ± 11.9 | 2.6 ± 12.1 | 0.142 |
| Preop PT (°) | 29.5 ± 11.1 | 30.7 ± 11.3 | 0.592 |
| Postop PT (°) | 16.9 ± 9.8 | 18.9 ± 9.9 | 0.089 |
| Preop TK (°) | 21.3 ± 16.2 | 16.2 ± 16.3 | 0.123 |
| Postop TK (°) | 38.8 ± 10.9 | 36.7 ± 11.1 | 0.355 |
| Preop C7CSVL (mm) | 45.4 ± 36.9 | 40.1 ± 34.1 | 0.166 |
| Postop C7CSVL (mm) | 8.0 ± 8.1 | 6.2 ± 7.2 | 0.142 |
| Preop CA (°) | 42.3 ± 32.9 | 39.1 ± 31.0 | 0.326 |
| Postop CA (°) | 16.2 ± 9.0 | 12.2 ± 8.1 | 0.162 |
| Preop L4 tilt (°) | 13.2 ± 8.8 | 7.2 ± 6.9 | 0.026 * |
| Postop L4 tilt (°) | 5.3 ± 4.1 | 2.1 ± 2.3 | 0.042 * |
| Group RR (n = 38) | Group SD (RR and SD) (n = 7) | Group KR (RR and KR) (n = 5) | Total | ||
|---|---|---|---|---|---|
| UIV-CSVL | Pre-measure (mm) | 19.9 ± 17.5 | 25.3 ± 3.9 | 32.1 ± 1.4 | 24.8 ± 5.9 |
| Post-measure (mm) | 6.2 ± 1.7 | 7.2 ± 1.8 | 7.7 ± 0.8 | 10.1 ± 2.2 | |
| ΔUIV-CSVL (mm) | 13.9 ± 2.1 | 20.1 ± 1.9 | 24.4 ± 1.1 | 14.7 ± 4.2 | |
| C7-CSVL | Preop (mm) | 39.2 ± 9.9 | 34.1 ± 9.1 | 35.5 ± 5.1 | 38.1 ± 9.8 |
