
Does Music Intervention Improve Anxiety in Dementia Patients? A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
,  , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Strategy and Selection Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment of Included Studies
2.5. Classification of the Music Intervention and Control Groups
2.6. Statistical Analyses
2.7. Subgroup Outcomes
3. Results
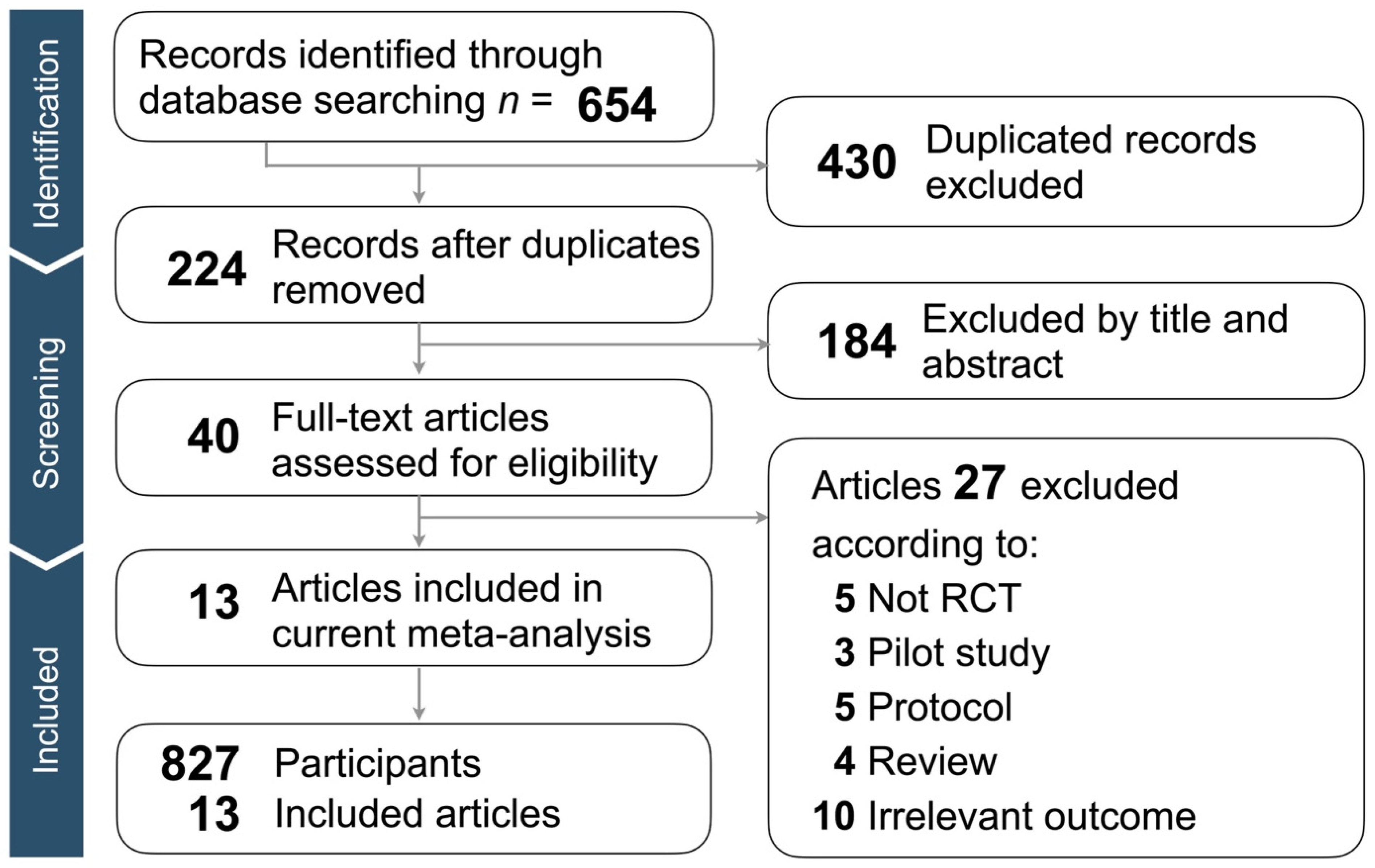
3.1. Identification of Eligible Studies
3.2. Study Characteristics and Patient Population
3.3. Quality Assessment of Included Articles
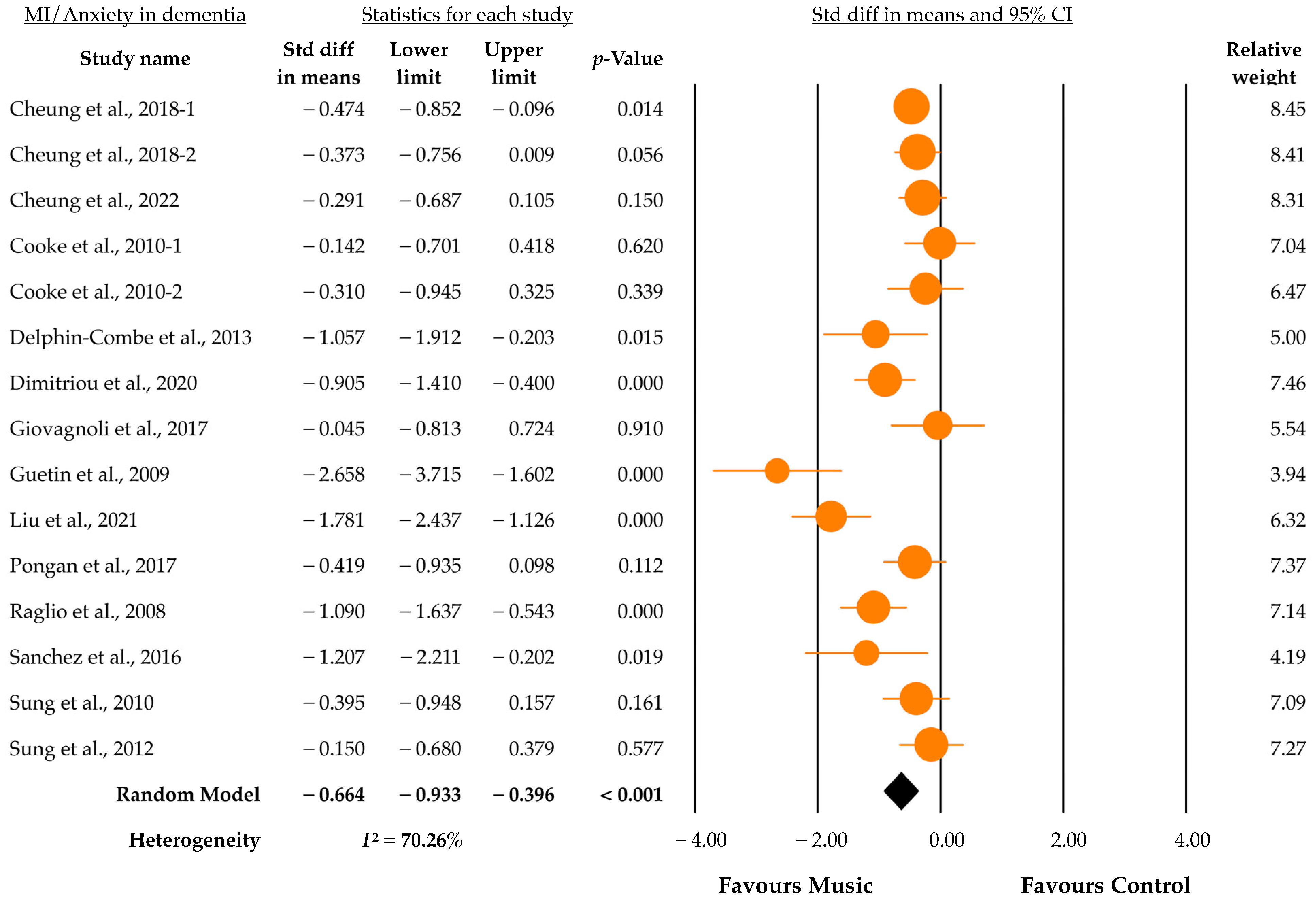
3.4. Outcomes of Music Intervention
3.5. Subgroup Analysis
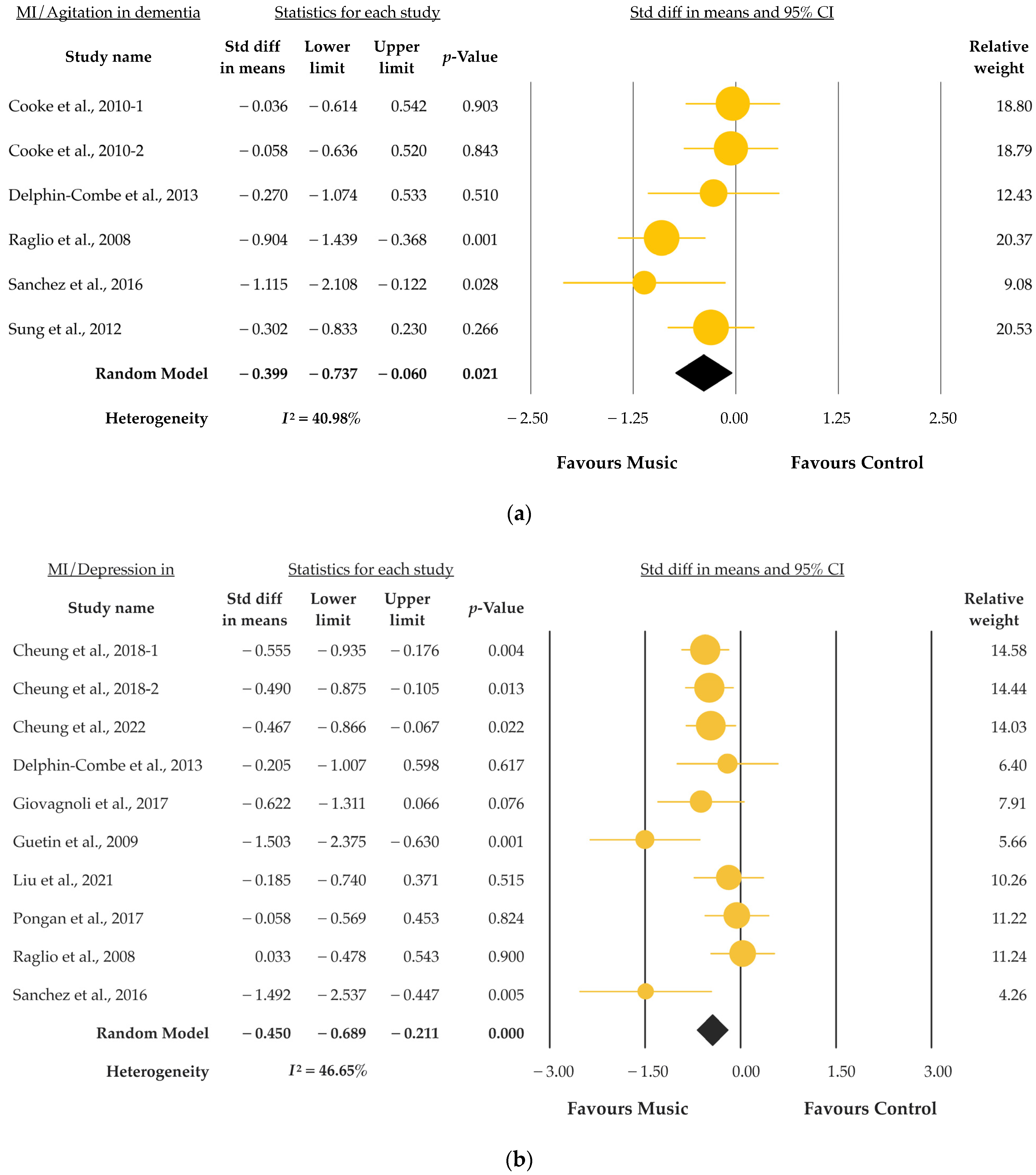
3.6. Secondary Outcome
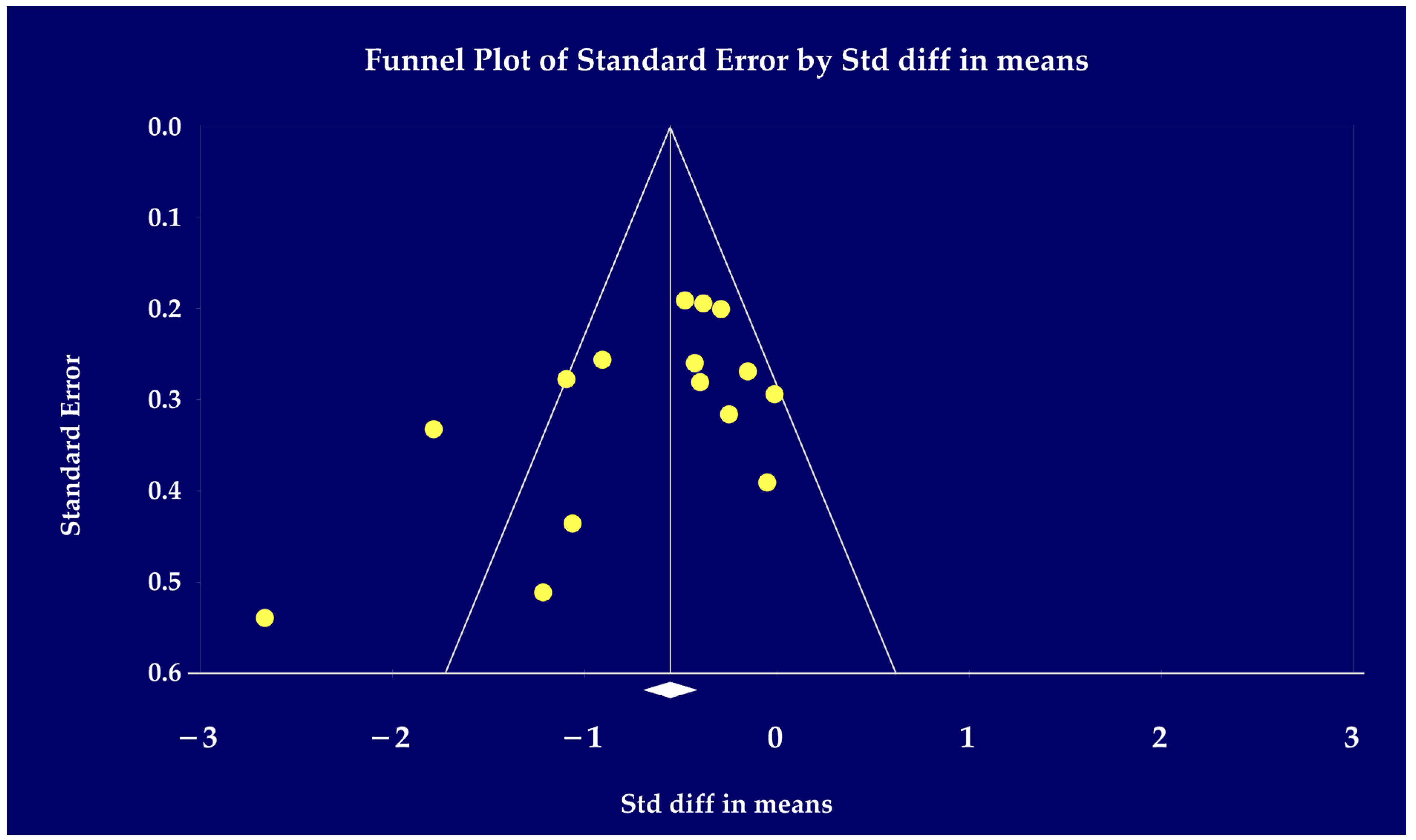
3.7. Evaluation of Publication Bias
4. Discussion
Strength and Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knopman, D.S.; Petersen, R.C. Mild Cognitive Impairment and Mild Dementia: A Clinical Perspective. Mayo Clin. Proc. 2014, 89, 1452–1459. [Google Scholar] [CrossRef] [PubMed]
- Orgeta, V.; Leung, P.; Del-Pino-Casado, R.; Qazi, A.; Orrell, M.; Spector, A.E.; Methley, A.M. Psychological treatments for depression and anxiety in dementia and mild cognitive impairment. Cochrane Database Syst. Rev. 2022, 4, CD009125. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.-U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, L.; McCurry, S.M.; Logsdon, R.; Gibbons, L.; Teri, L. Anxiety and Alzheimer’s Disease. J. Geriatr. Psychiatry Neurol. 2001, 14, 52–58. [Google Scholar] [CrossRef]
- Wortmann, M. Dementia: A global health priority—Highlights from an ADI and World Health Organization report. Alzheimer’s Res. Ther. 2012, 4, 40. [Google Scholar] [CrossRef]
- Finkel, S.I. Behavioral and psychological symptoms of dementia: A current focus for clinicians, researchers, and caregivers. J. Clin. Psychiatry 2001, 62 (Suppl. S21), 3–6. [Google Scholar]
