
Does Exercising with the Use of Virtual Reality during Haemodialysis Have an Impact on Plasma Levels of Interleukin 1β, Interleukin 6, and Interleukin 8?
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
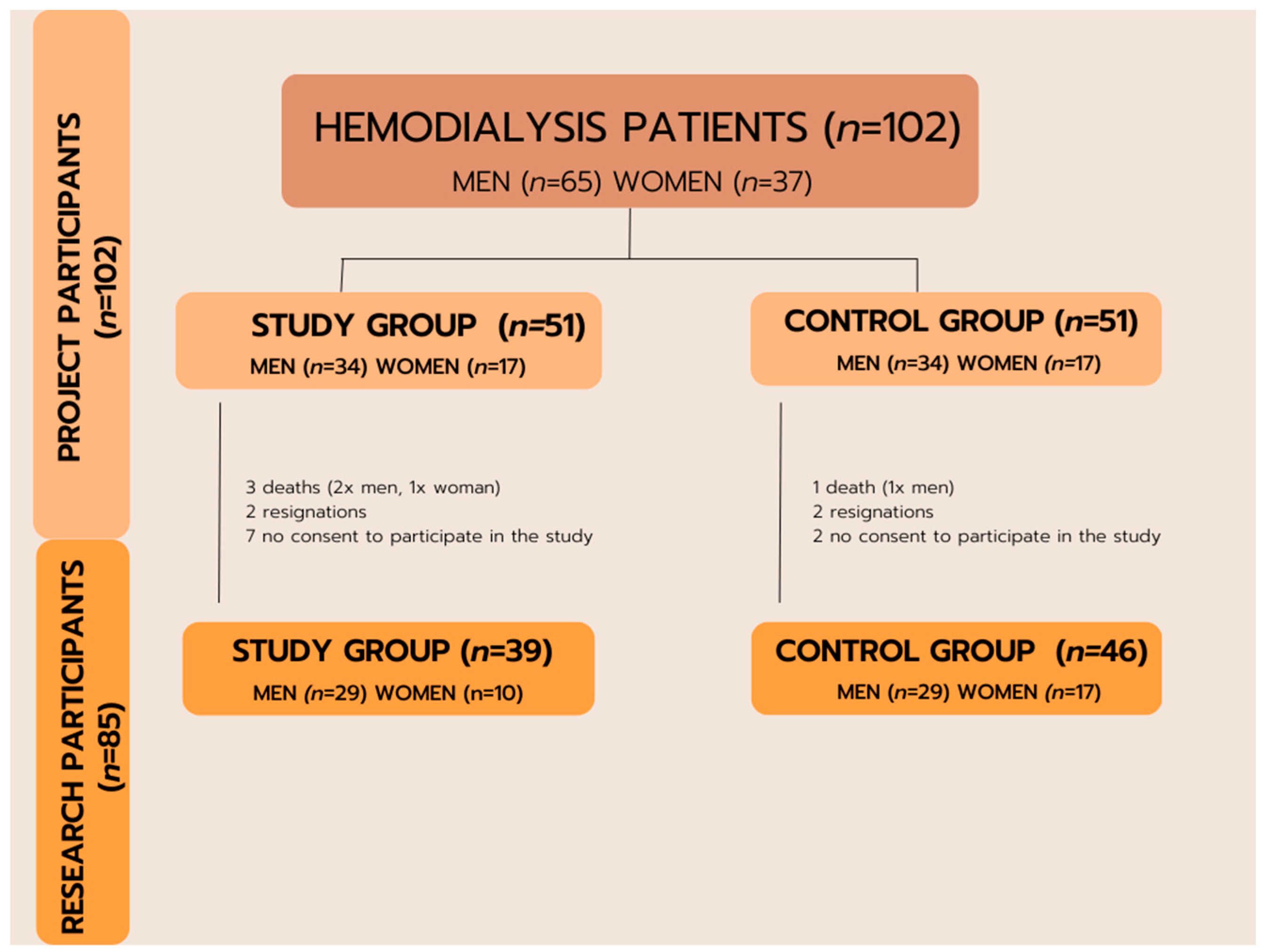
2.1. Study Process
- A base unit (responsible for connecting all components and initiating dedicated software);
- A rehabilitation rotor with a flywheel and manually set load (to perform exercises during dialysis);
- A VR goggles set (for the patient to experience virtual reality);
- A panoramic screen for the patient;
- A control touchscreen (for the operator—a doctor, a nurse, or a physiotherapist);
- A control panel (for the patient), digital joystick, and one button.
