

Prospective Study of Vonoprazan-Based First-Line Triple Therapy with Amoxicillin and Metronidazole for Clarithromycin-Resistant Helicobacter pylori

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Procedure
2.4. Treatment
2.5. Outcome
2.6. Safety Assessment
2.7. Statistical Analysis
3. Results
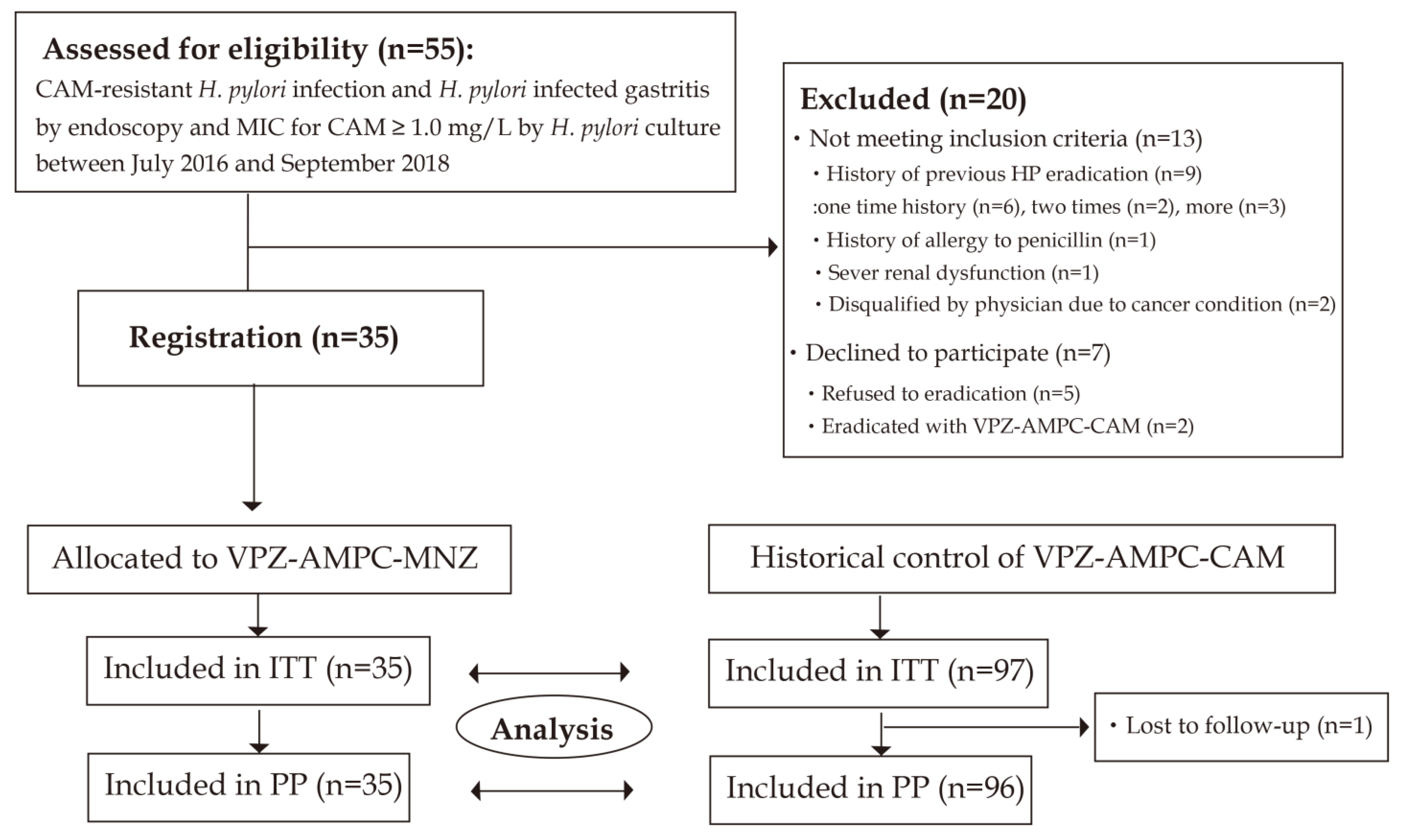
3.1. Study Flow
3.2. Baseline Characteristics
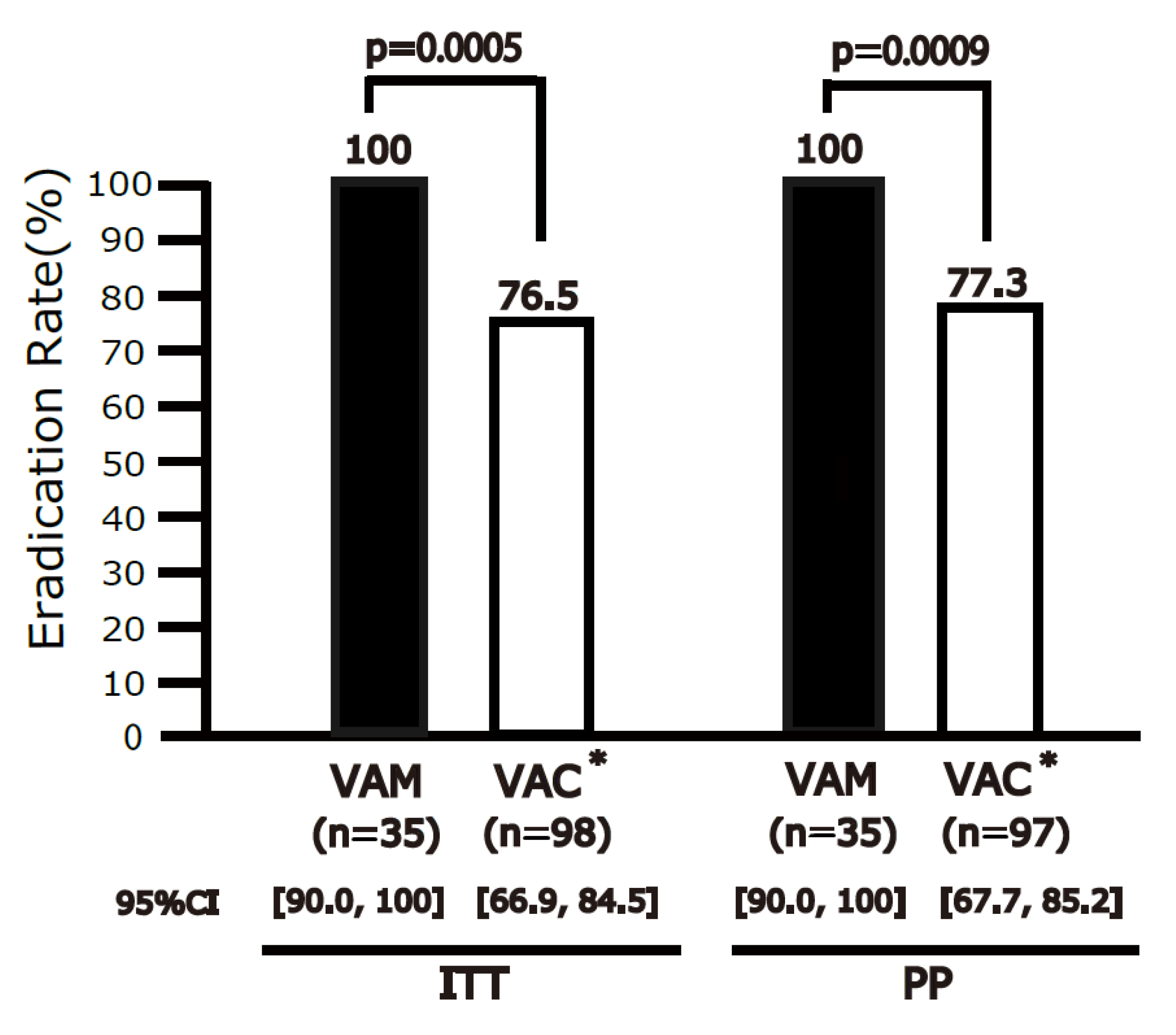
3.3. Efficacy
3.4. Safety and Compliance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, Y.C.; Chiang, T.H.; Chou, C.K.; Tu, Y.K.; Liao, W.C.; Wu, M.S.; Graham, D.Y. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis. Gastroenterology 2016, 150, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Herrero, R.; Park, J.Y.; Forman, D. The fight against gastric cancer-the IARC Working Group report. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Asaka, M.; Kato, M.; Sakamoto, N. Roadmap to eliminate gastric cancer with Helicobacter pylori eradication and consecutive surveillance in Japan. J. Gastroenterol. 2014, 49, 1–8. [Google Scholar] [CrossRef]
- Lee, S.Y. Current progress toward eradicating Helicobacter pylori in East Asian countries: Differences in the 2013 revised guidelines between China, Japan, and South Korea. World J. Gastroenterol. 2014, 20, 1493–1502. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase III, randomised, double-blind study. Gut 2016, 65, 1439–1446. [Google Scholar] [CrossRef]
- Kato, M.; Ota, H.; Okuda, M.; Kikuchi, S.; Satoh, K.; Shimoyama, T.; Suzuki, H.; Handa, O.; Furuta, T.; Mabe, K.; et al. Guidelines for the management of Helicobacter pylori infection in Japan: 2016 Revised Edition. Helicobacter 2019, 24, e12597. [Google Scholar] [CrossRef]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69.e14. [Google Scholar] [CrossRef]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. Correction: ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2018, 113, 1102. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef]
