


Current Knowledge on the Different Characteristics of Back Pain in Adults with and without Scoliosis: A Systematic Review

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Selection Criteria
2.2.1. Type of Study
2.2.2. Population
2.2.3. Search Strategy
2.2.4. Outcome Measures
2.2.5. Study Screening
2.2.6. Data Extraction
2.3. Quality Assessment
2.4. Evidence Synthesis and Statistical Analysis
3. Results
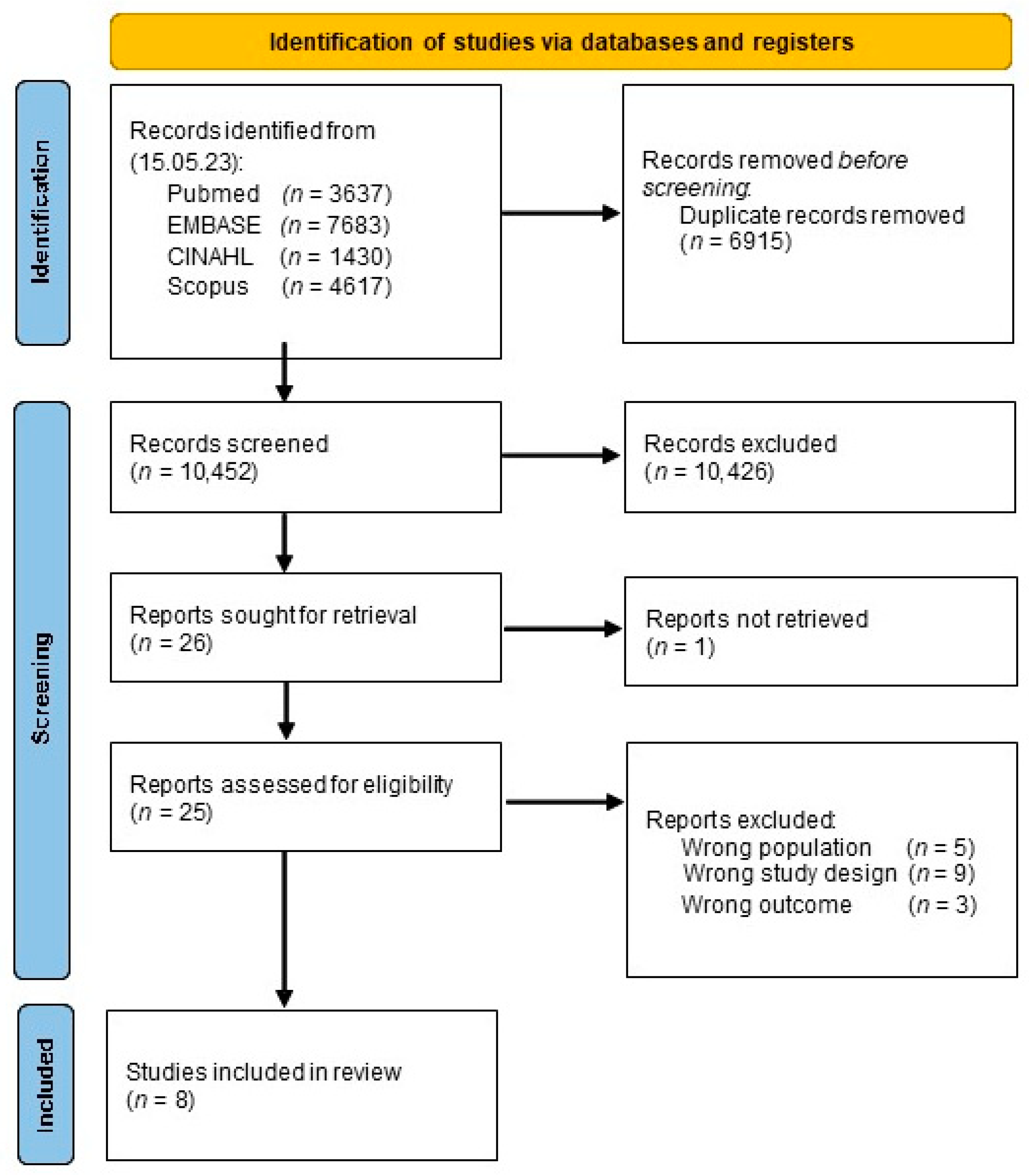
3.1. Study Selection
3.2. Critical Appraisal
3.3. Main Findings
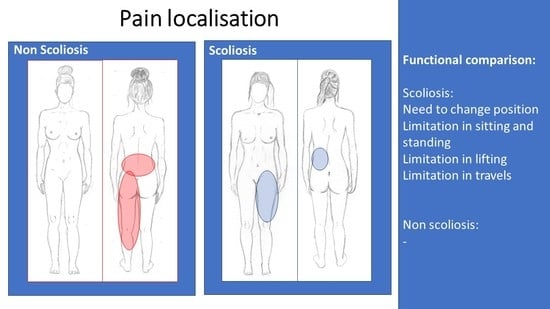
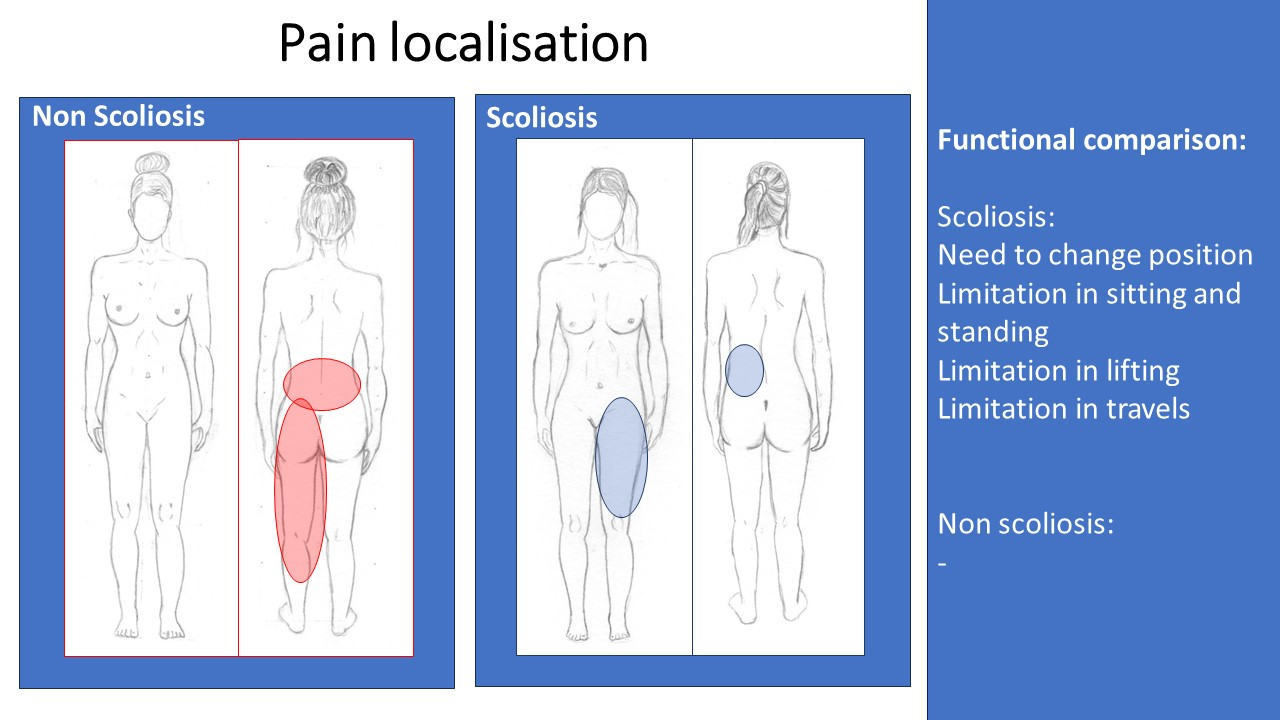
3.4. Pain Localization
3.5. Pain Intensity and Disability
3.6. Factors Influencing Pain
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- PubMed (via pubmed-ncbi.nlm.nih.gov/ accessed on 15 May 2023)
- (“spinal curvatures”[MeSH Terms]) OR (scoliosis[MeSH Terms]);
- ((“spinal curvatures*”[Title/Abstract]) OR (scoliosis*[Title/Abstract]) OR (“spinal deformit*”[Title/Abstract]);
- #1 OR #2;
- (back pain[MeSH Terms] OR sciatica[MeSH Terms] OR radiculopathy[MeSH Terms]);
- ((low back pain*[Title/Abstract]) OR (back pain*[Title/Abstract]) OR (spinal pain[Title/Abstract]) OR (backache*[Title/Abstract]) OR (back ache*[Title/Abstract]) OR (aching[Title/Abstract]) OR (lumbar pain[Title/Abstract]) OR (lumbo*[Title/Abstract]) OR (back disorder*[Title/Abstract]) OR sciatic*[Title/Abstract] OR radiculopat*[Title/Abstract]);
- #4 OR #5;
- #3 AND #6.