2.2. Statistical Analysis
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Susilo, H.; Thaha, M.; Pikir, B.S.; Alsagaff, M.Y.; Suryantoro, S.D.; Wungu, C.D.K.; Pratama, N.R.; Pakpahan, C.; Oceandy, D. The Role of Plasma Interleukin-6 Levels on Atherosclerotic Cardiovascular Disease and Cardiovascular Mortality Risk Scores in Javanese Patients with Chronic Kidney Disease. J. Pers. Med. 2022, 12, 1122. [Google Scholar] [CrossRef]
- Aksoy, A.; Akpınar, T.S.; Yıldız, A.; Akgül, S.U.; Torun, E.S.; Oğuz, F.S.; Yazici, H.; Erten, N.; Tascioglu, C.; Saka, B. Association of inflammation with nutritional status, lean body mass, and physical activity in non-dialysis-dependent chronic kidney disease. Clin. Sci. Nutr. 2019, 1, 16–23. [Google Scholar] [CrossRef]
- Lemos, D.R.; McMurdo, M.; Karaca, G.; Wilflingseder, J.; Leaf, I.A.; Gupta, N.; Miyoshi, T.; Susa, K.; Johnson, B.G.; Soliman, K.; et al. Interleukin-1β Activates a MYC-Dependent Metabolic Switch in Kidney Stromal Cells Necessary for Progressive Tubulointerstitial Fibrosis. J. Am. Soc. Nephrol. 2018, 29, 1690–1705. [Google Scholar] [CrossRef]
- Sims, J.E.; Smith, D.E. The IL-1 family: Regulators of immunity. Nat. Rev. Immunol. 2010, 10, 89–102. [Google Scholar] [CrossRef]
- Akchurin, O.; Patino, E.; Dalal, V.; Meza, K.; Bhatia, D.; Brovender, S.; Zhu, Y.-S.; Cunningham-Rundles, S.; Perelstein, E.; Kumar, J.; et al. Interleukin-6 Contributes to the Development of Anemia in Juvenile CKD. Kidney Int. Rep. 2018, 4, 470–483. [Google Scholar] [CrossRef]
- Buczko, W.; Danysz, A. Kompendium Farmakologii i Farmakoterapii, 6th ed.; Edra Urban & Partner: Wrocław, Poland, 2016; ISBN 978-83-65373-27-4. [Google Scholar]
- Gołąb, J.; Jakóbisiak, M.; Lasek, W.; Stokłosa, T. Immunologia, 7th ed.; Wydawnictwo Naukowe PWN.: Warszawa, Poland, 2017; ISBN 9788301194505. [Google Scholar]
- Mutschler, E.; Malinowska, B.; Droździk, M.; Kocić, I.; Pawlak, D.; Geisslinger, G.; Kroemer, H.K.; Menzel, S.; Ruth, P.; Grotthus, B.; et al. Mutschler—Farmakologia i Toksykologia: Podręcznik; MedPharm: Warszawa, Poland, 2016; ISBN 9788378460374. [Google Scholar]
- March, D.S.; Lai, K.B.; Neal, T.; Graham-Brown, M.P.M.; Highton, P.J.; Churchward, D.R.; Young, H.M.L.; Dungey, M.; Stensel, D.J.; Smith, A.C.; et al. Circulating endotoxin and inflammation: Associations with fitness, physical activity and the effect of a 6-month programme of cycling exercise during haemodialysis. Nephrol. Dial. Transplant. 2022, 25, 366–374. [Google Scholar] [CrossRef]
- Turoń-Skrzypińska, A.; Dutkiewicz, G.; Marchelek-Mysliwiec, M.; Dziedziejko, V.; Safranow, K.; Ryl, A.; Ciechanowski, K.; Rotter, I. Six-Month Physical Activity Versus Sclerostin and Interleukin 6 Concentration in Patients Receiving Renal Replacement Therapy by Hemodialysis—Pilot Study. Preprints 2020, 2020020362. [Google Scholar] [CrossRef]
