
Associations between Birth Weight and Adult Sleep Characteristics: A Cross-Sectional Analysis from the UAEHFS

 ,
,  ,
,  , ,
, ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
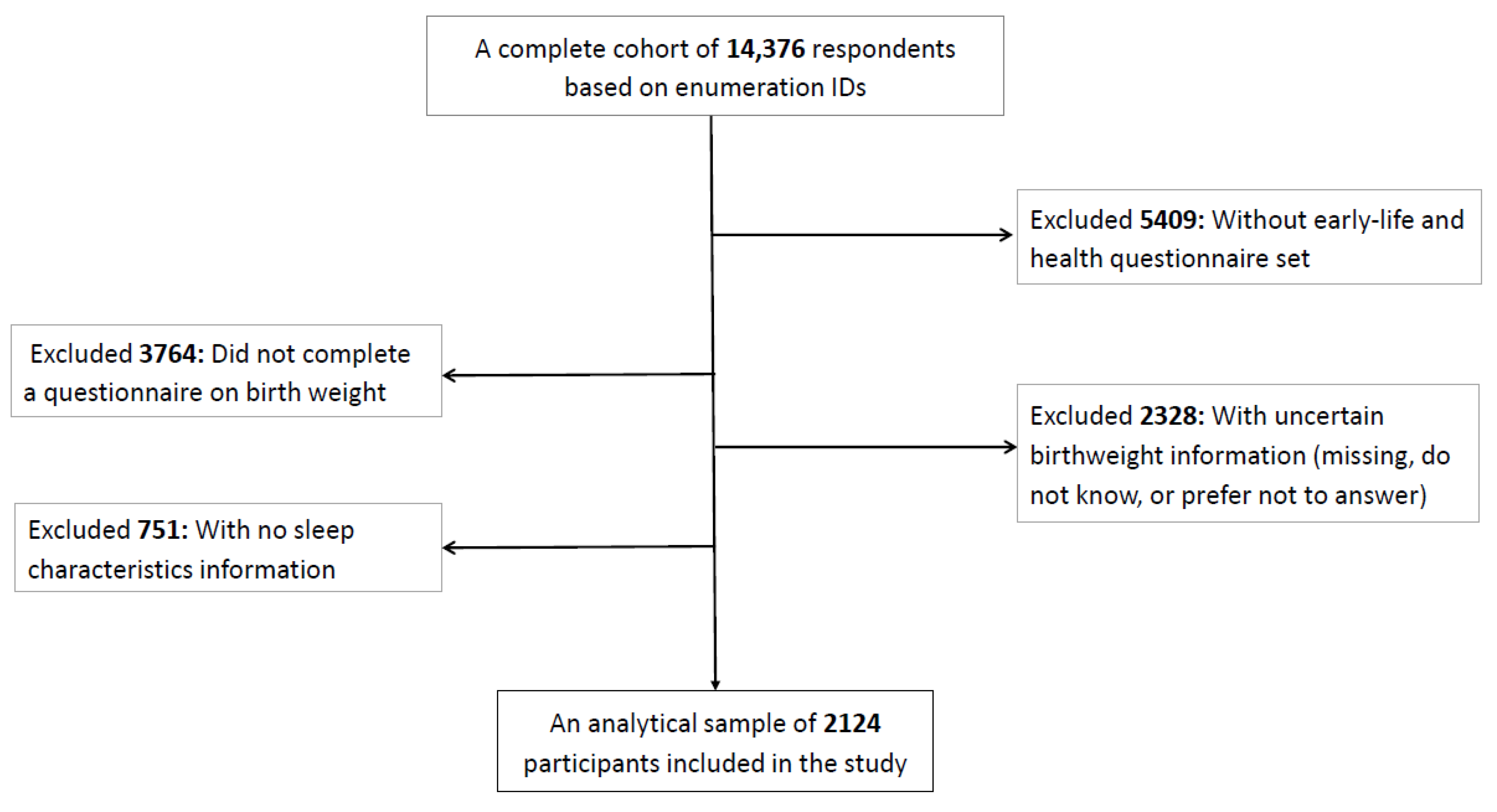
2.1. Study Design, Participants, and Setting
2.2. Measurements
2.2.1. Birth Weight and Adult Sleep Characteristics
2.2.2. Demographic Characteristics
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chaput, J.-P.; Dutil, C.; Featherstone, R.; Ross, R.; Giangregorio, L.; Saunders, T.J.; Janssen, I.; Poitras, V.J.; Kho, M.E.; Ross-White, A.; et al. Sleep timing, sleep consistency, and health in adults: A systematic review. Appl. Physiol. Nutr. Metab. 2020, 45, S232–S247. [Google Scholar] [CrossRef] [PubMed]
- Gadie, A.; Shafto, M.; Leng, Y.; Cam-CAN; Kievit, R.A. How are age-related differences in sleep quality associated with health outcomes? An epidemiological investigation in a UK cohort of 2406 adults. BMJ Open 2017, 7, e014920. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, A.; Stickley, A. The association between sleep problems and psychotic symptoms in the general population: A global perspective. Sleep 2015, 38, 1875–1885. [Google Scholar] [CrossRef] [PubMed]
- Léger, D.; Poursain, B.; Neubauer, D.; Uchiyama, M. An international survey of sleeping problems in the general population. Curr. Med. Res. Opin. 2008, 24, 307–317. [Google Scholar] [CrossRef]
- Buboltz, W., Jr.; Jenkins, S.M.; Soper, B.; Woller, K.; Johnson, P.; Faes, T. Sleep habits and patterns of college students: An expanded study. J. Coll. Couns. 2009, 2, 113–124. [Google Scholar] [CrossRef]
- Becker, S.P.; Jarrett, M.A.; Luebbe, A.M.; Garner, A.A.; Burns, G.L.; Kofler, M.J. Sleep in a large, multi-university sample of college students: Sleep problem prevalence, sex differences, and mental health correlates. Sleep Health 2018, 4, 174–181. [Google Scholar] [CrossRef]