- EMBASE (via Embase.com)
- 8.
- (‘scoliosis’/exp OR ‘spinal pain’/exp OR ‘spine malformation’/exp);
- 9.
- (‘spine diseas*’:ab,ti,kw OR ‘spinal curvature*’:ti,ab,kw OR ‘idiopathic* scoliosis’:ti,ab,kw OR ‘degenerative* scoliosis’:ti,ab,kw OR ‘de novo* scoliosis’:ti,ab,kw OR ‘spine malformat*’:ti,ab,kw OR ‘spinal deformit*’:ti,ab,kw OR ‘scoliosis*’:ti,ab,kw);
- 10.
- #1 OR #2;
- 11.
- ‘backache’/exp OR ‘sciatica’/exp;
- 12.
- (‘backache*’:ti,ab,kw OR ‘back pain*’:ti,ab,kw OR ‘low back pain*’:ti,ab,kw OR ‘scoliosis*’:ti,ab,kw OR ‘spinal pain*’:ti,ab,kw OR ‘back ache*’:ti,ab,kw OR ‘lumbar pain*’:ti,ab,kw OR ‘lumbo*’:ti,ab,kw OR ‘aching’:ti,ab,kw OR ‘back disorder*’:ti,ab,kw OR ‘sciatic*’:ti,ab,kw OR ‘radiculopat*’:ti,ab,kw);
- 13.
- #4 OR #5;
- 14.
- #3 AND #6.
- Scopus
- 15.
- TITLE-ABS-KEY(“spinal curvature*” OR “scoliosis*” OR ((“idiopathic*” OR “degenerativ*” OR “de novo*”) W/1 (“scoliosis”)));
- 16.
- TITLE-ABS-KEY(“back pain*” OR “low back pain*” OR ((“spinal” OR “lumbar”) W/1 (“pain*”)) OR “backache*” OR “back ache*” OR “aching” OR “lumbo*” OR “back disorder*” OR “sciatic*” OR “radiculopat*”)));
- 17.
- #1 AND #2.
- CINAHL (via EBSCOhost)
- 18.
- (MH “Spinal Curvatures+”) OR (MH “Scoliosis+”);
- 19.
- TI ((spinal W1 curvatures*) OR “scoliosis*” OR ((idiopathic* OR degenerativ* OR de novo*) N1 (scoliosis))) OR AB ((spinal W1 curvatures*) OR “scoliosis*” OR ((idiopathic* OR degenerativ* OR de novo*) N1 (scoliosis))) OR SU ((spinal W1 curvatures*) OR “scoliosis*” OR ((idiopathic* OR degenerativ* OR de novo*) N1 (scoliosis)));
- 20.
- #1 OR #2;
- 21.
- (MH “Back Pain+”) OR (MH “Sciatica”) OR (MH “Radiculopathy”);
- 22.
- TI (((back OR spinal OR lumbar) N1 (pain*)) OR backache OR sciatic* OR radiculopat*OR (back W1 ache*) OR aching OR lumbo* OR (back W1 disorder*)) OR AB (((back OR spinal OR lumbar) N1 (pain*)) OR backache OR sciatic* OR radiculopat*OR (back W1 ache*) OR aching OR lumbo* OR (back W1 disorder*)) OR SU (((back OR spinal OR lumbar) N1 (pain*)) OR backache OR sciatic* OR radiculopat*OR (back W1 ache*) OR aching OR lumbo* OR (back W1 disorder*));
- 23.
- #4 OR #5;
- 24.
- #3 AND #6.