- Gilowska, I. CXCL8 (interleukin 8)—The key inflammatory mediator in chronic obstructive pulmonary disease? Postepy Hig. Med. Dosw. 2014, 68, 842–850. [Google Scholar] [CrossRef]
- Baggiolini, M. Chemokines in pathology and medicine. J. Intern. Med. 2001, 250, 91–104. [Google Scholar] [CrossRef]
- Gracia-Iguacel, C.; González-Parra, E.; Barril-Cuadrado, G.; Sánchez, R.; Egido, J.; Ortiz-Arduán, A.; Carrero, J.J. Defining protein-energy wasting syndrome in chronic kidney disease: Prevalence and clinical implications. Nefrologia 2014, 34, 507–519. [Google Scholar] [CrossRef]
- Cannon, J.G.; Kluger, M.J. Endogenous pyrogen activity in human plasma after exercise. Science 1983, 220, 617–619. [Google Scholar] [CrossRef]
- De Araújo, C.C.; Silva, J.D.; Samary, C.S.; Guimarães, I.H.; Marques, P.S.; Oliveira, G.P.; Carmo, L.G.R.R.D.; Goldenberg, R.C.; Bakker-Abreu, I.; Diaz, B.L.; et al. Regular and moderate exercise before experimental sepsis reduces the risk of lung and distal organ injury. J. Appl. Physiol. 2012, 112, 1206–1214. [Google Scholar] [CrossRef]
- Koh, K.P.; Fassett, R.G.; Sharman, J.E.; Coombes, J.S.; Williams, A.D. Effect of intradialytic versus home-based aerobic exercise training on physical function and vascular parameters in hemodialysis patients: A randomized pilot study. Am. J. Kidney Dis. 2010, 55, 88–99. [Google Scholar] [CrossRef]
- Rutkowski, S.; Rutkowska, A.; Jastrzębski, D.; Racheniuk, H.; Pawełczyk, W.; Szczegielniak, J. Effect of Virtual Reality-Based Rehabilitation on Physical Fitness in Patients with Chronic Obstructive Pulmonary Disease. J. Hum. Kinet. 2019, 69, 149–157. [Google Scholar] [CrossRef]
- Jastrzębski, D.; Żebrowska, A.; Rutkowski, S.; Rutkowska, A.; Warzecha, J.; Ziaja, B.; Pałka, A.; Czyżewska, B.; Czyżewski, D.; Ziora, D. Pulmonary Rehabilitation with a Stabilometric Platform after Thoracic Surgery: A Preliminary Report. J. Hum. Kinet. 2018, 31, 79–87. [Google Scholar] [CrossRef]
- Fernández-González, P.; Carratalá-Tejada, M.; Monge'a-Pereira, E.; Collado-Vázquez, S.; Sánchez-Herrera Baeza, P.; Cuesta-Gómez, A.; Oña-Simbaña, E.D.; Jardón-Huete, A.; Molina-Rueda, F.; de Quirós, C.B.-B.; et al. Leap motion controlled video game-based therapy for upper limb rehabilitation in patients with Parkinson's disease: A feasibility study. Neuroeng. Rehabil. 2019, 16, 133. [Google Scholar] [CrossRef]
- Maggio, M.G.; De Cola, M.C.; Latella, D.; Maresca, G.; Finocchiaro, C.; La Rosa, G.; Cimino, V.; Sorbera, C.; Bramanti, P.; De Luca, R.; et al. What About the Role of Virtual Reality in Parkinson Disease's Cognitive Rehabilitation? Preliminary Findings from a Randomized Clinical Trial. J. Geriatr. Psychiatry Neurol. 2018, 31, 312–318. [Google Scholar] [CrossRef]
- Shahrbanian, S.; Ma, X.; Aghaei, N.; Korner-Bitensky, N. Use of virtual reality (immersive vs. non immersive) for pain management in children and adults: A systematic review of evidence from randomized controlled trials. Eur. J. Exp. Biol. 2012, 2, 1408–1422. [Google Scholar]
