
Changes in Health-Related Quality of Life in Patients with Therapy-Resistant Migraine during Treatment with Erenumab in an Ambulatory Care Setting

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.1.1. MIDAS
2.1.2. PROMIS
2.1.3. EQ-5D-VAS
2.2. Data Collection
2.3. Analysis
3. Results
3.1. Descriptive Statistics on Demographic and Clinical Characteristics of the Study Population
3.2. Characteristics of Treatment
3.3. Monthly Migraine Days
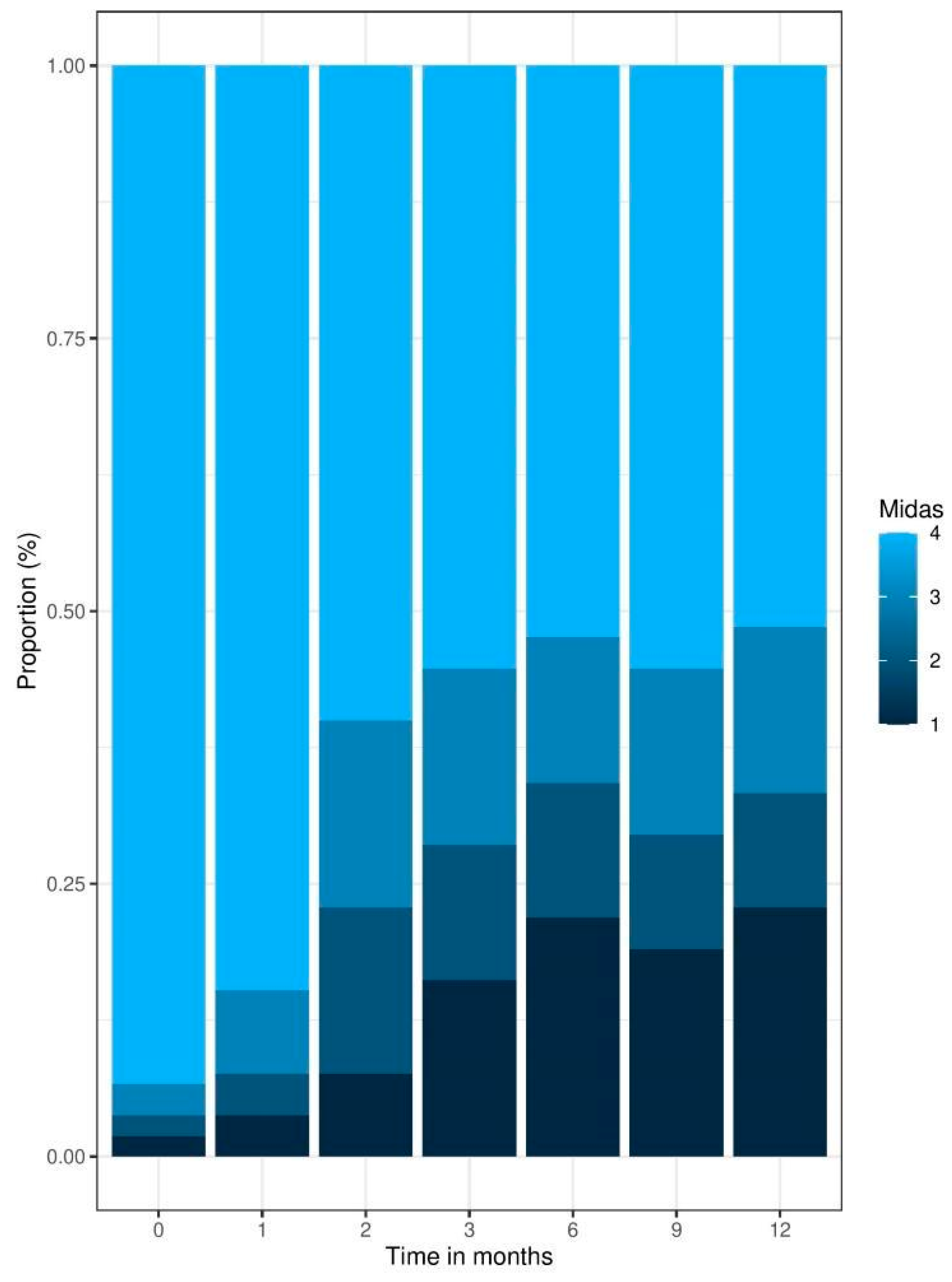
3.4. Patient-Reported Outcomes: MIDAS Score
3.5. Patient-Reported Outcomes: EQ-5D-VAS and PROMIS
3.6. Correlation Analyses
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goadsby, P.J.; Lipton, R.B.; Ferrari, M.D. Migraine—Current Understanding and Treatment. N. Engl. J. Med. 2002, 346, 257–270. [Google Scholar] [CrossRef]
- GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef]
- Buse, D.C.; Lipton, R.B.; Hallström, Y.; Reuter, U.; Tepper, S.J.; Zhang, F.; Sapra, S.; Picard, H.; Mikol, D.D.; Lenz, R.A. Migraine-related disability, impact, and health-related quality of life among patients with episodic migraine receiving preventive treatment with erenumab. Cephalalgia 2018, 38, 1622–1631. [Google Scholar] [CrossRef]
- US Food and Drug Administration. FDA Approves Novel Preventive Treatment for Migraine [Press Release]; US Food and Drug Administration: Beltsville, MD, USA, 2018.