- Dore, M.P.; Leandro, G.; Realdi, G.; Sepulveda, A.R.; Graham, D.Y. Effect of pretreatment antibiotic resistance to metronidazole and clarithromycin on outcome of Helicobacter pylori therapy: A meta-analytical approach. Dig. Dis. Sci. 2000, 45, 68–76. [Google Scholar] [CrossRef]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Lee, Y.C.; Wu, M.S. Rational Helicobacter pylori therapy: Evidence-based medicine rather than medicine-based evidence. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2014, 12, 177–186.e3; discussion e12-3. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Yamagishi, T.; Yagi, K.; Kataoka, M.; Kawakami, K.; Sofuni, A.; Itoi, T.; Sakai, Y.; Moriyasu, F.; Osaka, Y.; et al. Tailored eradication therapy based on fecal Helicobacter pylori clarithromycin sensitivities. J. Gastroenterol. Hepatol. 2008, 23 (Suppl. S2), S171–S174. [Google Scholar] [CrossRef] [PubMed]
- Sue, S.; Kuwashima, H.; Iwata, Y.; Oka, H.; Arima, I.; Fukuchi, T.; Sanga, K.; Inokuchi, Y.; Ishii, Y.; Kanno, M.; et al. The Superiority of Vonoprazan-based First-line Triple Therapy with Clarithromycin: A Prospective Multi-center Cohort Study on Helicobacter pylori Eradication. Intern. Med. 2017, 56, 1277–1285. [Google Scholar] [CrossRef]
- Nishizawa, T.; Maekawa, T.; Watanabe, N.; Harada, N.; Hosoda, Y.; Yoshinaga, M.; Yoshio, T.; Ohta, H.; Inoue, S.; Toyokawa, T.; et al. Clarithromycin Versus Metronidazole as First-line Helicobacter pylori Eradication: A Multicenter, Prospective, Randomized Controlled Study in Japan. J. Clin. Gastroenterol. 2015, 49, 468–471. [Google Scholar] [CrossRef]
- Mabe, K.; Okuda, M.; Kikuchi, S.; Amagai, K.; Yoshimura, R.; Kato, M.; Sakamoto, N.; Asaka, M. Randomized controlled trial: PPI-based triple therapy containing metronidazole versus clarithromycin as first-line treatment for Helicobacter pylori in adolescents and young adults in Japan. J. Infect. Chemother. Off. J. Jpn. Soc. Chemother. 2018, 24, 538–543. [Google Scholar] [CrossRef]
- Graham, D.Y. Vonoprazan Helicobacter pylori eradication therapy: Ethical and interpretation issues. Gut 2017, 66, 384–386. [Google Scholar] [CrossRef]
- Sue, S.; Ogushi, M.; Arima, I.; Kuwashima, H.; Nakao, S.; Naito, M.; Komatsu, K.; Kaneko, H.; Tamura, T.; Sasaki, T.; et al. Vonoprazan- vs proton-pump inhibitor-based first-line 7-day triple therapy for clarithromycin-susceptible Helicobacter pylori: A multicenter, prospective, randomized trial. Helicobacter 2018, 23, e12456. [Google Scholar] [CrossRef]
