
Trofinetide for Rett Syndrome: Highlights on the Development and Related Inventions of the First USFDA-Approved Treatment for Rare Pediatric Unmet Medical Need

 ,
,  , , , , , , and
, , , , , , and 
Abstract
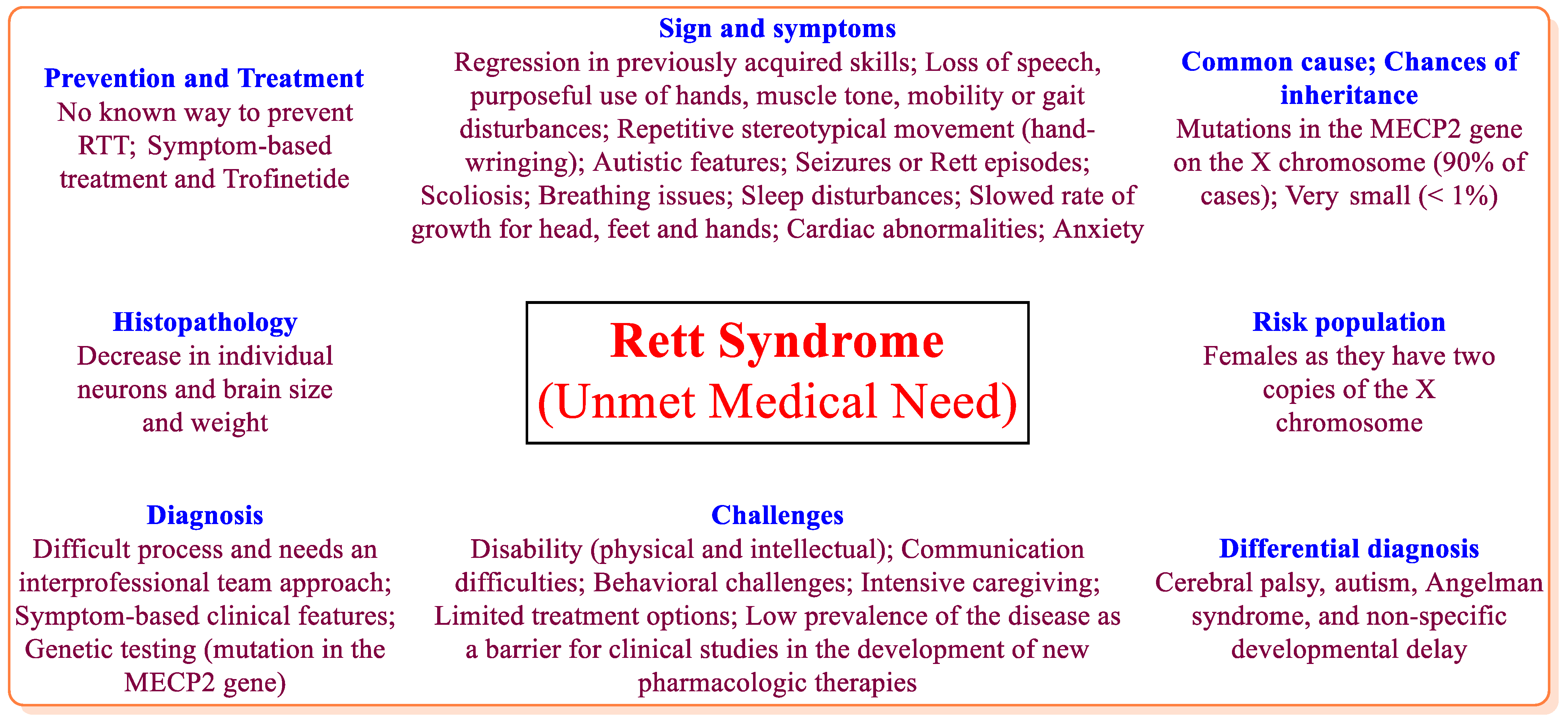
1. Introduction
2. Trofinetide
2.1. General Information
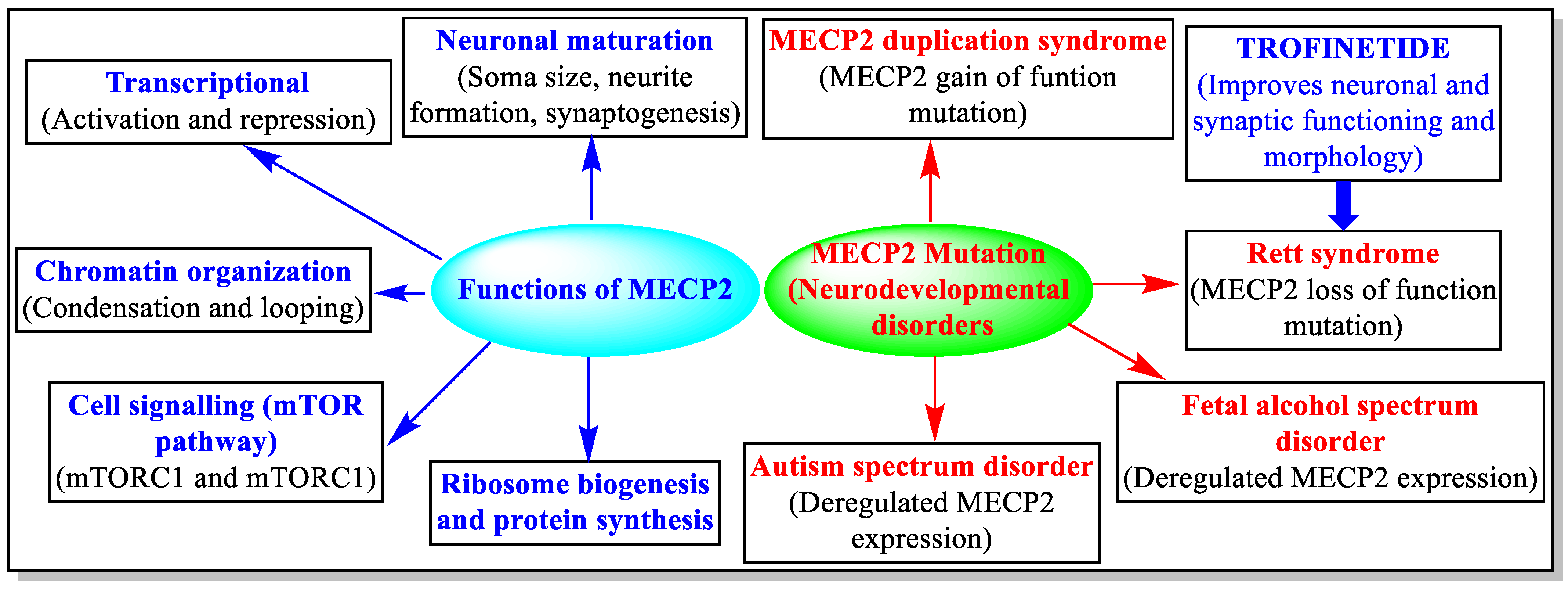
2.2. Mechanism of Action
2.3. Pre-Clinical Studies
2.4. Clinical Studies
2.5. Pharmacology
3. Patents Literature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Panayotis, N.; Ehinger, Y.; Felix, M.S.; Roux, J.-C. State-of-the-art therapies for Rett syndrome. Dev. Med. Child Neurol. 2023, 65, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.E.; Neul, J.L. Rett syndrome and MECP2 duplication syndrome: Disorders of MeCP2 dosage. Neuropsychiatr. Dis. Treat. 2022, 18, 2813–2835. [Google Scholar] [CrossRef] [PubMed]
- Hagberg, B.; Aicardi, J.; Dias, K.; Ramos, O. A progressive syndrome of autism, dementia, ataxia, and loss of purposeful hand use in girls: Rett’s syndrome: Report of 35 cases. Ann. Neurol. 1983, 14, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Amir, R.E.; Van den Veyver, I.B.; Wan, M.; Tran, C.Q.; Francke, U.; Zoghbi, H.Y. Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat. Genet. 1999, 23, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Percy, A.K. Progress in Rett Syndrome: From discovery to clinical trials. Wien. Med. Wochenschr. 2016, 166, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Tascini, G.; Dell’Isola, G.B.; Mencaroni, E.; Di Cara, G.; Striano, P.; Verrotti, A. Sleep Disorders in Rett Syndrome and Rett-Related Disorders: A Narrative Review. Front. Neurol. 2022, 13, 817195. [Google Scholar] [CrossRef]
- Petriti, U.; Dudman, D.C.; Scosyrev, E.; Lopez-Leon, S. Global prevalence of Rett syndrome: Systematic review and meta-analysis. Syst. Rev. 2023, 12, 5. [Google Scholar] [CrossRef]
