

Local Periarticular Infiltration with Dexmedetomidine Results in Superior Patient Well-Being after Total Knee Arthroplasty Compared with Peripheral Nerve Blocks: A Randomized Controlled Clinical Trial with a Follow-Up of Two Years
 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
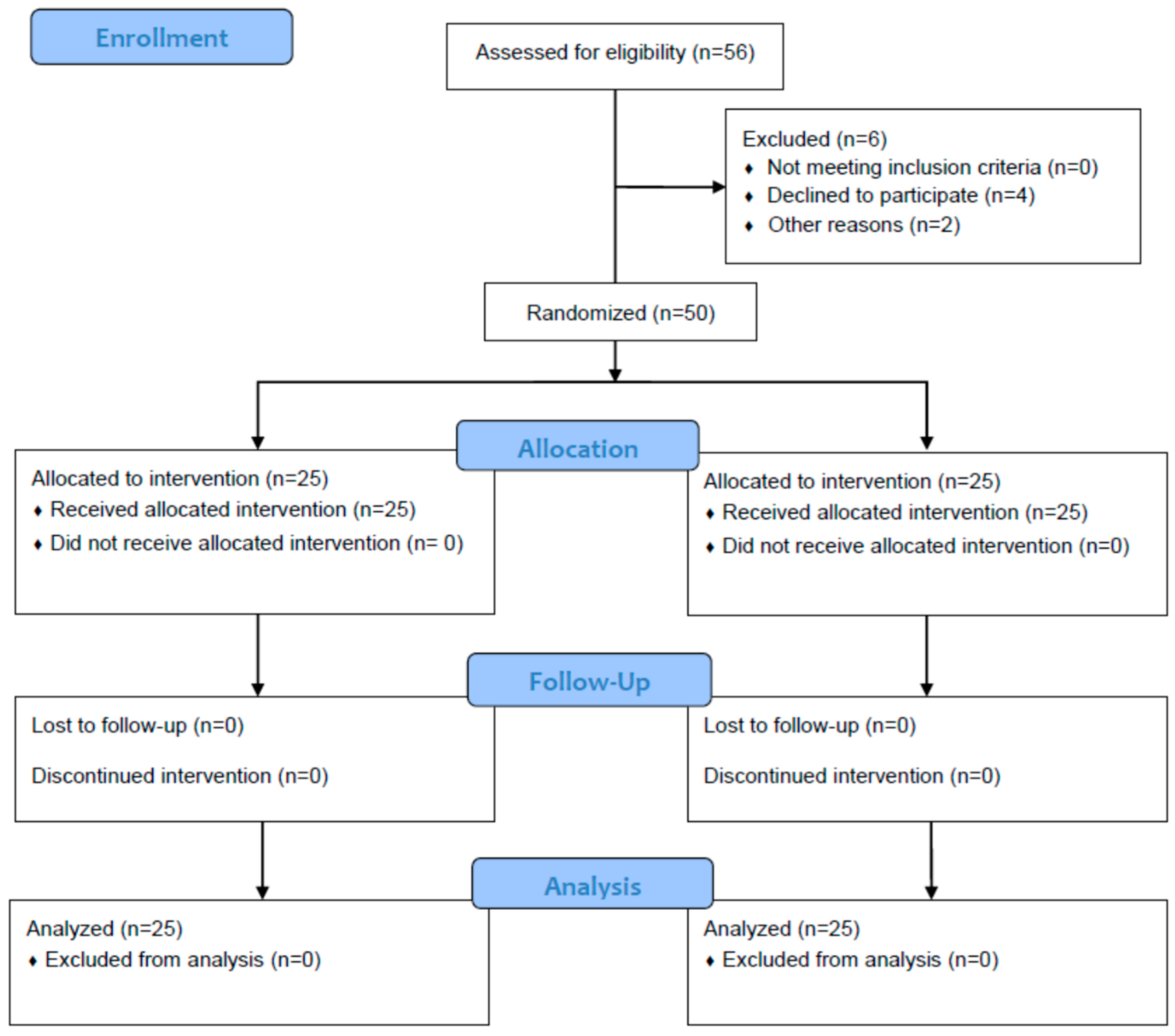
2.1. Study Population
2.2. Local Infiltration Anesthesia Procedures and Regional Anesthesia
2.3. Surgical Technique and Anesthetic Management
2.4. Outcome Measurement
2.5. Statistical Analysis
3. Results
3.1. Well-Being
3.2. Functional Outcome
3.3. Postoperative Improvement
3.4. Rank Correlation and Logistic Regression Analyses
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elmofty, D.H.; Buvanendran, A. Regional Anesthesia in Total Joint Arthroplasty: What Is the Evidence? J. Arthroplast. 2017, 32, S74–S76. [Google Scholar] [CrossRef] [PubMed]
- Elmallah, R.K.; Cherian, J.J.; Pierce, T.P.; Jauregui, J.J.; Harwin, S.F.; Mont, M.A. New and Common Perioperative Pain Management Techniques in Total Knee Arthroplasty. J. Knee Surg. 2016, 29, 169–178. [Google Scholar] [CrossRef]
- Baratta, J.L.; Gandhi, K.; Viscusi, E.R. Perioperative pain management for total knee arthroplasty. J. Surg. Orthop. Adv. 2014, 23, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Schittek, G.A.; Michaeli, K.; Labmayr, V.; Reinbacher, P.; Gebauer, D.; Smigaj, J.; Gollowitsch, J.; Rief, M.; Sampl, L.; Sandner-Kiesling, A.; et al. Influence of personalised music and ice-tea options on post-operative well-being in the post anaesthesia care unit after general or regional anaesthesia. A pre-post-analysis by means of a questionnaire. Intensiv. Crit. Care Nurs. 2021, 63, 102998. [Google Scholar] [CrossRef] [PubMed]
- Schittek, G.A.; Simonis, H.; Bornemann-Cimenti, H. Pain, nausea, vomiting, thirst, cold, … the challenge of well-being in post-operative patients. Intensiv. Crit. Care Nurs. 2021, 66, 103090. [Google Scholar] [CrossRef] [PubMed]
- Schittek, G.A.; Schwantzer, G.; Simonis, H.; Heschl, S.; Sandner-Kiesling, A.; Bornemann-Cimenti, H. Randomised controlled pilot trial of concepts for analgesia and sedation during placement of peripheral regional anaesthesia before operations. Eur. J. Anaesthesiol. 2021, 38, 183–184. [Google Scholar] [CrossRef]
- Hamilton, D.F.; Lane, J.V.; Gaston, P.; Patton, J.T.; MacDonald, D.; Simpson, A.H.R.W.; Howie, C.R. What determines patient satisfaction with surgery? A prospective cohort study of 4709 patients following total joint replacement. BMJ Open 2013, 3, e002525. [Google Scholar] [CrossRef]
