
Alopecias: Practical Tips for the Management of Biopsies and Main Diagnostic Clues for General Pathologists and Dermatopathologists


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Hair Types
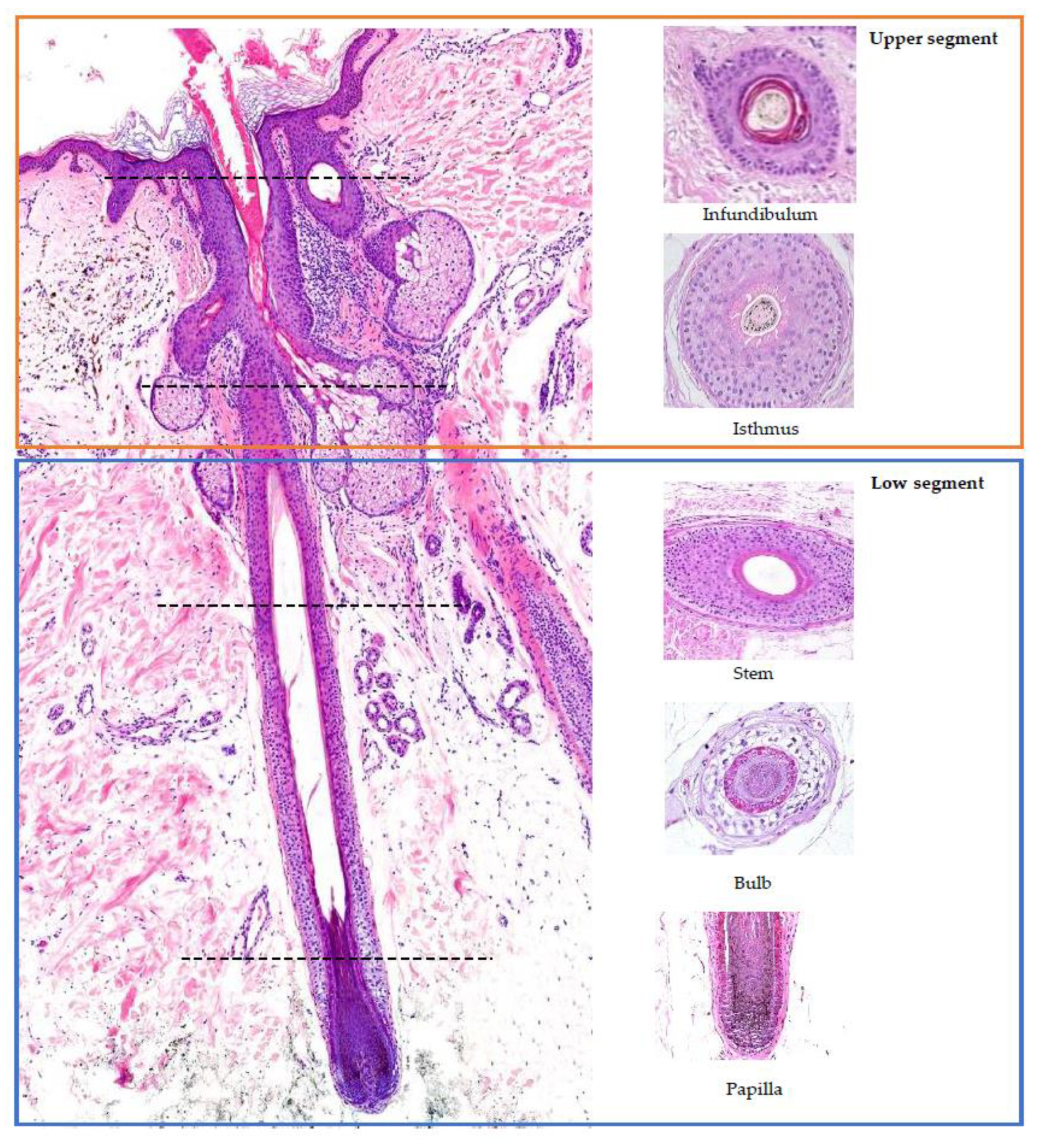
2. Hair Follicle Histology (Figure 1) [5,7,8,9,10]

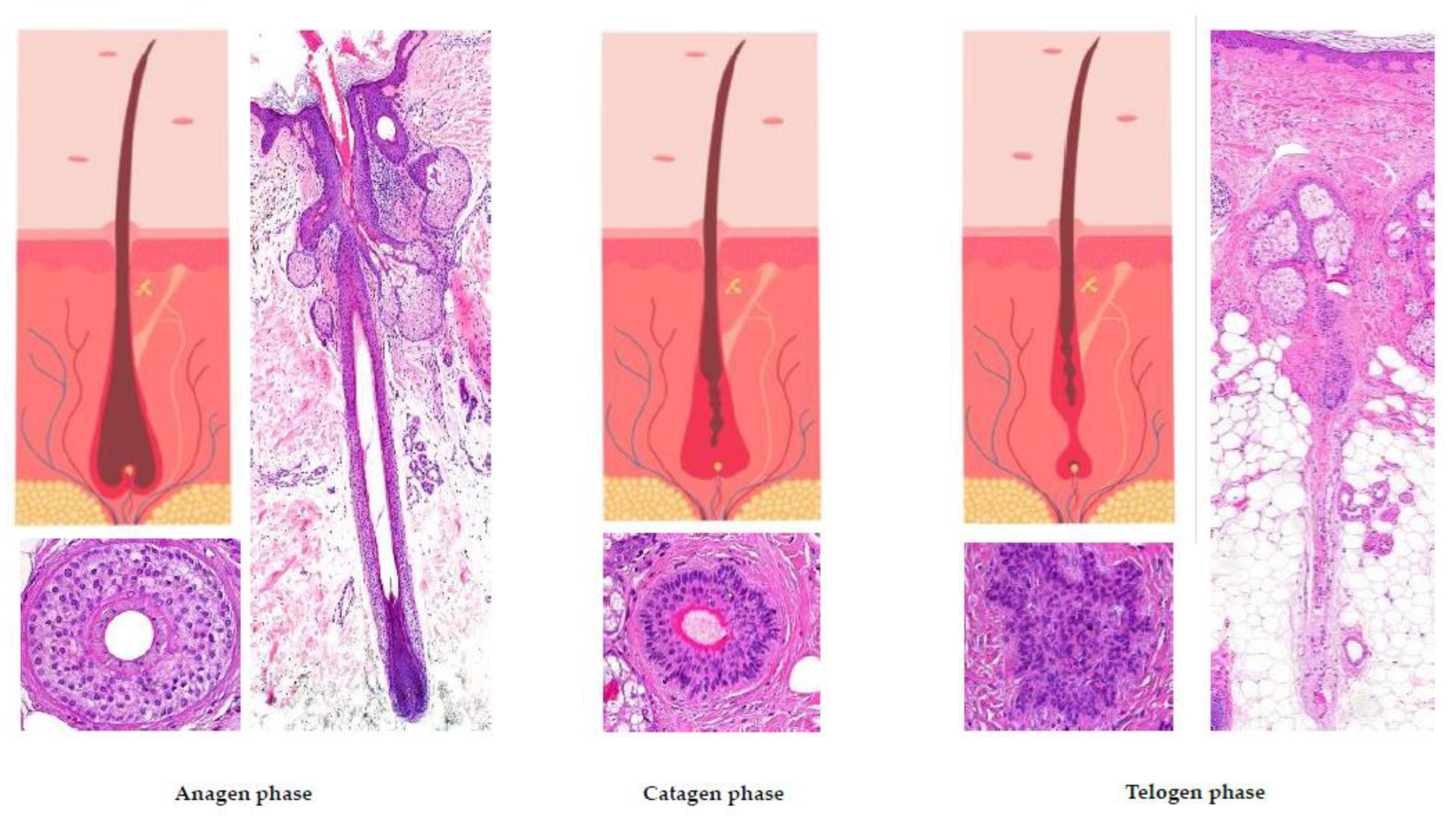
3. Hair Cycle (Figure 2) [5,8,9,11]