- Chen, C.; Hu, Z.; Jiang, Z.; Zhou, F. Prevalence of anxiety in patients with mild cognitive impairment: A systematic review and meta-analysis. J. Affect. Disord. 2018, 236, 211–221. [Google Scholar] [CrossRef]
- Clark, D.B.; Feske, U.; Masia, C.L.; Spaulding, S.A.; Brown, C.; Mammen, O.; Shear, M.K. Systematic assessment of social phobia in clinical practice. Depress. Anxiety 1997, 6, 47–61. [Google Scholar] [CrossRef]
- Sareen, J.; Cox, B.J.; Afifi, T.O.; De Graaf, R.; Asmundson, G.J.; Ten Have, M.; Stein, M.B. Anxiety disorders and risk for suicidal ideation and suicide attempts: A population-based longitudinal study of adults. Arch. Gen. Psychiatry 2005, 62, 1249–1257. [Google Scholar] [CrossRef]
- John, A.; Patel, U.; Rusted, J.; Richards, M.; Gaysina, D. Affective problems and decline in cognitive state in older adults: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 353–365. [Google Scholar] [CrossRef]
- Ramakers, I.H.G.B.; Visser, P.J.; Aalten, P.; Kester, A.; Jolles, J.; Verhey, F.R.J. Affective symptoms as predictors of alzheimer’s disease in subjects with mild cognitive impairment: A 10-year follow-up study. Psychol. Med. 2010, 40, 1193–1201. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.Y.; Costello, H.; Reeves, S.; Howard, R. The relationship between anxiety and incident agitation in alzheimer’s disease. J. Alzheimer’s Dis. 2020, 78, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ji, M.; Leng, M.; Li, X.; Zhang, X.; Wang, Z. Comparative efficacy of 11 non-pharmacological interventions on depression, anxiety, quality of life, and caregiver burden for informal caregivers of people with dementia: A systematic review and network meta-analysis. Int. J. Nurs. Stud. 2022, 129, 104204. [Google Scholar] [CrossRef]
- Su, K.-P.; Tseng, P.-T.; Lin, P.-Y.; Okubo, R.; Chen, T.-Y.; Chen, Y.-W.; Matsuoka, Y.J. Association of use of omega-3 polyunsaturated fatty acids with changes in severity of anxiety symptoms: A systematic review and meta-analysis. JAMA Netw. Open 2018, 1, e182327. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Fetzner, M.G.; DeBoer, L.B.; Powers, M.B.; Otto, M.W.; Smits, J.A. Let’s get physical: A contemporary review of the anxiolytic effects of exercise for anxiety and its disorders. Depress. Anxiety 2013, 30, 362–373. [Google Scholar] [CrossRef] [PubMed]