- Messier, J.; Adamovich, S.; Jack, D.; Hening, W.; Sage, J.; Poizner, H. Visuomotor learning in immersive 3D virtual reality in Parkinson’s disease and in aging. Exp. Brain Res. 2007, 179, 457–474. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, C.; Jia, Y.; Shi, C.; Choi, T.; Xiao, Q. Development of a Virtual Reality System for Early Mobilization of Critically Ill Patients. Stud. Health Technol. Inf. 2019, 264, 1805–1806. [Google Scholar] [CrossRef]
- Kamińska, M.S.; Miller, A.; Rotter, I.; Szylińska, A.; Grochans, E. The effectiveness of virtual reality training in reducing the risk of falls among elderly people. Clin. Interv. Aging 2018, 13, 2329–2338. [Google Scholar] [CrossRef]
- Segura-Ortí, E.; García-Testal, A. Intradialytic virtual reality exercise: Increasing physical activity through technology. Semin. Dial. 2019, 32, 331–335. [Google Scholar] [CrossRef]
- Cho, H.; Sohng, K.Y. The effect of a virtual reality exercise program on physical fitness, body composition, and fatigue in hemodialysis patients. J. Phys. Ther. Sci. 2014, 26, 1661–1665. [Google Scholar] [CrossRef]
- Heiwe, S.; Jacobson, S.H. Exercise training for adults with chronic kidney disease. Cochrane Database Syst. Rev. 2011, 10, CD003236. [Google Scholar] [CrossRef]
- Anding, K.; Bär, T.; Trojniak-Hennig, J.; Kuchinke, S.; Krause, R.; Rost, J.M.; Halle, M. A structured exercise programme during haemodialysis for patients with chronic kidney disease: Clinical benefit and long-term adherence. BMJ Open 2015, 5, e008709. [Google Scholar] [CrossRef]
- Manfredini, F.; Mallamaci, F.; D'Arrigo, G.; Baggetta, R.; Bolignano, D.; Torino, C.; Lamberti, N.; Bertoli, S.; Ciurlino, D.; Rocca-Rey, L.; et al. Exercise in Patients on Dialysis: A Multicenter, Randomized Clinical Trial. J. Am. Soc. Nephrol. 2017, 28, 1259–1268. [Google Scholar] [CrossRef]
- Baggetta, R.; D’Arrigo, G.; Torino, C.; ElHafeez, S.A.; Manfredini, F.; Mallamaci, F.; Zoccali, C.; Tripepi, G. Effect of a home based, low intensity, physical exercise program in older adultsdialysis patients: A secondary analysis of the EXCITE trial. BMC Geriatr. 2018, 18, 248. [Google Scholar] [CrossRef]
- Weber-Nowakowska, K.; Gębska, M.; Myślak, M.; Żyżniewska-Banaszak, E.; Stecko, M. Rola aktywności fizycznej w leczeniu pacjentów z przewlekłą chorobą nerek. Pomeranian J. Life Sci. 2017, 63, 27–30. [Google Scholar] [CrossRef][Green Version]
- Hornik, B.; Janusz-Jenczeń, M.; Włodarczyk, I. Przestrzeganie zaleceń aktywności fizycznej przez chorych hemodializowanych. In Profilaktyka i Edukacja Zdrowotna; Dybińska, E., Szpringer, M., Asienkiewicz, R., Eds.; Wydawnictwo Naukowe Neurocentrum: Lublin, Poland, 2017; pp. 109–122. [Google Scholar]