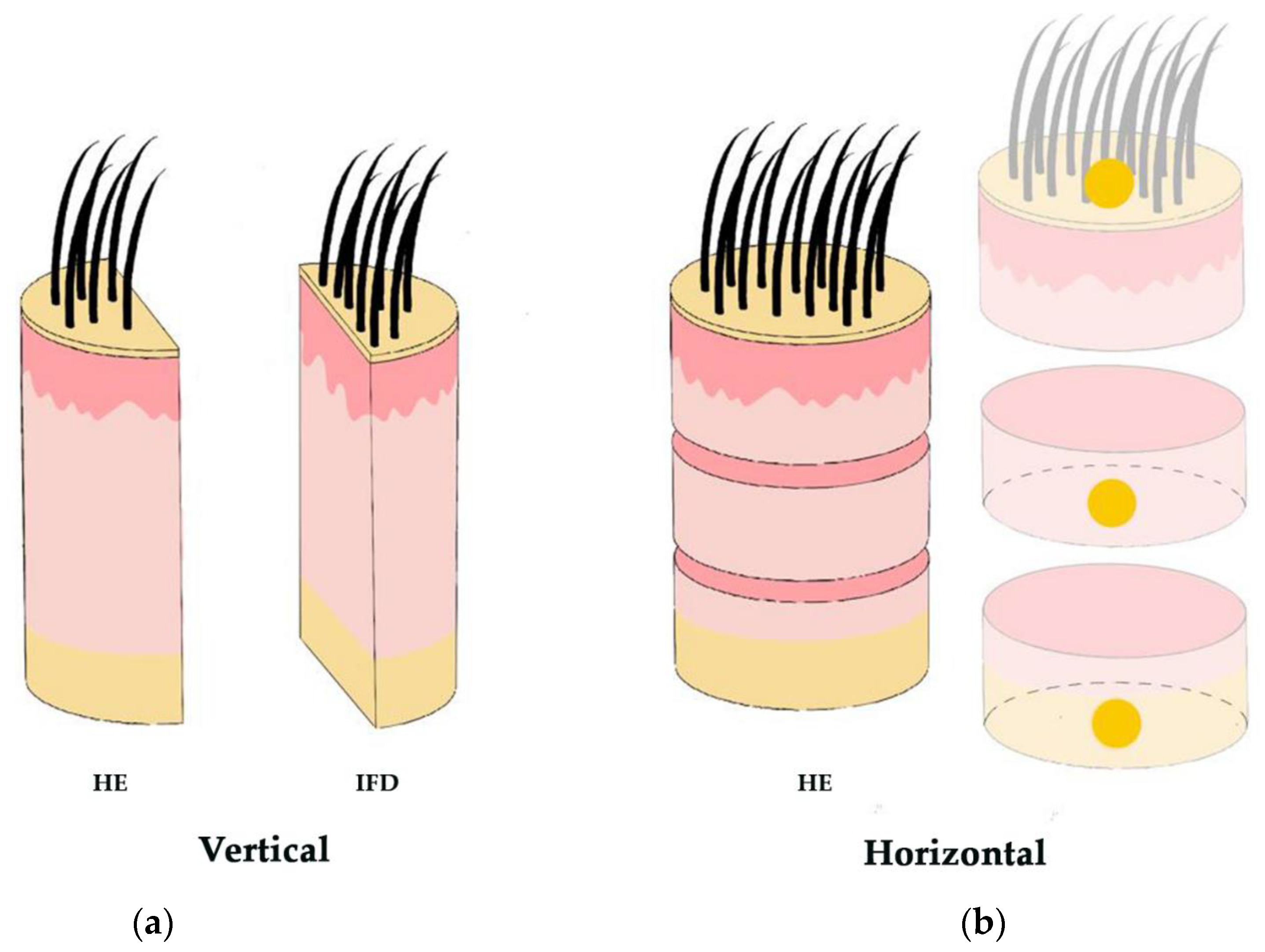
4. Adequate Hair Biopsy
5. Alopecia Classification
5.1. Nonscarring Alopecia [29]
- A.
- 1.
- Clinical Presentation:
- -
- Male pattern hair loss: characterized by bitemporal hairline recession, followed by the loss of hair in the frontotemporal and vertex regions.
- -
- Female pattern hair loss: typically manifests as diffuse hair loss, primarily affecting the central part of the scalp.
- 2.
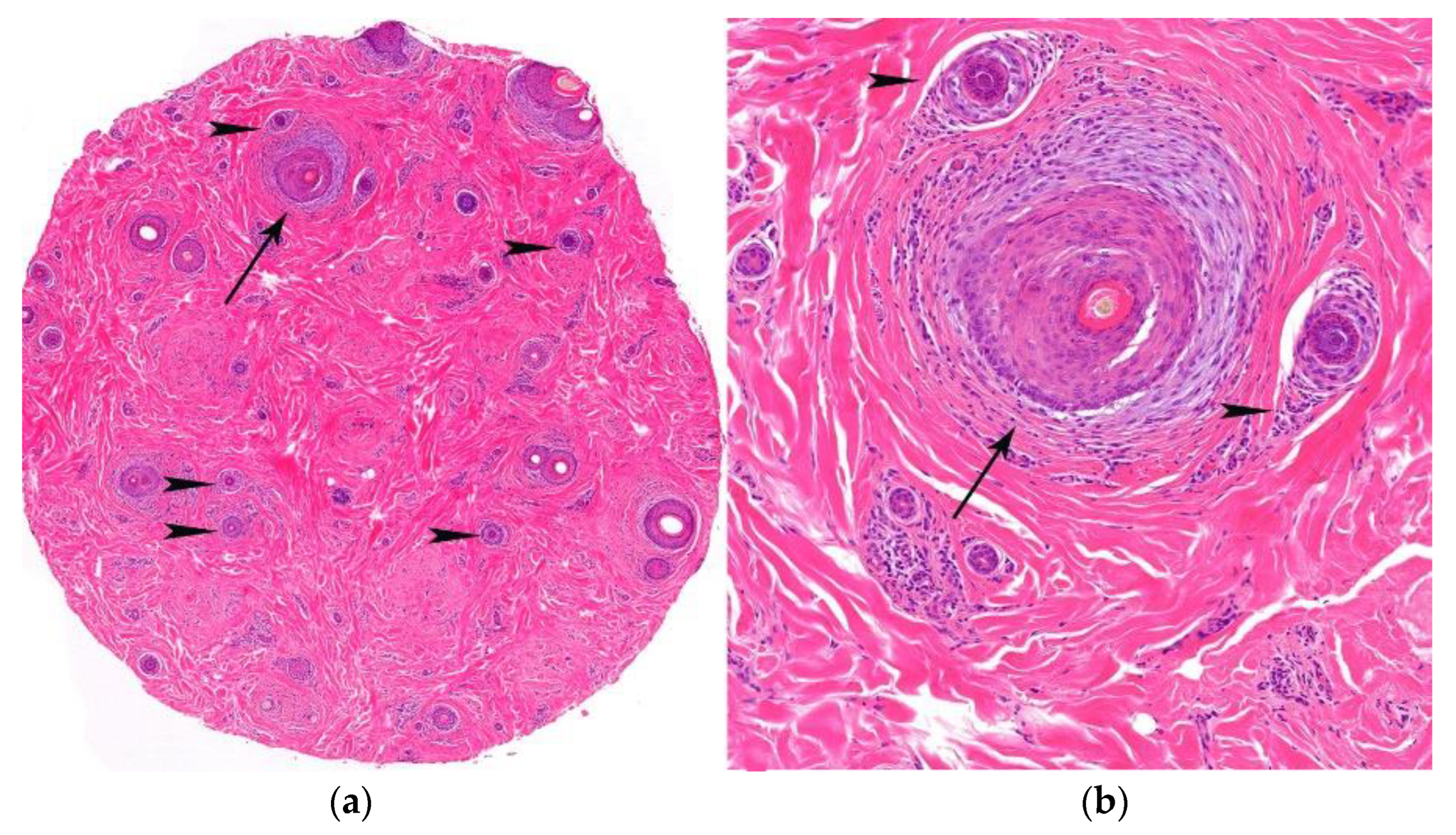
- Histological Features (Figure 7):
- -
- Increase in the vellus index: miniaturization of terminal hair.
- -
- Increase in the telogen index.
- -
- Sebaceous gland pseudohyperplasia.
- -
- Perifollicular lymphocytic infiltrate (70%).
- -
- Absence of concentric fibrosis.
- -
- Polarized light: negative birrefringence of follicular streamers/stelae.

- B.
- 1.
- Clinical Presentation:
- -
- Diffuse alopecia.
- -
- Acute or chronic (if the diffuse hair loss has lasted for more than 6 months).
- -
- Can be associated with androgenetic alopecia, especially in males; for this reason it is advisable to perform a biopsy from the occipital area.
- 2.
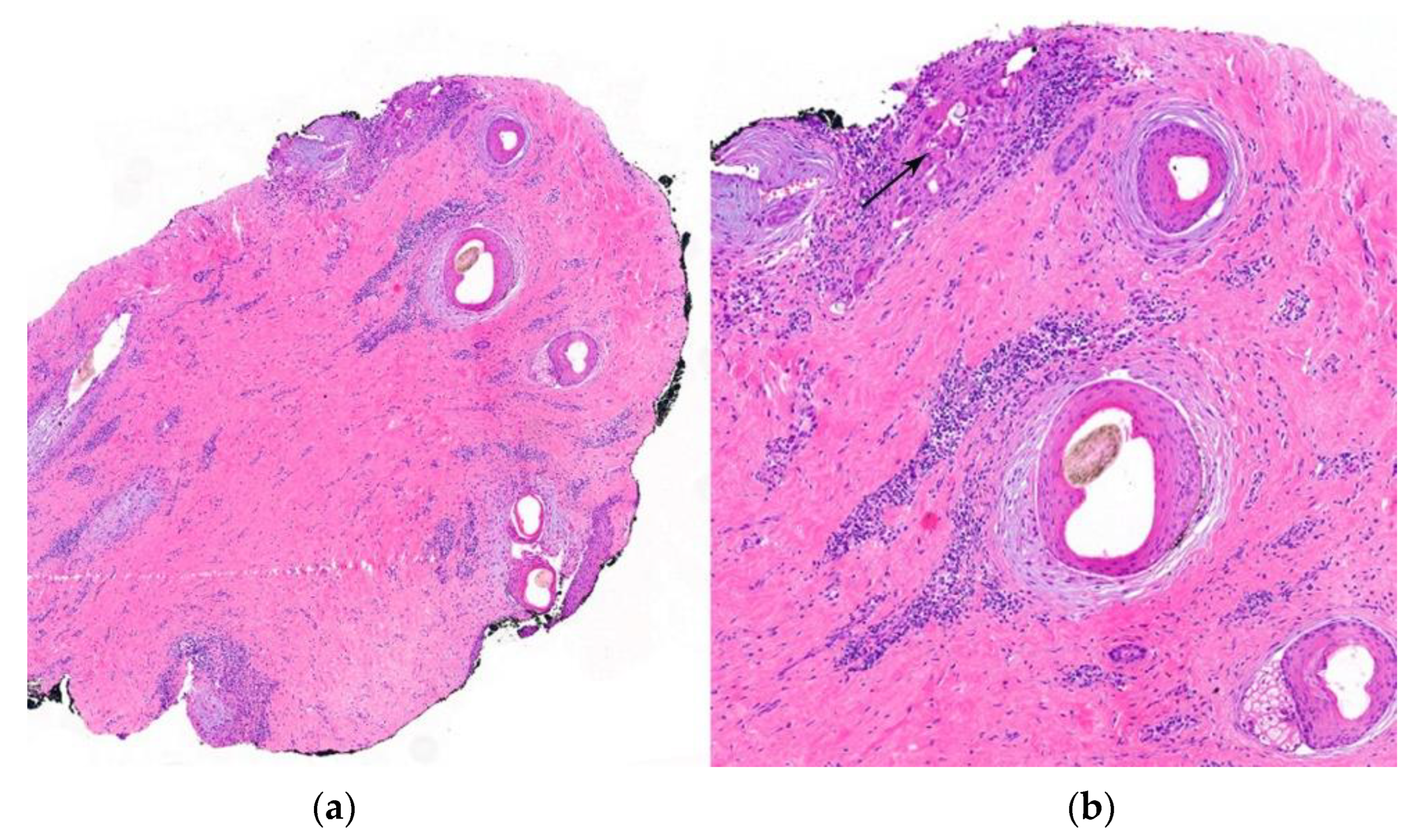
- Histological Findings (Figure 8):
- -
- Increase in the telogen index (>25% in initial phases).
- -
- Absence of inflammatory infiltrate.
- -
- Normal terminal and vellus hairs with an increase in follicular streamers in horizontal sections.
- -
- Differential diagnosis between chronic telogen effluvium and female pattern hair loss. In the former, the telogen/anagen ratio is 8:1; in the latter, it does not exceed 4:1.

