

Intraoperative Hemodynamics of Parasylvian Cortical Arteries for Predicting Postoperative Symptomatic Cerebral Hyperperfusion after Direct Revascularization in Patients with Moyamoya Disease: A Preliminary Study


Abstract
1. Introduction
2. Methods
Patient Selection
3. Data Collection and Analysis
3.1. Hemispheric Perfusion Analysis
3.2. Angiographic Analysis
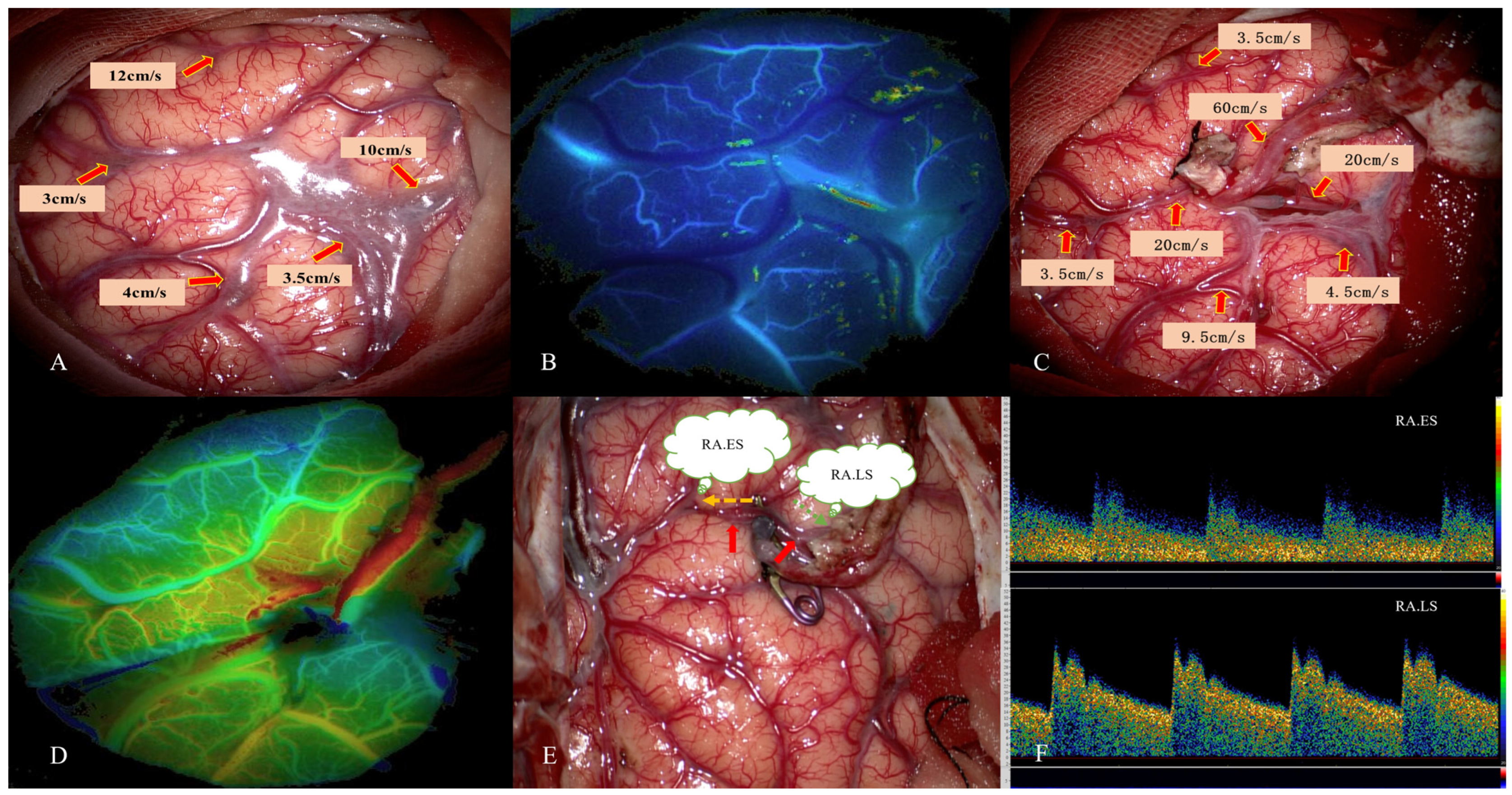
3.3. Data Collection and Analysis of MDU
3.4. Definition of Symptomatic CHS
4. Statistical Analysis
5. Results
5.1. Patient Characteristics
5.2. MDU Findings in Cases with CHS
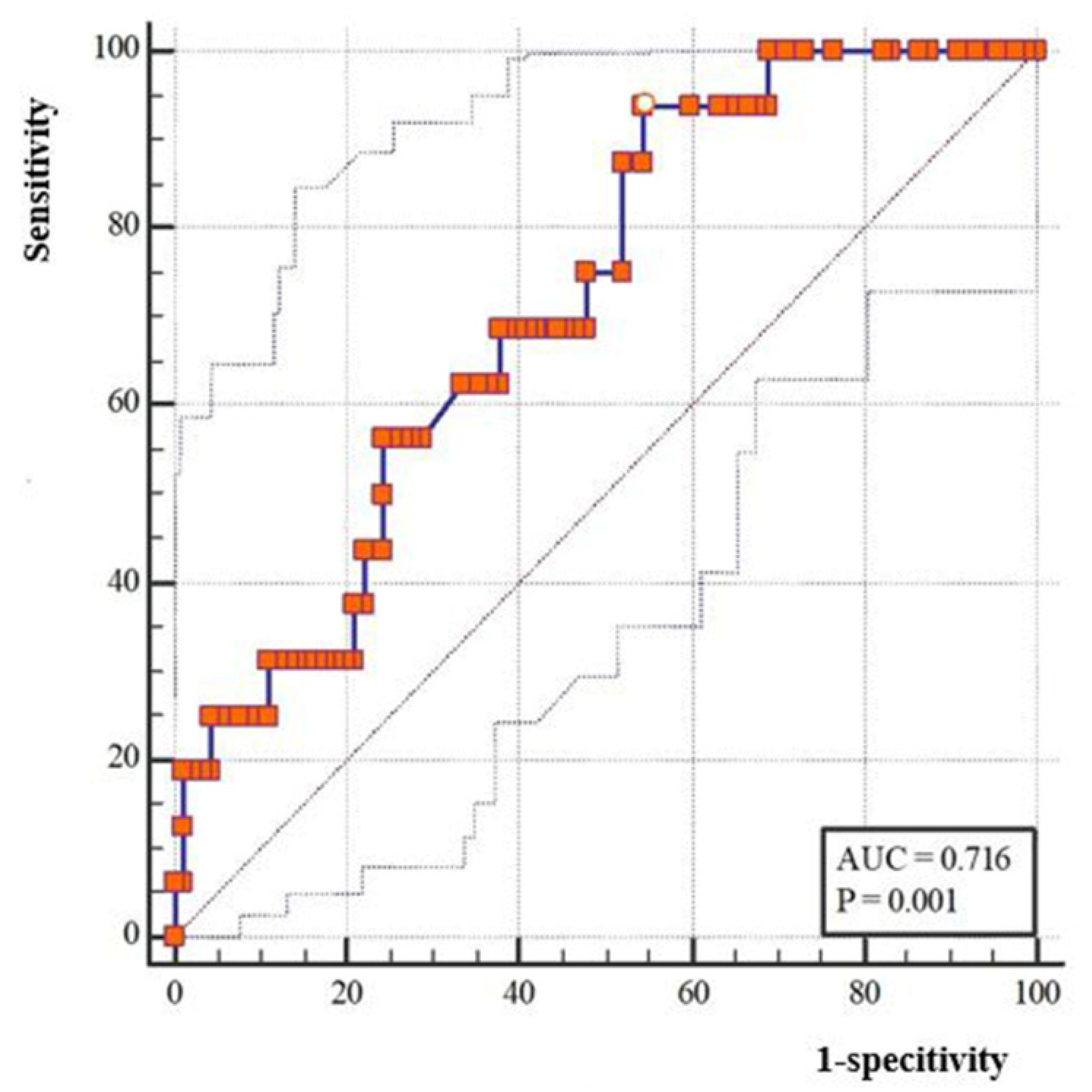
5.3. Potential Risk Factors of CHS
5.4. Correlation Analysis between Hemodynamics of RA.ES and Other Variables
6. Discussion
7. Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Suzuki, J.; Takaku, A. Cerebrovascular "moyamoya" disease. Disease showing abnormal net-like vessels in base of brain. Arch. Neurol. 1969, 20, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Acker, G.; Fekonja, L.; Vajkoczy, P. Surgical Management of Moyamoya Disease. Stroke 2018, 49, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Baaj, A.A.; Agazzi, S.; Sayed, Z.A.; Toledo, M.; Spetzler, R.F.; van Loveren, H. Surgical management of moyamoya disease: A review. Neurosurg. Focus 2009, 26, E7. [Google Scholar] [CrossRef] [PubMed]
- Houkin, K.; Ishikawa, T.; Yoshimoto, T.; Abe, H. Direct and indirect revascularization for moyamoya disease surgical techniques and peri-operative complications. Clin. Neurol. Neurosurg. 1997, 99 (Suppl. S2), S142–S145. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Shirane, R.; Fujimura, M.; Tominaga, T. Postoperative neurological deterioration in pediatric moyamoya disease: Watershed shift and hyperperfusion. J. Neurosurg. Pediatr. 2010, 6, 73–81. [Google Scholar] [CrossRef]
- Togao, O.; Mihara, F.; Yoshiura, T.; Tanaka, A.; Noguchi, T.; Kuwabara, Y.; Kaneko, K.; Matsushima, T.; Honda, H. Cerebral hemodynamics in Moyamoya disease: Correlation between perfusion-weighted MR imaging and cerebral angiography. AJNR Am. J. Neuroradiol. 2006, 27, 391–397. [Google Scholar]