- Dong, S.Q.; Singh, T.P.; Wei, X.; Yao, H.; Wang, H.L. A Japanese population-based meta-analysis of vonoprazan versus PPI for Helicobacter pylori eradication therapy: Is superiority an illusion? Helicobacter 2017, 22, e12438. [Google Scholar] [CrossRef]
- Sue, S.; Maeda, S. Is a Potassium-Competitive Acid Blocker Truly Superior to Proton Pump Inhibitors in Terms of Helicobacter pylori Eradication? Gut Liver 2021, 15, 799–810. [Google Scholar] [CrossRef]
- Liou, J.M.; Fang, Y.J.; Chen, C.C.; Bair, M.J.; Chang, C.Y.; Lee, Y.C.; Chen, M.-J.; Chen, C.-C.; Tseng, C.-H.; Hsu, Y.-C.; et al. Concomitant, bismuth quadruple, and 14-day triple therapy in the first-line treatment of Helicobacter pylori: A multicentre, open-label, randomised trial. Lancet 2016, 388, 2355–2365. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Suzuki, H.; Matsuzaki, J.; Tsugawa, H.; Fukuhara, S.; Miyoshi, S.; Hirata, K.; Seino, T.; Matsushita, M.; Masaoka, T.; et al. Efficacy of 10-day Sitafloxacin-Containing Third-Line Rescue Therapies for Helicobacter pylori Strains Containing the gyrA Mutation. Helicobacter 2016, 21, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Vaira, D.; Holton, J.; Menegatti, M.; Ricci, C.; Gatta, L.; Geminiani, A.; Miglioli, M. Review article:invasive and non-invasive tests for Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2000, 14 (Suppl. S3), 13–22. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; de la Morena, F.; Abraira, V. Accuracy of monoclonal stool antigen test for the diagnosis of H. pylori infection: A systematic review and meta-analysis. Am. J. Gastroenterol. 2006, 101, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Gotoda, T.; Kusano, C.; Ikehara, H.; Ichijima, R.; Ohyauchi, M.; Ito, H.; Kawamura, M.; Ogata, Y.; Ohtaka, M.; et al. Seven-day vonoprazan and low-dose amoxicillin dual therapy as first-line Helicobacter pylori treatment: A multicentre randomised trial in Japan. Gut 2020, 69, 1019–1026. [Google Scholar] [CrossRef]