| Postop (mm) | 7.2 ± 1.8 | 9.2 ± 1.9 | 8.5 ± 1.2 | 8.0 ± 1.8 |
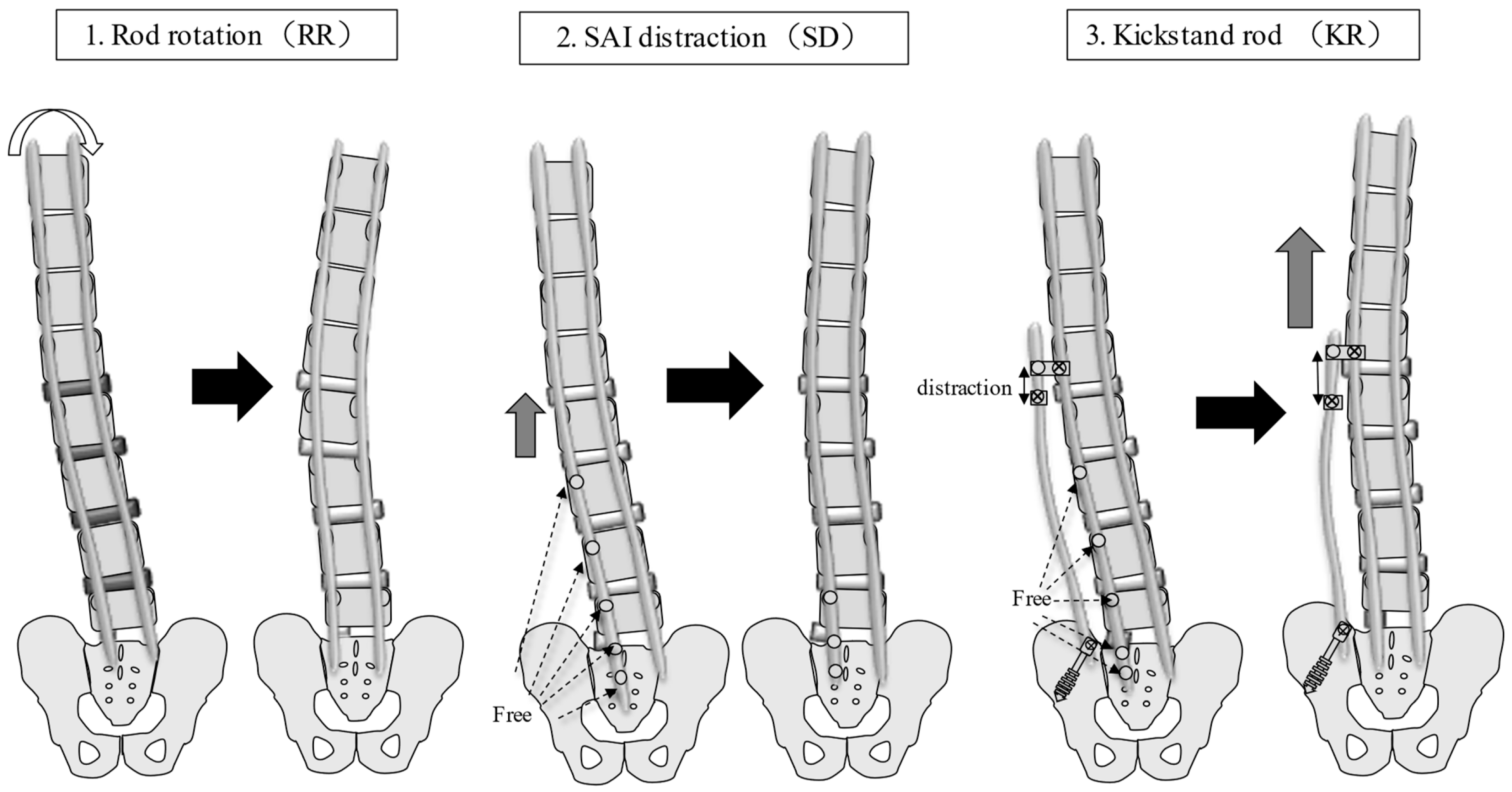
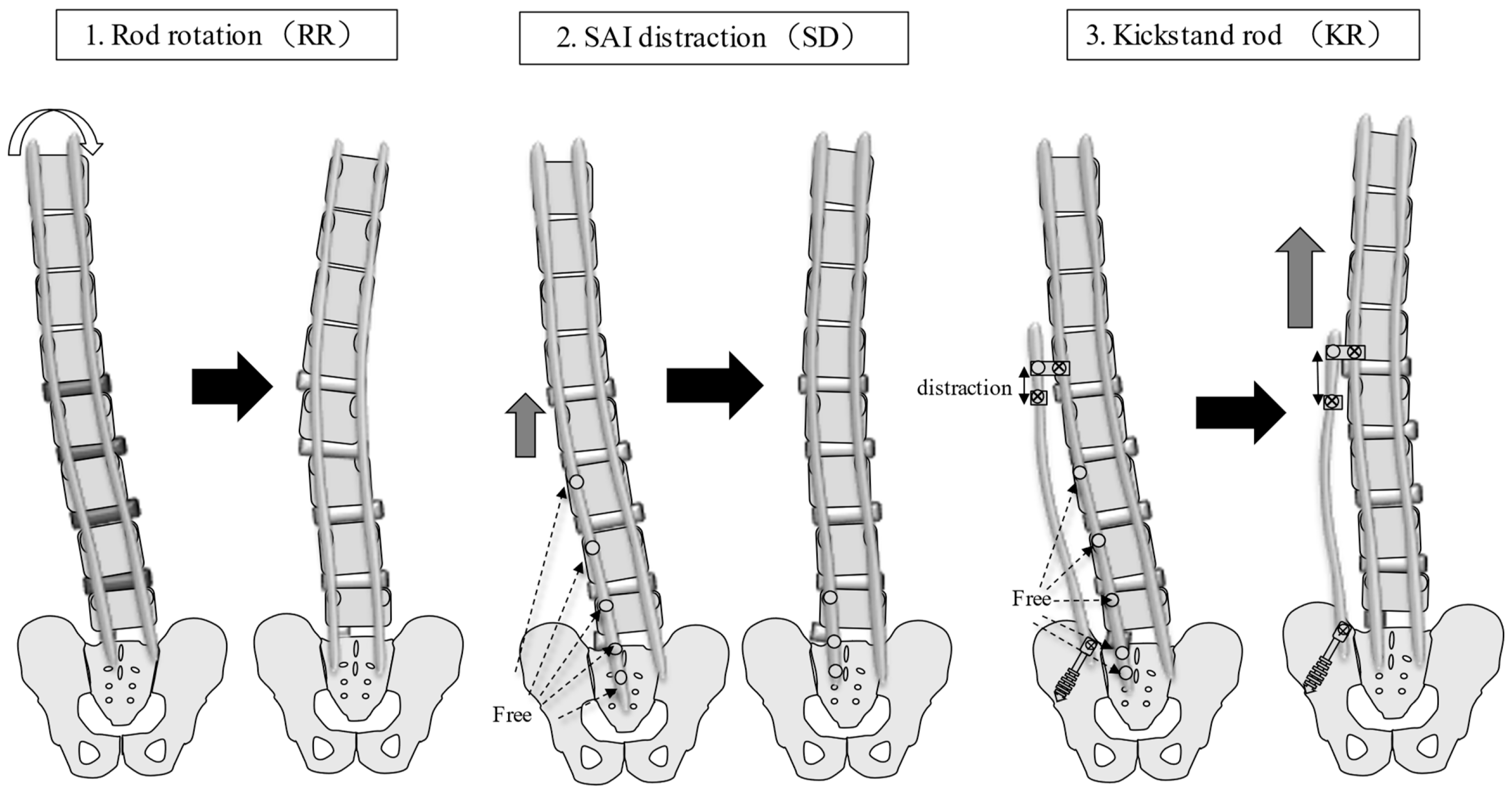
| Principle of Correction | Correction Force | Limitation of Correction | Required Time | |
|---|---|---|---|---|
| RR | Global imbalance | weak | limited | 2 or 3 min |
| SD | Correction of lumbosacral fractional curve | moderate | limited | About 5 min |
| KR | Correction of lumbosacral and global imbalance | strong | limited | More than 10 min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishihara, M.; Taniguchi, S.; Ono, N.; Adachi, T.; Tani, Y.; Paku, M.; Kawashima, K.; Ando, M.; Saito, T. New Effective Intraoperative Techniques for the Prevention of Coronal Imbalance after Circumferential Minimally Invasive Correction Surgery for Adult Spinal Deformity. J. Clin. Med. 2023, 12, 5670. https://doi.org/10.3390/jcm12175670