References
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT Guidelines: Orthopaedic and Rehabilitation Treatment of Idiopathic Scoliosis during Growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Hresko, M.T. Clinical Practice. Idiopathic Scoliosis in Adolescents. N. Engl. J. Med. 2013, 368, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Aebi, M. The Adult Scoliosis. Eur. Spine J. 2005, 14, 925–948. [Google Scholar] [CrossRef] [PubMed]
- McAviney, J.; Roberts, C.; Sullivan, B.; Alevras, A.J.; Graham, P.L.; Brown, B.T. The Prevalence of Adult de Novo Scoliosis: A Systematic Review and Meta-Analysis. Eur. Spine J. 2020, 29, 2960–2969. [Google Scholar] [CrossRef] [PubMed]
- Mayo, N.E.; Goldberg, M.S.; Poitras, B.; Scott, S.; Hanley, J. The Ste-Justine Adolescent Idiopathic Scoliosis Cohort Study. Part III: Back Pain. Spine 1994, 19, 1573–1581. [Google Scholar] [CrossRef]
- Gremeaux, V.; Casillas, J.-M.; Fabbro-Peray, P.; Pelissier, J.; Herisson, C.; Perennou, D. Analysis of Low Back Pain in Adults with Scoliosis. Spine 2008, 33, 402–405. [Google Scholar] [CrossRef]
- Jackson, R.P.; Simmons, E.H.; Stripinis, D. Incidence and Severity of Back Pain in Adult Idiopathic Scoliosis. Spine 1983, 8, 749–756. [Google Scholar] [CrossRef]
- Weinstein, S.L. Natural History. Spine 1999, 24, 2592–2600. [Google Scholar] [CrossRef]
- Schwab, F.; Farcy, J.-P.; Bridwell, K.; Berven, S.; Glassman, S.; Harrast, J.; Horton, W. A Clinical Impact Classification of Scoliosis in the Adult. Spine 2006, 31, 2109–2114. [Google Scholar] [CrossRef] [PubMed]
- Nations, U. World Population Projected to Reach 9.8 Billion in 2050, and 11.2 Billion in 2100. Available online: https://www.un.org/en/desa/world-population-projected-reach-98-billion-2050-and-112-billion-2100 (accessed on 14 February 2023).
- Diebo, B.G.; Shah, N.V.; Boachie-Adjei, O.; Zhu, F.; Rothenfluh, D.A.; Paulino, C.B.; Schwab, F.J.; Lafage, V. Adult Spinal Deformity. Lancet 2019, 394, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-Analysis of Observational Studies in Epidemiology: A Proposal for Reporting. Meta-Analysis Of Observational Studies in Epidemiology (MOOSE) Group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Pérennou, D.; Marcelli, C.; Hérisson, C.; Simon, L. Adult Lumbar Scoliosis. Epidemiologic Aspects in a Low-Back Pain Population. Spine 1994, 19, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Shen, J.; Chen, L.; Wang, H.; Yu, K.; Cong, H.; Zhou, J.; Lin, Y. Differences in Nonspecific Low Back Pain between Young Adult Females with and without Lumbar Scoliosis. Pain Res. Manag. 2019, 2019, 9758273. [Google Scholar] [CrossRef] [PubMed]
- Hoevenaars, E.H.W.; Beekhuizen, M.; O’Dowd, J.; Spruit, M.; van Hooff, M.L. Non-Surgical Treatment for Adult Spinal Deformity: Results of an Intensive Combined Physical and Psychological Programme for Patients with Adult Spinal Deformity and Chronic Low Back Pain-a Treatment-Based Cohort Study. Eur. Spine J. 2022, 31, 1189–1196. [Google Scholar] [CrossRef]
- Bissolotti, L.; Sani, V.; Gobbo, M.; Orizio, C. Analysis of Differences in Pain and Disability in People with Adult Scoliosis and Nonspecific Low Back Pain. Scoliosis 2013, 8, O11. [Google Scholar] [CrossRef][Green Version]