- Chermut, T.R.; Fonseca, L.; Figueiredo, N.; de Oliveira Leal, V.; Borges, N.A.; Cardozo, L.F.; Leite, P.E.C.; Alvarenga, L.; Regis, B.; Delgado, A.; et al. Effects of propolis on inflammation markers in patients undergoing hemodialysis: A randomized, double-blind controlled clinical trial. Complement Ther. Clin. Pr. 2023, 51, 101732. [Google Scholar] [CrossRef]
- Baião, V.M.; Cunha, V.A.; Duarte, M.P.; Andrade, F.P.; Ferreira, A.P.; Nóbrega, O.T.; Viana, J.L.; Ribeiro, H.S. Effects of Exercise on Inflammatory Markers in Individuals with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Metabolites 2023, 13, 795. [Google Scholar] [CrossRef]
- Castaneda, C.; Gordon, P.L.; Parker, R.C.; Uhlin, K.L.; Roubenoff, R.; Levey, A.S. Resistance training to reduce the malnutrition-inflammation complex syndrome of chronic kidney disease. Am. J. Kidney Dis. 2004, 43, 607–616. [Google Scholar] [CrossRef]
- Figueiredo, P.H.S.; Lima, M.M.O.; Costa, H.S.; Martins, J.B.; Flecha, O.D.; Gonçalves, P.F.; Alves, F.L.; Rodrigues, V.G.B.; Maciel, E.H.B.; Mendonça, V.A.; et al. Effects of the inspiratory muscle training and aerobic training on respiratory and functional parameters, inflammatory biomarkers, redox status and quality of life in hemodialysis patients: A randomized clinical trial. PLoS ONE 2018, 13, e0200727. [Google Scholar] [CrossRef]
- Cruz, L.G.D.; Zanetti, H.R.; Andaki, A.C.R.; Mota, G.R.D.; Barbosa Neto, O.; Mendes, E.L. Intradialytic aerobic training improves inflammatory markers in patients with chronic kidney disease: A randomized clinical trial. Mot. Rev. Educ. Física 2018, 24, e017517. [Google Scholar] [CrossRef][Green Version]
- Gołȩbiowski, T.; Kusztal, M.; Weyde, W.; Dziubek, W.; Woźniewski, M.; Madziarska, K.; Krajewska, M.; Letachowicz, K.; Strempska, B.; Klinger, M. A Program of physical rehabilitation during hemodialysis sessions improves the fitness of dialysis patients. Kidney Blood Press Res. 2012, 35, 290–296. [Google Scholar] [CrossRef]
- Tartibian, B.; FitzGerald, L.Z.; Azadpour, N.; Maleki, B.H. A randomized controlled study examining the effect of exercise on inflammatory cytokine levels in post-menopausal women. Post Reprod. Health 2015, 21, 9–15. [Google Scholar] [CrossRef]
- Ding, Y.; Xu, X. Effects of regular exercise on inflammasome activation-related inflammatory cytokine levels in older adults: A systematic review and meta-analysis. J. Sports Sci. 2021, 39, 2338–2352. [Google Scholar] [CrossRef]
- Della Guardia, L.; Codella, R. Exercise tolls the bell for key mediators of low-grade inflammation in dysmetabolic conditions. Cytokine Growth Factor Rev. 2021, 62, 83–93. [Google Scholar] [CrossRef]
- Saxena, A.; Fletcher, E.; Larsen, B.; Baliga, M.S.; Durstine, J.L.; Fayad, R. Effect of exercise on chemically-induced colitis in adiponectin deficient mice. J. Inflamm. 2012, 9, 30. [Google Scholar] [CrossRef]
- Zajaczkowska, M.M.; Bienias, B. Aktualny stan wiedzy na temat patogenezy, diagnostyki i leczenia przewlekłej choroby nerek. Med. OgÓLna I Nauk. O Zdrowiu 2013, 19, 1–7. [Google Scholar]