- Schittek, G.A.; Schwantzer, G.; Zoidl, P.; Orlob, S.; Holger, S.; Eichinger, M.; Sampl, L.; Bornemann-Cimenti, H.; Sandner-Kiesling, A. Adult patients’ wellbeing and disturbances during early recovery in the post anaesthesia care unit. A cross-sectional study. Intensiv. Crit. Care Nurs. 2020, 61, 102912. [Google Scholar] [CrossRef]
- Shi, Z.B.; Dang, X.Q. Efficacy of multimodal perioperative analgesia protocol with periarticular medication injection and nonsteroidal anti-inflammatory drug use in total knee arthroplasty. Niger. J. Clin. Pract. 2018, 21, 1221–1227. [Google Scholar]
- Lavand’homme, P.M.; Kehlet, H.; Rawal, N.; Joshi, G.P. Pain management after total knee arthroplasty: PROcedure SPEcific Postoperative Pain ManagemenT recommendations. Eur. J. Anaesthesiol. 2022, 39, 743–757. [Google Scholar] [CrossRef]
- Joshi, G.P.; Kehlet, H.; PROSPECT Working Group. Guidelines for perioperative pain management: Need for re-evaluation. Br. J. Anaesth. 2017, 119, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Parvataneni, H.K.; Shah, V.P.; Howard, H.; Cole, N.; Ranawat, A.S.; Ranawat, C.S. Controlling pain after total hip and knee arthroplasty using a multimodal protocol with local periarticular injections: A prospective randomized study. J. Arthroplast. 2007, 22, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Alqwbani, M.; Wang, Q.; Yang, Z.; Liao, R.; Kang, P. Ultrasound-guided adductor canal block combined with lateral femoral cutaneous nerve block for post-operative analgesia following total knee arthroplasty: A prospective, double-blind, randomized controlled study. Int. Orthop. 2021, 45, 1421–1429. [Google Scholar] [CrossRef]
- Fu, H.; Wang, J.; Zhang, W.; Cheng, T.; Zhang, X. Potential superiority of periarticular injection in analgesic effect and early mobilization ability over femoral nerve block following total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 291–298. [Google Scholar] [CrossRef]
- Keijsers, R.; van Delft, R.; Bekerom, M.P.J.v.D.; de Vries, D.C.A.A.; Brohet, R.M.; Nolte, P.A. Local infiltration analgesia following total knee arthroplasty: Effect on post-operative pain and opioid consumption—A meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 1956–1963. [Google Scholar] [CrossRef] [PubMed]
- Terkawi, A.S.; Mavridis, D.; Sessler, D.I.; Nunemaker, M.S.; Doais, K.S.; Terkawi, R.S.; Terkawi, Y.S.; Petropoulou, M.; Nemergut, E.C. Pain Management Modalities after Total Knee Arthroplasty: A Network Meta-analysis of 170 Randomized Controlled Trials. Anesthesiology 2017, 126, 923–937. [Google Scholar] [CrossRef]