- McPherson, T.; Berger, D.; Alagapan, S.; Fröhlich, F. Active and Passive Rhythmic Music Therapy Interventions Differentially Modulate Sympathetic Autonomic Nervous System Activity. J. Music. Ther. 2019, 56, 240–264. [Google Scholar] [CrossRef]
- Zhu, X.; Lazarov, A.; Dolan, S.; Bar-Haim, Y.; Dillon, D.G.; Pizzagalli, D.A.; Schneier, F. Resting state connectivity predictors of symptom change during gaze-contingent music reward therapy of social anxiety disorder. Psychol. Med. 2022, 53, 3115–3123. [Google Scholar] [CrossRef]
- Baird, A.; Samson, S. Music and dementia. Prog. Brain Res. 2015, 217, 207–235. [Google Scholar] [CrossRef]
- Gómez-Gallego, M.; Gómez-Gallego, J.C.; Gallego-Mellado, M.; García-García, J. Comparative efficacy of active group music intervention versus group music listening in alzheimer’s disease. Int. J. Environ. Res. Public Health 2021, 18, 8067. [Google Scholar] [CrossRef]
- Lu, G.; Jia, R.; Liang, D.; Yu, J.; Wu, Z.; Chen, C. Effects of music therapy on anxiety: A meta-analysis of randomized controlled trials. Psychiatry Res. 2021, 304, 114137. [Google Scholar] [CrossRef]
- Pavlicevic, M. Music Therapy in Context: Music, Meaning and Relationship; Jessica Kingsley Publishers: London, UK, 1997. [Google Scholar]
- Thaut, M.H. The future of music in therapy and medicine. Ann. N. Y. Acad. Sci. 2005, 1060, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Van Der Steen, J.T.; Smaling, H.J.; van der Wouden, J.C.; Bruinsma, M.S.; Scholten, R.J.; Vink, A.C. Music-based therapeutic interventions for people with dementia. Cochrane Database Syst. Rev. 2018, 7, CD003477. [Google Scholar] [CrossRef] [PubMed]