- C.
- 1.
- Clinical Presentation:
- -
- Alopecia areata typically presents as patchy hair loss characterized by one or more circumscribed plaques on the scalp or other hair-bearing areas. The affected areas of the scalp usually exhibit underlying normal skin without any signs of inflammation or scarring.
- -
- One notable feature in alopecia areata is the presence of “exclamation mark” hairs. These are short, broken hairs that taper at the base and are commonly found at the borders of bald patches.
- -
- Can involve the whole scalp (total alopecia areata) or entire body (universal alopecia areata).
- 2.
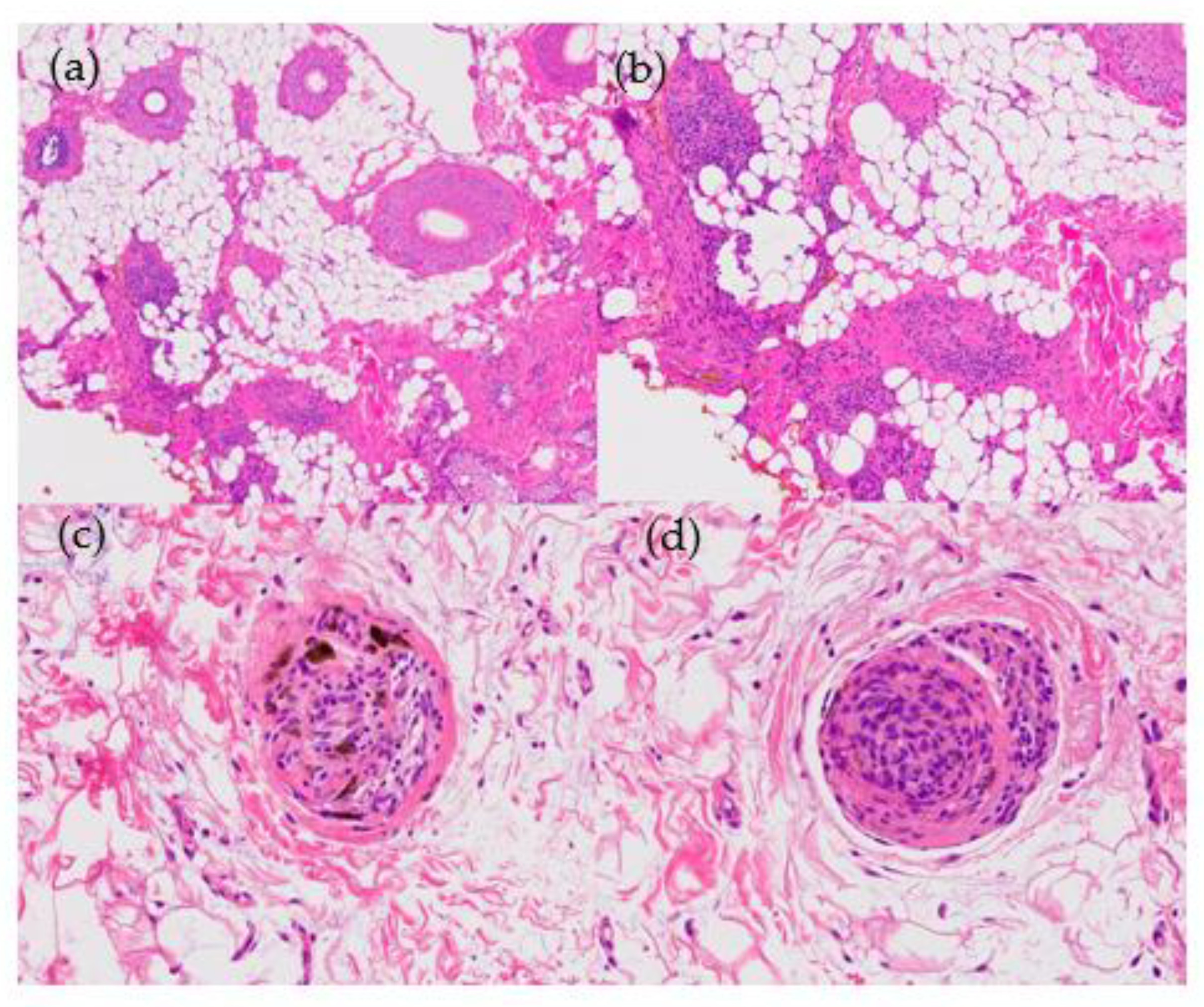
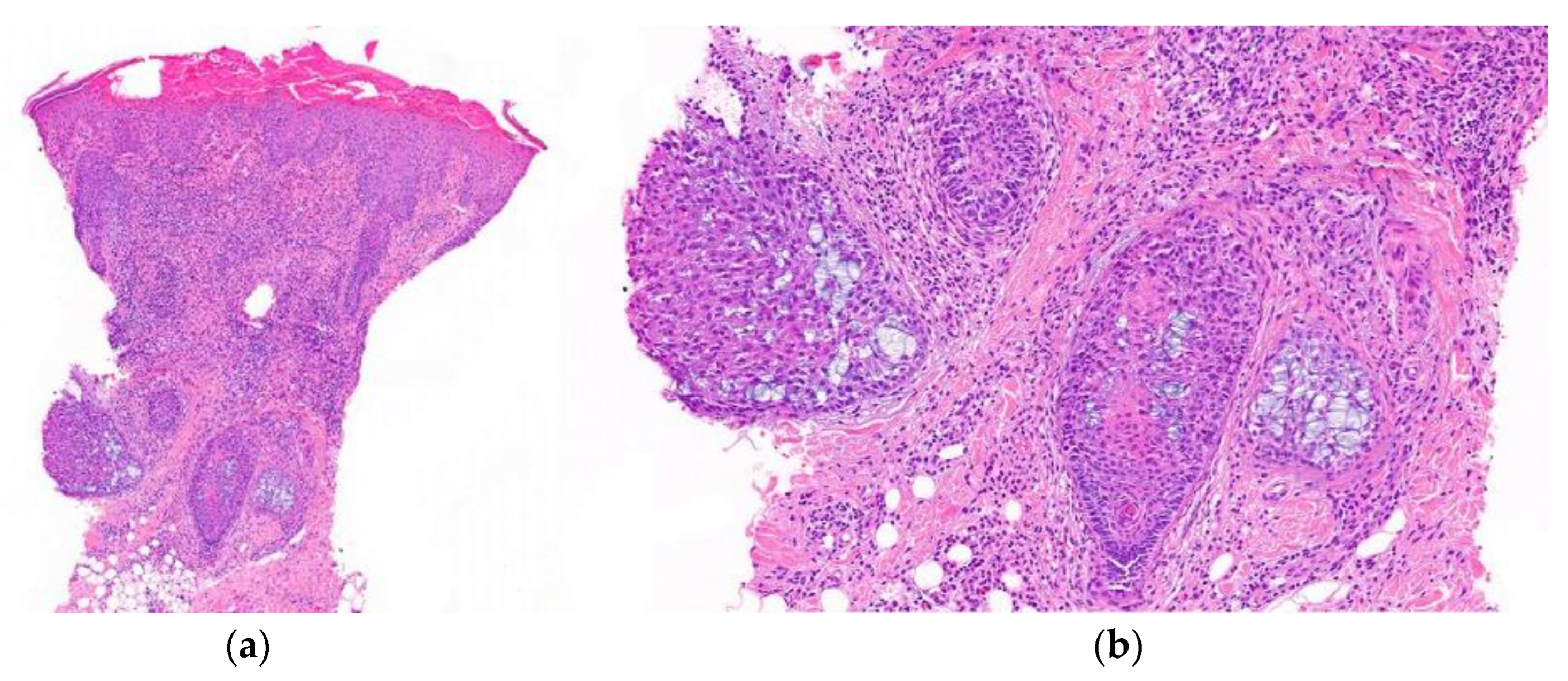
- Histological Features (Figure 9):
- -
- Peribulbar inflammatory infiltrate: during the active phase of alopecia areata, a characteristic peribulbar inflammatory infiltrate is seen around the anagen (growth) hair follicles (“swarm of bees”).
- -
- Apoptosis of matrix cells within the hair follicle can be observed.
- -
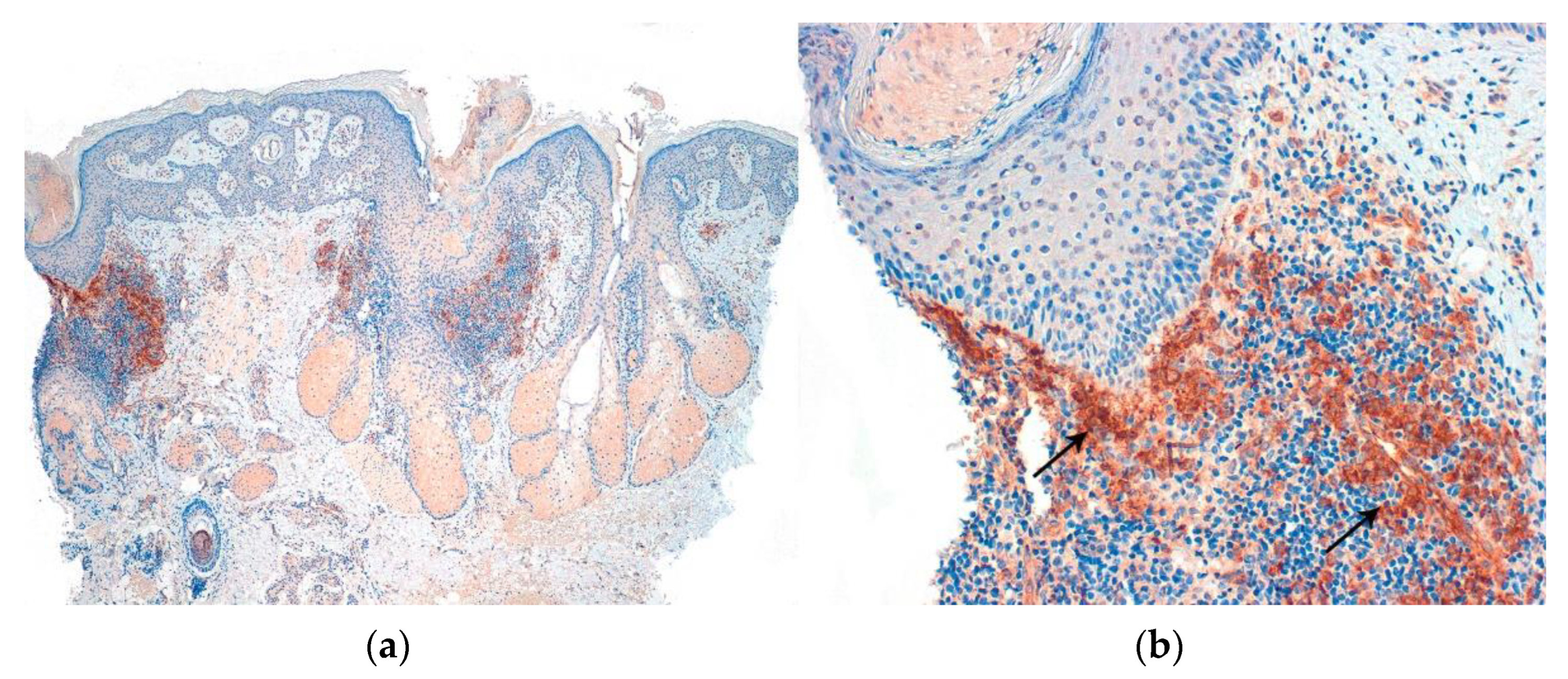
- Presence of lymphocytes, eosinophils, and melanin in follicular streamers (inactive phase). Utility of CD3 staining.
- -
- Increase in vellus index.
- -
- Increase in telogen index.