- Glaze, D.G.; Neul, J.L.; Kaufmann, W.E.; Berry-Kravis, E.; Condon, S.; Stoms, G.; Oosterholt, S.; Della Pasqua, O.; Glass, L.; Jones, N.E.; et al. Double-blind, randomized, placebo-controlled study of trofinetide in pediatric Rett syndrome. Neurology 2019, 92, e1912–e1925. [Google Scholar] [CrossRef]
- Banerjee, A.; Miller, M.T.; Li, K.; Sur, M.; Kaufmann, W.E. Towards a better diagnosis and treatment of Rett syndrome: A model synaptic disorder. Brain 2019, 142, 239–248. [Google Scholar] [CrossRef]
- Borloz, E.; Villard, L.; Roux, J.-C. Rett syndrome: Think outside the (skull) box. Fac. Rev. 2021, 10, 59. [Google Scholar] [CrossRef]
- Lyst, M.J.; Bird, A. Rett syndrome: A complex disorder with simple roots. Nat. Rev. Genet. 2015, 16, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Chahil, G.; Bollu, P.C. Rett Syndrome. 2022. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- International Rett Syndrome Foundation. About Rett Syndrome. Available online: https://www.rettsyndrome.org/about-rett-syndrome/ (accessed on 6 May 2023).
- Neul, J.L.; Percy, A.K.; Benke, T.A.; Berry-Kravis, E.M.; Glaze, D.G.; Peters, S.U.; Jones, N.E.; Youakim, J.M. Design and outcome measures of LAVENDER, a phase 3 study of trofinetide for Rett syndrome. Contemp. Clin. Trials. 2022, 114, 106704. [Google Scholar] [CrossRef]
- Gomathi, M.; Padmapriya, S.; Balachandar, V. Drug Studies on Rett Syndrome: From Bench to Bedside. J. Autism. Dev. Disord. 2020, 50, 2740–2764. [Google Scholar] [CrossRef]
- May, D.; Kponee-Shovein, K.; Mahendran, M.; Downes, N.; Sheng, K.; Lefebvre, P.; Cheng, W.Y. Epidemiology and patient journey of Rett syndrome in the United States: A real-world evidence study. BMC Neurol. 2023, 23, 141. [Google Scholar] [CrossRef]
- Harris, E. Trofinetide Receives FDA Approval as First Drug for Rett Syndrome. JAMA 2023, 329, 1142. [Google Scholar] [CrossRef] [PubMed]
- United States Food and Drug Administration. FDA Approves First Treatment for Rett Syndrome. Available online: https://www.fda.gov/drugs/news-events-human-drugs/fda-approves-first-treatment-rett-syndrome (accessed on 6 May 2023).