- Gemeinsamer Bundesausschuss (2019). Beschluss des Gemeinsamen Bundesausschusses über eine Änderung der Arzneimittel-Richtlinie (AM-RL): Anlage XII—Beschlüsse über die Nutzenbewertung von Arzneimitteln mit neuen Wirkstoffen nach § 35a SGB V Erenumab. Available online: https://www.g-ba.de/downloads/40-268-3273/2015-07-16_AM-RL-XII_Dulaglutid_2015-02-01-D-154_TrG.pdf (accessed on 3 May 2023).
- Novack, G.D. Real world evidence for pharmaceuticals. Ocul. Surf. 2019, 17, 584–588. [Google Scholar] [CrossRef]
- Baumhauer, J.F. Patient-Reported Outcomes—Are They Living Up to Their Potential? N. Engl. J. Med. 2017, 377, 6–9. [Google Scholar] [CrossRef]
- European Medicines Agency EMA. Integrating Patients’ Views in Clinical Studies of Anticancer Medicines. 2016. Available online: https://www.ema.europa.eu/en/news/integrating-patients-views-clinical-studies-anticancer-medicines (accessed on 3 May 2023).
- Greenhalgh, J.; Dalkin, S.; Gooding, K.; Gibbons, E.; Wright, J.; Meads, D.; Black, N.; Valderas, J.M.; Pawson, R. Health Services and Delivery Research. Functionality and Feedback: A Realist Synthesis of the Collation, Interpretation and Utilisation of Patient-Reported Outcome Measures Data to Improve Patient Care; NIHR Journals Library Copyright © Queen’s Printer and Controller of HMSO: Southampton, UK, 2017. [Google Scholar]
- Black, N. Patient reported outcome measures could help transform healthcare. BMJ 2013, 346, f167. [Google Scholar] [CrossRef]
- Williams, K.; Sansoni, J.; Morris, D.; Grootemaat, P.; Thompson, C. Patient-Reported Outcome Measures: Literature Review; Australian Commission on Safety and Quality in Health Care: Sydney, Australia, 2016.