- D.
- 1.
- Clinical Presentation:
- -
- Trichotillomania is characterized by a compulsive tendency, whether conscious or unconscious, to pull and twist one’s own hair.
- -
- Atypical patches of alopecia—these patches are typically irregular in shape and may appear as areas of partial or complete hair loss.
- -
- Presence of different hair lengths within the affected areas; the remaining hairs may appear frayed or have a jagged, uneven appearance.
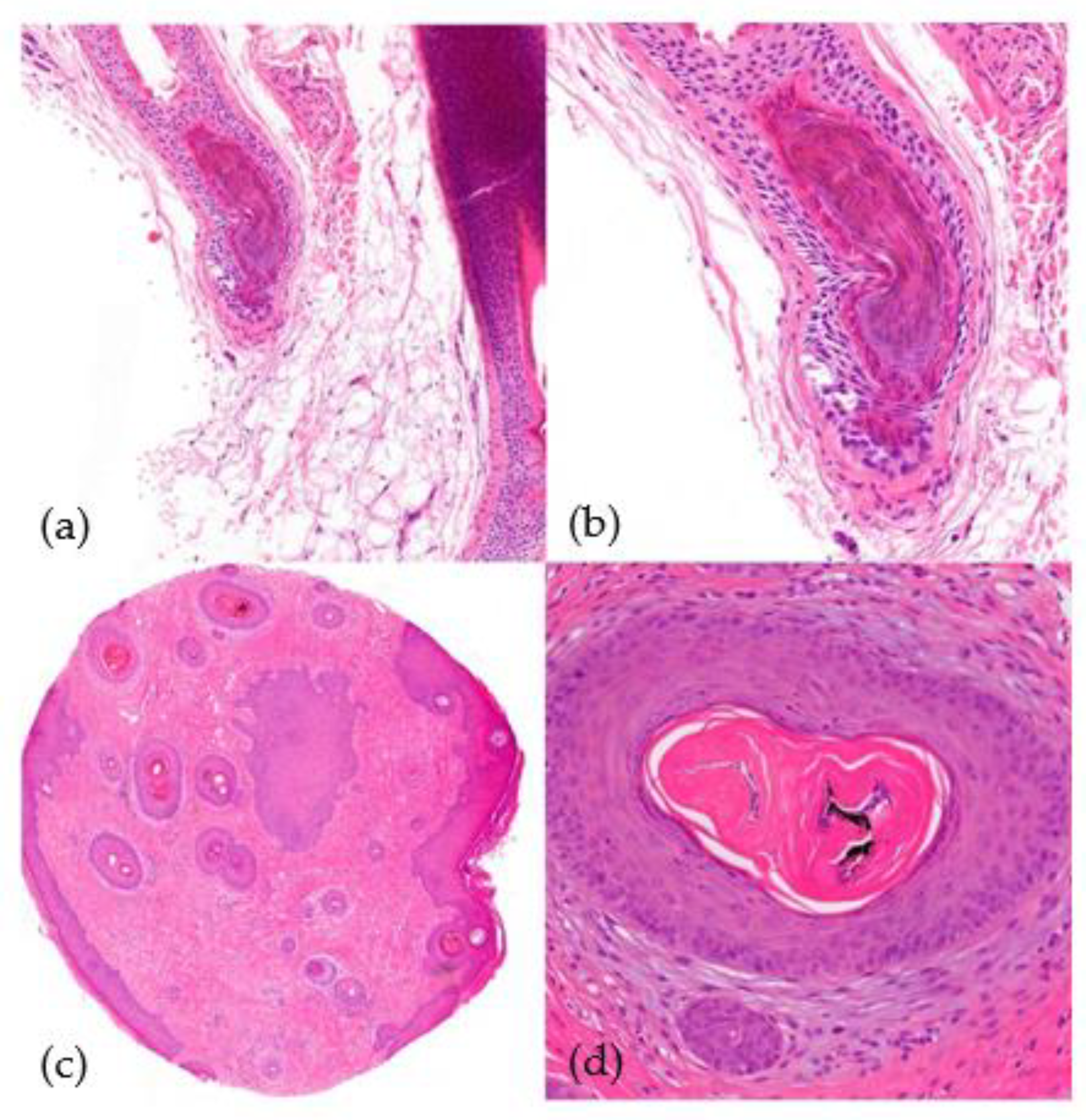
- 2.
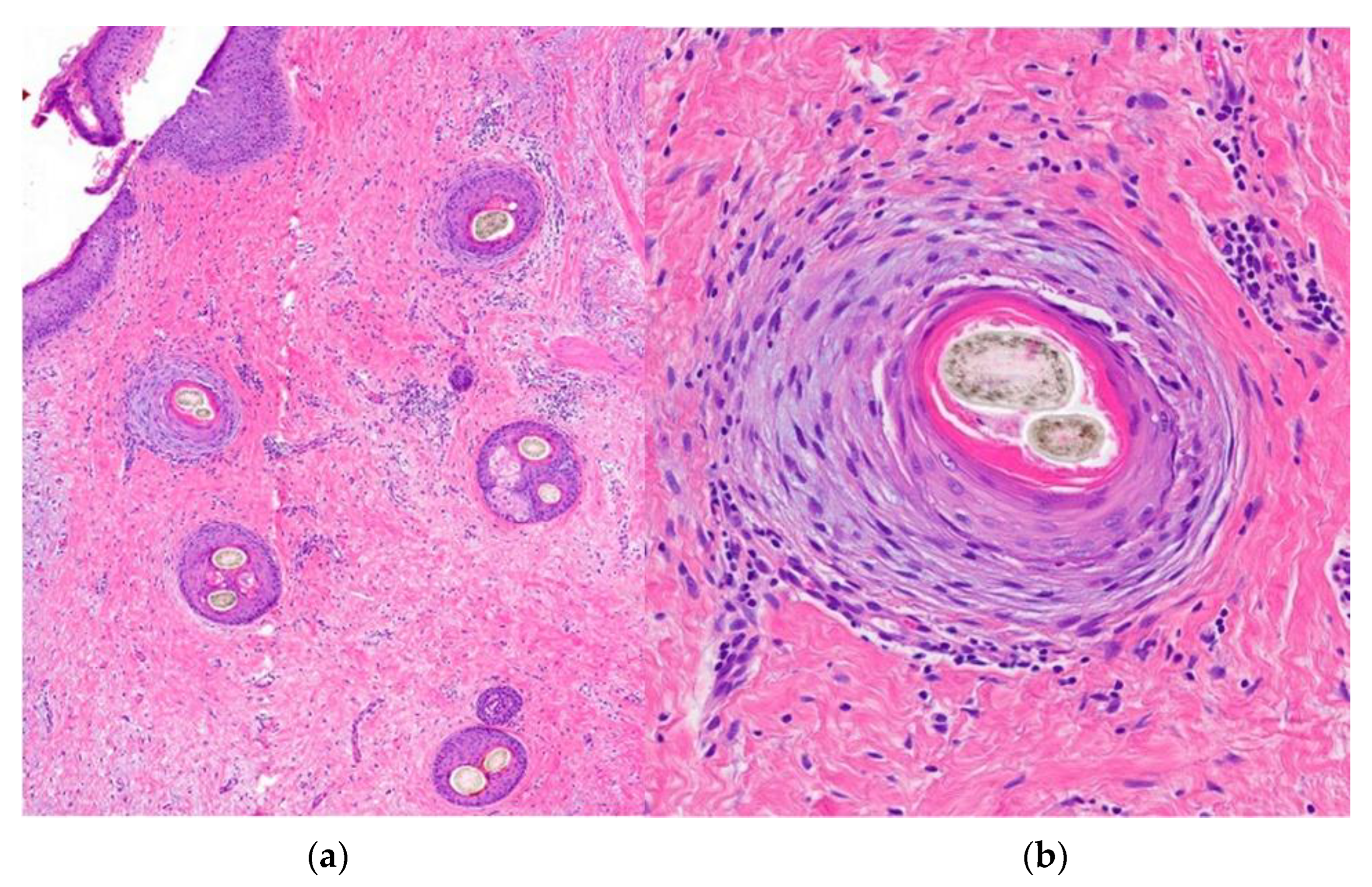
- Histological Findings (Figure 10):
- -
- Alternation of damaged and intact hair follicles.
- -
- Increased number of catagen hair follicles (>75%).
- -
- Bulbar epithelium distortion, hemorrhage, and pigmentary incontinence.
- -
- Trichomalacia (distortion of the hair shaft).