- United States Food and Drug Administration. Orange Book: Approved Drug Products with Therapeutic Equivalence Evaluations. Available online: https://www.accessdata.fda.gov/scripts/cder/ob/index.cfm (accessed on 6 May 2023).
- Acadia. DAYBUE™ (Trofinetide): The Only FDA-Approved Treatment for Rett Syndrome. Available online: https://acadia.com/our-medicines/daybue/ (accessed on 6 May 2023).
- Neuren Pharmaceuticals. DAYBUE™ (Trofinetide). Available online: https://www.neurenpharma.com/products/daybue-trofinetide (accessed on 6 May 2023).
- Center for Drug Evaluation and Research. Product Quality Review(s). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/217026Orig1s000ChemR.pdf (accessed on 6 May 2023).
- Center for Drug Evaluation and Research. Clinical Pharmacology Review(s). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/217026Orig1s000ClinPharmR.pdf (accessed on 6 May 2023).
- Lu, X.-C.M.; Chen, R.-W.; Yao, C.; Wei, H.; Yang, X.; Liao, Z.; Dave, J.R.; Tortella, F.C. NNZ-2566, a glypromate analog, improves functional recovery and attenuates apoptosis and inflammation in a rat model of penetrating ballistic-type brain injury. J. Neurotrauma 2009, 26, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Deacon, R.M.; Glass, L.; Snape, M.; Hurley, M.J.; Altimiras, F.J.; Biekofsky, R.R.; Cogram, P. NNZ-2566, a novel analog of (1–3) IGF-1, as a potential therapeutic agent for fragile X syndrome. Neuromolecular Med. 2015, 17, 71–82. [Google Scholar] [CrossRef]
- Bickerdike, M.J.; Thomas, G.B.; Batchelor, D.C.; Sirimanne, E.S.; Leong, W.; Lin, H.; Sieg, F.; Wen, J.; Brimble, M.A.; Harris, P.W.; et al. NNZ-2566: A Gly-Pro-Glu analogue with neuroprotective efficacy in a rat model of acute focal stroke. J. Neurol. Sci. 2009, 278, 85–90. [Google Scholar] [CrossRef]
- Pejhan, S.; Rastegar, M. Role of DNA Methyl-CpG-Binding Protein MeCP2 in Rett Syndrome Pathobiology and Mechanism of Disease. Biomolecules 2021, 11, 75. [Google Scholar] [CrossRef]
- Tillotson, R.; Bird, A. The Molecular Basis of MeCP2 Function in the Brain. J. Mol. Biol. 2020, 432, 1602–1623. [Google Scholar] [CrossRef]
- Itoh, M.; Ide, S.; Takashima, S.; Kudo, S.; Nomura, Y.; Segawa, M.; Kubota, T.; Mori, H.; Tanaka, S.; Horie, H.; et al. Methyl CpG-binding protein 2 (a mutation of which causes Rett syndrome) directly regulates insulin-like growth factor binding protein 3 in mouse and human brains. J. Neuropathol. Exp. Neurol. 2007, 66, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.-C.M.; Si, Y.; Williams, A.J.; Hartings, J.A.; Gryder, D.; Tortella, F.C. NNZ-2566, a glypromate analog, attenuates brain ischemia-induced non-convulsive seizures in rats. J. Cereb. Blood Flow Metab. 2009, 29, 1924–1932. [Google Scholar] [CrossRef]
- Wei, H.H.; Lu, X.-C.M.; Shear, D.A.; Waghray, A.; Yao, C.; Tortella, F.C.; Dave, J.R. NNZ-2566 treatment inhibits neuroinflammation and pro-inflammatory cytokine expression induced by experimental penetrating ballistic-like brain injury in rats. J. Neuroinflamm. 2009, 6, 19. [Google Scholar] [CrossRef] [PubMed]
- Cartagena, C.M.; Phillips, K.L.; Williams, G.L.; Konopko, M.; Tortella, F.C.; Dave, J.R.; Schmid, K.E. Mechanism of action for NNZ-2566 anti-inflammatory effects following PBBI involves upregulation of immunomodulator ATF3. Neuromol. Med. 2013, 15, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Berry-Kravis, E.; Horrigan, J.P.; Tartaglia, N.; Hagerman, R.; Kolevzon, A.; Erickson, C.A.; Hatti, S.; Snape, M.; Yaroshinsky, A.; Stoms, G.; et al. A Double-Blind, Randomized, Placebo-Controlled Clinical Study of Trofinetide in the Treatment of Fragile X Syndrome. Pediatr. Neurol. 2020, 110, 30–41. [Google Scholar] [CrossRef]
- Glaze, D.G.; Neul, J.L.; Percy, A.; Feyma, T.; Beisang, A.; Yaroshinsky, A.; Stoms, G.; Zuchero, D.; Horrigan, J.; Glass, L.; et al. A Double-Blind, Randomized, Placebo-Controlled Clinical Study of Trofinetide in the Treatment of Rett Syndrome. Pediatr. Neurol. 2017, 76, 37–46. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research. Clinical Review(s). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/217026Orig1s000MedR.pdf (accessed on 6 May 2023).
- Center for Drug Evaluation and Research. Non-Clinical Review(s). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/217026Orig1s000PharmR.pdf (accessed on 6 May 2023).
- Center for Drug Evaluation and Research. Summary Review. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/217026Orig1s000SumR.pdf (accessed on 6 May 2023).
- Center for Drug Evaluation and Research. Labeling. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/217026Orig1s000lbl.pdf (accessed on 6 May 2023).
- United States National Library of Medicine. Available online: https://www.clinicaltrials.gov/ (accessed on 6 May 2023).