- Weinstein, S.L.; Dolan, L.A.; Spratt, K.F.; Peterson, K.K.; Spoonamore, M.J.; Ponseti, I.V. Health and Function of Patients with Untreated Idiopathic Scoliosis: A 50-Year Natural History Study. JAMA 2003, 289, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Mostofi, K.; Gharaie Moghaddam, B.; Karimi Khouzan, R.; Daryabin, M. The Reliability of LERI’s Sign in L4 and L3 Radiculalgia. J. Clin. Neurosci. 2018, 50, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M. Differential Diagnosis of Back Pain in Adult Scoliosis (Non Operated Patients). Scoliosis 2010, 5, O44. [Google Scholar] [CrossRef]
- Kleimeyer, J.P.; Liu, N.; Hu, S.S.; Cheng, I.; Alamin, T.; Grottkau, B.E.; Kukreja, S.; Wood, K.B. The Relationship Between Lumbar Lateral Listhesis and Radiculopathy in Adult Scoliosis. Spine 2019, 44, 1003–1009. [Google Scholar] [CrossRef] [PubMed]
- Daniels, A.H.; Durand, W.M.; Lafage, R.; Zhang, A.S.; Hamilton, D.K.; Passias, P.G.; Kim, H.J.; Protopsaltis, T.; Lafage, V.; Smith, J.S.; et al. Lateral Thoracolumbar Listhesis as an Independent Predictor of Disability in Adult Scoliosis Patients: Multivariable Assessment Before and After Surgical Realignment. Neurosurgery 2021, 89, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Zaina, F.; Poggio, M.; Donzelli, S.; Negrini, S. Can Bracing Help Adults with Chronic Back Pain and Scoliosis? Short-Term Results from a Pilot Study. Prosthet. Orthot. Int. 2018, 42, 410–414. [Google Scholar] [CrossRef]
- Zaina, F.; Poggio, M.; Di Felice, F.; Donzelli, S.; Negrini, S. Bracing Adults with Chronic Low Back Pain Secondary to Severe Scoliosis: Six Months Results of a Prospective Pilot Study. Eur. Spine J. 2021, 30, 2962–2966. [Google Scholar] [CrossRef] [PubMed]
- Zaina, F.; Ferrario, I.; Caronni, A.; Scarano, S.; Donzelli, S.; Negrini, S. Measuring Quality of Life in Adults with Scoliosis: A Cross-Sectional Study Comparing SRS-22 and ISYQOL Questionnaires. J. Clin. Med. 2023, 12, 5071. [Google Scholar] [CrossRef]
- Mannion, A.F.; Elfering, A.; Bago, J.; Pellise, F.; Vila-Casademunt, A.; Richner-Wunderlin, S.; Domingo-Sàbat, M.; Obeid, I.; Acaroglu, E.; Alanay, A.; et al. Factor Analysis of the SRS-22 Outcome Assessment Instrument in Patients with Adult Spinal Deformity. Eur. Spine J. 2017, 27, 685–699. [Google Scholar] [CrossRef]
- Ha, K.-Y.; Jang, W.-H.; Kim, Y.-H.; Park, D.-C. Clinical Relevance of the SRS-Schwab Classification for Degenerative Lumbar Scoliosis. Spine 2016, 41, E282–E288. [Google Scholar] [CrossRef]
- Monticone, M.; Ambrosini, E.; Cazzaniga, D.; Rocca, B.; Motta, L.; Cerri, C.; Brayda-Bruno, M.; Lovi, A. Adults with Idiopathic Scoliosis Improve Disability after Motor and Cognitive Rehabilitation: Results of a Randomised Controlled Trial. Eur. Spine J. 2016, 25, 3120–3129. [Google Scholar] [CrossRef] [PubMed]
- McAviney, J.; Mee, J.; Fazalbhoy, A.; Du Plessis, J.; Brown, B.T. A Systematic Literature Review of Spinal Brace/Orthosis Treatment for Adults with Scoliosis between 1967 and 2018: Clinical Outcomes and Harms Data. BMC Musculoskelet. Disord. 2020, 21, 87. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Authors | Design | Setting | Evaluated Pain | Participants | Sample | Age | Type of Scoliosis (AAIS or De Novo) | Lumbar Curve Severity in Degrees (Before Treatment) | Presence of More than One Curve | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Recruitment from hospital/outpatient/general population | Country | Low back pain (LBP); Back pain (BP) | N° scoliosis; Female (F) %; | N° non- scoliosis; Female (F) | Scoliosis Mean (SD), Range in years (as reported by study) | Non- Scoliosis Mean (SD), Range in years (as reported by study) | As reported by study | As reported by study | As reported by study | |||