- Stenvinkel, P.; Ketteler, M.; Johnson, R.J.; Lindholm, B.; Pecoits-Filho, R.; Riella, M.; Heimbürger, O.; Cederholm, T.; Girndt, M. IL-10, IL-6, and TNF-alpha: Central factors in the altered cytokine network of uremia--the good, the bad, and the ugly. Kidney Int. 2005, 67, 1216–1233. [Google Scholar] [CrossRef]
- Cheema, B.S.B.; Abas, H.; Smith, B.C.F.; O'Sullivan, A.J.; Chan, M.; Patwardhan, A.; Kelly, J.; Gillin, A.; Pang, G.; Lloyd, B.; et al. Effect of resistance training during hemodialysis on circulating cytokines: A randomized controlled trial. Eur. J. Appl. Physiol. 2011, 111, 1437–1445. [Google Scholar] [CrossRef]
- Moraes, C.; Marinho, S.M.; da Nobrega, A.C.; Oliveira Bessa, B.; Jacobson, L.V.; Stockler-Pinto, M.B.; da Silva, W.S.; Mafra, D. Resistance exercise: A strategy to attenuate inflammation and protein-energy wasting in hemodialysis patients? Int. Urol. Nephrol. 2014, 46, 1655–1662. [Google Scholar] [CrossRef]
- Dungey, M.; Young, H.M.L.; Churchward, D.R.; Burton, J.O.; Smith, A.C.; Bishop, N.C. Regular exercise during haemodialysis promotes an anti-inflammatory leucocyte profile. Clin. Kidney J. 2017, 10, 813–821. [Google Scholar] [CrossRef]
- Liao, M.T.; Liu, W.C.; Lin, F.H.; Huang, C.F.; Chen, S.Y.; Liu, C.C.; Lin, S.-H.; Lu, K.-C.; Wu, C.-C. Intradialytic aerobic cycling exercise alleviates inflammation and improves endothelial progenitor cell count and bone density in hemodialysis patients. Medicine 2016, 95, e4134. [Google Scholar] [CrossRef]
- Meléndez-Oliva, E.; Sánchez-Vera Gómez-Trelles, I.; Segura-Orti, E.; Pérez-Domínguez, B.; García-Maset, R.; García-Testal, A.; Lavandera-Díaz, J.L. Effect of an aerobic and strength exercise combined program on oxidative stress and inflammatory biomarkers in patients undergoing hemodialysis: A single blind randomized controlled trial. Int. Urol. Nephrol. 2022, 54, 2393–2405. [Google Scholar] [CrossRef]
- Sugawara, K.; Takahashi, H.; Kasai, C.; Kiyokawa, N.; Watanabe, T.; Fujii, S.; Kashiwagura, T.; Honma, M.; Satake, M.; Shioya, T. Effects of nutritional supplementation combined with low-intensity exercise in malnourished patients with COPD. Respir. Med. 2010, 104, 1883–1889. [Google Scholar] [CrossRef]
- Dorneles, G.P.; Haddad, D.O.; Fagundes, V.O.; Vargas, B.K.; Kloecker, A.; Romão, P.R.; Peres, A. High intensity interval exercise decreases IL-8 and enhances the immunomodulatory cytokine interleukin-10 in lean and overweight-obese individuals. Cytokine 2016, 77, 1–9. [Google Scholar] [CrossRef]
- Nielsen, A.R.; Pedersen, B.K. The biological roles of exercise-induced cytokines: IL-6, IL-8, and IL-15. Appl. Physiol. Nutr. Metab. 2007, 32, 833–839. [Google Scholar] [CrossRef]
- Dogra, S.; Wolf, M.; Jeffrey, M.P.; Foley, R.C.A.; Logan-Sprenger, H.; Jones-Taggart, H.; Green-Johnson, J.M. Disrupting prolonged sitting reduces IL-8 and lower leg swell in active young adults. BMC Sports Sci. Med. Rehabil. 2019, 11, 23. [Google Scholar] [CrossRef]