- Stickley, A.; Leinsalu, M.; DeVylder, J.E.; Inoue, Y.; Koyanagi, A. Sleep problems and depression among 237 023 community-dwelling adults in 46 low-and middle-income countries. Sci. Rep. 2019, 9, 12011. [Google Scholar] [CrossRef]
- Lyytikäinen, P.; Lallukka, T.; Lahelma, E.; Rahkonen, O. Sleep problems and major weight gain: A follow-up study. Int. J. Obes. 2011, 35, 109–114. [Google Scholar] [CrossRef]
- Spiegel, K.; Tasali, E.; Leproult, R.; Van Cauter, E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat. Rev. Endocrinol. 2009, 5, 253–261. [Google Scholar] [CrossRef]
- Agbozo, F.; Abubakari, A.; Der, J.; Jahn, A. Prevalence of low birth weight, macrosomia and stillbirth and their relationship to associated maternal risk factors in Hohoe Municipality, Ghana. Midwifery 2016, 40, 200–206. [Google Scholar] [CrossRef]
- Axame, W.K.; Binka, F.N.; Kweku, M. Prevalence and factors associated with low birth weight and preterm delivery in the Hohoe municipality of Ghana. Adv. Public Health 2022, 2022, 3955869 . [Google Scholar] [CrossRef]
- De Mendonça, E.L.S.S.; de Lima Macêna, M.; Bueno, N.B.; de Oliveira, A.C.M.; Mello, C.S. Premature birth, low birth weight, small for gestational age and chronic non-communicable diseases in adult life: A systematic review with meta-analysis. Early Hum. Dev. 2020, 149, 105154. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Global Health Observatory; World Health Organization: Geneva, Switzerland, 2017; Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/low-birthweight-(-newborns-who-weigh-2.5kg) (accessed on 15 March 2023).
- World Health Organization. Global Nutrition Targets 2025, Low Birth Weight Policy Brief 2014; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/149020 (accessed on 15 March 2023).