| Perennou 1994 [13] | prospective controlled | Spine Rehabilitation Unit | France | LBP | 671 | 50 (7.5%); F 36 (72%) | 621 (92.5%); F 298 (48%) | 62.1 ± 12.4 (5 pz < 45 y) | 49.6 ± 15.5 | 14% AIS, 86% discovered during examination | 21.2 ± 11.4° (56% <20°, 28% 20–29; 10% 30–39; 6% ≥40° | only lumbar curves |
| Gremeaux 2008 [6] | prospective controlled | Spine Rehabilitation Unit | France | LBP | 100 | 50 (50%) F 68% | 50 (50%); F 66% | 62 ± 13.1 | 62 ± 13.7 | idiopathic and degenerative scoliosis | 23.1 ± 13.1° (10–75°) | only lumbar curves |
| Yuan 2019 [14] | cross- sectional | Department of Physical Therapy and Rehabilitation | China | LBP | 90 | 41 (45.5%) F 100% | 49 (54.5%); F 100% | 24.95 ± 2.90 | 24.73 ± 2.83 | 100% AIS | 26° | only lumbar curves |
| Jackson 1983 [7] | retrospective controlled | Department of Orthopaedics | Canada | BP | 377–245 report pain | 197 pts (52%)–101 pts (51%) report pain; | 180 pts (48%)–144 pts (80%) report pain | 31 | 36 | idiopathic scoliosis | 16 pts lumbar 38° | 45 pts thoracic curve 60°; 26 pts thoracolumbar 50°; 14 pts double curve 55°; |
| Mayo 1994 [5] | retrospective cohort study | Departments of Medicine and Department of Occupational Health, and Epidemiology and Biostatistics | Canada/USA | BP | 3231 (724 report pain) | 1476 (45.6%)–295 pts report pain; | 1755 (55.4%)–429 report pain | 100% AIS | ||||
| Hoevenars 2022 [15] | retrospective controlled | Outpatient | Netherlands | LBP | 320 | 80 (25%); F 79% | 240 (75%); F 79% | 50.9 (SD 14.1, min–max 21–76) | 50.1 (±12.0, 21–74) | 24 adult idiopathic scoliosis, 56 de novo degenerative lumbar scoliosis; | 21.4 (9.4, 11–72) | only lumbar curves |
| Bissolotti 2013 [16] | cross- sectional | Outpatient | Italy | LBP | 80 | 40 (50%); F 75% | 40 (50%); F 77.5% | 61.8 ± 11.5 | 58.2 ± 10.9 | Adult scoliosis | 27.1 ± 11.5° primary curve (range, 15–63°); thoracic curve 25.5 ± 22.3° (range, 8–58°) | |
| Weinstein 2003 [17] | prospective controlled | Department of Orthopaedic Surgery | USA | BP | 179 (88 report pain) | 117 (65.3)–71 (60%) pts report pain; F 89% | 62 (34.6%)–17 (10.4%) pts report pain; F 79.4% | 66 (range, 54–80 y) | <65 y: 23/62 (37); >65 y 39/62 (63) | Late-onset idiopathic scoliosis | 49.41 (SD 26.38) (range 15–90) lumbar, 89.54 (32.69) (range 50–155) Thoracolumbar, 84.50 (30.17) (range 23–156) thoracic | 48 (41%) thoracic curve, 14 (12%) thoracolumbar, 32 (27%) lumbar, 23 (20%) double major |
| Cross-Sectional | 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bissolotti 2013 [16] * | Unclear | No | Yes | No | No | Yes | Unclear | ||||
| Yuan 2019 [14] | Yes | Yes | Yes | No | No | Yes | Yes | ||||
| Longitudinal | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
| Gremeaux 2008 [6] | No | Yes | Yes | No | No | No | Yes | Yes | No | No | Yes |
| Hoevenars 2022 [15] | Yes | Yes | Yes | No | No | No | Yes | Yes | No | No | Yes |
| Jackson 1983 [7] | Yes | Yes | Yes | No | No | No | Yes | Unclear | Yes | Unclear | Unclear |
| Mayo 1994 [5] | No | Yes | Yes | Yes | Yes | No | Yes | Yes | No | No | Yes |
| Perennou 1994 [13] | No | Yes | Yes | No | No | No | Yes | Unclear | Unclear | Unclear | Yes |
| Weinstein 2003 [17] | No | Yes | Yes | No | No | No | Yes | Yes | No | No | Yes |
| Authors | Severity/Intensity of Pain | Location of BP | Referred/Lower Extremity Symptoms | Functional Status | ||||
|---|---|---|---|---|---|---|---|---|