- van Mook, W.N.; Rennenberg, R.J.; Schurink, G.W.; van Oostenbrugge, R.J.; Mess, W.H.; Hofman, P.A.; de Leeuw, P.W. Cerebral hyperperfusion syndrome. Lancet Neurol. 2005, 4, 877–888. [Google Scholar] [CrossRef]
- Zhao, W.G.; Luo, Q.; Jia, J.B.; Yu, J.L. Cerebral hyperperfusion syndrome after revascularization surgery in patients with moyamoya disease. Br. J. Neurosurg. 2013, 27, 321–325. [Google Scholar] [CrossRef]
- Zhao, M.; Deng, X.; Zhang, D.; Wang, S.; Zhang, Y.; Wang, R.; Zhao, J. Risk factors for and outcomes of postoperative complications in adult patients with moyamoya disease. J. Neurosurg. 2018, 130, 531–542. [Google Scholar] [CrossRef]
- Zhang, J.; Li, S.; Fujimura, M.; Lau, T.Y.; Wu, X.; Hu, M.; Zheng, H.; Xu, H.; Zhao, W.; Li, X.; et al. Hemodynamic analysis of the recipient parasylvian cortical arteries for predicting postoperative hyperperfusion during STA-MCA bypass in adult patients with moyamoya disease. J. Neurosurg. 2019, 134, 17–24. [Google Scholar] [CrossRef]
- Yang, D.; Zhang, X.; Tan, C.; Han, Z.; Su, Y.; Duan, R.; Shi, G.; Shao, J.; Cao, P.; He, S.; et al. Intraoperative transit-time ultrasonography combined with FLOW800 predicts the occurrence of cerebral hyperperfusion syndrome after direct revascularization of Moyamoya disease: A preliminary study. Acta Neurochir. 2021, 163, 563–571. [Google Scholar] [CrossRef]
- Fukui, M. Guidelines for the diagnosis and treatment of spontaneous occlusion of the circle of Willis (‘moyamoya’ disease). Research Committee on Spontaneous Occlusion of the Circle of Willis (Moyamoya Disease) of the Ministry of Health and Welfare, Japan. Clin. Neurol. Neurosurg. 1997, 99 (Suppl. S2), S238–S240. [Google Scholar] [CrossRef]
- Yin, H.; Liu, X.; Zhang, D.; Zhang, Y.; Wang, R.; Zhao, M.; Zhao, J. A Novel Staging System to Evaluate Cerebral Hypoperfusion in Patients With Moyamoya Disease. Stroke 2018, 49, 2837–2843. [Google Scholar] [CrossRef]
- Fujimura, M.; Kaneta, T.; Mugikura, S.; Shimizu, H.; Tominaga, T. Temporary neurologic deterioration due to cerebral hyperperfusion after superficial temporal artery-middle cerebral artery anastomosis in patients with adult-onset moyamoya disease. Surg. Neurol. 2007, 67, 273–282. [Google Scholar] [CrossRef]