Ishihara M, Taniguchi S, Ono N, Adachi T, Tani Y, Paku M, Kawashima K, Ando M, Saito T. New Effective Intraoperative Techniques for the Prevention of Coronal Imbalance after Circumferential Minimally Invasive Correction Surgery for Adult Spinal Deformity. Journal of Clinical Medicine. 2023; 12(17):5670. https://doi.org/10.3390/jcm12175670
Chicago/Turabian StyleIshihara, Masayuki, Shinichirou Taniguchi, Naoto Ono, Takashi Adachi, Yoichi Tani, Masaaki Paku, Koki Kawashima, Muneharu Ando, and Takanori Saito. 2023. "New Effective Intraoperative Techniques for the Prevention of Coronal Imbalance after Circumferential Minimally Invasive Correction Surgery for Adult Spinal Deformity" Journal of Clinical Medicine 12, no. 17: 5670. https://doi.org/10.3390/jcm12175670
APA StyleIshihara, M., Taniguchi, S., Ono, N., Adachi, T., Tani, Y., Paku, M., Kawashima, K., Ando, M., & Saito, T. (2023). New Effective Intraoperative Techniques for the Prevention of Coronal Imbalance after Circumferential Minimally Invasive Correction Surgery for Adult Spinal Deformity. Journal of Clinical Medicine, 12(17), 5670. https://doi.org/10.3390/jcm12175670