- Soffin, E.M.; Memtsoudis, S.G. Anesthesia and analgesia for total knee arthroplasty. Minerva Anestesiol. 2018, 84, 1406–1412. [Google Scholar] [CrossRef] [PubMed]
- Schittek, G.A.; Reinbacher, P.; Rief, M.; Gebauer, D.; Leithner, A.; Vielgut, I.; Labmayr, V.; Simonis, H.; Köstenberger, M.; Bornemann-Cimenti, H.; et al. Combined femoral and popliteal nerve block is superior to local periarticular infiltration anaesthesia for postoperative pain control after total knee arthroplasty. Knee Surgery Sports Traumatol. Arthrosc. 2022, 30, 4046–4053. [Google Scholar] [CrossRef]
- Danninger, T.; Opperer, M.; Memtsoudis, S.G. Perioperative pain control after total knee arthroplasty: An evidence based review of the role of peripheral nerve blocks. World J. Orthop. 2014, 5, 225–232. [Google Scholar] [CrossRef]
- Abdallah, F.W.; Chan, V.W.S.; Gandhi, R.; Koshkin, A.; Abbas, S.; Brull, R. The analgesic effects of proximal, distal, or no sciatic nerve block on posterior knee pain after total knee arthroplasty: A double-blind placebo-controlled randomized trial. Anesthesiology 2014, 121, 1302–1310. [Google Scholar] [CrossRef]
- Qin, L.; You, D.; Zhao, G.; Li, L.; Zhao, S. A comparison of analgesic techniques for total knee arthroplasty: A network meta-analysis. J. Clin. Anesthesia 2021, 71, 110257. [Google Scholar] [CrossRef] [PubMed]
- Memtsoudis, S.G.; Danninger, T.; Rasul, R.; Poeran, J.; Gerner, P.; Stundner, O.; Mariano, E.R.; Mazumdar, M. Inpatient falls after total knee arthroplasty: The role of anesthesia type and peripheral nerve blocks. Anesthesiology 2014, 120, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ma, Y.; Xiao, L. Postoperative Pain Management in Total Knee Arthroplasty. Orthop. Surg. 2019, 11, 755–761. [Google Scholar] [CrossRef]
- Lychagin, A.V.; Gritsyuk, A.A.; Rosenberg, N.; Ceo, S.M.L. Postoperative Pain Control by Local Infiltration Analgesia and Peripheral Nerve Block in Primary Prosthetic Total Knee Arthroplasty. Rambam Maimonides Med. J. 2022, 13, e0019. [Google Scholar] [CrossRef]
- Tian, Y.; Tang, S.; Sun, S.; Zhang, Y.; Chen, L.; Xia, D.; Wang, Y.; Ren, L.; Huang, Y. Comparison between local infiltration analgesia with combined femoral and sciatic nerve block for pain management after total knee arthroplasty. J. Orthop. Surg. Res. 2020, 15, 41. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Kim, D.-Y.; Hwang, J.-T.; Song, D.-K.; Na Lee, H.; Jang, J.S.; Lee, S.-S.; Hwang, S.M.; Moon, S.H.; Shim, J.-H. Dexmedetomidine combined with suprascapular nerve block and axillary nerve block has a synergistic effect on relieving postoperative pain after arthroscopic rotator cuff repair. Knee Surgery Sports Traumatol. Arthrosc. 2021, 29, 4022–4031. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Zhang, Z.; Ma, W.; Liu, R.; Li, Q.; Li, Y. Perineural Dexmedetomidine Reduces the Median Effective Concentration of Ropivacaine for Adductor Canal Block. Med. Sci. Monit. 2021, 27, e929857. [Google Scholar] [CrossRef]