- Darwish, M.; Youakim, J.M.; Harlick, J.; DeKarske, D.; Stankovic, S. A Phase 1, Open-Label Study to Evaluate the Effects of Food and Evening Dosing on the Pharmacokinetics of Oral Trofinetide in Healthy Adult Subjects. Clin. Drug Investig. 2022, 42, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Oosterholt, S.P.; Horrigan, J.; Jones, N.; Glass, L.; Della Pasqua, O. Population pharmacokinetics of NNZ-2566 in healthy subjects. Eur. J. Pharm. Sci. 2017, 109, S98–S107. [Google Scholar] [CrossRef]
- Center for Drug Evaluation and Research. Risk Assessment and Risk Mitigation Review(s). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2023/217026Orig1s000RiskR.pdf (accessed on 6 May 2023).
- Almehmadi, M.; Allahyani, M.; Alsaiari, A.A.; Alshammari, M.K.; Alharbi, A.S.; Hussain, K.H.; Alsubaihi, L.I.; Kamal, M.; Alotaibi, S.S.; Alotaibi, A.N.; et al. A Glance at the Development and Patent Literature of Tecovirimat: The First-in-Class Therapy for Emerging Monkeypox Outbreak. Viruses 2022, 14, 1870. [Google Scholar] [CrossRef]
- Ashour, M.A.; Fatima, W.; Imran, M.; Ghoneim, M.M.; Alshehri, S.; Shakeel, F. A Review on the Main Phytoconstituents, Traditional Uses, Inventions, and Patent Literature of Gum Arabic Emphasizing Acacia seyal. Molecules 2022, 27, 1171. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.A.; Abida; Alshrari, A.S.; Eltahir Mudawid, M.M.; Alshammari, M.K.; Harshan, A.A.; Alshammari, N.A. Small molecules as kinetoplastid specific proteasome inhibitors for leishmaniasis: A patent review from 1998 to 2021. Expert. Opin. Ther. Pat. 2022, 32, 591–604. [Google Scholar] [CrossRef]
- Imran, M.; Khan, S.A.; Asdaq, S.M.B.; Almehmadi, M.; Abdulaziz, O.; Kamal, M.; Alshammari, M.K.; Alsubaihi, L.I.; Hussain, K.H.; Alharbi, A.S.; et al. An insight into the discovery, clinical studies, compositions, and patents of macozinone: A drug targeting the DprE1 enzyme of Mycobacterium tuberculosis. J. Infect. Public Health 2022, 15, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Sara, V.R. Neuromodulatory Peptide. European Patent Application Publication Number EP0366638A2, 2 May 1990. [Google Scholar]
- Gluckman, P.D.; Williams, C.E. Composition and Methods to Improve Neural Outcome. PCT Patent Application Publication Number WO9517204A1, 29 June 1995. [Google Scholar]
- Gluckman, P.D.; Williams, C.E.; Guan, J. Regulation of Neural Enzymes. PCT Patent Application Publication Number WO9814202A1, 9 April 1998. [Google Scholar]
- Gluckman, P.D.; Guan, J.; Alexi, T. Regulation of tyrosine hydroxylase. PCT Patent Application Publication Number WO9965509A1, 23 December 1999. [Google Scholar]
- Scheepens, A.; Williams, C.E.; Gluckman, P.D.; Clark, R.G. Neuroprotective Effect of Growth Hormone. United States Patent Number US7304029B1, 4 December 2007. [Google Scholar]
- Gluckman, P.; Alexi, T. GPE Analogs. PCT Patent Application Publication Number WO0216408A2, 28 February 2002. [Google Scholar]
- Abood, N.A.; Brimble, M.A. GPE Analogs and Peptidomimetics. United States Patent Number US7041314B2, 9 May 2006. [Google Scholar]
- Gluckman, P.D.; Thomas, G.B.; Guan, J.; Dragunow, M.; Anand, A.K.; Sieg, F.; Brimble, M.A. Effects of Glycyl-2 Methyl Prolyl Glutamate on Neurodegeneration. United States Patent Number US7605177B2, 20 October 2009. [Google Scholar]
- Gluckman, P.D.; Brimble, M.A.; Wilson, D.; Tortella, F.C.; Williams, A.J.; Lu, X.M.; Hartings, J.A.; Gryder, D. Treatment of Non-Convulsive Seizures in Brain Injury Using G-2-Methyl-Prolyl Glutamate. United States Patent Number US7714020B2, 11 May 2010. [Google Scholar]
- Wen, J.; Thomas, G.B.; Bickerdike, M.J. Oral Formulations of Glycyl-2-Methylprolyl-Glutamate. United States Patent Number US7887839B2, 15 February 2011. [Google Scholar]
- Wen, J.; Thomas, G.B.; Bickerdike, M.J. Oral Formulations of Glycyl-2-Methylprolyl-Glutamate. United States Patent Number US8178125B2, 15 May 2012. [Google Scholar]
- Wen, J.; Thomas, G.B.; Bickerdike, M.J. Oral Formulations of Glycyl-2-Methylprolyl-Glutamate. United States Patent Number US8496963B2, 30 July 2013. [Google Scholar]
- Glass, L.; Bickerdike, M.J.; Snape, M.F. Treatment of Fragile X Syndrome Using Glycyl-L-2-Methylprolyl-L-Glutamate. United States Patent Number US9708366B2, 18 July 2017. [Google Scholar]
- Glass, L.I.; Bickerdike, M.J.; Snape, M.F.; De Cogram, P.P. Treatment of Autism Spectrum Disorders Using Glycyl-l-2-Methylprolyl-l-Glumatic Acid. United States Patent Application Publication Number US2015224164A1, 13 August 2015. [Google Scholar]
- Glass, L.I.; Bickerdike, M.J.; Snape, M.F. Treatment of Rett Syndrome Using Glycyl-L-2-Methylprolyl-L-Glutamic Acid. United States Patent Number US9212204B2, 15 December 2015. [Google Scholar]
- Kole, R.; Marshall, J.; Owen, M. Enhanced Delivery of Antioxidants for Treatment of Central Nervous System Disorders Involving Oxidative Stress. United States Patent Number US11612642B2, 28 March 2023. [Google Scholar]