- Li, Y.; Ley, S.H.; VanderWeele, T.J.; Curhan, G.C.; Rich-Edwards, J.W.; Willett, W.C.; Forman, J.P.; Hu, F.B.; Qi, L. Joint association between birth weight at term and later life adherence to a healthy lifestyle with risk of hypertension: A prospective cohort study. BMC Med. 2015, 13, 175. [Google Scholar] [CrossRef] [PubMed]
- Yarmolinsky, J.; Mueller, N.T.; Duncan, B.B.; Chor, D.; Bensenor, I.M.; Griep, R.H.; Appel, L.J.; Barreto, S.M.; Schmidt, M.I. Sex-specific associations of low birth weight with adult-onset diabetes and measures of glucose homeostasis: Brazilian Longitudinal Study of Adult Health. Sci. Rep. 2016, 6, 37032. [Google Scholar] [CrossRef] [PubMed]
- Jeanne, T.L.; Hooker, E.R.; Nguyen, T.; Messer, L.C.; Sacks, R.M.; Andrea, S.B.; Boone-Heinonen, J. High birth weight modifies association between adolescent physical activity and cardiometabolic health in women and not men. Prev. Med. 2018, 108, 29–35. [Google Scholar] [CrossRef]
- Rockenbach, G.; Luft, V.; Mueller, N.; Duncan, B.; Stein, M.; Vigo, Á.; Matos, S.M.; Fonseca, M.J.M.; Barreto, S.M.; Benseñor, I.M.; et al. Sex-specific associations of birth weight with measures of adiposity in mid-to-late adulthood: The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Int. J. Obes. 2016, 40, 1286–1291. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Zhang, Z.-X.; Li, W.-H.; Feng, K.; Sun, Q.; Cohen, H.J.; Xu, T.; Wang, H.; Liu, A.-M.; Gong, X.-M.; et al. Low birth weight is associated with components of the metabolic syndrome. Metabolism 2010, 59, 1282–1286. [Google Scholar] [CrossRef]
- Kwon, E.J.; Kim, Y.J. What is fetal programming?: A lifetime health is under the control of in utero health. Obstet. Gynecol. Sci. 2017, 60, 506–519. [Google Scholar] [CrossRef]
- Strang-Karlsson, S.; Räikkönen, K.; Kajantie, E.; Andersson, S.; Hovi, P.; Heinonen, K.; Pesonen, A.-K.; Järvenpää, A.-L.; Eriksson, J.G.; Paavonen, E.J. Sleep quality in young adults with very low birth weight—The Helsinki study of very low birth weight adults. J. Pediatr. Psychol. 2008, 33, 387–395. [Google Scholar] [CrossRef]
- Hovi, P.; Andersson, S.; Eriksson, J.G.; Järvenpää, A.L.; Strang-Karlsson, S.; Mäkitie, O.; Kajantie, E. Glucose regulation in young adults with very low birth weight. N. Engl. J. Med. 2007, 356, 2053–2063. [Google Scholar] [CrossRef]
- Abdulle, A.; Alnaeemi, A.; Aljunaibi, A.; Al Ali, A.; Al Saedi, K.; Al Zaabi, E.; Oumeziane, N.; Al Bastaki, M.; Al-Houqani, M.; Al Maskari, F.; et al. The UAE healthy future study: A pilot for a prospective cohort study of 20,000 United Arab Emirates nationals. BMC Public Health 2018, 18, 101. [Google Scholar] [CrossRef]
- Iguacel, I.; Escartín, L.; Fernández-Alvira, J.M.; Iglesia, I.; Labayen, I.; Moreno, L.A.; Samper, M.P.; Rodríguez, G. Early life risk factors and their cumulative effects as predictors of overweight in Spanish children. Int. J. Public Health 2018, 63, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Alhouqani, S.; Al Manhali, M.; Al Essa, A.; Al-Houqani, M. Evaluation of the Arabic version of STOP-Bang questionnaire as a screening tool for obstructive sleep apnea. Sleep Breath 2015, 19, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation. World Health Organ Technol. Rep. Ser. 2000, 894, 1–253. Available online: https://apps.who.int/iris/handle/10665/42330 (accessed on 27 February 2023).