- Herman, J.; Urits, I.; Eskander, J.; Kaye, A.; Viswanath, O. Adductor Canal Block Duration of Analgesia Successfully Prolonged With Perineural Dexmedetomidine and Dexamethasone in Addition to IPACK Block for Total Knee Arthroplasty. Cureus 2020, 12, e10566. [Google Scholar] [CrossRef]
- LA Via, L.; Santonocito, C.; Bartolotta, N.; Lanzafame, B.; Morgana, A.; Continella, C.; Cirica, G.; Astuto, M.; Sanfilippo, F. α-2 agonists vs. fentanyl as adjuvants for spinal anesthesia in elective cesarean section: A meta-analysis. Minerva Anestesiol. 2023, 89, 445–454. Available online: https://www.minervamedica.it/index2.php?show=R02Y2023N05A0445 (accessed on 25 July 2023). [CrossRef]
- Zhang, X.; Wang, D.; Shi, M.; Luo, Y. Efficacy and Safety of Dexmedetomidine as an Adjuvant in Epidural Analgesia and Anesthesia: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin. Drug Investig. 2017, 37, 343–354. Available online: http://link.springer.com/10.1007/s40261-016-0477-9 (accessed on 25 July 2023). [CrossRef]
- Marhofer, P.; Brummett, C.M. Safety and efficiency of dexmedetomidine as adjuvant to local anesthetics. Curr. Opin. Anaesthesiol. 2016, 29, 632–637. Available online: https://journals.lww.com/00001503-201610000-00020 (accessed on 25 July 2023). [CrossRef] [PubMed]
- Fisher, D.A.; David, P. Advancing Patient Outcomes and Economic Value in Total Knee Arthroplasty: The Evidence of the ATTUNE® Knee System. 2020. Available online: https://www.jnjmedtech.com/system/files/pdf/164232-210110_137851-200422_ATTUNE_Evidence.pdf (accessed on 25 July 2023).
- Meftah, M.; Ranawat, A.S.; Ranawat, C.S. Ten-Year Follow-up of a Rotating-Platform, Posterior-Stabilized Total Knee Arthroplasty. J. Bone Jt. Surg. 2012, 94, 426–432. Available online: https://journals.lww.com/00004623-201203070-00006 (accessed on 25 July 2023). [CrossRef] [PubMed]
- Prodromidis, A.D.; Chloros, G.D.; Thivaios, G.C.; Sutton, P.M.; Pandit, H.; Giannoudis, P.V.; Charalambous, C.P. High rate of radiolucent lines following the cemented original design of the ATTUNE total knee arthroplasty. Bone Jt. J. 2023, 105-B, 610–621. Available online: https://boneandjoint.org.uk/doi/10.1302/0301-620X.105B6.BJJ-2022-0675.R1 (accessed on 25 July 2023).