- Fujimura, M.; Mugikura, S.; Kaneta, T.; Shimizu, H.; Tominaga, T. Incidence and risk factors for symptomatic cerebral hyperperfusion after superficial temporal artery-middle cerebral artery anastomosis in patients with moyamoya disease. Surg. Neurol. 2009, 71, 442–447. [Google Scholar] [CrossRef]
- Nomura, S.; Yamaguchi, K.; Ishikawa, T.; Kawashima, A.; Okada, Y.; Kawamata, T. Factors of Delayed Hyperperfusion and the Importance of Repeated Cerebral Blood Flow Evaluation for Hyperperfusion After Direct Bypass for Moyamoya Disease. World Neurosurg. 2018, 118, e468–e472. [Google Scholar] [CrossRef]
- Cho, H.; Jo, K.I.; Yu, J.; Yeon, J.Y.; Hong, S.C.; Kim, J.S. Low flow velocity in the middle cerebral artery predicting infarction after bypass surgery in adult moyamoya disease. J. Neurosurg. 2017, 126, 1573–1577. [Google Scholar] [CrossRef]
- Hwang, I.; Cho, W.S.; Yoo, R.E.; Kang, K.M.; Yoo, D.H.; Yun, T.J.; Choi, S.H.; Kim, J.H.; Kim, J.E.; Sohn, C.H. Revascularization Evaluation in Adult-Onset Moyamoya Disease after Bypass Surgery: Superselective Arterial Spin Labeling Perfusion MRI Compared with Digital Subtraction Angiography. Radiology 2020, 297, 630–637. [Google Scholar] [CrossRef]
- Fujimura, M.; Niizuma, K.; Endo, H.; Sato, K.; Inoue, T.; Shimizu, H.; Tominaga, T. Quantitative analysis of early postoperative cerebral blood flow contributes to the prediction and diagnosis of cerebral hyperperfusion syndrome after revascularization surgery for moyamoya disease. Neurol. Res. 2015, 37, 131–138. [Google Scholar] [CrossRef]
- Heros, R.C.; Scott, R.M.; Kistler, J.P.; Ackerman, R.H.; Conner, E.S. Temporary neurological deterioration after extracranial-intracranial bypass. Neurosurgery 1984, 15, 178–185. [Google Scholar] [CrossRef]
- Wang, J.Z.; Mu, J.; Zhang, D.; Zheng, S.; Zhu, X.; Wei, X. Clinical use of color Doppler ultrasonography to predict and evaluate the collateral development of two common revascularizations in patients with moyamoya disease. Front. Neurol. 2022, 13, 976695. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.J.; Tang, S.C.; Tsai, L.K.; Lee, C.W.; Chen, Y.F.; Liu, H.M.; Yang, S.H.; Hsieh, Y.L.; Kuo, M.F.; Jeng, J.S. Greater ultrasonographic changes in pediatric moyamoya patients compared with adults after indirect revascularization surgeries. J. Neurosurg. Pediatr. 2018, 22, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Ge, P.; Li, Y.; Wang, J.; Shi, Z.; Zhang, J.; He, L.; Cheng, L.; Zhang, D.; He, W. Association Between Ultrasound Parameters and History of Ischemic or Hemorrhagic Stroke in Patients With Moyamoya Disease. Front. Neurol. 2021, 12, 570843. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.R.; Lu, V.M.; Elarjani, T.; Silva, M.A.; Jamshidi, A.M.; Cajigas, I.; Morcos, J.J. One-donor, two-recipient extracranial-intracranial bypass series for moyamoya and cerebral occlusive disease: Rationale, clinical and angiographic outcomes, and intraoperative blood flow analysis. J. Neurosurg. 2022, 136, 627–636. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Values |
|---|---|
| No. of patients | 101 |
| No. of hemispheres | 106 |
| Age, years | 50.03 ± 8.79 |
| Gender (male) | 56 (52.83%) |
| Onset type | |
| Hemorrhagic | 20 (18.87%) |
| Ischemic | 86 (81.13%) |
| Surgical side (left) | 52 (49.05%) |
| Previous infarction | 61 (57.55%) |
| Hypertension | 52 (49.06%) |
| Diabetes | 18 (16.98%) |
| Suzuki stage | |
| I | 13 (12.26%) |
| II | 26 (24.53%) |
| III | 39 (36.79%) |
| IV | 16 (15.09%) |
| V | 8 (7.55%) |
| VI | 4 (3.77%) |
| Puff smoke | |
| None | 19 (17.92%) |
| Sparse | 35 (33.02%) |
| Dense | 52 (49.06%) |
| No | Sex | Age | HT | DB | SS | MV | FD | RA | BG | Cor | Syl | Op Side | Symptoms | Time |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 35 | 0 | 0 | 5 | sparse | sylvian | 7 | 50 | 23 | 83 | lt | aphasia | Po3 |
| 2 | F | 57 | 1 | 0 | 6 | sparse | Cortex | 8 | 40 | 20 | 23 | lt | aphasia | |
| 3 | M | 49 | 0 | 1 | 3 | dense | Cortex | 3 | 77 | 28 | 73 | lt | Seizures | Po5 |
| 4 | M | 52 | 1 | 0 | 3 | dense | Cortex | 5 | 70 | 8 | 27 | lt | verbal dys, hemorrhage | Po2 |
| 5 | F | 39 | 1 | 0 | 6 | none | sylvian | 7 | 83 | 32 | 30 | rt | headache, verbal dys | Po3 |
| 6 | M | 49 | 1 | 1 | 3 | dense | sylvian | 7 | 73 | 53 | 50 | rt | hemorrhage | Po2 |