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J. Clin. Epidemiol. 2010, 63, 1179–1194. [Google Scholar] [CrossRef]
- Deshpande, P.R.; Rajan, S.; Sudeepthi, B.L.; Abdul Nazir, C.P. Patient-reported outcomes: A new era in clinical research. Perspect. Clin. Res. 2011, 2, 137–144. [Google Scholar] [CrossRef]
- Karsten, M.M.; Speiser, D.; Hartmann, C.; Zeuschner, N.; Lippold, K.; Kiver, V.; Gocke, P.; Kirchberger, V.; Blohmer, J.-U. Web-Based Patient-Reported Outcomes Using the International Consortium for Health Outcome Measurement Dataset in a Major German University Hospital: Observational Study. JMIR Cancer 2018, 4, e11373. [Google Scholar] [CrossRef]
- Lavallee, D.C.; Chenok, K.E.; Love, R.M.; Petersen, C.; Holve, E.; Segal, C.D.; Franklin, P.D. Incorporating Patient-Reported Outcomes into Health Care to Engage Patients and Enhance Care. Health Aff. 2016, 35, 575–582. [Google Scholar] [CrossRef]
- Stewart, W.F.; Lipton, R.B.; Dowson, A.J.; Sawyer, J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology 2001, 56 (Suppl. 1), S20–S28. [Google Scholar] [CrossRef]
- Benz, T.; Lehmann, S.; Gantenbein, A.R.; Sandor, P.S.; Stewart, W.F.; Elfering, A.; Aeschlimann, A.G.; Angst, F. Translation, cross-cultural adaptation and reliability of the German version of the migraine disability assessment (MIDAS) questionnaire. Health Qual. Life Outcomes 2018, 16, 42. [Google Scholar] [CrossRef]
- Tang, E.; Ekundayo, O.; Peipert, J.D.; Edwards, N.; Bansal, A.; Richardson, C.; Bartlett, S.J.; Howell, D.; Li, M.; Cella, D.; et al. Validation of the Patient-Reported Outcomes Measurement Information System (PROMIS)-57 and -29 item short forms among kidney transplant recipients. Qual. Life Res. 2019, 28, 815–827. [Google Scholar] [CrossRef]
- Cella, D.; Choi, S.W.; Condon, D.M.; Schalet, B.; Hays, R.D.; Rothrock, N.E.; Yount, S.; Cook, K.F.; Gershon, R.C.; Amtmann, D.; et al. PROMIS(®) Adult Health Profiles: Efficient Short-Form Measures of Seven Health Domains. Value Health 2019, 22, 537–544. [Google Scholar] [CrossRef]
- Craig, B.M.; Reeve, B.B.; Brown, P.M.; Cella, D.; Hays, R.D.; Lipscomb, J.; Pickard, A.S.; Revicki, D.A. US valuation of health outcomes measured using the PROMIS-29. Value Health 2014, 17, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Scheffler, A.; Messel, O.; Wurthmann, S.; Nsaka, M.; Kleinschnitz, C.; Glas, M.; Naegel, S.; Holle, D. Erenumab in highly therapy-refractory migraine patients: First German real-world evidence. J. Headache Pain 2020, 21, 84. [Google Scholar] [CrossRef]
- Raffaelli, B.; Kalantzis, R.; Mecklenburg, J.; Overeem, L.H.; Neeb, L.; Gendolla, A.; Reuter, U. Erenumab in Chronic Migraine Patients Who Previously Failed Five First-Line Oral Prophylactics and OnabotulinumtoxinA: A Dual-Center Retrospective Observational Study. Front. Neurol. 2020, 11, 417. [Google Scholar] [CrossRef] [PubMed]
- Lentsch, S.d.V.; Verhagen, I.E.; Hoek, T.C.v.D.; MaassenVanDenBrink, A.; Terwindt, G.M. Treatment with the monoclonal calcitonin gene-related peptide receptor antibody erenumab: A real-life study. Eur. J. Neurol. 2021, 28, 4194–4203. [Google Scholar] [CrossRef] [PubMed]
- Ashina, M.; Goadsby, P.J.; Reuter, U.; Silberstein, S.; Dodick, D.W.; Xue, F.; Zhang, F.; Paiva da Silva Lima, G.; Cheng, S.; Mikol, D.D. Long-term efficacy and safety of erenumab in migraine prevention: Results from a 5-year, open-label treatment phase of a randomized clinical trial. Eur. J. Neurol. 2021, 28, 1716–1725. [Google Scholar] [CrossRef] [PubMed]