- Indelli, P.F.; Marcucci, M.; Pipino, G.; Charlton, S.; Carulli, C.; Innocenti, M. The Effects of Femoral Component Design on the Patello-Femoral Joint in a PS Total Knee Arthroplasty. Arch. Orthop. Trauma Surg. 2014, 134, 59–64. [Google Scholar] [CrossRef]
- Clary, C.W.; Fitzpatrick, C.K.; Maletsky, L.P.; Rullkoetter, P.J. The Influence of Total Knee Arthroplasty Geometry on Mid-Flexion Stability: An Experimental and Finite Element Study. J. Biomech. 2013, 46, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Cerquiglini, A.; Henckel, J.; Hothi, H.; Allen, P.; Lewis, J.; Eskelinen, A.; Skinner, J.; Hirschmann, M.T.; Hart, A.J. Analysis of the Attune Tibial Tray Backside: A Comparative Retrieval Study. Bone Jt. Res. 2019, 8, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef]
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Scott, W.N. Rationale of the Knee Society clinical rating system. Clin. Orthop. Relat. Res. 1989, 248, 13–14. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Xie, F.; Ye, H.; Zhang, Y.; Liu, X.; Lei, T.; Li, S.-C. Extension from inpatients to outpatients: Validity and reliability of the Oxford Knee Score in measuring health outcomes in patients with knee osteoarthritis. Int. J. Rheum. Dis. 2011, 14, 206–210. [Google Scholar] [CrossRef]
- Thomsen, M.G.; Latifi, R.; Kallemose, T.; Barfod, K.W.; Husted, H.; Troelsen, A. Good validity and reliability of the forgotten joint score in evaluating the outcome of total knee arthroplasty. Acta Orthop. 2016, 87, 280–285. [Google Scholar] [CrossRef]
- Maurice-Szamburski, A.; Bruder, N.; Loundou, A.; Capdevila, X.; Auquier, P. Development and validation of a perioperative satisfaction questionnaire in regional anesthesia. Anesthesiology 2013, 118, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Beckhoff, M.; Klotz, K.-F.; Heinzinger, M.; Gerlach, K.; Ocker, H.; Schmucker, P.; Hüppe, M.; Prüßmann, M. Reliability and validity of the Anaesthesiological Questionnaire for electively operated patients. Anaesthesist 2003, 52, 311–320. [Google Scholar] [CrossRef]
- Simons, G.; Baldwin, D.S. A critical review of the definition of ‘wellbeing’ for doctors and their patients in a post COVID-19 era. Int. J. Soc. Psychiatry 2021, 67, 984–991. [Google Scholar] [CrossRef]
- Clement, N.D.; Burnett, R. Patient satisfaction after total knee arthroplasty is affected by their general physical well-being. Knee Surgery Sports Traumatol. Arthrosc. 2013, 21, 2638–2646. [Google Scholar] [CrossRef]
- Lopez-Olivo, M.A.; Ingleshwar, A.; Landon, G.C.; Siff, S.J.; Barbo, A.; Lin, H.Y.; Suarez-Almazor, M.E. Psychosocial Determinants of Total Knee Arthroplasty Outcomes Two Years After Surgery. ACR Open Rheumatol. 2020, 2, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Kampitak, W.; Tanavalee, A.; Ngarmukos, S.; Amarase, C.; Songthamwat, B.; Boonshua, A. Comparison of Adductor Canal Block Versus Local Infiltration Analgesia on Postoperative Pain and Functional Outcome after Total Knee Arthroplasty: A Randomized Controlled Trial. Malays. Orthop. J. 2018, 12, 7–14. [Google Scholar] [CrossRef]