| Scoliosis | Non-Scoliosis | Scoliosis | Non-Scoliosis | Scoliosis | Non-Scoliosis | Scoliosis | Non-Scoliosis | |
| Perennou 1994 [13] | _ | _ | _ | _ | 40% radicular pain: 26% Sciatica, 14% cruralgia | 44.3% radicular pain: 38% Sciatica, 6.3% cruralgia | _ | _ |
| Gremeaux 2008 [6] | 60% little or usual; 40% considerable or severe | 68% little or usual, 32% considerable or severe | _ | _ | 56% (sciatica 26%; cruralgia 26%, neurological claudication 10%, buttock pain 30%), Inguinal dysesthesia 30%, 10% costo-iliac syndrome; Buttock pain (20% little or usual; 45% considerable or severe) Inguinal pain (16.6%; 70%) Obturator neuralgia (3.3%; 30%) | 44% (sciatica 32%; cruralgia 12%, neurological claudication 8%, buttock pain 34%) Inguinal dysesthesia 6%; 0% costo-iliac syndrome | _ | _ |
| Yuan 2019 [14] | 3.5 NRS | 5.5 NPRS | 32 (78%) left-sided lumbar pain, 9 (21%) right-sided lumbar pain; 78% pain on the convex side | 83.7% midline or symmetrical pain | _ | _ | _ | |
| Jackson 1983 [7] | 3.3 (scale from 0 to 5) | _ | 44% pain at lower junctional segment /compensatory curves below the major deformity; DM: 35% mainly junctional area, 44% localised pain in lower junctional levels and in lesser curves below. TL and L mainly junctional and fractional curve segments below MC in 46% and 44%; lumbosacral half-curve segment was most painful. | 65% of patients complained of limb distress, including buttock and thigh pain, before treatment. | _ | _ | _ | |
| Mayo 1994 [5] | _ | _ | Spreading pain (curves > 40°), generalised back pain (curves > 20°) | _ | _ | _ | Limitations in lifting, walking, standing, travel, sitting. Need to change position and lie down/rest. | _ |
| Hoevenaars 2022 [15] | 58.4 (19.1) NRS | 60.4(19.1) | _ | _ | _ | _ | 39.5 (±12) ODI | 40.2 (±12.1) ODI |
| Bissolotti 2013 [16] | NRS 5.9 ± 1.8 (range 2–10) | 5.1 ± 2.2 | _ | _ | 27% sciatic pain | 47% (sciatic pain) | 33.9 ± 17% ODI | 32.6 ± 18.8% ODI |
| Weinstein 2003 [17] | Little/moderate score 1–2: 48/71 (68%); quite bad/unbearable score 3–5: 23/71 (32%) | Little/moderate score 1–2: 12/17 (71%); quite bad/unbearable score 3–5: 5/17 (29%) | _ | _ | _ | _ | 37 pts (39%) felt they had a disability | 16 pts (30%) felt they had a disability |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaina, F.; Marchese, R.; Donzelli, S.; Cordani, C.; Pulici, C.; McAviney, J.; Negrini, S. Current Knowledge on the Different Characteristics of Back Pain in Adults with and without Scoliosis: A Systematic Review. J. Clin. Med. 2023, 12, 5182. https://doi.org/10.3390/jcm12165182
Zaina F, Marchese R, Donzelli S, Cordani C, Pulici C, McAviney J, Negrini S. Current Knowledge on the Different Characteristics of Back Pain in Adults with and without Scoliosis: A Systematic Review. Journal of Clinical Medicine. 2023; 12(16):5182. https://doi.org/10.3390/jcm12165182
Chicago/Turabian StyleZaina, Fabio, Rosemary Marchese, Sabrina Donzelli, Claudio Cordani, Carmelo Pulici, Jeb McAviney, and Stefano Negrini. 2023. "Current Knowledge on the Different Characteristics of Back Pain in Adults with and without Scoliosis: A Systematic Review" Journal of Clinical Medicine 12, no. 16: 5182. https://doi.org/10.3390/jcm12165182
APA StyleZaina, F., Marchese, R., Donzelli, S., Cordani, C., Pulici, C., McAviney, J., & Negrini, S. (2023). Current Knowledge on the Different Characteristics of Back Pain in Adults with and without Scoliosis: A Systematic Review. Journal of Clinical Medicine, 12(16), 5182. https://doi.org/10.3390/jcm12165182