- Tsoi, K.K.; Chan, J.Y.; Ng, Y.-M.; Lee, M.M.; Kwok, T.C.; Wong, S.Y. Receptive music therapy is more effective than interactive music therapy to relieve behavioral and psychological symptoms of dementia: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2018, 19, 568–576. [Google Scholar] [CrossRef]
- Chang, Y.-S.; Chu, H.; Yang, C.-Y.; Tsai, J.-C.; Chung, M.-H.; Liao, Y.-M.; Chi, M.-J.; Liu, M.F.; Chou, K.R. The efficacy of music therapy for people with dementia: A meta-analysis of randomised controlled trials. J. Clin. Nurs. 2015, 24, 3425–3440. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2. Hg. V. Cochrane; John Wiley & Sons: Hoboken, NJ, USA, 2022. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Cheung, D.S.K.; Lai, C.K.Y.; Wong, F.K.Y.; Leung, M.C.P. The effects of the music-with-movement intervention on the cognitive functions of people with moderate dementia: A randomized controlled trial. Aging Ment. Health 2018, 22, 306–315. [Google Scholar] [CrossRef]
- Cheung, D.S.K.; Ho, L.Y.W.; Chan, L.C.K.; Kwok, R.K.H.; Lai, C.K.Y. A home-based dyadic music-with-movement intervention for people with dementia and caregivers: A hybrid type 2 cluster-randomized effectiveness-implementation design. Clin. Interv. Aging 2022, 17, 1199–1216. [Google Scholar] [CrossRef]
- Cooke, M.L.; Moyle, W.; Shum, D.H.; Harrison, S.D.; Murfield, J.E. A randomized controlled trial exploring the effect of music on agitated behaviours and anxiety in older people with dementia. Aging Ment. Health 2010, 14, 905–916. [Google Scholar] [CrossRef]
- Delphin-Combe, F.; Rouch, I.; Martin-Gaujard, G.; Relland, S.; Krolak-Salmon, P. Effect of a Non-Pharmacological Intervention, Voix d’or(®), on Behavior Disturbances in Alzheimer Disease and Associated Disorders. Geriatr Psychol Neuropsychiatr Vieil 11 (2013): 323–330. Available online: http://www.jle.com/fr/revues/gpn/e-docs/effet_dune_intervention_non_medicamenteuse_voix_dor_sur_les_troubles_du_comportement_dans_la_maladie_dalzheimer_ou_une_maladie_apparentee_297882/article.phtml. (accessed on 17 August 2023).