- Palm, A.; Janson, C.; Lindberg, E. The impact of obesity and weight gain on development of sleep problems in a population-based sample. Sleep Med. 2015, 16, 593–597. [Google Scholar] [CrossRef] [PubMed]
- Denman, D.C.; Baldwin, A.S.; Betts, A.C.; McQueen, A.; Tiro, J.A. Reducing “I don’t know” responses and missing survey data: Implications for measurement. Med. Decis. Mak. 2018, 38, 673–682. [Google Scholar] [CrossRef]
- The World Bank. Low-Birthweight Babies—United Arab Emirates. 2023. Available online: https://data.worldbank.org/indicator/SH.STA.BRTW.ZS?locations=AE (accessed on 13 January 2023).
- Taha, Z.; Ali Hassan, A.; Wikkeling-Scott, L.; Papandreou, D. Factors associated with preterm birth and low birth weight in Abu Dhabi, the United Arab Emirates. Int. J. Environ. Res. Public Health 2020, 17, 1382. [Google Scholar] [CrossRef]
- Mindell, J.A.; Lee, C.; Sadeh, A. Young child and maternal sleep in the Middle East. Sleep Med. 2017, 32, 75–82. [Google Scholar] [CrossRef]
- Alafif, N.; Alruwaili, N.W. Sleep Duration, Body Mass Index, and Dietary Behaviour among KSU Students. Nutrients 2023, 15, 510. [Google Scholar] [CrossRef]
- Trotti, L.M. Waking up is the hardest thing I do all day: Sleep inertia and sleep drunkenness. Sleep Med. Rev. 2017, 35, 76–84. [Google Scholar] [CrossRef]
- Vallat, R.; Meunier, D.; Nicolas, A.; Ruby, P. Hard to wake up? The cerebral correlates of sleep inertia assessed using combined behavioral, EEG and fMRI measures. NeuroImage 2019, 184, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Tassi, P.; Muzet, A. Sleep inertia. Sleep Med. Rev. 2000, 4, 341–353. [Google Scholar] [CrossRef]
- Gössel-Symank, R.; Grimmer, I.; Korte, J.; Siegmund, R. Actigraphic monitoring of the activity-rest behavior of preterm and full-term infants at 20 months of age. Chronobiol. Int. 2004, 21, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Hoppenbrouwers, T.; Hodgman, J.E.; Rybine, D.; Fabrikant, G.; Corwin, M.; Crowell, D.; Weese-Mayer, D.E. Sleep architecture in term and preterm infants beyond the neonatal period: The influence of gestational age, steroids, and ventilatory support. Sleep 2005, 28, 1428–1436. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, T.; Grecian, S.; Reynolds, R. Sex differences in early-life programming of the hypothalamic–pituitary–adrenal axis in humans suggest increased vulnerability in females: A systematic review. J. Dev. Orig. Health Dis. 2017, 8, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Carrier, J.; Semba, K.; Deurveilher, S.; Drogos, L.; Cyr-Cronier, J.; Lord, C.; Sekerovick, Z. Sex differences in age-related changes in the sleep-wake cycle. Front. Neuroendocrinol. 2017, 47, 66–85. [Google Scholar] [CrossRef]
- Reynolds, R.M. Glucocorticoid excess and the developmental origins of disease: Two decades of testing the hypothesis–2012 Curt Richter Award Winner. Psychoneuroendocrinology 2013, 38, 1–11. [Google Scholar] [CrossRef]
- Van Dalfsen, J.H.; Markus, C.R. The influence of sleep on human hypothalamic–pituitary–adrenal (HPA) axis reactivity: A systematic review. Sleep Med. Rev. 2018, 39, 187–194. [Google Scholar] [CrossRef]