- E.
- 1.
- Clinical Findings:
- -
- Form of alopecia caused by excessive inappropriate hair styling.
- -
- Hair loss occurs in areas that experience the most traction, especially the temples (frequently seen among black people).
- -
- Over time, it may transform into a cicatricial alopecia (known as follicular degeneration syndrome).
- 2.
- Histological Features:
- -
- Similar to trichotillomania.
5.2. Scarring Alopecias [29]
5.2.1. Primary Scarring Alopecias [45,46]
Associated to Lymphocytic Infiltrate [49]
- A.
- 1.
- Clinical Presentation:
- -
- Affects approximately 50% of patients.
- -
- Middle-aged women; presenting as papules or erythematodesquamative plaques with associated pigmentary disorders, including hypo- and hyperpigmentation.
- -
- Follicular obliteration may occur.
- 2.
- Histological Features (Figure 11):
- -
- Hyperkeratosis predominantly involving the infundibulum of the hair follicle.
- -
- Vacuolar interface dermatitis; primarily affects the follicular epithelium and the dermoepidermal junction.
- -
- Presence of isolated Civatte’s bodies [51].
- -
- Superficial and deep perivascular and periadnexal lymphocytic infiltrate.
- -
- Pigmentary incontinence.
- -
- Increased dermal mucin.
- -
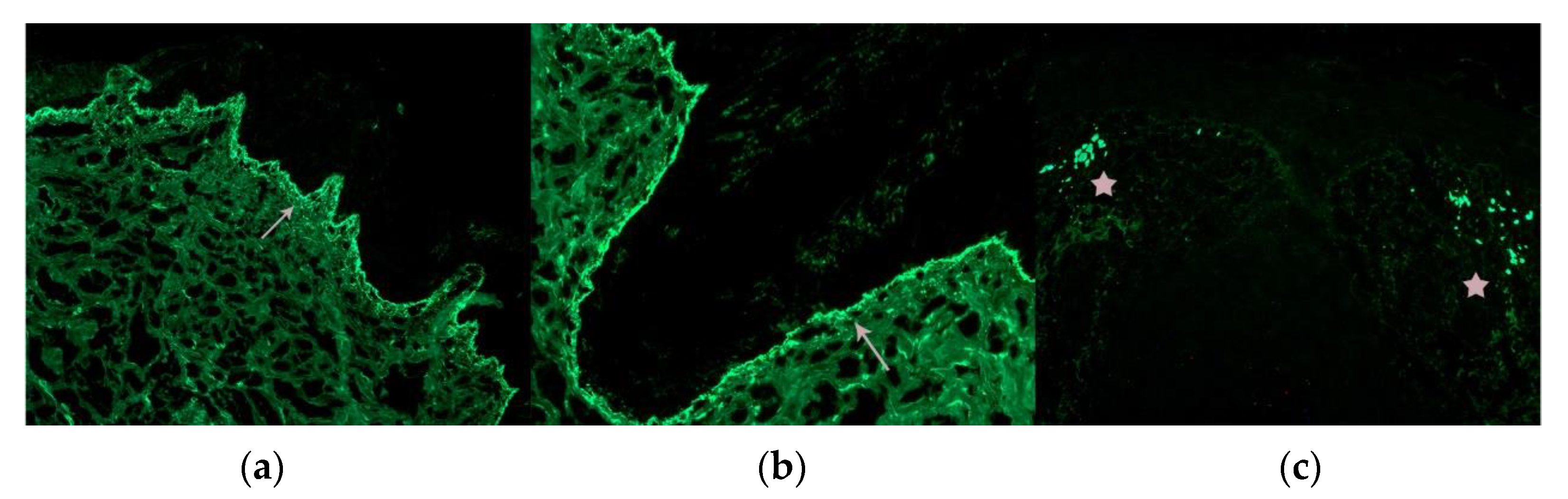
- Immunofluorescence (IFD) testing reveals a positive lupus band characterized by granular deposits of IgG, IgM, and/or C3 at the dermoepidermal junction and follicular epithelium.
- -
- Orcein staining reveals elastic fiber destruction throughout the entire dermis (advanced stages).

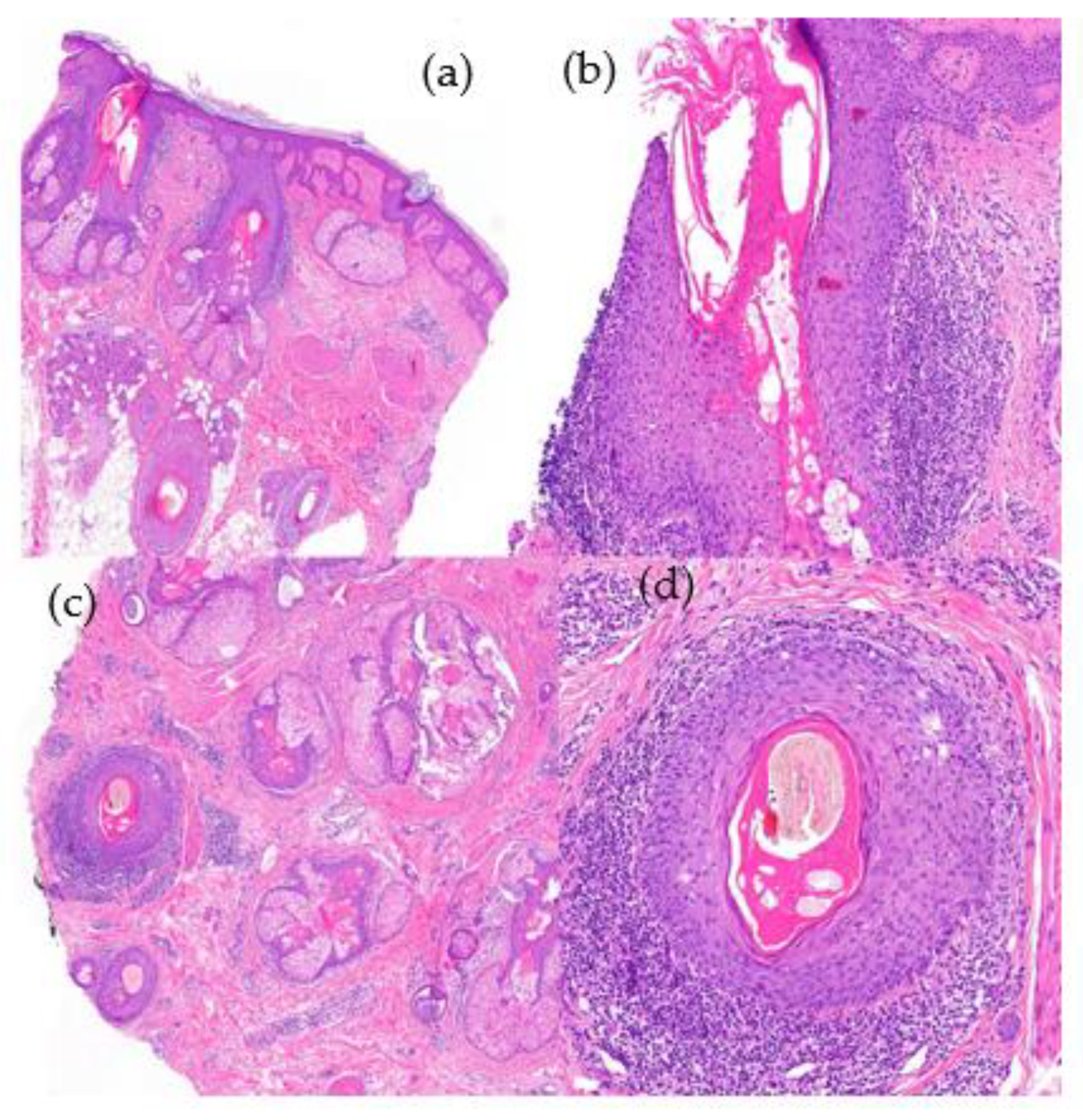
- B.
- Lichen planopilaris (LPP)
- B.1.
- 1.
- Clinical Presentation:
- -
- Atrophic plaques with perifollicular hyperkeratosis and erythema; affects middle-aged women more frequently than men.
- 2.
- Histological Features (Figure 12):
- -
- Hypergranulosis and infundibular hyperkeratosis.
- -
- Lichenoid interface dermatitis observed in the follicular epithelium, specifically the infundibulum and isthmus, as well as at the dermoepidermal junction.
- -
- Lymphocytic infiltration of the follicular epithelium.
- -
- Presence of abundant Civatte’s bodies (necrotic keratinocytes) within the follicular epithelium (detectable through positive cytokeratin staining) [51].
- -
- Concentric perifollicular fibrosis (advanced stages) with retraction clefts.
- -
- Orcein staining reveals a cradle cap scar centered around the follicle.
- -
- Immunofluorescence (IFD) testing is positive for IgM deposits in the follicular epithelium.
- -
- IFD: the abundant Civatte bodies are frequently positive for IgM.