- Hirose, L.; Nosaka, K.; Newton, M.; Laveder, A.; Kano, M.; Peake, J.; Suzuki, K. Changes in inflammatory mediators following eccentric exercise of the elbow flexors. Exerc. Immunol. Rev. 2004, 10, 75–90. [Google Scholar]
- Peake, J.; Nosaka, K.; Suzuki, K. Characterization of inflammatory responses to eccentric exercise in humans. Exerc. Immunol. Rev. 2005, 11, 64–85. [Google Scholar]
- Petersen, A.M.W.; Pedersen, B.K. Antiinflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef]
- Suzuki, K.; Nakaji, S.; Yamada, M.; Totsuka, M.; Sato, K.; Sugawara, K. Systemic inflammatory response to exhaustive exercise. Cytokine kinetics. Exerc. Immunol. Rev. 2002, 8, 46–48. [Google Scholar]
- Hu, L.; Klein, J.D.; Hassounah, F.; Cai, H.; Zhang, C.; Xu, P.; Wang, X.H. Low-frequency electrical stimulation attenuates muscle atrophy in CKD-a potential treatment strategy. J. Am. Soc. Nephrol. 2015, 26, 626–635. [Google Scholar] [CrossRef]
- Jiao, B.; An, C.; Du, H.; Tran, M.; Wang, P.; Zhou, D.; Wang, Y. STAT6 Deficiency Attenuates Myeloid Fibroblast Activation and Macrophage Polarization in Experimental Folic Acid Nephropathy. Cells 2021, 10, 3057. [Google Scholar] [CrossRef]
- An, C.; Jiao, B.; Du, H.; Tran, M.; Song, B.; Wang, P.; Zhou, D.; Wang, Y. Jumonji domain-containing protein-3 (JMJD3) promotes myeloid fibroblast activation and macrophage polarization in kidney fibrosis. Br. J. Pharmacol. 2023, 180, 2250–2265. [Google Scholar] [CrossRef]
- Dungey, M.; Hull, K.L.; Smith, A.C.; Burton, J.O.; Bishop, N.C. Inflammatory Factors and Exercise in Chronic Kidney Disease. Int. J. Endocrinol. 2013, 2013, 569831. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (n = 39) | Control Group (n = 46) | p | ||||
|---|---|---|---|---|---|---|
| Age, mean ± SD; Me | 57.56 ± 17.61; 63.0 | 62.63 ± 15.47; 64.0 | 0.266 * | |||
| BMI, mean ± SD; Me | 26.49 ± 3.76; 25.5 | 27.00 ± 4.69; 26.8 | 0.582 | |||
| Sex, n (%) | Males | 29 | 74.36% | 29 | 63.04% | 0.264 |
| Females | 10 | 25.64% | 17 | 36.96% | ||
| Professional activity, n (%) | no | 26 | 72.22% | 40 | 88.89% | 0.103^ |
| Yes | 10 | 27.78% | 5 | 11.11% | ||
| Professional activity before the start of haemodialysis, n (%) | no | 10 | 27.78% | 21 | 46.67% | 0.082 |
| Yes | 26 | 72.22% | 24 | 53.33% | ||
| Type of job, n (%) | blue-collar | 18 | 47.37% | 18 | 54.55% | 0.829 |
| white-collar | 11 | 28.95% | 7 | 21.21% | ||
| no job | 9 | 23.68% | 8 | 24.24% | ||
| Currently smoking cigarettes, n (%) | No | 30 | 76.92% | 35 | 76.09% | 0.868 |
| Yes | 9 | 23.08% | 11 | 23.91% | ||
| Number of cigarettes per day, mean ± SD; Me | 14.44 ± 6.13; 15.0 | 14.09 ± 7.41; 10.0 | 0.676 * | |||
| How many years ago quit smoking, mean ± SD; Me | 9.71 ± 10.95; 5.0 | 16.67 ± 16.17; 13.0 | 0.520 * | |||
| Number of HD per week, mean ± SD; Me | 2.95 ± 0.23; 3.0 | 2.98 ± 0.15; 3.0 | 0.805 * | |||