- Kastelik, J.; Fuchs, M.; Krämer, M.; Trauzeddel, R.F.; Ertmer, M.; von Roth, P.; Perka, C.; Kirschbaum, S.M.; Tafelski, S.; Treskatsch, S. Local infiltration anaesthesia versus sciatic nerve and adductor canal block for fast-track knee arthroplasty: A randomised controlled clinical trial. Eur. J. Anaesthesiol. 2019, 36, 255–263. [Google Scholar] [CrossRef]
- Uesugi, K.; Kitano, N.; Kikuchi, T.; Sekiguchi, M.; Konno, S.-I. Comparison of peripheral nerve block with periarticular injection analgesia after total knee arthroplasty: A randomized, controlled study. Knee 2014, 21, 848–852. [Google Scholar] [CrossRef]
- Hertog, A.D.; Gliesche, K.; Timm, J.; Mühlbauer, B.; Zebrowski, S. Pathway-controlled fast-track rehabilitation after total knee arthroplasty: A randomized prospective clinical study evaluating the recovery pattern, drug consumption, and length of stay. Arch. Orthop. Trauma Surg. 2012, 132, 1153–1163. [Google Scholar] [CrossRef]
- Henderson, K.G.; Wallis, J.A.; Snowdon, D.A. Active physiotherapy interventions following total knee arthroplasty in the hospital and inpatient rehabilitation settings: A systematic review and meta-analysis. Physiotherapy 2018, 104, 25–35. [Google Scholar] [CrossRef]
- Castorina, S.; Guglielmino, C.; Castrogiovanni, P.; Szychlinska, M.A.; Ioppolo, F.; Massimino, P.; Leonardi, P.; Maci, C.; Iannuzzi, M.; Di Giunta, A.; et al. Clinical evidence of traditional vs fast track recovery methodologies after total arthroplasty for osteoarthritic knee treatment. A retrospective observational study. Muscles Ligaments Tendons J. 2017, 7, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Lützner, J.; Gehring, R.; Beyer, F. Slightly better pain relief but more frequently motor blockade with combined nerve block analgesia compared to continuous intraarticular analgesia after total knee arthroplasty. Knee Surgery Sports Traumatol. Arthrosc. 2020, 28, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Perlas, A.; Kirkham, K.R.; Billing, R.; Tse, C.; Brull, R.; Gandhi, R.; Chan, V.W.S. The impact of analgesic modality on early ambulation following total knee arthroplasty. Reg. Anesthesia Pain Med. 2013, 38, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, M.M.; Dadheech, A.N.; Wakankar, H.M.; Ganjewar, N.V.; Hedgire, S.S.; Pandit, H.G. Randomized Prospective Comparative Study of Adductor Canal Block vs Periarticular Infiltration on Early Functional Outcome after Unilateral Total Knee Arthroplasty. J. Arthroplast. 2019, 34, 2360–2364. [Google Scholar] [CrossRef]
- Yu, S.; Szulc, A.; Walton, S.; Bosco, J.; Iorio, R. Pain Control and Functional Milestones in Total Knee Arthroplasty: Liposomal Bupivacaine versus Femoral Nerve Block. Clin. Orthop. Relat. Res. 2017, 475, 110–117. [Google Scholar] [CrossRef]
- Fan, L.; Yu, X.; Zan, P.; Liu, J.; Ji, T.; Li, G. Comparison of Local Infiltration Analgesia with Femoral Nerve Block for Total Knee Arthroplasty: A Prospective, Randomized Clinical Trial. J. Arthroplast. 2015, 31, 1361–1365. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0883540315011092 (accessed on 25 July 2023).