- Blower, C.; Peterson, M.; Shaw, J.M.; Bonnar, J.A.; Moniotte, E.D.F.P.; Bousmanne, M.B.C.; Betti, C.; Decroos, K.W.L.; Ayoub, M. Compositions of Trofinetide. United States Patent Number US11370755B2, 28 June 2022. [Google Scholar]
- Blower, C.; Peterson, M.; Shaw, J.M.; Bonnar, J.A.; Moniotte, E.D.F.P.; Bousmanne, M.B.C.; Betti, C.; Decroos, K.W.L.; Ayoub, M. Compositions of Trofinetide. United States Patent Application Publication Number US2022324799A1, 13 October 2022. [Google Scholar]
- Peterson, M.; Carlos, M.; Bousmanne, M.B.C.; Betti, C.; Jonaitis, D.T.; Mccracken, L.M.; Grove, L. Crystalline Forms of Trofinetide. United States Patent Application Publication Number US2023023114A1, 26 January 2023. [Google Scholar]
- Darwish, M.; Youakim, J.M.; Glass, L.I.; Jones, N.E.; Oosterholt, S.P.; Pasqua, O.D. Methods and Compositions for Treatment of Rett Syndrome. United States Patent Application Publication Number US2022339138A1, 27 October 2022. [Google Scholar]
- Vigneault, F.; Levin, M.; Ingber, D.; Novak, R. Drugs for Treating Neurodevelopmental Disorders. PCT Patent Application Publication Number WO2022246277A2, 24 November 2022. [Google Scholar]
- Page, D.; Levy, J. Treating Disorders Associated with DYRK1A Dysfunction. PCT Patent Application Publication Number WO2022165250A1, 4 August 2022. [Google Scholar]
- Silva-Reis, S.C.; Sampaio-Dias, I.E.; Costa, V.M.; Correia, X.C.; Costa-Almeida, H.F.; García-Mera, X.; Rodríguez-Borges, J.E. Concise Overview of Glypromate Neuropeptide Research: From Chemistry to Pharmacological Applications in Neurosciences. ACS Chem. Neurosci. 2023, 14, 554–572. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.T.; Patwari, P.; Pancoast, J. Compounds and Methods for Modulating Pharmacokinetics. United States Patent Number US9790264B2, 17 October 2017. [Google Scholar]
- Hamidi, T.; Singh, A.K.; Chen, T. Genetic alterations of DNA methylation machinery in human diseases. Epigenomics 2015, 7, 247–265. [Google Scholar] [CrossRef]
- Tropea, D.; Giacometti, E.; Wilson, N.R.; Beard, C.; McCurry, C.; Fu, D.D.; Flannery, R.; Jaenisch, R.; Sur, M. Partial reversal of Rett Syndrome-like symptoms in MeCP2 mutant mice. Proc. Natl. Acad. Sci. USA 2009, 106, 2029–2034. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, O.S.; Ho, E.; Barnes, K.V.; O’Leary, H.M.; Pereira, L.M.; Finkelstein, Y.; Nelson, C.A.; Vogel-Farley, V.; DeGregorio, G.; Holm, I.A.; et al. Safety, pharmacokinetics, and preliminary assessment of efficacy of mecasermin (recombinant human IGF-1) for the treatment of Rett syndrome. Proc. Natl. Acad. Sci. USA 2014, 111, 4596–4601. [Google Scholar] [CrossRef]
- Alshammari, M.K.; Fatima, W.; Alraya, R.A.; Khuzaim Alzahrani, A.; Kamal, M.; Alshammari, R.S.; Alshammari, S.A.; Alharbi, L.M.; Alsubaie, N.S.; Alosaimi, R.B.; et al. Selenium and COVID-19: A spotlight on the clinical trials, inventive compositions, and patent literature. J. Infect. Public Health 2022, 15, 1225–1233. [Google Scholar] [CrossRef]
- Imran, M.; Arora, M.K.; Chaudhary, A.; Khan, S.A.; Kamal, M.; Alshammari, M.M.; Alharbi, R.M.; Althomali, N.A.; Alzimam, I.M.; Alshammari, A.A.; et al. MmpL3 Inhibition as a Promising Approach to Develop Novel Therapies against Tuberculosis: A Spotlight on SQ109, Clinical Studies, and Patents Literature. Biomedicines 2022, 10, 2793. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Active Ingredient (Proprietary Name; Applicant) | Dosage Form (Route; Strength; Approval Date; Marketing Status) | Marketing Exclusivity | Approved Indication |
|---|---|---|---|
| Trofinetide (Daybue; Acadia Pharmaceuticals) | Solution (Oral; 200 mg/mL; 10 March 2023; Prescription) | New chemical entity exclusivity expires on 10 March 2028; Orphan drug exclusivity expires on 10 March 2030 | Rett syndrome or symptoms thereof in patients of ≥2 years of age |
| Parameter | Finding |
|---|---|
| Mechanism of action (MoA) | There was no specific description of the MoA. According to the sponsor, Trofinetide improves neuronal and synaptic functioning and morphology. |
| Kinase binding assay | No significant evidence of strong binding/inhibition was found. |
| Safety | No adverse effects in rats [CNS (350 mg/kg, IV bolus); respiratory system (700 mg/kg, IV single dose); heart rate or arterial blood pressure (800 mg/kg, IV single dose)]; the QTcV interval was slightly prolonged at dose ≥ 400 mg/kg; IC50 (≥20 mM) on hERG current. |
| ADME | Tmax of approximately 2 h (oral 60, 90, 600, 600, and 900 mg/kg/day) in rats; distributed to most tissues in rats (oral 200 mg/kg); no metabolite was revealed brain, plasma, urine feces, or bile of rat (oral 200 mg/kg); excreted in the urine and feces. |
| Toxicology | Well tolerated (1000 mg/kg BID, oral, 26 weeks) in rats and (500 mg/kg BID, oral, 39 weeks) in dogs. |
| Genetic toxicology | No mutagenic effect in the Ames assay (2000 mg/kg/day, oral); negative results in genetic-related assays. |
| Fertility | No adverse effects in female or male rats (1000 mg/kg BID, oral). |
| Carcinogenicity | No study has been conducted yet. The USFDA has asked to conduct a carcinogenicity study during postmarketing surveillance. |