| 7 | F | 35 | 1 | 1 | 2 | sparse | Cortex | 1 | 63 | 70 | 70 | rt | verbal dys | Po1 |
| 8 | F | 52 | 1 | 0 | 3 | dense | Cortex | 8 | 47 | 1 | 50 | lt | aphasia | Po2 |
| 9 | M | 35 | 0 | 0 | 3 | dense | sylvian | 9 | 24 | 24 | 17 | rt | headache | Po2 |
| 10 | F | 60 | 0 | 0 | 4 | dense | Cortex | 4 | 49 | 15 | 30 | lt | verbal dys | Po3 |
| 11 | M | 40 | 0 | 1 | 4 | dense | sylvian | 3 | 67 | 53 | 80 | rt | headache | Po2 |
| 12 | M | 60 | 0 | 0 | 4 | dense | Cortex | 4 | 54 | 5 | 13 | lt | headache | Po2 |
| 13 | F | 51 | 0 | 0 | 2 | sparse | sylvian | 5 | 26 | 10 | 15 | lt | verbal dys | Po4 |
| 14 | F | 71 | 1 | 0 | 5 | sparse | Cortex | 7 | 47 | 3 | 21 | lt | aphasia | Po5 |
| 15 | F | 46 | 0 | 0 | 5 | sparse | sylvian | 8 | 57 | 6 | 75 | lt | verbal dys | Po3 |
| 16 | M | 56 | 0 | 0 | 3 | dense | Cortex | 2 | 27 | 2 | 17 | lt | SAH, aphasia | Po15 minPo3 |
| CHS | p Value | ||||
|---|---|---|---|---|---|
| Variables | No (n = 90) | Yes (n = 16) | Univariate | Multivariate | OR (95%CI) |
| Gender (male, n, %) | 49 (54.4%) | 7 (43.8%) | 0.588 a | ||
| Age (years) | 50.79 ± 9.13 | 49.19 ± 10.45 | 0.529 b | ||
| Op side (left, n, %) | 41 (45.6%) | 11 (68.8%) | 0.108 a | 0.043 * | 4.58 (1.05–19.97) |
| Onset type | 0.990 a | ||||
| Hemorrhagic | 17 (18.9%) | 3 (18.8%) | |||
| Ischemic | 73 (81.1%) | 13 (81.3%) | |||
| Post infarction | 49 (54.4%) | 12 (75.0%) | 0.172 a | ||
| Hypertension | 45 (50.0%) | 7 (43.8%) | 0.788 a | ||
| Diabetes | 14 (15.6%) | 4 (25.0%) | 0.467 a | ||
| Suzuki stage | 0.008 c* | 0.017 * | 5.47 (1.99–15.05) | ||
| Early | 37 (41.1%) | 2 (12.5%) | 0.046 | — | ref |
| Middle | 46 (51.1%) | 9 (56.3%) | 0.705 | 0.028 * | 13.40 (1.32–136.62) |
| Advanced | 7 (7.8%) | 5 (31.3%) | 0.017 * | 0.005 * | 37.20 (3.07–451.30) |
| Puff smoke | 0.281 c | ||||
| None | 18 (20.0%) | 1 (6.3%) | |||
| Sparse | 29 (32.2%) | 6 (37.5%) | |||
| Dense | 43 (47.8%) | 9 (56.3%) | |||
| PSCAs direction | 0.766 a | ||||
| Sylvian | 43 (47.8%) | 7 (43.8%) | |||
| Cortex | 47 (52.2%) | 9 (56.3%) | |||
| Pre MVV (RA) | 11.24 ± 6.42 | 7.12 ± 4.95 | 0.007 b* | 0.064 | 0.88 (0.78–1.33) |
| Post MVV (RA) | |||||