- Dimitriou, T.D.; Verykouki, E.; Papatriantafyllou, J.; Konsta, A.; Kazis, D.; Tsolaki, M. Non-pharmacological interventions for the anxiety in patients with dementia. A cross-over randomised controlled trial. Behav. Brain Res. 2020, 390, 112617. [Google Scholar] [CrossRef] [PubMed]
- Giovagnoli, A.R.; Manfredi, V.; Parente, A.; Schifano, L.; Oliveri, S.; Avanzini, G. Cognitive training in Alzheimer’s disease: A controlled randomized study. Neurol. Sci. 2017, 38, 1485–1493. [Google Scholar] [CrossRef] [PubMed]
- Guétin, S.; Portet, F.; Picot, M.C.; Pommié, C.; Messaoudi, M.; Djabelkir, L.; Olsen, A.L.; Cano, M.M.; Lecourt, E.; Touchon, J. Effect of music therapy on anxiety and depression in patients with alzheimer’s type dementia: Randomised, controlled study. Dement. Geriatr. Cogn. Disord. 2009, 28, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.N.; Liou, Y.J.; Wang, W.C.; Su, K.C.; Yeh, H.L.; Lau, C.I.; Hu, L.Y.; Tsai, S.J.; Chen, H.Y. Group music intervention using percussion instruments to reduce anxiety among elderly male veterans with alzheimer disease. Med. Sci. Monit. 2021, 27, e928714. [Google Scholar] [CrossRef] [PubMed]
- Pongan, E.; Tillmann, B.; Leveque, Y.; Trombert, B.; Getenet, J.C.; Auguste, N.; Dauphinot, V.; El Haouari, H.; Navez, M.; Dorey, J.M.; et al. Can musical or painting interventions improve chronic pain, mood, quality of life, and cognition in patients with mild alzheimer’s disease? Evidence from a randomized controlled trial. J. Alzheimers Dis. 2017, 60, 663–677. [Google Scholar] [CrossRef] [PubMed]
- Raglio, A.; Bellelli, G.; Traficante, D.; Gianotti, M.; Ubezio, M.C.; Villani, D.; Trabucchi, M. Efficacy of music therapy in the treatment of behavioral and psychiatric symptoms of dementia. Alzheimer Dis. Assoc. Disord. 2008, 22, 158–162. [Google Scholar] [CrossRef]
- Sánchez, A.; Maseda, A.; Marante-Moar, M.P.; de Labra, C.; Lorenzo-López, L.; Millán-Calenti, J.C. Comparing the effects of multisensory stimulation and individualized music sessions on elderly people with severe dementia: A randomized controlled trial. J. Alzheimers Dis. 2016, 52, 303–315. [Google Scholar] [CrossRef]
- Sung, H.-C.; Chang, A.M.; Lee, W.-L. A preferred music listening intervention to reduce anxiety in older adults with dementia in nursing homes. J. Clin. Nurs. 2010, 19, 1056–1064. [Google Scholar] [CrossRef]
- Sung, H.-C.; Lee, W.-L.; Li, T.-L.; Watson, R. A group music intervention using percussion instruments with familiar music to reduce anxiety and agitation of institutionalized older adults with dementia. Int. J. Geriatr. Psychiatry 2012, 27, 621–627. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Matziorinis, A.M.; Koelsch, S. The promise of music therapy for alzheimer’s disease: A review. Ann. N. Y. Acad. Sci. 2022, 1516, 11–17. [Google Scholar] [CrossRef]
- Calsolaro, V.; Femminella, G.D.; Rogani, S.; Esposito, S.; Franchi, R.; Okoye, C.; Rengo, G.; Monzani, F. Behavioral and psychological symptoms in dementia (bpsd) and the use of antipsychotics. Pharmaceuticals 2021, 14, 246. [Google Scholar] [CrossRef]
- Nguyen, K.T.; Xiao, J.; Chan, D.N.S.; Zhang, M.; Chan, C.W.H. Effects of music intervention on anxiety, depression, and quality of life of cancer patients receiving chemotherapy: A systematic review and meta-analysis. Support. Care Cancer 2022, 30, 5615–5626. [Google Scholar] [CrossRef] [PubMed]
- Coulton, S.; Clift, S.; Skingley, A.; Rodriguez, J. Effectiveness and cost-effectiveness of community singing on mental health-related quality of life of older people: Randomised controlled trial. Br. J. Psychiatry 2015, 207, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Rickson, D.; Jiang, C. The mechanism of music for reducing psychological stress: Music preference as a mediator. Arts Psychother. 2016, 48, 62–68. [Google Scholar] [CrossRef]
- Swaminathan, S.; Schellenberg, E.G. Current emotion research in music psychology. Emot. Rev. 2015, 7, 189–197. [Google Scholar] [CrossRef]
- Watkins, G.R. Music therapy: Proposed physiological mechanisms and clinical implications. Clin. Nurse Spec. 1997, 11, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Karageorghis, C.I.; Bruce, A.C.; Pottratz, S.T.; Stevens, R.C.; Bigliassi, M.; Hamer, M. Psychological and Psychophysiological Effects of Recuperative Music Postexercise; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2018. [Google Scholar]
- Ellis, R.J.; Thayer, J.F. Music and autonomic nervous system (dys) function. Music. Percept. 2010, 27, 317–326. [Google Scholar] [CrossRef]
- Pohjavaara, P.; Telaranta, T.; Väisänen, E. The role of the sympathetic nervous system in anxiety: Is it possible to relieve anxiety with endoscopic sympathetic block? Nord. J. Psychiatry 2003, 57, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, S. Rhythm to Recovery: A Practical Guide to using Rhythmic Music, Voice and Movement for Social and Emotional Development; Jessica Kingsley Publishers: London, UK, 2016. [Google Scholar]