- Fogelholm, M.; Kronholm, E.; Kukkonen-Harjula, K.; Partonen, T.; Partinen, M.; Härmä, M. Sleep-related disturbances and physical inactivity are independently associated with obesity in adults. Int. J. Obes. 2007, 31, 1713–1721. [Google Scholar] [CrossRef]
- Yusufali, A.; Bazargani, N.; Muhammed, K.; Gabroun, A.; AlMazrooei, A.; Agrawal, A.; Al-Mulla, A.; Hajat, C.; Baslaib, F.; Philip, J.; et al. Opportunistic screening for CVD risk factors: The Dubai shopping for cardiovascular risk study (DISCOVERY). Glob. Hear. 2015, 10, 265–272. [Google Scholar] [CrossRef]
- Mamdouh, H.; Hussain, H.Y.; Ibrahim, G.M.; Alawadi, F.; Hassanein, M.; Al Zarooni, A.; Al Suwaidi, H.; Hassan, A.; Alsheikh-Ali, A.; Alnakhi, W.K. Prevalence and associated risk factors of overweight and obesity among adult population in Dubai: A population-based cross-sectional survey in Dubai, the United Arab Emirates. BMJ Open 2023, 13, e062053. [Google Scholar] [CrossRef] [PubMed]
- Byberg, L.; McKeigue, P.; Zethelius, B.; Lithell, H. Birth weight and the insulin resistance syndrome: Association of low birth weight with truncal obesity and raised plasminogen activator inhibitor-1 but not with abdominal obesity or plasma lipid disturbances. Diabetologia 2000, 43, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Fatima, Y.; Doi, S.A.; Mamun, A. Sleep quality and obesity in young subjects: A meta-analysis. Obes. Rev. 2016, 17, 1154–1166. [Google Scholar] [CrossRef]
- Patel, S.R.; Hayes, A.L.; Blackwell, T.; Evans, D.S.; Ancoli-Israel, S.; Wing, Y.K.; Stone, K.L. The association between sleep patterns and obesity in older adults. Int. J. Obes. 2014, 38, 1159–1164. [Google Scholar] [CrossRef]
- Meurling, I.J.; O’Shea, D.; Garvey, J.F. Obesity and sleep: A growing concern. Curr. Opin. Pulm. Med. 2019, 25, 602–608. [Google Scholar] [CrossRef]
- Iglowstein, I.; Latal Hajnal, B.; Molinari, L.; Largo, R.H.; Jenni, O.G. Sleep behaviour in preterm children from birth to age 10 years: A longitudinal study. Acta Paediatr. 2006, 95, 1691–1693. [Google Scholar] [CrossRef] [PubMed]
- Jaworowicz, D.J.; Nie, J.; Bonner, M.R.; Han, D.; Vito, D.; Hutson, A.; Potischman, N.; Trevisan, M.; Muti, P.; Freudenheim, J.L. Agreement between self-reported birth weight and birth certificate weights. J. Dev. Orig. Health Dis. 2010, 1, 106–113. [Google Scholar] [CrossRef]
- Tehranifar, P.; Liao, Y.; Flom, J.D.; Terry, M.B. Validity of self-reported birth weight by adult women: Sociodemographic influences and implications for life-course studies. Am. J. Epidemiol. 2009, 170, 910–917. [Google Scholar] [CrossRef]
- Nilsen, T.S.; Kutschke, J.; Brandt, I.; Harris, J.R. Validity of self-reported birth weight: Results from a Norwegian twin sample. Twin Res. Hum. Genet. 2017, 20, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Girschik, J.; Fritschi, L.; Heyworth, J.; Waters, F. Validation of self-reported sleep against actigraphy. J. Epidemiol. 2012, 22, 462–468. [Google Scholar] [CrossRef]