- Sue, S.; Shibata, W.; Sasaki, T.; Kaneko, H.; Irie, K.; Kondo, M.; Maeda, S. Randomized trial of vonoprazan-based versus proton-pump inhibitor-based third-line triple therapy with sitafloxacin for Helicobacter pylori. J. Gastroenterol. Hepatol. 2019, 34, 686–692. [Google Scholar] [CrossRef]
- Furuta, T.; Yamade, M.; Higuchi, T.; Takahashi, S.; Ishida, N.; Tani, S.; Tamura, S.; Iwaizumi, M.; Hamaya, Y.; Osawa, S.; et al. Expectations for the Dual Therapy with Vonoprazan and Amoxicillin for the Eradication of H. pylori. J. Clin. Med. 2023, 12, 3110. [Google Scholar] [CrossRef]
- Matsumoto, H.; Shiotani, A.; Katsumata, R.; Fujita, M.; Nakato, R.; Murao, T.; Ishii, M.; Kamada, T.; Haruma, K.; Graham, D.Y. Helicobacter pylori Eradication with Proton Pump Inhibitors or Potassium-Competitive Acid Blockers: The Effect of Clarithromycin Resistance. Dig. Dis. Sci. 2016, 61, 3215–3220. [Google Scholar] [CrossRef]
- Noda, H.; Noguchi, S.; Yoshimine, T.; Goji, S.; Adachi, K.; Tamura, Y.; Izawa, S.; Ebi, M.; Yamamoto, S.; Ogasawara, N.; et al. A Novel Potassium-Competitive Acid Blocker Improves the Efficacy of Clarithromycin-containing 7-day Triple Therapy against Helicobacter pylori. J. Gastrointest. Liver Dis. 2016, 25, 283–288. [Google Scholar] [CrossRef]
- Horie, R.; Handa, O.; Ando, T.; Ose, T.; Murakami, T.; Suzuki, N.; Sendo, R.; Imamoto, E.; Itoh, Y. Helicobacter pylori eradication therapy outcome according to clarithromycin susceptibility testing in Japan. Helicobacter 2020, 25, e12698. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| VPZ-AMPC-MNZ | VPZ-AMPC-CAM * | p | |
|---|---|---|---|
| Age | 62.3 ± 13.7 | 64.8 ± 12.7 | 0.35 |
| Male, % | 71.4 | 45.9 | 0.01 |
| Smoking, % | 20.0 | 14.3 | 0.43 |
| Endoscopic findings, % | |||
| Gastroduodenal ulcer | 5.7 | 4.0 | |
| Gastric cancer | 2.9 | 1.0 | 0.51 |
| Gastritis only | 91.4 | 95.0 | |
| Diagnosis of infection, % | |||
| Culture | 100 | 100 | 1 |
| CAM resistance, % | 100 (35/35) | 100 (98/98) | 1 |
| AMPC resistance, % | 0 (0/35) | 0 (0/98) | 1 |
| MNZ resistance, % | 3.4 (1/29) | N/A | |
| STFX resistance, % | 37.9 (11/29) | N/A |
| Any (Score 1, 2 or 3) | VPZ-AMPC-MNZ | VPZ-AMPC-CAM * | p |