- Driessen, M.T.; Cohen, J.M.; Patterson-Lomba, O.; Thompson, S.F.; Seminerio, M.; Carr, K.; Totev, T.I.; Sun, R.; Yim, E.; Mu, F.; et al. Real-world effectiveness of fremanezumab in migraine patients initiating treatment in the United States: Results from a retrospective chart study. J. Headache Pain 2022, 23, 47. [Google Scholar] [CrossRef] [PubMed]
- Vernieri, F.; Brunelli, N.; Marcosano, M.; Aurilia, C.; Egeo, G.; Lovati, C.; Favoni, V.; Perrotta, A.; Maestrini, I.; Rao, R.; et al. Maintenance of response and predictive factors of 1-year GalcanezumAb treatment in real-life migraine patients in Italy: The multicenter prospective cohort GARLIT study. Eur. J. Neurol. 2023, 30, 224–234. [Google Scholar] [CrossRef]
- Hong, J.B.; Lange, K.S.; Overeem, L.H.; Triller, P.; Raffaelli, B.; Reuter, U. A Scoping Review and Meta-Analysis of Anti-CGRP Monoclonal Antibodies: Predicting Response. Pharmaceuticals 2023, 16, 934. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D. Preventive Migraine Treatment. Continuum 2015, 21, 973–989. [Google Scholar]
- Tassorelli, C.; Diener, H.-C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Ashina, M.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of preventive treatment of chronic migraine in adults. Cephalalgia 2018, 38, 815–832. [Google Scholar] [CrossRef]
- Reuter, U.; Goadsby, P.J.; Lanteri-Minet, M.; Wen, S.; Hours-Zesiger, P.; Ferrari, M.D.; Klatt, J. Efficacy and tolerability of erenumab in patients with episodic migraine in whom two-to-four previous preventive treatments were unsuccessful: A randomised, double-blind, placebo-controlled, phase 3b study. Lancet 2018, 392, 2280–2287. [Google Scholar] [CrossRef] [PubMed]
- Martelletti, P.; Schwedt, T.J.; Lanteri-Minet, M.; Quintana, R.; Carboni, V.; Diener, H.-C.; Ruiz De La Torre, E.; Craven, A.; Rasmussen, A.V.; Evans, S.; et al. My Migraine Voice survey: A global study of disease burden among individuals with migraine for whom preventive treatments have failed. J. Headache Pain 2018, 19, 115. [Google Scholar] [CrossRef] [PubMed]
- Minen, M.T.; De Dhaem, O.B.; Van Diest, A.K.; Powers, S.; Schwedt, T.J.; Lipton, R.; Silbersweig, D. Migraine and its psychiatric comorbidities. J. Neurol. Neurosurg. Psychiatry 2016, 87, 741–749. [Google Scholar] [CrossRef]
- Straube, A.; Stude, P.; Gaul, C.; Schuh, K.; Koch, M. Real-world evidence data on the monoclonal antibody erenumab in migraine prevention: Perspectives of treating physicians in Germany. J. Headache Pain 2021, 22, 133. [Google Scholar] [CrossRef]
- Diener, H.C.; Förderreuther, S.; Gaul, C.; Giese, F.; Hamann, T.; Holle-Lee, D.; Jürgens, T.P.; Kamm, K.; Kraya, T.; Lampl, C.; et al. Prevention of migraine with monoclonal antibodies against CGRP or the CGRP receptor: Addition to the S1 guideline: Therapy of migraine attacks and prevention of migraine. Recommendations of the Germany Society of Neurology and the German Migraine and Headache Society. Neurol. Res. Pract. 2020, 2, 11. [Google Scholar]
- Lipton, R.B.; Tepper, S.J.; Reuter, U.; Silberstein, S.; Stewart, W.F.; Nilsen, J.; Leonardi, D.K.; Desai, P.; Cheng, S.; Mikol, D.D.; et al. Erenumab in chronic migraine: Patient-reported outcomes in a randomized double-blind study. Neurology 2019, 92, e2250–e2260. [Google Scholar] [CrossRef] [PubMed]