- Theunissen, M.; Peters, M.L.; Bruce, J.; Gramke, H.-F.; Marcus, M.A. Preoperative Anxiety and Catastrophizing. Clin. J. Pain 2012, 28, 819–841. Available online: https://journals.lww.com/00002508-201211000-00010 (accessed on 25 July 2023). [CrossRef]
- Jack, K.; McLean, S.M.; Moffett, J.K.; Gardiner, E. Barriers to treatment adherence in physiotherapy outpatient clinics: A systematic review. Man. Ther. 2010, 15, 220–228. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1356689X09002094 (accessed on 25 July 2023). [CrossRef]
- Aso, K.; Izumi, M.; Sugimura, N.; Okanoue, Y.; Kamimoto, Y.; Yokoyama, M.; Ikeuchi, M. Additional benefit of local infiltration of analgesia to femoral nerve block in total knee arthroplasty: Double-blind randomized control study. Knee Surgery Sports Traumatol. Arthrosc. 2019, 27, 2368–2374. [Google Scholar] [CrossRef]
- Surdam, J.W.; Licini, D.J.; Baynes, N.T.; Arce, B.R. The use of exparel (liposomal bupivacaine) to manage postoperative pain in unilateral total knee arthroplasty patients. J. Arthroplast. 2015, 30, 325–329. [Google Scholar] [CrossRef]
- Essving, P.; Axelsson, K.; Kjellberg, J.; Wallgren, A.; Gupta, A.; Lundin, A. Reduced morphine consumption and pain intensity with local infiltration analgesia (LIA) following total knee arthroplasty. Acta Orthop. 2010, 81, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Spangehl, M.J.; Clarke, H.D.; Hentz, J.G.; Misra, L.; Blocher, J.L.; Seamans, D.P. The Chitranjan Ranawat Award: Periarticular injections and femoral & sciatic blocks provide similar pain relief after TKA: A randomized clinical trial. Clin. Orthop. Relat. Res. 2015, 473, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Cicekci, F.; Yildirim, A.; Önal,, Ö.; Celik, J.B.; Kara, I. Ultrasound-guided adductor canal block using levobupivacaine versus periarticular levobupivacaine infiltration after total knee arthroplasty: A randomized clinical trial. Sao Paulo Med. J. 2019, 137, 45–53. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| USRA, N = 25 | LIA, N = 25 | p-Value | |
|---|---|---|---|
| Age (years) | 67.6 (±11.0) | 68.6 (±10.2) | 0.771 |
| Female (%) | 10 (40) | 12 (48) | 0.569 |
| BMI (kg/m2) | 27.8 [24.3 to 33.8] | 28.4 [25.7 to 31.6] | 0.734 |
| ASA 1 (%) | 1 (4) | 0 (0) | |
| ASA 2 (%) | 7 (28) | 10 (40) | 0.437 |
| ASA 3 (%) | 17 (68) | 15 (60) | |
| General anesthesia (%) | 11 (44) | 5 (20) | 0.037 |
| Spinal anesthesia (%) | 14 (56) | 20 (80) | |
| Days of hospitalization | 6.0 [6.0 to 7.0] | 6.0 [6.0 to 7.0] | 0.639 |
| Well-being, N (%) | |||
| No: 22 (88%) Yes: 3 (12%) | No: 15 (60%) Yes: 10 (40%) | 0.024 |
| No: 5 (11%) Yes: 42 (89%) | No: 4 (9%) Yes: 43 (91%) | 1.000 |
| No: 5 (11%) Yes: 42 (89%) | No: 4 (9%) Yes: 43 (91%) | 1.000 |
| USRA (n = 25) | LIA (n = 25) | p-Value | |
|---|---|---|---|
| Range of Motion | |||
| 105 [100–115] | 95 [85–115] | 0.412 |
| 90 [90–100] | 90 [90–100] | 0.593 |
| 115 [110–120] | 115 [110–120] | 0.734 |
| 118 [90–145] | 119 [100–145] | 0.825 |
| 123 [100–150] | 123 [100–150] | 0.241 |