| Pre- and postnatal development | None of the doses tested (up to 1000 mg/kg BID, oral) caused any ill effects on pregnant rats. |
| Embryofetal development studies | No adverse effects were observed in rats (up to 1000 mg/kg BID, oral) and rabbits (up to 300 mg/kg BID, oral) during the period of organogenesis. |
| NCT Number (Other IDs; Title Acronym; Sponsor; Locations) | Phase (Status; Numbers Enrolled; Results; Last Update on Database; Completion Date) | Primary Purpose (Intervention) |
|---|---|---|
| NCT04181723 (ACP-2566-003; Lavender; Acadia Pharmaceuticals; United States) | 3 (Completed; 187; Submitted, but not published; 2 November 2022; 28 October 2021) | Treatment (Efficacy of Trofinetide solution (oral or by gastrostomy tube) versus placebo in females (5–20 years) with RTT) |
| NCT04279314 (ACP-2566-004; LILAC™; Acadia Pharmaceuticals; United States) | 3 (Completed; 154; No result posted; 23 September 2022; 19 August 2022) | Treatment (Safety and tolerability of Trofinetide (oral or by gastrostomy tube) in girls and women with RTT for 40 weeks) |
| NCT04776746 (ACP-2566-005; Not mentioned; Acadia Pharmaceuticals; United States) | 3 (Active, not recruiting; 78; No result posted; 4 April 2023; July 2023) | Treatment (Safety and tolerability of Trofinetide (oral or by gastrostomy tube) in girls and women with RTT for 32 months) |
| NCT04988867 (ACP-2566-009; Daffodil™; Acadia Pharmaceuticals; United States) | 2/3 (Active, not recruiting; 15; No result posted; 6 May 2022; July 2023) | Treatment (Safety and tolerability of oral solution of Trofinetide in girls of 2–5 years age suffering from RTT) |
| NCT02715115 (Neu-2566-RETT-002; Not mentioned; Acadia Pharmaceuticals; United States) | 2 (Completed; 82; Published; 14 August 2020; 5 January 2017) | Treatment (Safety and tolerability of Trofinetide solution in females (5–15 years) with RTT) |
| NCT01703533 (Neu-2566-RETT-001; Not mentioned; Acadia Pharmaceuticals; United States) | 2 (Completed; 67; No result posted; 5 February 2018; September 2014) | Treatment (Safety and tolerability of Trofinetide solution (35 to 70 mg/kg BID) in adolescent/adult females with RTT) |
| NCT00961779 (Neu-2566-HV-004; Not mentioned; Neuren Pharmaceuticals; Australia) | 1 (Completed; 39; No result posted; 7 October 2014; September 2010) | Treatment (Safety and pharmacokinetic parameters of NNZ-2566 in healthy female) |
| NCT01420042 (Neu-2566-HV-005; Not mentioned; Neuren Pharmaceuticals; Australia) | 1 (Completed; 24; No result posted; 22 November 2012; September 2012) | Treatment (Safety and pharmacokinetic parameters of NNZ-2566) |
| Parameter | Summary |
|---|---|
| Dosage form; Route | Pink-red strawberry-flavored solution (200 mg/mL) in 500 mL capacity bottle containing 450 mL solution; Oral and via gastrostomy (G) tube |
| Dose | Two times a day (BD) (morning and evening) based on the patient’s weight (25 mL BD, 9 kg to <12 kg; 30 mL BD, ≥12 kg < 20 kg; 40 mL BD, ≥20 kg < 35 kg; 50 mL BD, ≥35 kg < 50 kg; 60 mL BD, ≥50 kg); Trofinetide can be taken with or without food |
| Pharmacokinetic parameters | Cmax = 139.5–215.8 μg/mL; Tmax = 2–3 h; AUC = 839.6–1109.2 ng/mL/hour; Half-life = 1.5 h; Bioavailability = 84%; Distribution = 80 L; Protein binding ≤ 6%; Excreted unchanged (up to 80%) in urine with minor excretion in feces (15%); No information about clearance |
| Metabolism | CYP450 and uridine diphosphate glucuronosyltransferase (UGT) play a non-significant role in Trofinetide metabolism; Hepatic metabolism is non-significant; No major metabolites are reported; Trofinetide is a weak inhibitor of CYP3A4; In vitro, studies revealed that Trofinetide is an inhibitor of OATP1B1 and OATP1B3. |
| Adverse reaction | Mild to moderate Diarrhea (up to 85% of patients), weight loss (decreased appetite), vomiting, fever, seizure, anxiety, fatigue, and nasopharyngitis. The concomitant administration of loperamide can handle diarrhea. |
| Warning | Diarrohea is one of the major adverse effects. Therefore, concomitant laxative use must be avoided; Weight loss monitoring is also required. |
| Drug/food interaction | No significant effect is expected with co-administration of CYP450 enzyme inducers or inhibitors; Trofinetide can increase the AUC of drugs metabolized by CYP3A4 (e.g., midazolam); Drug monitoring is needed with concomitant use of drugs metabolized via OATP1B1 and OATP1B3; High-fat meal affects the absorption of Trofinetide, but to a negligible extent; No contraindication is revealed for Trofinetide. |
| Special population | Pregnancy and lactation (No adequate data generated as pregnancy among RTT patients is rarely expected); Geriatric patients and patients with compromised kidney/liver functions need drug monitoring due to lack of proper safety data. |
| Toxicity | No information about acute toxicity (LD50) |
| QT prolongation | Trofinetide can prolong QTcF interval; No significant effect on ECG. |