- Speranza, L.; Pulcrano, S.; Perrone-Capano, C.; di Porzio, U.; Volpicelli, F. Music affects functional brain connectivity and is effective in the treatment of neurological disorders. Rev. Neurosci. 2022, 33, 789–801. [Google Scholar] [CrossRef]
- Koelsch, S.; Siebel, W.A. Towards a neural basis of music perception. Trends Cogn. Sci. 2005, 9, 578–584. [Google Scholar] [CrossRef]
- Sittler, M.C.; Worschech, F.; Wilz, G.; Fellgiebel, A.; Wuttke-Linnemann, A. Psychobiological mechanisms underlying the health-beneficial effects of music in people living with dementia: A systematic review of the literature. Physiol. Behav. 2021, 233, 113338. [Google Scholar] [CrossRef]
- Flo, B.K.; Matziorinis, A.M.; Skouras, S.; Sudmann, T.T.; Gold, C.; Koelsch, S. Study protocol for the alzheimer and music therapy study: An rct to compare the efficacy of music therapy and physical activity on brain plasticity, depressive symptoms, and cognitive decline, in a population with and at risk for alzheimer’s disease. PLoS ONE 2022, 17, e0270682. [Google Scholar] [CrossRef] [PubMed]
- Särkämö, T.; Tervaniemi, M.; Huotilainen, M. Music perception and cognition: Development, neural basis, and rehabilitative use of music. Wiley Interdiscip. Rev. Cogn. Sci. 2013, 4, 441–451. [Google Scholar] [CrossRef]
- Du, J.; Shi, P.; Fang, F.; Yu, H. Effect of music intervention on subjective scores, heart rate variability, and prefrontal hemodynamics in patients with chronic pain. Front. Hum. Neurosci. 2022, 16, 1057290. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; He, H.; Duan, M.; Li, S.; Li, C.; Chen, X.; Yao, G.; Chang, X.; Shu, H.; Wang, H.; et al. The effects of music intervention on pallidum-dmn circuit of schizophrenia. BioMed Res. Int. 2020, 2020, 107065. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; He, H.; Duan, M.; Chen, X.; Chang, X.; Lai, Y.; Li, J.; Liu, T.; Luo, C.; Yao, D. The effects of music intervention on functional connectivity strength of the brain in schizophrenia. Neural Plast. 2018, 2018, 2821832. [Google Scholar] [CrossRef]
- Satoh, M.; Yuba, T.; Tabei, K.I.; Okubo, Y.; Kida, H.; Sakuma, H.; Tomimoto, H. Music therapy using singing training improves psychomotor speed in patients with alzheimer’s disease: A neuropsychological and fmri study. Dement. Geriatr. Cogn. Disord. Extra 2015, 5, 296–308. [Google Scholar] [CrossRef]
- Feng, K.; Shen, C.-Y.; Ma, X.-Y.; Chen, G.-F.; Zhang, M.-L.; Xu, B.; Liu, X.-M.; Sun, J.-J.; Zhang, X.-Q.; Liu, P.-Z.; et al. Effects of music therapy on major depressive disorder: A study of prefrontal hemodynamic functions using fnirs. Psychiatry Res. 2019, 275, 86–93. [Google Scholar] [CrossRef]
- Chatterjee, D.; Hegde, S.; Thaut, M. Neural plasticity: The substratum of music-based interventions in neurorehabilitation. NeuroRehabilitation 2021, 48, 155–166. [Google Scholar] [CrossRef]
- Koelsch, S. A coordinate-based meta-analysis of music-evoked emotions. NeuroImage 2020, 223, 117350. [Google Scholar] [CrossRef]
- Bhargav, H.; George, S.; Varambally, S.; Gangadhar, B.N. Yoga and psychiatric disorders: A review of biomarker evidence. Int. Rev. Psychiatry 2021, 33, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Xianjian, C.; Datao, X. Effects of tai chi chuan on the physical and mental health of the elderly: A systematic review. Phys. Act. Health 2021, 5. [Google Scholar] [CrossRef]
- Bai, H.; Xu, S.; Wu, Q.; Xu, S.; Sun, K.; Wu, J.; Xia, X.; Liu, Y.; Zhang, H.; Lu, S. Clinical events associated with acupuncture intervention for the treatment of chronic inflammation associated disorders. Mediat. Inflamm. 2020, 2020, 2675785. [Google Scholar] [CrossRef]
- Okada, K.; Kurita, A.; Takase, B.; Otsuka, T.; Kodani, E.; Kusama, Y.; Atarashi, H.; Mizuno, K. Effects of music therapy on autonomic nervous system activity, incidence of heart failure events, and plasma cytokine and catecholamine levels in elderly patients with cerebrovascular disease and dementia. Int. Heart J. 2009, 50, 95–110. [Google Scholar] [CrossRef]
- Kimura, L.F.; Novaes, L.S.; Picolo, G.; Munhoz, C.D.; Cheung, C.W.; Camarini, R. How environmental enrichment balances out neuroinflammation in chronic pain and comorbid depression and anxiety disorders. Br. J. Pharmacol. 2022, 179, 1640–1660. [Google Scholar] [CrossRef]
- Raglio, A.; Filippi, S.; Bellandi, D.; Stramba-Badiale, M. Global music approach to persons with dementia: Evidence and practice. Clin. Interv. Aging 2014, 1669–1676. [Google Scholar] [CrossRef] [PubMed]
- Raglio, A.; Bellandi, D.; Baiardi, P.; Gianotti, M.; Ubezio, M.C.; Zanacchi, E.; Granieri, E.; Imbriani, M.; Stramba-Badiale, M. Effect of active music therapy and individualized listening to music on dementia: A multicenter randomized controlled trial. J. Am. Geriatr. Soc. 2015, 63, 1534–1539. [Google Scholar] [CrossRef]
- Nair, B.R.; Browne, W.; Marley, J.; Heim, C. Music and dementia. Degener. Neurol. Neuromuscul. Dis. 2013, 47–51. [Google Scholar] [CrossRef]