- Scarlett, S.; Nolan, H.N.; Kenny, R.A.; O’Connell, M.D. Discrepancies in self-reported and actigraphy-based sleep duration are associated with self-reported insomnia symptoms in community dwelling older adults. Sleep Health 2021, 7, 83–92. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic Characteristics | Total Sample (N = 2124) | Male, 45.9% (N = 974) | Female, 54.1% (N = 1150) |
|---|---|---|---|
| Age, year (mean ± SD) | 27.2 ± 7.6 | 28.9 ± 7.4 | 25.8 ± 7.5 |
| Current BMI, kg/m2 (mean ± SD) | 27.2 ± 6.6 | 28.3 ± 5.9 | 26.3 ± 6.9 |
| Normal or below (<25 kg/m2) | 735 (34.6) | 237 (24.3) | 498 (43.3) |
| Overweight (25 to <30 kg/m2) | 554 (26.1) | 319 (32.8) | 235 (20.4) |
| Obese (≥30 kg/m2) | 521 (24.5) | 266 (27.3) | 255 (22.2) |
| Missing | 314 (14.8) | 152 (15.6) | 162 (14.1) |
| Marital status, n (%) | |||
| Never married | 1251 (58.9) | 437 (44.9) | 814 (70.8) |
| Ever married | 873(41.1) | 689 (55.1) | 336 (29.2) |
| Urbanicity, n (%) | |||
| Rural or other non-urban | 244 (11.5) | 98 (10.1) | 146 (12.7) |
| Urban | 1717 (80.8) | 780 (80.1) | 937 (81.5) |
| Missing | 163 (7.7) | 96 (9.9) | 67 (5.8) |
| Education attainment, n (%) | |||
| <6 years of schooling or missing | 72 (3.4) | 35 (3.6) | 37 (3.2) |
| 6 to 12 years of schooling | 930 (43.8) | 437 (44.9) | 493 (42.9) |
| ≥12+ years of schooling | 1122 (52.8) | 502 (51.5) | 620 (53.9) |
| Overall health status, n (%) | |||
| Poor or fair | 399 (18.8) | 149 (15.3) | 250 (21.7) |
| Good or excellent | 1633 (76.9) | 771 (79.2) | 862 (75.0) |
| Missing | 92 (4.3) | 54 (5.5) | 38 (3.3) |
| Birth weight, n (%) | |||
| Low birth weight or LBW (<2.5 kg) | 709 (33.4) | 285 (29.3) | 424 (36.9) |
| Normal birth weight (≥2.5 kg) | 1415 (66.6) | 689 (70.7) | 726 (63.1) |
| Sleep Characteristics | Total Sample (N = 2124) | Male, 45.9% (N = 974) | Female, 54.1% (N = 1150) |
|---|---|---|---|
| Sleep duration, mean ± SD | 7.1 ± 2.1 | 6.9 ± 1.9 | 7.1 ± 1.9 |
| Sleep duration, n (%) | |||
| Normal (6–9 h/day) | 1487 (70.0) | 683 (70.1) | 804 (69.9) |
| Short (<6 h/day)/Long (>9 h/day) | 528 (24.9) | 233 (23.9) | 295 (25.7) |
| Missing | 109 (5.1) | 58 (6.0) | 51 (4.4) |
| Difficulty waking up in the morning, n (%) | |||
| No (easy) | 1241 (58.4) | 605 (62.1) | 636 (55.3) |
| Yes (not easy) | 749 (35.3) | 291 (30.0) | 458 (39.8) |
| Missing | 134 (6.3) | 78 (8.0) | 56 (4.9) |
| Nap during the day, n (%) | |||
| Never/rarely | 687 (32.3) | 272 (27.9) | 415 (36.1) |
| Sometimes/usually | 1328 (62.5) | 639 (65.6) | 689 (59.9) |
| Missing | 109 (5.1) | 63 (6.5) | 46 (4.0) |
| Sleep problems at night, n (%) | |||
| Never/rarely | 621 (29.2) | 329 (33.8) | 292 (25.4) |
| Sometimes/usually | 1387 (65.3) | 577 (59.2) | 810 (70.4) |
| Missing | 116 (5.5) | 68 (7.0) | 48 (4.2) |
| Snoring, n (%) | |||
| No | 1535 (72.3) | 651 (66.8) | 884 (76.9) |
| Yes | 240 (11.3) | 150 (15.4) | 90 (7.8) |
| Missing | 349 (16.4) | 173 (17.8) | 176 (15.3) |
| Daytime tiredness or sleepiness, n (%) | |||
| No | 710 (33.4) | 386 (39.6) | 324 (28.2) |
| Yes | 1187 (55.9) | 474 (48.7) | 713 (62.0) |
| Missing | 227 (10.7) | 114 (11.7) | 113 (9.8) |
| Ever-stop breathing during sleep, n (%) | |||