| RA.ES | 36.23 ± 23.81 | 41.56 ± 26.68 | 0.421 b | 0.186 | |
| Post/pre fold | 2.1 (1.40, 6.25) | 4.75 (2.30, 11.10) | 0.008 c* | 0.003 * | 1.17 (1.06–1.30) |
| RA.LS | 22.51 ± 16.06 | 22.06 ± 20.83 | 0.922 b | 0.278 | |
| Post/pre fold | 2.0 (1.17, 3.23) | 2.25 (0.83, 6.67) | 0.694 c | 0.651 | |
| Post MVV (bypass) | 51.41 ± 28.61 | 53.37 ± 18.23 | 0.722 b | 0.541 | |
| RA.ES | Gender | Age | Onset Type | Pre Infarction | HT | DB | MV | SS |
|---|---|---|---|---|---|---|---|---|
| r | −0.075 | −0.122 | −0.222 * | 0.252 ** | 0.085 | 0.308 ** | −0.075 | −0.143 |
| p | 0.442 | 0.213 | 0.022 | 0.009 | 0.386 | 0.001 | 0.442 | 0.144 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, Z.; Wu, L.; Wang, Y.; Li, W.; Wang, J.; Yang, Y.; Hang, C. Intraoperative Hemodynamics of Parasylvian Cortical Arteries for Predicting Postoperative Symptomatic Cerebral Hyperperfusion after Direct Revascularization in Patients with Moyamoya Disease: A Preliminary Study. J. Clin. Med. 2023, 12, 3855. https://doi.org/10.3390/jcm12113855
Shi Z, Wu L, Wang Y, Li W, Wang J, Yang Y, Hang C. Intraoperative Hemodynamics of Parasylvian Cortical Arteries for Predicting Postoperative Symptomatic Cerebral Hyperperfusion after Direct Revascularization in Patients with Moyamoya Disease: A Preliminary Study. Journal of Clinical Medicine. 2023; 12(11):3855. https://doi.org/10.3390/jcm12113855
Chicago/Turabian StyleShi, Zhiyong, Lingyun Wu, Yi Wang, Wei Li, Juan Wang, Yongbo Yang, and Chunhua Hang. 2023. "Intraoperative Hemodynamics of Parasylvian Cortical Arteries for Predicting Postoperative Symptomatic Cerebral Hyperperfusion after Direct Revascularization in Patients with Moyamoya Disease: A Preliminary Study" Journal of Clinical Medicine 12, no. 11: 3855. https://doi.org/10.3390/jcm12113855
APA StyleShi, Z., Wu, L., Wang, Y., Li, W., Wang, J., Yang, Y., & Hang, C. (2023). Intraoperative Hemodynamics of Parasylvian Cortical Arteries for Predicting Postoperative Symptomatic Cerebral Hyperperfusion after Direct Revascularization in Patients with Moyamoya Disease: A Preliminary Study. Journal of Clinical Medicine, 12(11), 3855. https://doi.org/10.3390/jcm12113855