- IQWiG. Allgemeine Methoden: Version 6.1/Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen. Gesundheitswesen IfQuWi, 61st ed.; Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen: Cologne, Germany, 2022. [Google Scholar]
- Robblee, J.; Devick, K.L.; Mendez, N.; Potter, J.; Slonaker, J.; Starling, A.J. Real-World Patient Experience With Erenumab for the Preventive Treatment of Migraine. Headache 2020, 60, 2014–2025. [Google Scholar] [CrossRef] [PubMed]
- Gendolla, A.; Rauer, N.; Kraemer, S.; Schwerdtner, I.; Straube, A. Epidemiology, Demographics, Triptan Contraindications, and Prescription Patterns of Patients with Migraine: A German Claims Database Study. Neurol. Ther. 2022, 11, 167–183. [Google Scholar] [CrossRef]
- Roessler, T.; Zschocke, J.; Roehrig, A.; Friedrichs, M.; Friedel, H.; Katsarava, Z. Administrative prevalence and incidence, characteristics and prescription patterns of patients with migraine in Germany: A retrospective claims data analysis. J. Headache Pain 2020, 21, 85. [Google Scholar] [CrossRef] [PubMed]
- Buse, D.C.; Rupnow, M.F.; Lipton, R.B. Assessing and managing all aspects of migraine: Migraine attacks, migraine-related functional impairment, common comorbidities, and quality of life. Mayo Clin. Proc. 2009, 84, 422–435. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 145 1 |
|---|---|
| Age | 52 (45, 58) |
| Female | 84.1 (122) |
| BMI | 24.5 (21.5, 27.3) |
| Type of migraine | |
| Chronic | 78.6 (114) |
| Episodic | 21.4 (31) |
| Relationship status | |
| Married/in a relationship | 71.7 (104) |
| Unmarried/single | 23.4 (34) |
| Divorced/separated | 4.1 (6) |
| Widowed | 0.7 (1) |
| Work status | |
| Working full-time | 42.8 (62) |
| Working part-time | 22.8 (33) |
| Not working by choice | 13.1 (19) |
| Unable to work due to migraine | 11.0 (16) |
| Unable to work due to another condition | 8.3 (12) |
| Seeking employment | 2.0 (2) |
| Comorbidities | |
| None | 37.2 (54) |
| Depression | 24.1 (35) |
| High blood pressure | 20.0 (29) |
| Joint diseases | 17.2 (25) |
| Autoimmune diseases | 9.0 (13) |
| Gastrointestinal diseases | 9.7 (14) |
| Anxiety disorder | 8.3 (12) |
| Cancer | 4.1 (6) |
| Anemia | 4.1 (6) |
| Kidney diseases | 2.8 (4) |
| Liver diseases | 2.1 (3) |
| Diabetes | 2.1 (3) |
| Heart diseases | 2.1 (3) |
| (a) | |||||||
|---|---|---|---|---|---|---|---|
| Time in months | 0, N = 145 1 | 1, N = 145 1 | 2, N = 145 1 | 3, N = 145 1 | 6, N = 145 1 | 9, N = 145 1 | 12, N = 145 1 |
| Dose | |||||||
| 70 mg | 140 (97%) | 114 (79%) | 105 (72%) | 100 (69%) | 99 (68%) | 96 (66%) | 96 (66%) |
| 140 mg | 5 (3.4%) | 31 (21%) | 40 (28%) | 45 (31%) | 46 (32%) | 49 (34%) | 49 (34%) |
| (b) | |||||||
| Characteristic | N = 39 1 | ||||||
| Reason for interruption of treatment | |||||||
| Lack of efficacy | 25 (64%) | ||||||
| Planned therapy break | 4 (10%) | ||||||
| Side effects | 5 (13%) | ||||||
| Other | 5 (13%) | ||||||
| Time in Months | 1, N = 85 1 | 2, N = 85 1 | 3, N = 85 1 | 6, N = 85 1 | 9, N = 85 1 | 12, N = 85 1 |
|---|---|---|---|---|---|---|
| Clinical Relevance ≥ 30% | 27 (32%) | 41 (48%) | 40 (47%) | 36 (42%) | 38 (45%) | 34 (40%) |