| KSKS Pain | |||
| 59 [55–64] | 55 [53–67] | 0.464 |
| 65 [62–67] | 75 [68–92] | 0.011 |
| 92 [89–97] | 90 [73–96] | 0.907 |
| 96 [80–100] | 95 [87–100] | 0.497 |
| 98 [90–100] | 98 [94–100] | 0.189 |
| KSKS Function | |||
| 50 [50–70] | 50 [50–60] | 0.565 |
| 20 [20–50] | 30 [30–60] | 0.257 |
| 50 [50–70] | 50 [50–60] | 0.757 |
| 83 [65–100] | 84 [50–100] | 0.659 |
| 93 [65–100] | 93 [80–100] | 0.643 |
| WOMAC | |||
| 57.1 [54.2–63.4] | 58.6 [55–62.3] | 0.846 |
| 72.3 [65.9–78] | 77.4 [75.1–80.3] | 0.081 |
| 90.1 [85.3–94.1] | 90.5 [90.3–95.3] | 0.294 |
| 92.6 [86–100] | 93.4 [86–100] | 0.711 |
| 94.1 [90–100] | 95.8 [90–100] | 0.754 |
| OKS | |||
| 19 [17–23] | 16 [14–22] | 0.255 |
| 31 [27–36] | 31 [27–36] | 0.712 |
| 38 [28–42] | 37 [28–41] | 0.862 |
| 43 [31–45] | 43 [32–46] | 0.897 |
| FJS | |||
| 48 [47–51] | 51 [49–53] | 0.090 |
| 62 [48–75] | 63 [49–78] | 0.382 |
| 80 [60–92] | 82 [58–94] | 0.827 |
| Exp (B) | 95% CI for Exp (B) | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| male sex | 0.622 | 9 (50%) | 30 (86%) | 0.009 |
| LIA | 5.254 | 13 (72%) | 27 (77%) | 0.743 |
| GA | 0.748 | 4 (22%) | 11 (31%) | 0.539 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reinbacher, P.; Schittek, G.A.; Draschl, A.; Hecker, A.; Leithner, A.; Klim, S.M.; Brunnader, K.; Koutp, A.; Hauer, G.; Sadoghi, P. Local Periarticular Infiltration with Dexmedetomidine Results in Superior Patient Well-Being after Total Knee Arthroplasty Compared with Peripheral Nerve Blocks: A Randomized Controlled Clinical Trial with a Follow-Up of Two Years. J. Clin. Med. 2023, 12, 5088. https://doi.org/10.3390/jcm12155088
Reinbacher P, Schittek GA, Draschl A, Hecker A, Leithner A, Klim SM, Brunnader K, Koutp A, Hauer G, Sadoghi P. Local Periarticular Infiltration with Dexmedetomidine Results in Superior Patient Well-Being after Total Knee Arthroplasty Compared with Peripheral Nerve Blocks: A Randomized Controlled Clinical Trial with a Follow-Up of Two Years. Journal of Clinical Medicine. 2023; 12(15):5088. https://doi.org/10.3390/jcm12155088
Chicago/Turabian StyleReinbacher, Patrick, Gregor A. Schittek, Alexander Draschl, Andrzej Hecker, Andreas Leithner, Sebastian Martin Klim, Kevin Brunnader, Amir Koutp, Georg Hauer, and Patrick Sadoghi. 2023. "Local Periarticular Infiltration with Dexmedetomidine Results in Superior Patient Well-Being after Total Knee Arthroplasty Compared with Peripheral Nerve Blocks: A Randomized Controlled Clinical Trial with a Follow-Up of Two Years" Journal of Clinical Medicine 12, no. 15: 5088. https://doi.org/10.3390/jcm12155088
APA StyleReinbacher, P., Schittek, G. A., Draschl, A., Hecker, A., Leithner, A., Klim, S. M., Brunnader, K., Koutp, A., Hauer, G., & Sadoghi, P. (2023). Local Periarticular Infiltration with Dexmedetomidine Results in Superior Patient Well-Being after Total Knee Arthroplasty Compared with Peripheral Nerve Blocks: A Randomized Controlled Clinical Trial with a Follow-Up of Two Years. Journal of Clinical Medicine, 12(15), 5088. https://doi.org/10.3390/jcm12155088