- B.2.
- 1.
- Clinical Presentation:
- -
- Post-menopausal women but may be also seen in men and premenopausal women.
- -
- Regression of the frontemporal hairline and eyebrow loss.
- -
- Facial papules and in other body areas.
- 2.
- Histological Features:
- -
- Similar to classic LPP.
- -
- -
- “Follicular triad”—simultaneous involvement of terminal hair follicles, intermediate follicles, and vellus follicles at various stages of the hair follicle cycle (a key finding during the initial phases of the disease) [64].
- -
- Adipose infiltration of the arrector pili muscle and displacement of the eccrine glands [65].
- B.3.
- 1.
- Clinical Presentation:
- -
- Cicatricial alopecia of the scalp.
- -
- Presence of keratotic follicular papules on the trunk and extremities.
- -
- Reversible loss of pubic and/or axillary hair.
- 2.
- Histological Features:
- -
- Similar to that of LPP and FFA.
- B.4.
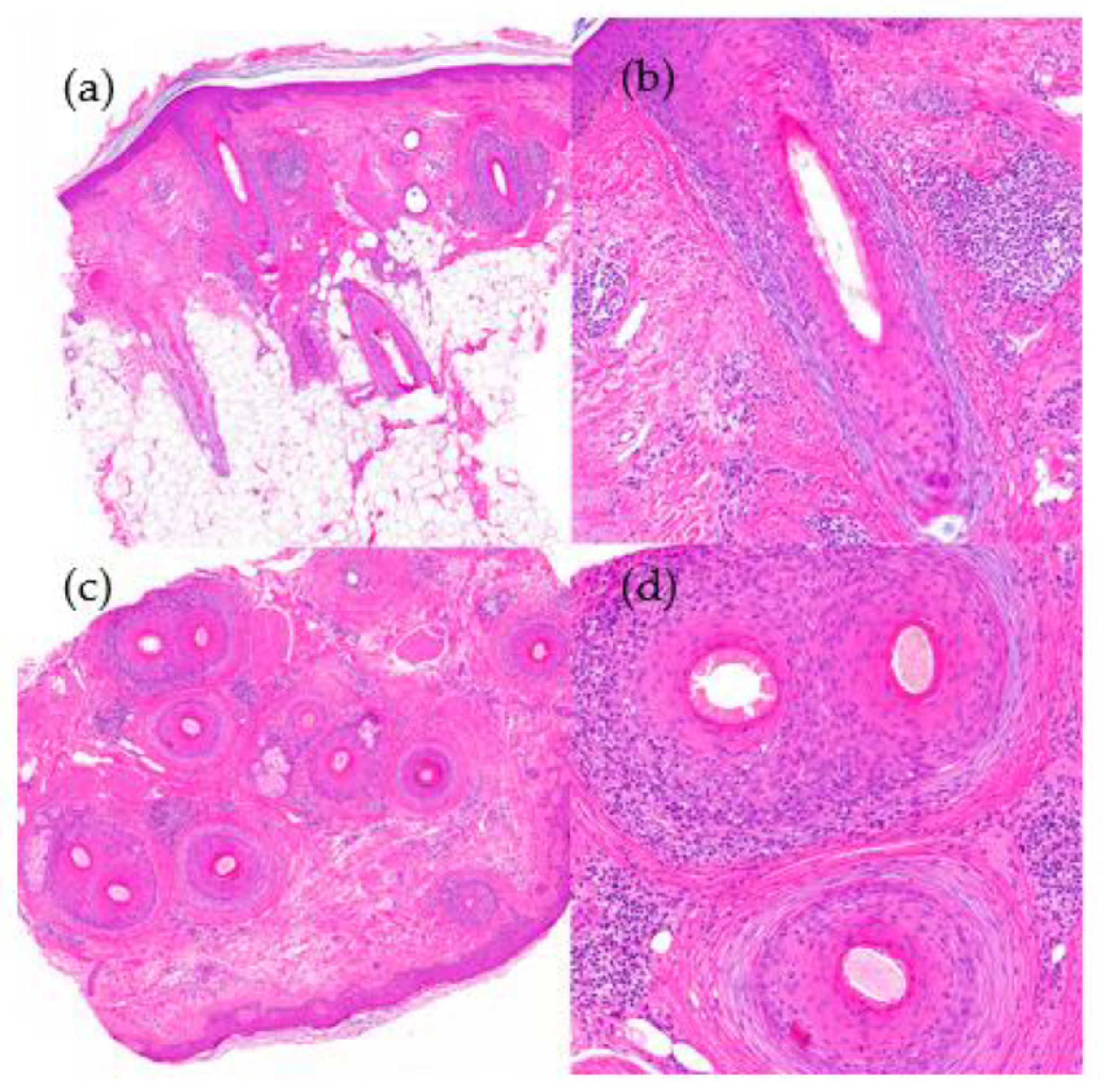
- Fibrosing alopecia in a pattern distribution (FAPD) [68]
- 1.
- Clinical Presentation:
- -
- Described by Zinkernagel an Trüeb in the year 2000 [69]; considered as an exaggerated inflammatory response to hair follicles affected by androgenetic alopecia.
- -
- It exhibits characteristics of both androgenetic alopecia and LPP.
- -
- Primarily affects the androgen-dependent areas of the scalp while sparing areas that are androgen-independent, such as the occipital region.
- -
- Perifollicular hyperkeratosis, loss of follicular ostium, and variation in hair shaft diameter are observed [70].
- 2.
- Histological Features (Figure 13):
- -
- Increase in vellus index (hair follicle miniaturization).
- -
- Lymphocytic perifollicular infiltrate (isthmus and infundibulum) with lamellar concentric perifollicular fibrosis [70].

- C.
- Pseudopelade of Brocq [50]
- 1.
- Clinical Features:
- -
- Middle-aged women with small alopecic plaques with normal underlying skin. These plaques have irregular borders and are devoid of keratotic papules or perifollicular erythema.
- -
- Primarily affects the vertex and parietal areas of the scalp.
- 2.
- Histological Features (Figure 14):
- -
- No definitive histological criteria have been described. No interface dermatitis is seen.
- -
- Concentric fibroplasia centered around the hair follicles.
- -
- Loss of sebaceous glands with preservation of the arrector pili muscle.
- -
- Granuloma formation around the naked hair follicles.
- -
- -
- IFD is negative.

- D.
- 1.
- Clinical Presentation: see definition. More commonly seen among black people.
- 2.
- Histological Features (Figure 15):
- -
- -
- Perifollicular lymphocytic infiltrate around the superior portion of the hair follicle.
- -
- Lamellar fibroplasia with sebaceous gland loss.
- -
- Atrophy of the follicular wall.
- -
- Duplication of hair shafts.
- -
- Premature desquamation of the internal root sheath (Giemsa staining).
- -
- Orcein staining: similar to pseudopelade of Brocq.

- E.
- 1.
- Clinical Presentation:
- -
- Predominant involvement of the head and neck in the form of grouped papules with a follicular distribution, erythematous patches, and/or fluctuating plaques, especially in the primary forms found in children and young adults [51].
- -
- Numerous lesions on the trunk and extremities can be seen in secondary forms and older patients.
- 2.
- Histological Features (Figure 16):
- -
- Follicular mucinosis: Mucin deposition initially affects the external root sheath and the infundibulum of the hair follicle [51]. In later stages, the entire hair follicle and sebaceous glands may be involved.
- -
- Lymphocytic infiltrate—there is a presence of lymphocytic infiltrate both peri and intrafollicularly.
- -
- Cytological atypia and monoclonal rearrangement in idiopathic and secondary forms.

- F.
- Keratosis follicularis spinulosa decalvans (KFSD) [80]
- 1.
- Clinical Presentation:
- -
- Patches of hair loss with follicular papules, hyperkeratosis, and pustules.
- 2.
- Histological Features [51]:
- -
- Abnormal keratinization with hypergranulosis and compact hyperkeratosis affecting the infundibulum, followed by spongiosis and neutrophilic infiltrate.
- -
- In later stages, chronic lymphocytic inflammation and fibrosis with a perifollicular distribution is observed.
- -
- In the final stages, destruction of the hair follicle with fibrosis and tricogranulomas can be observed.
Lichenoid Folliculitis
Associated to Neutrophilic Inflammation
- A.
- 1.
- Clinical Features:
- -
- Typically presents as alopecic patches with follicular pustules predominantly seen along the active borders.
- -
- More frequently around the crown, but it can also involve other regions, such as the beard, axilla, pubic area, arms, and legs.
- -
- Tufting, where multiple hairs emerge from a single hair follicle, is frequent.
- 2.
- Histological Features (Figure 17):
- -
- Infundibular dilation with peri- and intrafollicular neutrophilic infiltrate in early stages.
- -
- Polymorphous infiltrate in advanced stages (lymphocytes, plasma cells, histiocytes, and multinucleated giant cells).
- -
- Follicular loss and scarring.
- -
- Naked hair shafts.
- -
- Negative fungal stains (PAS, Grocott).
- -
- Involvement of the interfollicular dermis.

Mixed Primary Cicatricial Alopecias
5.2.2. Secondary Scarring Alopecia [83]
- A.
- Tinea capitis [84]
- 1.
- Clinical Features:
- -
- Common features include scaling, erythema (redness), and hair loss in the affected areas of the scalp.
- -
- Hair may appear brittle and broken, and there may be evidence of inflammation and crusting.
- 2.
- Histological Features (Figure 18):
- -
- Endothrix—fungi are found inside the hair shaft.
- -
- Ectothrix—fungi are seen around the hair shaft.
- -
- Polymorphous inflammatory infiltrate.
- -
- Damage of the follicular epithelium.
- -
- Positive fungal stains (PAS, Grocott).