| Patent/Application Number (Status on 6 May 2023; Applicant; Filing Date; Publication Date) | Summary |
|---|---|
| EP0366638A2 (Withdrawn; Kabigen; 24 October 1989; 2 May 1990) | This patent application disclosed that some peptides, including GPE (gly-pro-glu), are effective as a neuromodulator. These peptides either stimulate or inhibit neural activity within the CNS and affect the electrical properties of neurons. It claimed the use of GPE for medicinal and diagnostic use [47]. |
| WO9517204A1 (Lapsed; Auckland Uniservices Limited; 20 December 1994; 29 June 1995) | This patent application revealed GPE’s neuroprotective effects. It claimed a method of treating neural damage with a therapeutically effective amount of GPE [48]. |
| WO9814202A1 (Lapsed; Auckland Uniservices Limited; 6 October 1997; 9 April 1998) | This patent application unveiled that administration of GPE augments the concentration of choline acetyltransferase (ChAT), glutamic acid decarboxylase (GAD), and nitric oxide synthase (NOS) in CNS. It claimed a method of treating diseases caused by the enzymes’ imbalanced activity [49]. |
| WO9965509A1 (Lapsed; Neuronz Limited; 15 June 1999; 23 December 1999) | This patent application discovered that GPE’s administration could augment the concentration of tyrosine hydroxylase in the brain and may be useful for treating Parkinson’s disease [50]. |
| US7304029B1 (Expired; Neuren Pharmaceuticals; 3 September 1999; 4 December 2007) | A method of protecting neurons from degeneration, ischemia, or hypoxia by administering growth hormone or its derivatives, including GPE and IGF-1 [51]. |
| WO0216408A2 (Withdrawn; Neuronz Limited; 24 August 2001; 28 February 2002) | This patent application disclosed GPE analogs for treating brain injury and neurodegenerative diseases [52]. |
| US7041314B2 (Expired; Neuren Pharmaceuticals; 24 May 2002; 9 May 2006) | This patent generically claims Trofinetide and its pharmaceutical compositions with a pharmaceutically acceptable excipient for administration by different routes (intravenous, subcutaneous, topical, intraspinal, aerosol, etc.). It further claims treatment of neural degeneration by administering the claimed compositions of Trofinetide [53]. |
| US7605177B2 (Patented case; Neuren Pharmaceuticals; 20 December 2005; 20 October 2009) | Treating neurological injury caused by traumatic brain injury by administering a therapeutically effective amount of Trofinetide alone or in combination with another anti-apoptotic or neuroprotective agent. It also claims treatment of seizures induced by traumatic brain injury by administering a pharmacologically effective amount of Trofinetide [54]. |
| US7714020B2 (Patented case; Neuren Pharmaceuticals; 4 April 2006; 11 May 2010) | A treatment of traumatic brain injury and non-convulsive seizure using Trofinetide (0.01–10 mg/kg/hour) alone or in combination with another therapeutic agent (phenytoin, phenobarbital, diazepam, acetazolamide, dextromethorphan, etc.) [55]. |
| US7887839B2 (Patented case; Neuren Pharmaceuticals; 15 September 2008; 15 February 2011) | A pharmaceutical emulsion comprising an oil, a surfactant (polyoxyethylene (20) sorbitan monooleate, and sorbitan monooleate), and Trofinetide. The composition may optionally contain a permeability enhancer (sodium caprate and sodium taurocholate). It also claims a tablet comprising the above-mentioned pharmaceutical composition, a binder, and an enteric coating. The claimed composition can be used for treating neurological disorders [56]. |
| US8178125B2 (Patented case; Neuren Pharmaceuticals; 14 February 2011; 15 May 2012) | A pharmaceutical emulsion composition comprising one caprylic triglyceride, a surfactant, and Trofinetide [57]. |
| US8496963B2 (Patented case; Neuren Pharmaceuticals; 14 May 2012; 30 July 2013) | An emulsion comprising Trofinetide and a lipid-containing carboxylic acid. It also claims pharmaceutical composition comprising Trofinetide and a peptide conjugating agent (ethyl 2-cyanoacrylate) [58]. |
| US9708366B2 (Patented case; Neuren Pharmaceuticals; 27 January 2012; 18 July 2017) | A method for treating Fragile X Syndrome (FXS) using an aqueous solution of Trofinetide (0.001 to 100 mg/Kg) alone or combined with a second therapeutic agent [59]. |
| US2015224164A1 (Discontinued; Neuren Pharmaceuticals; 9 February 2015; 13 August 2015) | A method for treating autism spectrum disorder (RTT, FXS, etc.) using Trofinetide alone or combined with another therapeutic agent on a need basis [60]. |
| US9212204B2 (Patented case; Neuren Pharmaceuticals; 26 January 2015; 15 December 2015) | This patent claims a method for treating RTT symptoms with an aqueous solution of Trofinetide. The claimed solution may contain a second therapeutic agent, including IGF-I, GPE, selegiline, and fluoxetine [61]. |
| US11612642B2 (Patented case; Beyond Barriers Therapeutics; 27 April 2020; 28 March 2023) | A method of treating a CNS disorder using an antioxidant (N-acetylcysteine to increase glutathione level in the brain) intranasally alone or in combination with Trofinetide, progesterone, matrix metallopeptidase 9, or NSAIDs [62]. |