- Dingle, G.A.; Sharman, L.S.; Bauer, Z.; Beckman, E.; Broughton, M.; Bunzli, E.; Davidson, R.; Draper, G.; Fairley, S.; Farrell, C.; et al. How do music activities affect health and well-being? A scoping review of studies examining psychosocial mechanisms. Front. Psychol. 2021, 12, 713818. [Google Scholar] [CrossRef]
- Yehuda, N. Music and stress. J. Adult Dev. 2011, 18, 85–94. [Google Scholar] [CrossRef]
- Brancatisano, O.; Baird, A.; Thompson, W.F. Why is music therapeutic for neurological disorders? The therapeutic music capacities model. Neurosci. Biobehav. Rev. 2020, 112, 600–615. [Google Scholar] [CrossRef]
- Vink, A.C.; Bruinsma, M.S.; Scholten, R.J. Music therapy for people with dementia. Cochrane Database Syst. Rev. 2003. [Google Scholar]
- Wall, M.; Duffy, A. The effects of music therapy for older people with dementia. Br. J. Nurs. 2010, 19, 108–113. [Google Scholar] [CrossRef]
- Koger, S.M.; Chapin, K.; Brotons, M. Is music therapy an effective intervention for dementia? A meta-analytic review of literature. J. Music. Ther. 1999, 36, 2–15. [Google Scholar] [CrossRef]
- Krout, R.E. Music listening to facilitate relaxation and promote wellness: Integrated aspects of our neurophysiological responses to music. Arts Psychother. 2007, 34, 134–141. [Google Scholar] [CrossRef]
- Garrido, S.; Stevens, C.J.; Chang, E.; Dunne, L.; Perz, J. Music and Dementia: Individual Differences in Response to Personalized Playlists. J. Alzheimer’s Dis. 2018, 64, 933–941. [Google Scholar] [CrossRef]
- Pavlicevic, M. Groups in Music: Strategies from Music Therapy; Jessica Kingsley Publishers: London, UK, 2003. [Google Scholar]
- Carroll, D.; Lefebvre, C. Clinical Improvisation Techniques in Music Therapy: A Guide for Students, Clinicians and Educators; Charles C Thomas Publisher: Springfield, IL, USA, 2013. [Google Scholar]
- Lee, C. The analysis of therapeutic improvisatory music. In Art and Music: Therapy and Research; Routledge: London, UK, 2019; pp. 35–50. [Google Scholar]
- Goodarzi, Z.; Samii, L.; Azeem, F.; Sekhon, R.; Crites, S.; Pringsheim, T.; Smith, E.E.; Ismail, Z.; Holroyd-Leduc, J. Detection of anxiety symptoms in persons with dementia: A systematic review. Alzheimer’s Dementia Diagn. Assess. Dis. Monit. 2019, 11, 340–347. [Google Scholar] [CrossRef]
- Snow, A.L.; Huddleston, C.; Robinson, C.; Kunik, M.E.; Bush, A.L.; Wilson, N.; Calleo, J.; Paukert, A.; Kraus-Schuman, C.; Petersen, N.J.; et al. Psychometric properties of a structured interview guide for the rating for anxiety in dementia. Aging Ment. Health 2012, 16, 592–602. [Google Scholar] [CrossRef]
- Koerner, N.; Antony, M.M.; Dugas, M.J. Limitations of the hamilton anxiety rating scale as a primary outcome measure in randomized, controlled trials of treatments for generalized anxiety disorder. Am. J. Psychiatry 2010, 167, 103–104. [Google Scholar] [CrossRef]
- Cummings, J.L. The neuropsychiatric inventory: Assessing psychopathology in dementia patients. Neurology 1997, 48, 10S–16S. [Google Scholar] [CrossRef]
- Fernández-Blázquez, M.; Ávila-Villanueva, M.; López-Pina, J.; Zea-Sevilla, M.; Frades-Payo, B. Psychometric properties of a new short version of the state-trait anxiety inventory (stai) for the assessment of anxiety in the elderly. Neurol. (Engl. Ed.) 2015, 30, 352–358. [Google Scholar] [CrossRef]
- Brzezińska, A.; Bourke, J.; Rivera-Hernández, R.; Tsolaki, M.; Woźniak, J.; Kaźmierski, J. Depression in dementia or dementia in depression? Systematic review of studies and hypotheses. Curr. Alzheimer Res. 2020, 17, 16–28. [Google Scholar] [CrossRef]
- Livingston, G.; Kelly, L.; Lewis-Holmes, E.; Baio, G.; Morris, S.; Patel, N.; Omar, R.Z.; Katona, C.; Cooper, C. Non-pharmacological interventions for agitation in dementia: Systematic review of randomised controlled trials. Br. J. Psychiatry 2014, 205, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Shamai-Leshem, D.; Lazarov, A.; Pine, D.S.; Bar-Haim, Y. A randomized controlled trial of gaze-contingent music reward therapy for major depressive disorder. Depress. Anxiety 2021, 38, 134–145. [Google Scholar] [CrossRef]
- Erkkilä, J.; Punkanen, M.; Fachner, J.; Ala-Ruona, E.; Pöntiö, I.; Tervaniemi, M.; Vanhala, M.; Gold, C. Individual music therapy for depression: Randomised controlled trial. Br. J. Psychiatry 2011, 199, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Morales, C.; Calero, R.; Moreno-Morales, P.; Pintado, C. Music therapy in the treatment of dementia: A systematic review and meta-analysis. Front. Med. 2020, 7, 160. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.C. Effectiveness of music intervention on cognitive function and neuropsychiatric symptoms in the elderly with dementia: A meta-analysis. Front. Nurs. 2022, 9, 143–153. [Google Scholar] [CrossRef]
- Li, H.-C.; Wang, H.-H.; Lu, C.-Y.; Chen, T.-B.; Lin, Y.-H.; Lee, I. The effect of music therapy on reducing depression in people with dementia: A systematic review and meta-analysis. Geriatr. Nurs. 2019, 40, 510–516. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors and Year | Country | Study Design | Comparison | N | Age, Y Mean (SD) | Dementia Types | Dementia Severity Level | Session Style | Type/Genres/Titles of Music | Equip | Control Type | Control Descriptions | Frequency | Rating Scales |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cheung et al., 2018 [31] | Hong Kong | Multi-RCT | Music-1 Music-2 Social activity | 58 54 53 | 85.71 (6.68) 84.50 (6.82) 85.58 (7.46) | Mixed | Moderate | AMT/PMT | Multiple music | Live/SPK | Active | Social activity | 40 min/twice a week/6 weeks | RAID |