| No | 1536 (72.3) | 687 (70.5) | 849 (73.8) |
| Yes | 226 (10.6) | 122 (12.5) | 104 (9.0) |
| Missing | 362 (17.0) | 165 (17.0) | 197 (17.1) |
| Sleep Characteristics | Crude Model | Adjusted Model * | ||
|---|---|---|---|---|
| RR [95% CI] | p-Value | RR [95% CI] | p-Value | |
| Sleep duration | ||||
| Normal birth weight | (Reference) | (Reference) | ||
| Low birth weight | 1.03 [0.88–1.20] | 0.750 | 0.96 [0.81–1.14] | 0.630 |
| Difficulty waking up in the morning | ||||
| Normal birthweight | (Reference) | (Reference) | ||
| Low birth weight | 1.20 [1.07–1.34] | 0.002 | 1.17 [1.04–1.33] | 0.012 |
| Nap during the day | ||||
| Normal birth weight | (Reference) | (Reference) | ||
| Low birth weight | 0.98 [0.92–1.05] | 0.624 | 0.99 [0.92–1.06] | 0.752 |
| Sleep problems at night | ||||
| Normal birth weight | (Reference) | (Reference) | ||
| Low birth weight | 1.02 [0.96–1.09] | 0.471 | 1.01 [0.95–1.08] | 0.761 |
| Snoring | ||||
| Normal birth weight | (Reference) | (Reference) | ||
| Low birth weight | 0.85 [0.66–1.10] | 0.221 | 1.01 [0.77–1.31] | 0.986 |
| Daytime tiredness or sleepiness | ||||
| Normal birth weight | (Reference) | (Reference) | ||
| Low birth weight | 1.05 [0.97–1.12] | 0.234 | 1.03 [0.95–1.11] | 0.489 |
| Ever stop breathing during sleep | ||||
| Normal birth weight | (Reference) | (Reference) | ||
| Low birth weight | 0.97 [0.75–1.26] | 0.818 | 1.12 [0.85–1.48] | 0.411 |
| Sleep Characteristics | Male (N = 974) | Female (N = 1150) | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model * | Crude Model | Adjusted Model * | |||||
| RR [95% CI] | p-Value | RR [95% CI] | p-Value | RR [95% CI] | p-Value | RR [95% CI] | p-Value | |
| Sleep duration | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 0.99 [0.77–1.26] | 0.914 | 0.87 [0.65–1.16] | 0.339 | 1.05 [0.86–1.28] | 0.670 | 1.02 [0.82–1.27] | 0.850 |
| Difficulty waking up in the morning | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 1.15 [0.94–1.41] | 0.172 | 1.14 [0.92–1.43] | 0.236 | 1.18 [1.03–1.36] | 0.021 | 1.19 [1.02–1.38] | 0.024 |
| Nap during the day | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 0.99 [0.90–1.09] | 0.839 | 0.98 [0.88–1.08] | 0.664 | 0.99 [0.91–1.10] | 0.974 | 0.99 [0.90–1.10] | 0.909 |
| Sleep problems at night | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 1.02 [0.91–1.13] | 0.762 | 1.01 [0.90–1.14] | 0.815 | 1.01 [0.93–1.08] | 0.928 | 1.01 [0.93–1.09] | 0.826 |
| Snoring | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 0.85 [0.61–1.19] | 0.342 | 0.97 [0.69–1.37] | 0.874 | 0.99 [0.67–1.50] | 0.999 | 1.02 [0.66–1.57] | 0.936 |
| Daytime tiredness or sleepiness | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 1.03 [0.90–1.17] | 0.688 | 1.01 [0.88–1.17] | 0.868 | 1.02 [0.94–1.11] | 0.647 | 1.04 [0.95–1.13] | 0.444 |
| Ever-stop breathing during sleep | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 1.05 [0.74–1.51] | 0.760 | 1.24 [0.85–1.79] | 0.261 | 0.93 [0.64–1.37] | 0.722 | 0.99 [0.65–1.50] | 0.959 |
| Sleep Characteristics | Normal/Low Weight (N = 735) | Overweight/Obese (1075) | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model * | Crude Model | Adjusted Model * | |||||