| US11370755B2 (Patented case; Neuren Pharmaceuticals; 14 June 2021; 28 June 2022) | The patent relates to the compositions and commercially feasible manufacturing process of Trofinetide. It claims a composition comprising Trofinetide and a side product of Formula II (0.001 to 2 wt%) produced during the manufacturing process of Trofinetide. It also claims a composition comprising about 98 wt% and 100 wt% of Trofinetide on an anhydrous basis [63]. |
| US2022324799A1 (Under examination; Neuren Pharmaceuticals; 23 June 2022; 13 October 2022) | The compositions and commercially feasible manufacturing process of Trofinetide. A composition comprising Trofinetide and two side products (Formula II or Formula III in a concentration of 0.001 to 2 wt%) produced during the manufacturing process of Trofinetide. It also claims a kit containing a dosage form comprising Trofinetide, a side product of Formula II (0.001 to 2 wt%) produced during the manufacturing process of Trofinetide, and instructions for administration to a subject in need thereof [64]. |
| US2023023114A1 (Under examination; Acadia Pharmaceuticals; 12 July 2022; 26 January 2023) | Crystalline Trofinetide hydrate is characterized by its powder x-ray diffraction pattern, d-spacings, FT-Raman spectrum, low-frequency Raman spectrum, 13C solid-state nuclear magnetic resonance spectrum, melting point (71.71–72.06 °C, infrared spectrum, near-infrared spectrum or a combination thereof. It also claims an aqueous pharmaceutical formulation comprising the crystalline Trofinetide hydrate for treating RTT, FXS, autism spectrum disorder, and other neurodevelopmental disorders [65]. |
| US2022339138A1 (Under examination; Acadia Pharmaceuticals; 1 February 2022; 27 October 2022) | A method of treating RTT by administering a pharmaceutical composition of Trofinetide to the patient with MECP2 mutation in a daily amount of (a) 4–10 g if the patient weighs between 8 and 11.9 kg; (b) 10.1–14.0 g if the patient weighs between 12–20 kg; (c) 14.1–18.0 g if the patient weighs between 20.1 and 35 kg; (d) 18.1–22.0 g if the patient weighs between 35.1 and 50 kg; or (e) 22.1–26 g if the patient weighs between 50.1 and 150 kg [66]. |
| WO2022246277A2 (No national phase entry; Harvard College and Tufts Medical Center; 20 May 2022; 24 November 2022) | A method of treating RTT and a symptom of CDKL5 deficiency disorder with a therapeutically effective amount of vorinostat, ivermectin, and Bacteroides fragilis or a polysaccharide isolated from Bacteroides fragilis alone or in combination thereof. It further claims a composition comprising (a) two or more of vorinostat, ivermectin, Trofinetide, and Bacteroides fragilis or a polysaccharide isolated from Bacteroides fragilis and (b) a pharmaceutically acceptable excipient [67]. |
| WO2022165250A1 (No national phase entry; University of Florida; 28 January 2022; 4 August 2022) | A method of treating a DYRK1A-related disorder (autism spectrum disorder, intellectual disability, microcephaly, and sociability deficits) using IGF-1, Trofinetide, or NNZ-2591. The claimed treatment method improves sociability, decreases microcephaly, increases spine density, and/or improves synaptic function [68]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hudu, S.A.; Elmigdadi, F.; Qtaitat, A.A.; Almehmadi, M.; Alsaiari, A.A.; Allahyani, M.; Aljuaid, A.; Salih, M.; Alghamdi, A.; Alrofaidi, M.A.; et al. Trofinetide for Rett Syndrome: Highlights on the Development and Related Inventions of the First USFDA-Approved Treatment for Rare Pediatric Unmet Medical Need. J. Clin. Med. 2023, 12, 5114. https://doi.org/10.3390/jcm12155114
Hudu SA, Elmigdadi F, Qtaitat AA, Almehmadi M, Alsaiari AA, Allahyani M, Aljuaid A, Salih M, Alghamdi A, Alrofaidi MA, et al. Trofinetide for Rett Syndrome: Highlights on the Development and Related Inventions of the First USFDA-Approved Treatment for Rare Pediatric Unmet Medical Need. Journal of Clinical Medicine. 2023; 12(15):5114. https://doi.org/10.3390/jcm12155114
Chicago/Turabian StyleHudu, Shuaibu A., Fayig Elmigdadi, Aiman Al Qtaitat, Mazen Almehmadi, Ahad Amer Alsaiari, Mamdouh Allahyani, Abdulelah Aljuaid, Magdi Salih, Adel Alghamdi, Mohammad A. Alrofaidi, and et al. 2023. "Trofinetide for Rett Syndrome: Highlights on the Development and Related Inventions of the First USFDA-Approved Treatment for Rare Pediatric Unmet Medical Need" Journal of Clinical Medicine 12, no. 15: 5114. https://doi.org/10.3390/jcm12155114
APA StyleHudu, S. A., Elmigdadi, F., Qtaitat, A. A., Almehmadi, M., Alsaiari, A. A., Allahyani, M., Aljuaid, A., Salih, M., Alghamdi, A., Alrofaidi, M. A., Abida, & Imran, M. (2023). Trofinetide for Rett Syndrome: Highlights on the Development and Related Inventions of the First USFDA-Approved Treatment for Rare Pediatric Unmet Medical Need. Journal of Clinical Medicine, 12(15), 5114. https://doi.org/10.3390/jcm12155114