| Cheung et al., 2022 [32] | Hong Kong | Cluster-RCT | Music Control | 55 45 | 79.53 (8.53) | Mixed | Moderate | AMT | Patients Preferences | SPK | Waitlist | Waitlist | 30–45 min/3 times a week/12 weeks | RAID |
| Cooke et al., 2010 [33] | Australia | Crossover | Music Control | 23 23 | 65–95+ | Mixed | Moderate | AMT/PMT | Patients Preferences | Live | Passive | Reading | 40 min/3 times a week/8 weeks | RAID |
| Delphin-Combe et al., 2013 [34] | France | RCT | Music Control | 12 12 | 79.20 (6.90) 79.00 (6.70) | AD | Moderate | AMT | Multiple music | Live | Active | Board games | 30 min/5 times a week/2 weeks | HAM-A |
| Dimitriou et al., 2020 [35] | Greece | Multi-Crossover | Music Exercise | 20 20 | 74.70 (7.17) | Mixed | Mild | PMT | Old songs | SPK | Active | Exercise/Aromatherapy and Massage | 45 min/5 times a week/1 week | NPI |
| Giovagnoli et al., 2017 [36] | Italy | Multi-RCT | Music Cognitive training | 17 17 | 73.92 (7.74) 73.50 (5.96) | Mixed | Moderate | AMT | Improvisation | Live | Active | Cognitive training | 45 min/twice a week/12 weeks | STAI |
| Guétin et al., 2009 [37] | France | RCT | Music Control | 14 12 | 85.20 (6.00) 86.90 (5.20) | AD | Mild | PMT | Multiple music | Live | Passive | Rest and reading | 20 min/once a week/24 weeks | HAM-A |
| Liu et al., 2021 [38] | Taiwan | RCT | Music Control | 25 25 | 86.60 (4.50) 86.90 (5.70) | AD | Mild | AMT | Old songs | Live | Passive | Rest and reading | 60 min/once a week/12 weeks | HAM-A |
| Pongan et al., 2017 [39] | France | RCT | Music Control | 31 28 | 78.80 (7.43) 80.20 (5.71) | AD | Mild | AMT | Patients Preferences | Live | Active | Painting | 120 min/once a week/12 weeks | STAI |
| Raglio et al., 2008 [40] | Italy | RCT | Music Control | 30 29 | 84.40 (5.50) 85.80 (5.40) | Mixed | Moderate | AMT | Improvisation | Live | Active | Educational and entertainment activities | 30 min/10 times/16 weeks | NPI |
| Sánchez et al., 2016 [41] | Spain | RCT | Music Control | 99 | 88.73 (7.36) 88.09 (6.80) | Mixed | Sever | PMT | Patients Preferences | SPK | Active | Multi-Sensory Stimulation | 30 min/twice a week/16 weeks | RAID |
| Sung et al., 2010 [42] | Taiwan | RCT | Music Control | 29 23 | 80.12 (7.55) | Mixed | Moderate | AMT | Old songs | SPK | Passive | Treatment as usual | 30 min/twice a week/6 weeks | RAID |
| Sung et al., 2012 [43] | Taiwan | RCT | Music Control | 27 28 | 81.37 (9.14) 79.50 (8.76) | Mixed | Mild-Moderate | AMT/PMT | Old songs | SPK | Passive | Treatment as usual | 30 min/twice a week/6 weeks | RAID |
| Subgroup | k | Effect Size (SMD) | 95% Confidence Interval | p |
|---|---|---|---|---|
| Dementia type | ||||
| AD | 5 | −1.144 | −1.978 to −0.310 | 0.007 |
| Mix | 10 | −0.481 | −0.681 to −0.281 | <0.001 |
| Therapy type | ||||
| AMT | 6 | −0.798 | −1.256 to −0.340 | 0.001 |
| PMT | 5 | −0.967 | −1.566 to −0.367 | 0.002 |
| AMT + PMT | 4 | −0.231 | −0.484 to 0.022 | 0.073 |
| Music type | ||||
| Improvisation | 2 | −0.603 | −1.625 to 0.418 | 0.247 |
| Multiple music | 4 | −0.976 | −1.664 to −0.287 | 0.005 |
| Old song | 4 | −0.789 | −1.440 to −0.139 | 0.017 |
| Patients’ preferences | 5 | −0.348 | −0.592 to −0.104 | 0.005 |
| Presentation | ||||
| Live music | 8 | −0.651 | −1.026 to −0.276 | 0.001 |
| Pre-record | 7 | −0.694 | −1.112 to −0.276 | 0.001 |
| Rating scale | ||||
| RAID | 8 | −0.355 | −0.527 to −0.183 | <0.001 |
| non-RAID | 7 | −1.075 | −1.593 to −0.557 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ting, B.; Chen, D.T.-L.; Hsu, W.-T.; Liang, C.-S.; Malau, I.A.; Li, W.-C.; Lee, S.-L.; Jingling, L.; Su, K.-P. Does Music Intervention Improve Anxiety in Dementia Patients? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2023, 12, 5497. https://doi.org/10.3390/jcm12175497
Ting B, Chen DT-L, Hsu W-T, Liang C-S, Malau IA, Li W-C, Lee S-L, Jingling L, Su K-P. Does Music Intervention Improve Anxiety in Dementia Patients? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2023; 12(17):5497. https://doi.org/10.3390/jcm12175497
Chicago/Turabian StyleTing, Berne, Daniel Tzu-Li Chen, Wei-Ti Hsu, Chih-Sung Liang, Ikbal Andrian Malau, Wei-Chih Li, Sheau-Ling Lee, Li Jingling, and Kuan-Pin Su. 2023. "Does Music Intervention Improve Anxiety in Dementia Patients? A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 12, no. 17: 5497. https://doi.org/10.3390/jcm12175497
APA StyleTing, B., Chen, D. T.-L., Hsu, W.-T., Liang, C.-S., Malau, I. A., Li, W.-C., Lee, S.-L., Jingling, L., & Su, K.-P. (2023). Does Music Intervention Improve Anxiety in Dementia Patients? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 12(17), 5497. https://doi.org/10.3390/jcm12175497