| RR [95% CI] | p-Value | RR [95% CI] | p-Value | RR [95% CI] | p-Value | RR [95% CI] | p-Value | |
| Sleep duration | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 0.91 [0.70–1.18] | 0.465 | 0.90 [0.69–1.17] | 0.426 | 1.03 [0.82–1.29] | 0.829 | 1.01 [0.80–1.26] | 0.993 |
| Difficulty waking up in the morning | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 1.24 [1.05–1.47] | 0.012 | 1.20 [1.02–1.43] | 0.032 | 1.20 [1.01–1.43] | 0.049 | 1.15 [0.96–1.37] | 0.141 |
| Nap during the day | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 0.99 [0.89–1.10] | 0.816 | 0.98 [0.88–1.10] | 0.751 | 0.97 [0.88–1.07] | 0.581 | 0.99 [0.90–1.09] | 0.830 |
| Sleep night problems | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 0.98 [0.88–1.08] | 0.618 | 0.97 [0.88–1.07] | 0.542 | 1.05 [0.97–1.15] | 0.244 | 1.04 [0.96–1.14] | 0.345 |
| Snoring | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 0.76 [0.41–1.40] | 0.371 | 0.80 [0.43–1.51] | 0.499 | 0.92 [0.68–1.25] | 0.604 | 1.06 [0.80–1.42] | 0.674 |
| Daytime tiredness or sleepiness | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 1.02 [0.91–1.14] | 0.800 | 0.99 [0.88–1.11] | 0.836 | 1.08 [0.98–1.20] | 0.133 | 1.06 [0.96–1.17] | 0.269 |
| Ever-stop breathing during sleep | ||||||||
| Normal birth weight | (Reference) | (Reference) | (Reference) | (Reference) | ||||
| Low birth weight | 1.09 [0.65–1.84] | 0.742 | 1.18 [0.69–2.03] | 0.547 | 1.04 [0.76–1.44] | 0.799 | 1.11 [0.81–1.53] | 0.522 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juber, N.F.; Abdulle, A.; Ahmad, A.; Leinberger-Jabari, A.; Dhaheri, A.S.A.; Al-Maskari, F.; AlAnouti, F.; Al-Houqani, M.; Ali, M.H.; El-Shahawy, O.; et al. Associations between Birth Weight and Adult Sleep Characteristics: A Cross-Sectional Analysis from the UAEHFS. J. Clin. Med. 2023, 12, 5618. https://doi.org/10.3390/jcm12175618
Juber NF, Abdulle A, Ahmad A, Leinberger-Jabari A, Dhaheri ASA, Al-Maskari F, AlAnouti F, Al-Houqani M, Ali MH, El-Shahawy O, et al. Associations between Birth Weight and Adult Sleep Characteristics: A Cross-Sectional Analysis from the UAEHFS. Journal of Clinical Medicine. 2023; 12(17):5618. https://doi.org/10.3390/jcm12175618
Chicago/Turabian StyleJuber, Nirmin F., Abdishakur Abdulle, Amar Ahmad, Andrea Leinberger-Jabari, Ayesha S. Al Dhaheri, Fatma Al-Maskari, Fatme AlAnouti, Mohammad Al-Houqani, Mohammed Hag Ali, Omar El-Shahawy, and et al. 2023. "Associations between Birth Weight and Adult Sleep Characteristics: A Cross-Sectional Analysis from the UAEHFS" Journal of Clinical Medicine 12, no. 17: 5618. https://doi.org/10.3390/jcm12175618
APA StyleJuber, N. F., Abdulle, A., Ahmad, A., Leinberger-Jabari, A., Dhaheri, A. S. A., Al-Maskari, F., AlAnouti, F., Al-Houqani, M., Ali, M. H., El-Shahawy, O., Sherman, S., Shah, S. M., Loney, T., Idaghdour, Y., & Ali, R. (2023). Associations between Birth Weight and Adult Sleep Characteristics: A Cross-Sectional Analysis from the UAEHFS. Journal of Clinical Medicine, 12(17), 5618. https://doi.org/10.3390/jcm12175618