| Clinical Relevance ≥ 50% | 17 (20%) | 28 (33%) | 30 (35%) | 26 (31%) | 26 (31%) | 26 (31%) |
| Characteristic | 0, N = 105 1 | 1, N = 105 1 | 2, N = 105 1 | 3, N = 105 1 | 6, N = 105 1 | 9, N = 105 1 | 12, N = 105 1 | Test Statistic | p-Value 2 |
|---|---|---|---|---|---|---|---|---|---|
| EQ5DVAS Score | 56.0 (45.0, 75.0) | 70.0 (54.0, 80.0) | 70.0 (53.0, 81.0) | 74.0 (57.0, 85.0) | 70.0 (50.0, 80.0) | 70.0 (50.0, 84.0) | 69.0 (51.0, 81.0) | 3.3 | 0.003 |
| Score: Anxiety—PROMIS- 29 | 55.8 (48.0, 59.5) | 53.7 (48.0, 57.7) | 51.2 (48.0, 55.8) | 48.0 (40.3, 55.8) | 51.2 (40.3, 55.8) | 51.2 (40.3, 57.7) | 51.2 (40.3, 57.7) | 4.4 | < 0.001 |
| Score: Fatigue—PROMIS- 29 | 57.0 (51.0, 64.6) | 53.1 (48.6, 60.7) | 53.1 (48.6, 58.8) | 51.0 (48.6, 58.8) | 51.0 (48.6, 60.7) | 51.0 (48.6, 60.7) | 53.1 (48.6, 58.8) | 3.5 | 0.002 |
| Score: Ability to Participate in Social Roles and Activities—PROMIS-29 | 42.3 (37.3, 48.1) | 44.2 (42.3, 51.9) | 44.2 (42.3, 51.9) | 48.1 (42.3, 51.9) | 48.1 (42.3, 51.9) | 46.2 (42.3, 51.9) | 46.2 (42.3, 51.9) | 4.7 | < 0.001 |
| Score: Physical Function— PROMIS-29 | 41.8 (36.7, 45.3) | 41.8 (37.9, 45.3) | 43.4 (40.4, 56.9) | 45.3 (39.1, 56.9) | 45.3 (40.4, 56.9) | 45.3 (40.4, 56.9) | 45.3 (40.4, 56.9) | 5.3 | < 0.001 |
| Score: Sleep Disturbance— PROMIS-29 | 52.4 (46.2, 57.9) | 52.4 (46.2, 56.1) | 50.5 (43.8, 57.9) | 50.5 (46.2, 54.3) | 50.5 (43.8, 56.1) | 52.4 (43.8, 57.9) | 50.5 (46.2, 57.9) | 0.90 | 0.5 |
| Score: Depression— PROMIS-29 | 53.9 (49.0, 58.9) | 51.8 (49.0, 57.3) | 51.8 (41.0, 57.3) | 51.8 (49.0, 57.3) | 51.8 (49.0, 55.7) | 51.8 (49.0, 57.3) | 53.9 (49.0, 57.3) | 2.5 | 0.022 |
| Score: Pain Interference— PROMIS-29 | 62.5 (59.9, 66.6) | 57.1 (53.9, 62.5) | 57.1 (53.9, 62.5) | 57.1 (53.9, 61.2) | 55.6 (53.9, 62.5) | 58.5 (53.9, 62.5) | 57.1 (53.9, 62.5) | 6.0 | < 0.001 |
| Score: Pain Intensity— PROMIS-29 | 7.0 (5.0, 7.0) | 4.0 (2.0, 7.0) | 4.0 (3.0, 6.0) | 4.0 (3.0, 6.0) | 4.0 (2.0, 6.0) | 5.0 (2.0, 6.0) | 5.0 (2.0, 7.0) | 5.8 | < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haneke, H.; Sulaiman, S.; Nickel, S.; Raffaelli, B.; Jansen, J.-P.; Kirchberger, V. Changes in Health-Related Quality of Life in Patients with Therapy-Resistant Migraine during Treatment with Erenumab in an Ambulatory Care Setting. J. Clin. Med. 2023, 12, 5619. https://doi.org/10.3390/jcm12175619
Haneke H, Sulaiman S, Nickel S, Raffaelli B, Jansen J-P, Kirchberger V. Changes in Health-Related Quality of Life in Patients with Therapy-Resistant Migraine during Treatment with Erenumab in an Ambulatory Care Setting. Journal of Clinical Medicine. 2023; 12(17):5619. https://doi.org/10.3390/jcm12175619
Chicago/Turabian StyleHaneke, Hannah, Schirin Sulaiman, Sina Nickel, Bianca Raffaelli, Jan-Peter Jansen, and Valerie Kirchberger. 2023. "Changes in Health-Related Quality of Life in Patients with Therapy-Resistant Migraine during Treatment with Erenumab in an Ambulatory Care Setting" Journal of Clinical Medicine 12, no. 17: 5619. https://doi.org/10.3390/jcm12175619
APA StyleHaneke, H., Sulaiman, S., Nickel, S., Raffaelli, B., Jansen, J.-P., & Kirchberger, V. (2023). Changes in Health-Related Quality of Life in Patients with Therapy-Resistant Migraine during Treatment with Erenumab in an Ambulatory Care Setting. Journal of Clinical Medicine, 12(17), 5619. https://doi.org/10.3390/jcm12175619