5.3. Multifactorial Alopecias
6. Algorithms
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Triantafyllidi, H.; Grafakos, A.; Ikonomidis, I.; Pavlidis, G.; Trivilou, P.; Schoinas, A.; Lekakis, J. Severity of Alopecia Predicts Coronary Changes and Arterial Stiffness in Untreated Hypertensive Men. J. Clin. Hypertens. 2017, 19, 51–57. [Google Scholar] [CrossRef]
- He, H.; Xie, B.; Xie, L. Male Pattern Baldness and Incidence of Prostate Cancer: A Systematic Review and Meta-Analysis. Medicine 2018, 97, e11379. [Google Scholar] [CrossRef] [PubMed]
- Goren, A.; Vaño-Galván, S.; Wambier, C.G.; McCoy, J.; Gomez-Zubiaur, A.; Moreno-Arrones, O.M.; Shapiro, J.; Sinclair, R.D.; Gold, M.H.; Kovacevic, M.; et al. A Preliminary Observation: Male Pattern Hair Loss among Hospitalized COVID-19 Patients in Spain—A Potential Clue to the Role of Androgens in COVID-19 Severity. J. Cosmet. Dermatol. 2020, 19, 1545–1547. [Google Scholar] [CrossRef]
- Nguyen, B.; Tosti, A. Alopecia in Patients with COVID-19: A Systematic Review and Meta-Analysis. JAAD Int. 2022, 7, 67–77. [Google Scholar] [CrossRef]
- Buffoli, B.; Rinaldi, F.; Labanca, M.; Sorbellini, E.; Trink, A.; Guanziroli, E.; Rezzani, R.; Rodella, L.F. The Human Hair: From Anatomy to Physiology. Int. J. Dermatol. 2014, 53, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Bernárdez, C.; Molina-Ruiz, A.M.; Requena, L. Histopatología de las alopecias. Parte I: Alopecias no cicatriciales. Actas Dermo-Sifiliográficas 2015, 106, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Koch, S.L.; Tridico, S.R.; Bernard, B.A.; Shriver, M.D.; Jablonski, N.G. The Biology of Human Hair: A Multidisciplinary Review. Am. J. Hum. Biol. 2020, 32, e23316. [Google Scholar] [CrossRef] [PubMed]
- Park, A.M.; Khan, S.; Rawnsley, J. Hair Biology: Growth and Pigmentation. Facial Plast. Surg. Clin. N. Am. 2018, 26, 415–424. [Google Scholar] [CrossRef]
- Moreno, C.; Requena, C.; Requena, L. Embriología, histología y fisiología del foliculo piloso. In Neoplasias Anexiales Cutáneas; Grupo Aula Médica: Madrid, Spain, 2004; pp. 185–201. [Google Scholar]
- Restrepo, R.; Calonje, E.E. Diseases of the hair. In McKee’s Pathology of the Skin with Clinical Correlations; Elsevier: London, UK, 2012; Volume 22, pp. 967–1050. [Google Scholar]
- Ackerman, A.B. An algorithmic method based on pattern analysis. In Histologic Diagnosis of Inflammatory Skin Diseases; Ardor Scribendi: New York, NY, USA, 2005. [Google Scholar]
- Hordinsky, M. Scarring Alopecia: Diagnosis and New Treatment Options. Dermatol. Clin. 2021, 39, 383–388. [Google Scholar] [CrossRef]
- Elston, D.M.; McCollough, M.L.; Angeloni, V.L. Vertical and Transverse Sections of Alopecia Biopsy Specimens: Combining the Two to Maximize Diagnostic Yield. J. Am. Acad. Dermatol. 1995, 32, 454–457. [Google Scholar] [CrossRef]
- Elston, D.M.; Ferringer, T.; Dalton, S.; Fillman, E.; Tyler, W. A Comparison of Vertical versus Transverse Sections in the Evaluation of Alopecia Biopsy Specimens. J. Am. Acad. Dermatol. 2005, 53, 267–272. [Google Scholar] [CrossRef]
- Stefanato, C.M. Histopathology of Alopecia: A Clinicopathological Approach to Diagnosis. Histopathology 2010, 56, 24–38. [Google Scholar] [CrossRef]
- Trachsler, S.; Trueb, R.M. Value of Direct Immunofluorescence for Differential Diagnosis of Cicatricial Alopecia. Dermatology 2005, 211, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Headington, J.T. Transverse Microscopic Anatomy of the Human Scalp. A Basis for a Morphometric Approach to Disorders of the Hair Follicle. Arch. Dermatol. 1984, 120, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Frishberg, D.P.; Sperling, L.C.; Guthrie, V.M. Transverse Scalp Sections: A Proposed Method for Laboratory Processing. J. Am. Acad. Dermatol. 1996, 35, 220–222. [Google Scholar] [CrossRef] [PubMed]
- LaSenna, C.; Miteva, M. Special Stains and Immunohistochemical Stains in Hair Pathology. Am. J. Dermatopathol. 2016, 38, 327–337. [Google Scholar] [CrossRef]
- Fung, M.A.; Sharon, V.R.; Ratnarathorn, M.; Konia, T.H.; Barr, K.L.; Mirmirani, P. Elastin Staining Patterns in Primary Cicatricial Alopecia. J. Am. Acad. Dermatol. 2013, 69, 776–782. [Google Scholar] [CrossRef]
- Miteva, M.; Tosti, A. Polarized Microscopy as a Helpful Tool to Distinguish Chronic Nonscarring Alopecia from Scarring Alopecia. Arch. Dermatol. 2012, 148, 91–94. [Google Scholar] [CrossRef]
- Kolivras, A.; Thompson, C. Primary Scalp Alopecia: New Histopathological Tools, New Concepts and a Practical Guide to Diagnosis. J. Cutan. Pathol. 2017, 44, 53–69. [Google Scholar] [CrossRef]
- Kamyab, K.; Rezvani, M.; Seirafi, H.; Mortazavi, S.; Teymourpour, A.; Abtahi, S.; Nasimi, M. Distinguishing Immunohistochemical Features of Alopecia Areata from Androgenic Alopecia. J. Cosmet. Dermatol. 2019, 18, 422–426. [Google Scholar] [CrossRef]
- Fening, K.; Parekh, V.; McKay, K. CD123 Immunohistochemistry for Plasmacytoid Dendritic Cells Is Useful in the Diagnosis of Scarring Alopecia. J. Cutan. Pathol. 2016, 43, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, S.; Tirumalae, R.; Inchara, Y.K. Plasmacytoid Dendritic Cell Marker (CD123) Expression in Scarring and Non-Scarring Alopecia. J. Cutan. Aesthetic Surg. 2022, 15, 179–182. [Google Scholar] [CrossRef]
- Nguyen, J.V.; Hudacek, K.; Whitten, J.A.; Rubin, A.I.; Seykora, J.T. The HoVert Technique: A Novel Method for the Sectioning of Alopecia Biopsies. J. Cutan. Pathol. 2011, 38, 401–406. [Google Scholar] [CrossRef]
- Wain, E.M.; Stefanato, C.M. Four Millimetres: A Variable Measurement? Br. J. Dermatol. 2007, 156, 404. [Google Scholar] [CrossRef]
- Adams, L.; Amphlett, A.; Gardette, E.; Deroide, F.; Jones, J. The Modified HoVert (MHoVert) Method Improves Diagnostic Certainty Compared to the St John’s Protocol for Alopecia Biopsy Specimens: A Retrospective Single Center Study. J. Cutan. Pathol. 2023. [Google Scholar] [CrossRef]
- Sellheyer, K.; Bergfeld, W.F. Histopathologic Evaluation of Alopecias. Am. J. Dermatopathol. 2006, 28, 236–259. [Google Scholar] [CrossRef]
- Price, V.H. Androgenetic Alopecia in Women. J. Investig. Dermatol. Symp. Proc. 2003, 8, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, V.N.; Aggarwal, A.K.; Srivastava, G.; Rajput, P. Male Pattern Androgenetic Alopecia. Skinmed 2006, 5, 128–135. [Google Scholar] [CrossRef]
- Piraccini, B.M.; Alessandrini, A. Androgenetic Alopecia. G Ital. Dermatol. Venereol. 2014, 149, 15–24. [Google Scholar]
- Rebora, A. Telogen Effluvium: A Comprehensive Review. Clin. Cosmet. Investig. Dermatol. 2019, 12, 583–590. [Google Scholar] [CrossRef]
- Werner, B.; Mulinari-Brenner, F. Clinical and Histological Challenge in the Differential Diagnosis of Diffuse Alopecia: Female Androgenetic Alopecia, Telogen Effluvium and Alopecia Areata—Part I. An. Bras. Dermatol. 2012, 87, 742–747. [Google Scholar] [CrossRef]
- Zhou, C.; Li, X.; Wang, C.; Zhang, J. Alopecia Areata: An Update on Etiopathogenesis, Diagnosis, and Management. Clin. Rev. Allergy Immunol. 2021, 61, 403–423. [Google Scholar] [CrossRef] [PubMed]
- Pratt, C.H.; King, L.E.; Messenger, A.G.; Christiano, A.M.; Sundberg, J.P. Alopecia Areata. Nat. Rev. Dis. Primers 2017, 3, 17011. [Google Scholar] [CrossRef] [PubMed]
- Simakou, T.; Butcher, J.P.; Reid, S.; Henriquez, F.L. Alopecia Areata: A Multifactorial Autoimmune Condition. J. Autoimmun. 2019, 98, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Hautmann, G.; Hercogova, J.; Lotti, T. Trichotillomania. J. Am. Acad. Dermatol. 2002, 46, 807–826. [Google Scholar] [CrossRef]
- Thakur, B.K.; Verma, S.; Raphael, V.; Khonglah, Y. Extensive Tonsure Pattern Trichotillomania-Trichoscopy and Histopathology Aid to the Diagnosis. Int. J. Trichology 2013, 5, 196–198. [Google Scholar] [CrossRef] [PubMed]
- Muller, S.A. Trichotillomania: A Histopathologic Study in Sixty-Six Patients. J. Am. Acad. Dermatol. 1990, 23, 56–62. [Google Scholar] [CrossRef]
- Donovan, J.C.; Mirmirani, P. Transversely Sectioned Biopsies in the Diagnosis of End-Stage Traction Alopecia. Dermatol. Online J. 2013, 19, 11. [Google Scholar]
- Ngwanya, R.M.; Adeola, H.A.; Beach, R.A.; Gantsho, N.; Walker, C.L.; Pillay, K.; Prokopetz, R.; Gumedze, F.; Khumalo, N.P. Reliability of Histopathology for the Early Recognition of Fibrosis in Traction Alopecia: Correlation with Clinical Severity. Dermatopathology 2019, 6, 170–181. [Google Scholar] [CrossRef]
- Samrao, A.; Mirmirani, P. Postpartum Telogen Effluvium Unmasking Traction Alopecia. Skin. Appendage Disord. 2022, 8, 328–332. [Google Scholar] [CrossRef]
- Olsen, E.A.; Bergfeld, W.F.; Cotsarelis, G.; Price, V.H.; Shapiro, J.; Sinclair, R.; Solomon, A.; Sperling, L.; Stenn, K.; Whiting, D.A.; et al. Summary of North American Hair Research Society (NAHRS)-Sponsored Workshop on Cicatricial Alopecia, Duke University Medical Center, February 10 and 11, 2001. J. Am. Acad. Dermatol. 2003, 48, 103–110. [Google Scholar] [CrossRef]
- Uchiyama, M. Primary Cicatricial Alopecia: Recent Advances in Evaluation and Diagnosis Based on Trichoscopic and Histopathological Observation, Including Overlapping and Specific Features. J. Dermatol. 2022, 49, 37–54. [Google Scholar] [CrossRef]