| Diarrhea | 34% | 16% | 0.07 |
| Dysgeusia | 19% | 15% | 0.77 |
| Nausea | 16% | 8% | 0.31 |
| Anorexia | 19% | 10% | 0.33 |
| Abdominal pain | 13% | 10% | 0.73 |
| Heartburn | 16% | 16% | 1 |
| Hives | 0% | 2% | 1 |
| Headache | 3% | 16% | 0.09 |
| Abdominal fullness | 31% | 30% | 1 |
| Belch | 22% | 13% | 0.38 |
| Vomiting | 0% | 0% | 1 |
| General malaise | 16% | 12% | 0.75 |
| Other | 13% | 5% | 0.23 |
| Score 3 | VPZ-AMPC-MNZ | VPZ-AMPC-CAM * | p |
| Diarrhea | 0% | 0% | 1 |
| Dysgeusia | 0% | 8% | 0.16 |
| Nausea | 0% | 0% | 1 |
| Anorexia | 9% | 0% | 0.04 |
| Abdominal pain | 0% | 0% | 1 |
| Heartburn | 0% | 3% | 0.54 |
| Hives | 0% | 3% | 0.54 |
| Headache | 0% | 0% | 1 |
| Abdominal fullness | 9% | 10% | 1 |
| Belch | 6% | 8% | 1 |
| Vomiting | 0% | 0% | 1 |
| General malaise | 3% | 0% | 0.35 |
| Other | 0% | 0% | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sue, S.; Suzuki, Y.; Sasaki, T.; Kaneko, H.; Irie, K.; Komatsu, K.; Maeda, S. Prospective Study of Vonoprazan-Based First-Line Triple Therapy with Amoxicillin and Metronidazole for Clarithromycin-Resistant Helicobacter pylori. J. Clin. Med. 2023, 12, 5443. https://doi.org/10.3390/jcm12175443
Sue S, Suzuki Y, Sasaki T, Kaneko H, Irie K, Komatsu K, Maeda S. Prospective Study of Vonoprazan-Based First-Line Triple Therapy with Amoxicillin and Metronidazole for Clarithromycin-Resistant Helicobacter pylori. Journal of Clinical Medicine. 2023; 12(17):5443. https://doi.org/10.3390/jcm12175443
Chicago/Turabian StyleSue, Soichiro, Yuichi Suzuki, Tomohiko Sasaki, Hiroaki Kaneko, Kuniyasu Irie, Kazuto Komatsu, and Shin Maeda. 2023. "Prospective Study of Vonoprazan-Based First-Line Triple Therapy with Amoxicillin and Metronidazole for Clarithromycin-Resistant Helicobacter pylori" Journal of Clinical Medicine 12, no. 17: 5443. https://doi.org/10.3390/jcm12175443
APA StyleSue, S., Suzuki, Y., Sasaki, T., Kaneko, H., Irie, K., Komatsu, K., & Maeda, S. (2023). Prospective Study of Vonoprazan-Based First-Line Triple Therapy with Amoxicillin and Metronidazole for Clarithromycin-Resistant Helicobacter pylori. Journal of Clinical Medicine, 12(17), 5443. https://doi.org/10.3390/jcm12175443