| Duration of dialysis [min], mean ± SD; Me | 223.85 ± 20.47; 240.0 | 216.52 ± 28.92; 210.0 | 0.110 * | |||
| Concomitant diseases | ||||||
| Diabetes, n (%) | 5 | 14.71% | 13 | 28.89% | 0.224 ^ | |
| Arterial hypertension, n (%) | 25 | 73.53% | 32 | 71.11% | 0.812 | |
| Epilepsy, n (%) | 4 | 12% | 3 | 7% | 0.697 | |
| Ophthalmic, n (%) | 8 | 24% | 15 | 33% | 0.484 | |
| Neurological, n (%) | 2 | 6% | 3 | 6.52% | 0.745 ^ | |
| Treatment with another renal replacement therapy, n (%) | 7 | 20.59% | 8 | 17.78% | 0.979 | |
| Interleukin | Sensitivity | Assay Range |
|---|---|---|
| 1β | 0.22 pg/mL | 0.3–7500 pg/mL |
| 6 | 1.0 pg/mL | 1.5–300 pg/mL |
| 8 | 0.9 ng/L | 1–350 ng/L |
| Study Group (n = 39) | Control Group (n = 46) | p | |||||
|---|---|---|---|---|---|---|---|
| Mean | Me | SD | Mean | Me | SD | ||
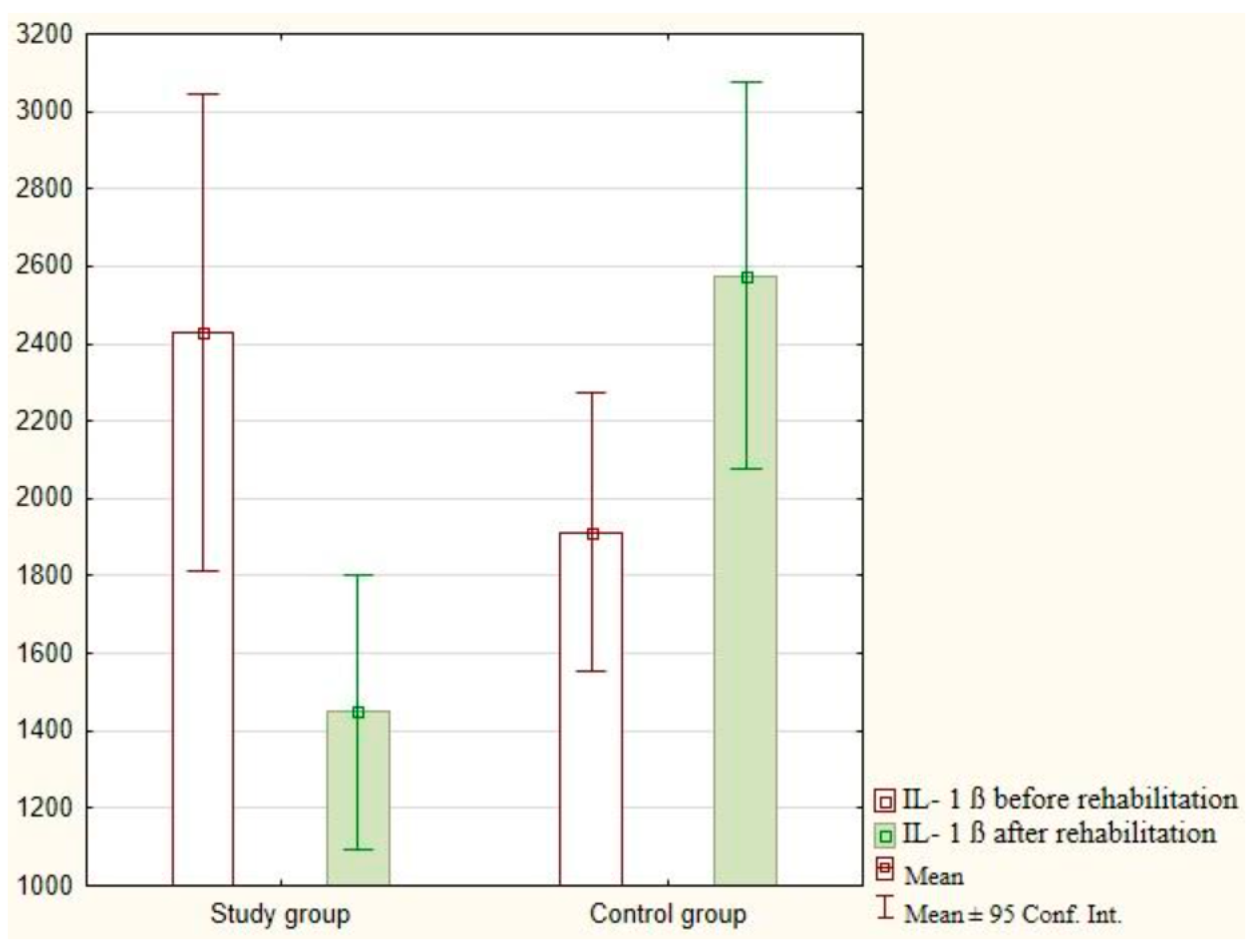
| IL-1β—measurement 1 | 2428.99 | 1831.90 | 1794.83 | 1913.22 | 1348.35 | 1212.25 | 0.360 |
| IL-1β—measurement 2 | 1448.34 | 1164.70 | 997.75 | 2575.40 | 1899.90 | 1658.73 | <0.001 * |
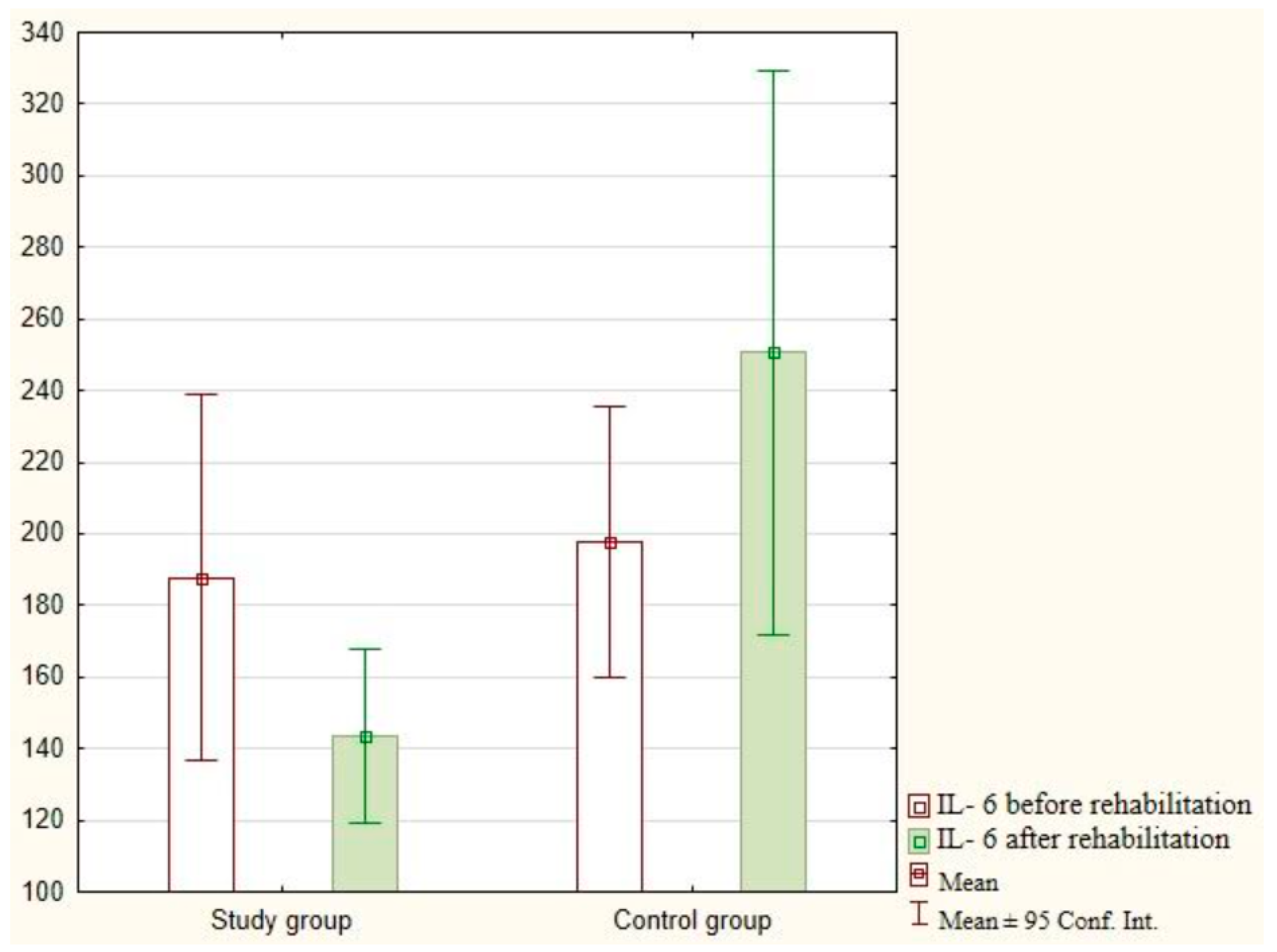
| IL-6 measurement 1 | 187.83 | 143.46 | 146.86 | 197.53 | 150.44 | 127.66 | 0.353 |
| IL-6 measurement 2 | 143.49 | 131.17 | 65.09 | 250.54 | 159.75 | 255.98 | 0.040 * |
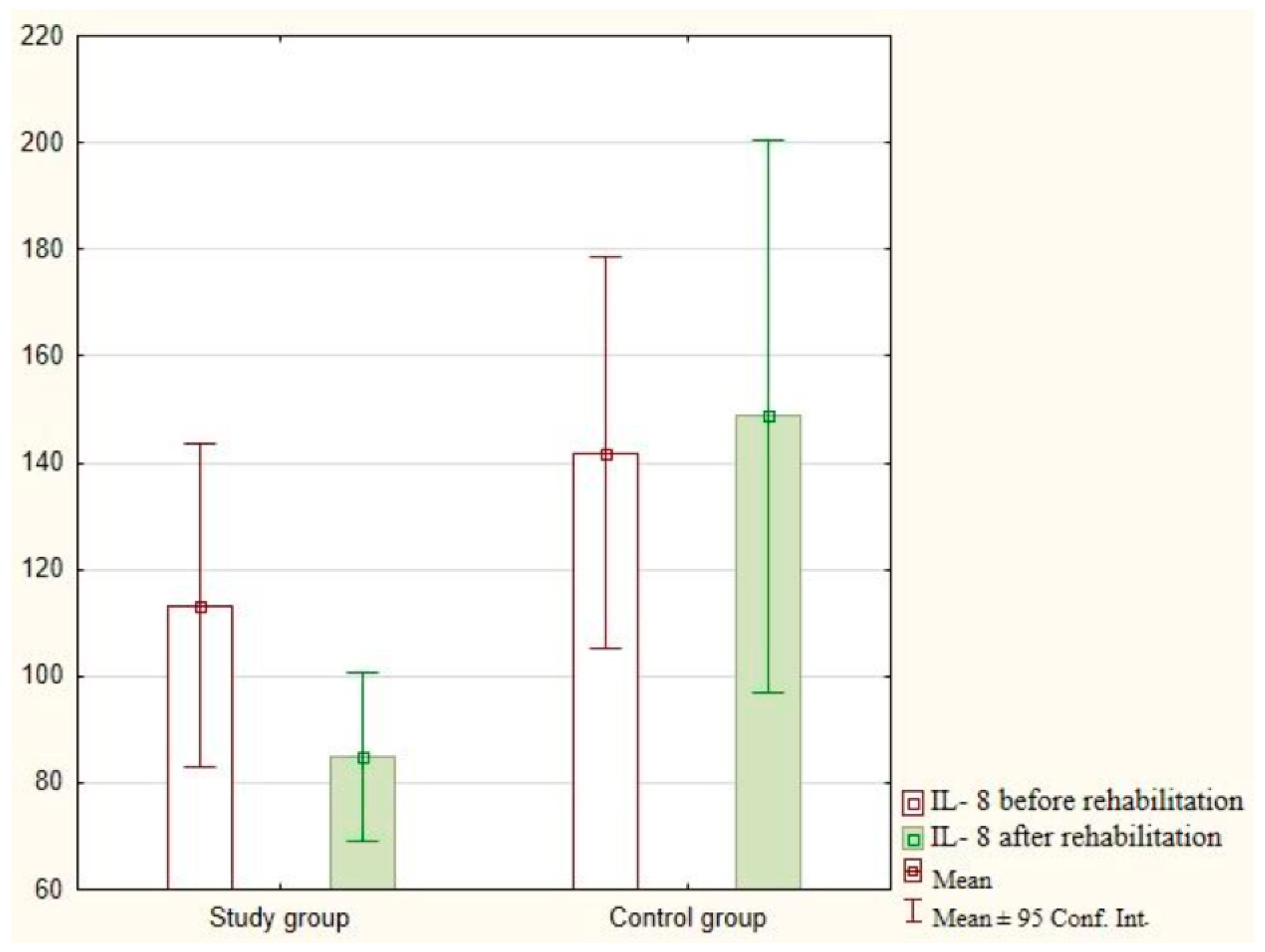
| IL-8 measurement 1 | 113.28 | 104.94 | 75.33 | 141.83 | 98.23 | 119.40 | 0.476 |
| IL-8 measurement 2 | 84.89 | 83.38 | 31.74 | 148.73 | 101.39 | 153.29 | 0.044 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turoń-Skrzypińska, A.; Rotter, I.; Przybyciński, J.; Szylińska, A.; Mińko, A.; Ciechanowski, K.; Dutkiewicz, G. Does Exercising with the Use of Virtual Reality during Haemodialysis Have an Impact on Plasma Levels of Interleukin 1β, Interleukin 6, and Interleukin 8? J. Clin. Med. 2023, 12, 5358. https://doi.org/10.3390/jcm12165358
Turoń-Skrzypińska A, Rotter I, Przybyciński J, Szylińska A, Mińko A, Ciechanowski K, Dutkiewicz G. Does Exercising with the Use of Virtual Reality during Haemodialysis Have an Impact on Plasma Levels of Interleukin 1β, Interleukin 6, and Interleukin 8? Journal of Clinical Medicine. 2023; 12(16):5358. https://doi.org/10.3390/jcm12165358
Chicago/Turabian StyleTuroń-Skrzypińska, Agnieszka, Iwona Rotter, Jarosław Przybyciński, Aleksandra Szylińska, Alicja Mińko, Kazimierz Ciechanowski, and Grażyna Dutkiewicz. 2023. "Does Exercising with the Use of Virtual Reality during Haemodialysis Have an Impact on Plasma Levels of Interleukin 1β, Interleukin 6, and Interleukin 8?" Journal of Clinical Medicine 12, no. 16: 5358. https://doi.org/10.3390/jcm12165358
APA StyleTuroń-Skrzypińska, A., Rotter, I., Przybyciński, J., Szylińska, A., Mińko, A., Ciechanowski, K., & Dutkiewicz, G. (2023). Does Exercising with the Use of Virtual Reality during Haemodialysis Have an Impact on Plasma Levels of Interleukin 1β, Interleukin 6, and Interleukin 8? Journal of Clinical Medicine, 12(16), 5358. https://doi.org/10.3390/jcm12165358