- Somani, N.; Bergfeld, W.F. Cicatricial Alopecia: Classification and Histopathology. Dermatol. Ther. 2008, 21, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.; Guitart, J.; Gerami, P.; Yazdan, P. Eccrine Duct Dilation as a Marker of Cicatricial Alopecia. Am. J. Dermatopathol. 2017, 39, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.L.; Doytcheva, K.; Guitart, J.; Gerami, P.; Yazdan, P. Dilation of Multiple Eccrine Ducts as a Highly Specific Marker for Cicatricial Alopecia. Am. J. Dermatopathol. 2019, 41, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Bolduc, C.; Sperling, L.C.; Shapiro, J. Primary Cicatricial Alopecia: Lymphocytic Primary Cicatricial Alopecias, Including Chronic Cutaneous Lupus Erythematosus, Lichen Planopilaris, Frontal Fibrosing Alopecia, and Graham-Little Syndrome. J. Am. Acad. Dermatol. 2016, 75, 1081–1099. [Google Scholar] [CrossRef]
- Sperling, L.C.; Cowper, S.E. The Histopathology of Primary Cicatricial Alopecia. Semin. Cutan. Med. Surg. 2006, 25, 41–50. [Google Scholar] [CrossRef]
- Bernárdez, C.; Molina-Ruiz, A.M.; Requena, L. Histopatología de las alopecias. Parte II: Alopecias cicatriciales. Actas Dermo-Sifiliográficas 2015, 106, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Vañó-Galván, S.; Saceda-Corralo, D.; Moreno-Arrones, Ó.M.; Camacho-Martinez, F.M. Updated Diagnostic Criteria for Frontal Fibrosing Alopecia. J. Am. Acad. Dermatol. 2018, 78, e21–e22. [Google Scholar] [CrossRef]
- Poblet, E.; Jiménez, F.; Pascual, A.; Piqué, E. Frontal Fibrosing Alopecia versus Lichen Planopilaris: A Clinicopathological Study. Int. J. Dermatol. 2006, 45, 375–380. [Google Scholar] [CrossRef]
- Esteban-Lucía, L.; Molina-Ruiz, A.M.; Requena, L. Update on Frontal Fibrosing Alopecia. Actas Dermosifiliogr. 2017, 108, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Porriño-Bustamante, M.L.; Fernández-Pugnaire, M.A.; Arias-Santiago, S. Frontal Fibrosing Alopecia: A Review. J. Clin. Med. 2021, 10, 1805. [Google Scholar] [CrossRef]
- Chew, A.-L.; Bashir, S.J.; Wain, E.M.; Fenton, D.A.; Stefanato, C.M. Expanding the Spectrum of Frontal Fibrosing Alopecia: A Unifying Concept. J. Am. Acad. Dermatol. 2010, 63, 653–660. [Google Scholar] [CrossRef]
- Porriño-Bustamante, M.L.; Montero-Vílchez, T.; Pinedo-Moraleda, F.J.; Fernández-Flores, Á.; Fernández-Pugnaire, M.A.; Arias-Santiago, S. Frontal Fibrosing Alopecia and Sunscreen Use: A Cross-Sectional Study of Actinic Damage. Acta Derm. Venereol. 2022, 102, adv00757. [Google Scholar] [CrossRef] [PubMed]
- Porriño-Bustamante, M.L.; Pinedo-Moraleda, F.J.; Fernández-Flores, Á.; Montero-Vílchez, T.; Fernández-Pugnaire, M.A.; Arias-Santiago, S. Frontal Fibrosing Alopecia: A Histopathological Comparison of the Frontal Hairline with Normal-Appearing Scalp. J. Clin. Med. 2022, 11, 4121. [Google Scholar] [CrossRef]
- Donati, A.; Molina, L.; Doche, I.; Valente, N.S.; Romiti, R. Facial Papules in Frontal Fibrosing Alopecia: Evidence of Vellus Follicle Involvement. Arch. Dermatol. 2011, 147, 1424–1427. [Google Scholar] [CrossRef] [PubMed]
- López-Pestaña, A.; Tuneu, A.; Lobo, C.; Ormaechea, N.; Zubizarreta, J.; Vildosola, S.; Del Alcazar, E. Facial Lesions in Frontal Fibrosing Alopecia (FFA): Clinicopathological Features in a Series of 12 Cases. J. Am. Acad. Dermatol. 2015, 73, 987.e1–987.e6. [Google Scholar] [CrossRef]
- Rakhshan, A.; Momenpour, N.; Dadkhahfar, S.; Gheisari, M. Histopathological and Immunohistochemical Features of Facial Papules in Frontal Fibrosing Alopecia. Clin. Exp. Dermatol. 2021, 46, 1248–1254. [Google Scholar] [CrossRef]
- Fernandez-Flores, A.; Manjón, J.A. Histopathology of Keratotic Papules of the Limbs in Frontal Fibrosing Alopecia. J. Cutan. Pathol. 2016, 43, 468–471. [Google Scholar] [CrossRef]
- Miteva, M. Frontal Fibrosing Alopecia Involving the Limbs Shows Inflammatory Pattern on Histology: A Review of 13 Cases. Am. J. Dermatopathol. 2020, 42, 226–229. [Google Scholar] [CrossRef]
- Miteva, M.; Tosti, A. The Follicular Triad: A Pathological Clue to the Diagnosis of Early Frontal Fibrosing Alopecia. Br. J. Dermatol. 2012, 166, 440–442. [Google Scholar] [CrossRef]
- Miteva, M.; Castillo, D.; Sabiq, S. Adipose Infiltration of the Dermis, Involving the Arrector Pili Muscle, and Dermal Displacement of Eccrine Sweat Coils: New Histologic Observations in Frontal Fibrosing Alopecia. Am. J. Dermatopathol. 2019, 41, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, M.; Mikkilineni, R.; Konstadt, J. Lassueur-Graham-Little-Piccardi Syndrome. Dermatol. Online J. 2007, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- László, F.G. Graham-Little-Piccardi-Lasseur Syndrome: Case Report and Review of the Syndrome in Men. Int. J. Dermatol. 2014, 53, 1019–1022. [Google Scholar] [CrossRef] [PubMed]
- Jerjen, R.; Pinczewski, J.; Sinclair, R.; Bhoyrul, B. Clinicopathological Characteristics and Treatment Outcomes of Fibrosing Alopecia in a Pattern Distribution: A Retrospective Cohort Study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2440–2447. [Google Scholar] [CrossRef] [PubMed]
- Zinkernagel, M.S.; Trüeb, R.M. Fibrosing Alopecia in a Pattern Distribution: Patterned Lichen Planopilaris or Androgenetic Alopecia with a Lichenoid Tissue Reaction Pattern? Arch. Dermatol. 2000, 136, 205–211. [Google Scholar] [CrossRef]
- Griggs, J.; Trüeb, R.M.; Gavazzoni Dias, M.F.R.; Hordinsky, M.; Tosti, A. Fibrosing Alopecia in a Pattern Distribution. J. Am. Acad. Dermatol. 2021, 85, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Brocq, L. Alopecia. J. Cutan. Vener. Dis. 1885, 3, 49–50. [Google Scholar]
- Silvers, D.N.; Katz, B.E.; Young, A.W. Pseudopelade of Brocq Is Lichen Planopilaris: Report of Four Cases That Support This Nosology. Cutis 1993, 51, 99–105. [Google Scholar]
- Amato, L.; Mei, S.; Massi, D.; Gallerani, I.; Fabbri, P. Cicatricial Alopecia; a Dermatopathologic and Immunopathologic Study of 33 Patients (Pseudopelade of Brocq Is Not a Specific Clinico-Pathologic Entity). Int. J. Dermatol. 2002, 41, 8–15. [Google Scholar] [CrossRef]
- Baeza-Hernández, G.; Jaquero-Valero, M.I.; Rubio-Aguilera, R.F.; Araya-Umaña, L.C.; Horcajada-Reales, C.; Moreno-Torres, A. Elastic Stain in Pseudopelade of Brocq: A Helpful Histopathological Diagnostic Clue. Dermatol. Pract. Concept. 2023, 13, e2023088. [Google Scholar] [CrossRef]
- Roche, F.C.; Fischer, A.S.; Williams, D.; Ogunleye, T.; Seykora, J.T.; Taylor, S.C. Central Centrifugal Cicatricial Alopecia: Histologic Progression Correlates with Advancing Age. J. Am. Acad. Dermatol. 2022, 86, 178–179. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.W.; Motaparthi, K.; Hsu, S. Central Centrifugal Cicatricial Alopecia and Lichen Planopilaris Can Look Identical on Histopathology. Skinmed 2020, 18, 365–366. [Google Scholar] [PubMed]
- Hooper, K.K.; Smoller, B.R.; Brown, J.A. Idiopathic Follicular Mucinosis or Mycosis Fungoides? Classification and Diagnostic Challenges. Cutis 2015, 95, E9–E14. [Google Scholar]
- Khalil, J.; Kurban, M.; Abbas, O. Follicular Mucinosis: A Review. Int. J. Dermatol. 2021, 60, 159–165. [Google Scholar] [CrossRef]
- Vignon-Pennamen, M.-D. Groupe d’histopathologie cutanée de la Société franc¸aise de dermatologie [Follicular mucinosis]. Ann. Dermatol. Venereol. 2011, 138, 707–709. [Google Scholar] [CrossRef] [PubMed]
- Bellet, J.S.; Kaplan, A.L.; Selim, M.A.; Olsen, E.A. Keratosis Follicularis Spinulosa Decalvans in a Family. J. Am. Acad. Dermatol. 2008, 58, 499–502. [Google Scholar] [CrossRef]
- Uchiyama, M.; Harada, K.; Tobita, R.; Irisawa, R.; Tsuboi, R. Histopathologic and Dermoscopic Features of 42 Cases of Folliculitis Decalvans: A Case Series. J. Am. Acad. Dermatol. 2021, 85, 1185–1193. [Google Scholar] [CrossRef]
- Rossi, A.; Garelli, V.; Muscianese, M.; Pranteda, G.; Caro, G.; D’Arino, A.; Fortuna, M.C. Clinical and Trichoscopic Correlation of Primary Neutrophilic Scarring Alopecia: Folliculitis Decalvans and Dissecting Cellulitis. G. Ital. Dermatol. Venereol. 2020, 155, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Nanda, S.; De Bedout, V.; Miteva, M. Alopecia as a Systemic Disease. Clin. Dermatol. 2019, 37, 618–628. [Google Scholar] [CrossRef]
- Elmas, Ö.F.; Durdu, M. Histopathology in the Diagnosis of Tinea Capitis: When to Do, How to Interpret? Mycopathologia 2023. [Google Scholar] [CrossRef] [PubMed]
- Wohltmann, W.E.; Sperling, L. Histopathologic Diagnosis of Multifactorial Alopecia. J. Cutan. Pathol. 2016, 43, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Eudy, G.; Solomon, A.R. The Histopathology of Noncicatricial Alopecia. Semin. Cutan. Med. Surg. 2006, 25, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Kanti, V.; Röwert-Huber, J.; Vogt, A.; Blume-Peytavi, U. Cicatricial Alopecia. J. Dtsch. Dermatol. Ges. 2018, 16, 435–461. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinedo-Moraleda, F.; Tristán-Martín, B.; Dradi, G.G. Alopecias: Practical Tips for the Management of Biopsies and Main Diagnostic Clues for General Pathologists and Dermatopathologists. J. Clin. Med. 2023, 12, 5004. https://doi.org/10.3390/jcm12155004
Pinedo-Moraleda F, Tristán-Martín B, Dradi GG. Alopecias: Practical Tips for the Management of Biopsies and Main Diagnostic Clues for General Pathologists and Dermatopathologists. Journal of Clinical Medicine. 2023; 12(15):5004. https://doi.org/10.3390/jcm12155004
Chicago/Turabian StylePinedo-Moraleda, Fernando, Belén Tristán-Martín, and Giulia Greta Dradi. 2023. "Alopecias: Practical Tips for the Management of Biopsies and Main Diagnostic Clues for General Pathologists and Dermatopathologists" Journal of Clinical Medicine 12, no. 15: 5004. https://doi.org/10.3390/jcm12155004
APA StylePinedo-Moraleda, F., Tristán-Martín, B., & Dradi, G. G. (2023). Alopecias: Practical Tips for the Management of Biopsies and Main Diagnostic Clues for General Pathologists and Dermatopathologists. Journal of Clinical Medicine, 12(15), 5004. https://doi.org/10.3390/jcm12155004