

Sagittal Spinal Alignment in People with Chronic Spinal Cord Injury and Normal Individual: A Comparison Study Using 3D Ultrasound Imaging

 ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Sample
2.2. Inclusion and Exclusion Criteria
2.3. Experimental Protocol and Assessment
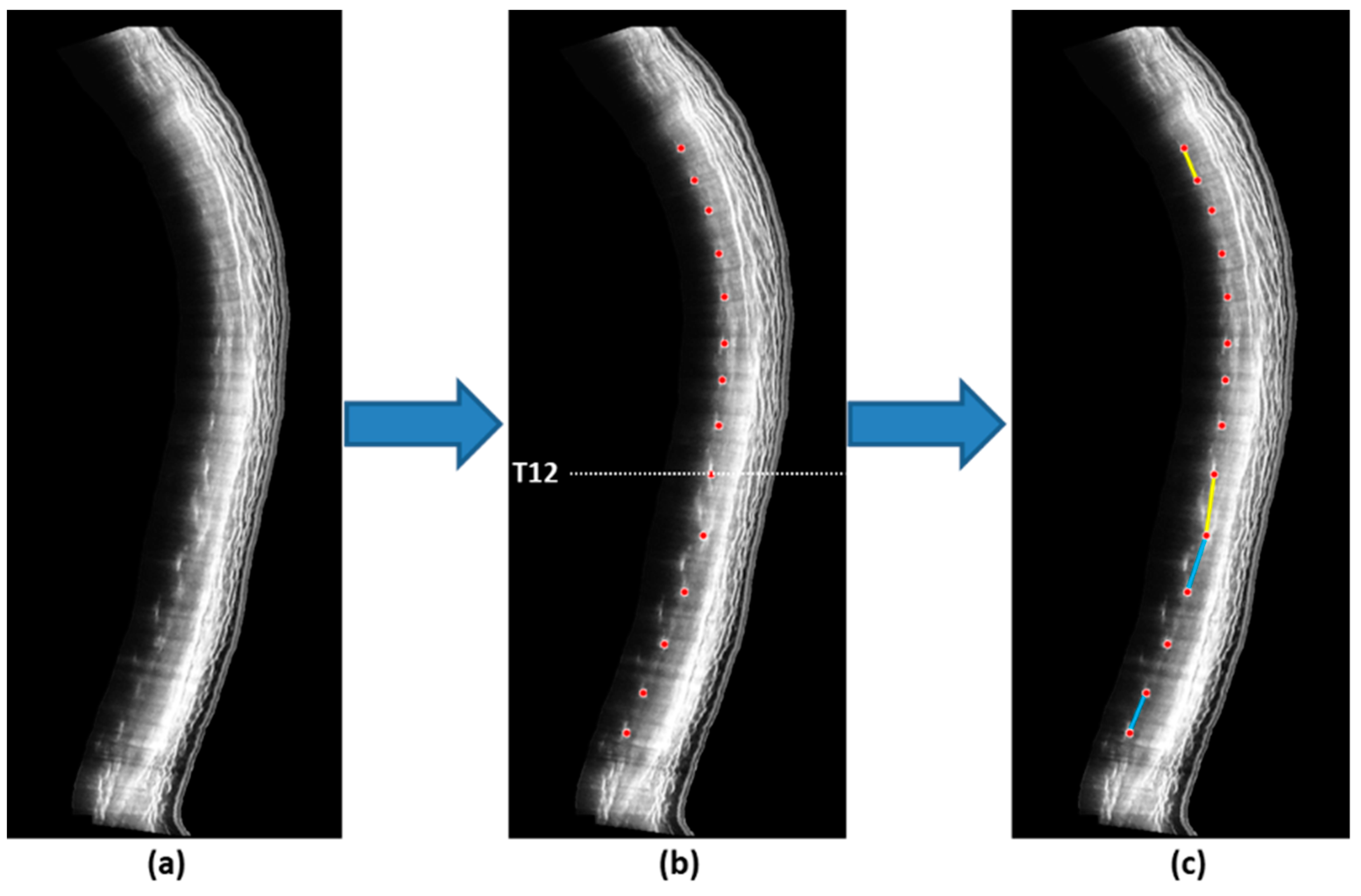
2.4. Scanning Procedure
2.5. Data Processing and Analysis
2.6. Statistical Analysis
3. Results
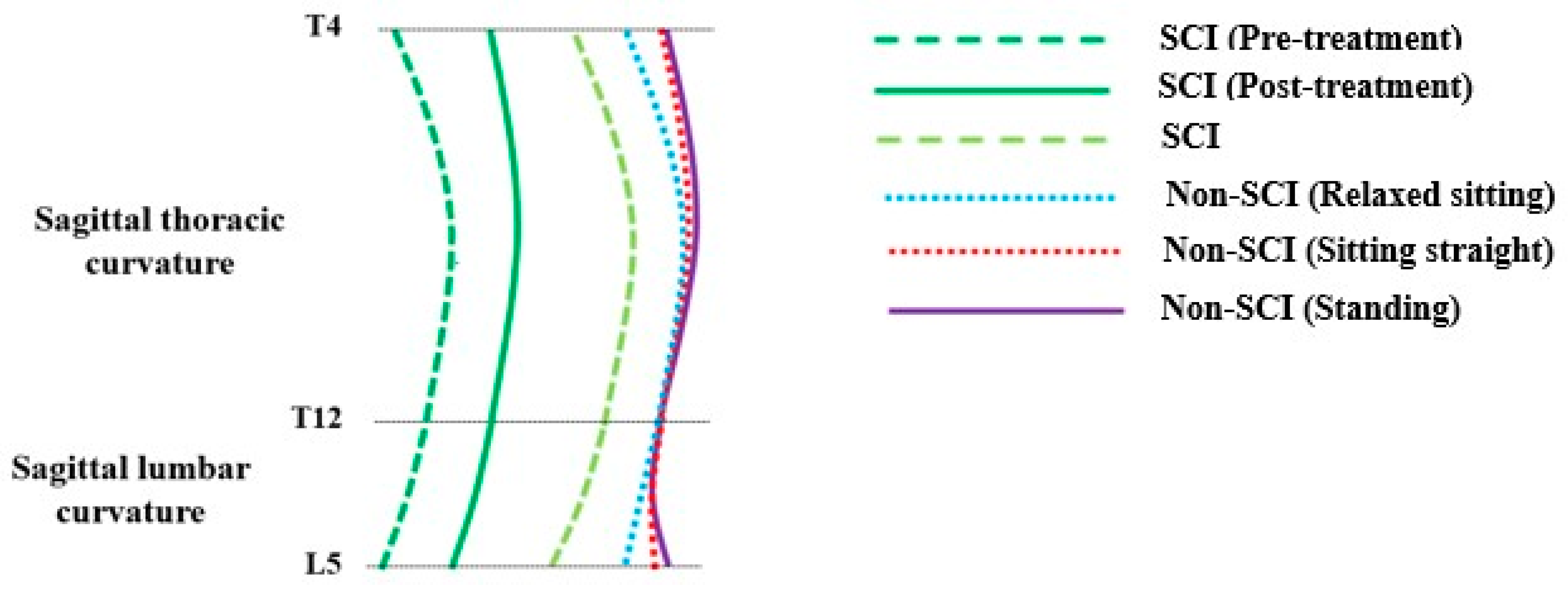
3.1. Participants’ Characteristics and Overall Sagittal Spinal Profile
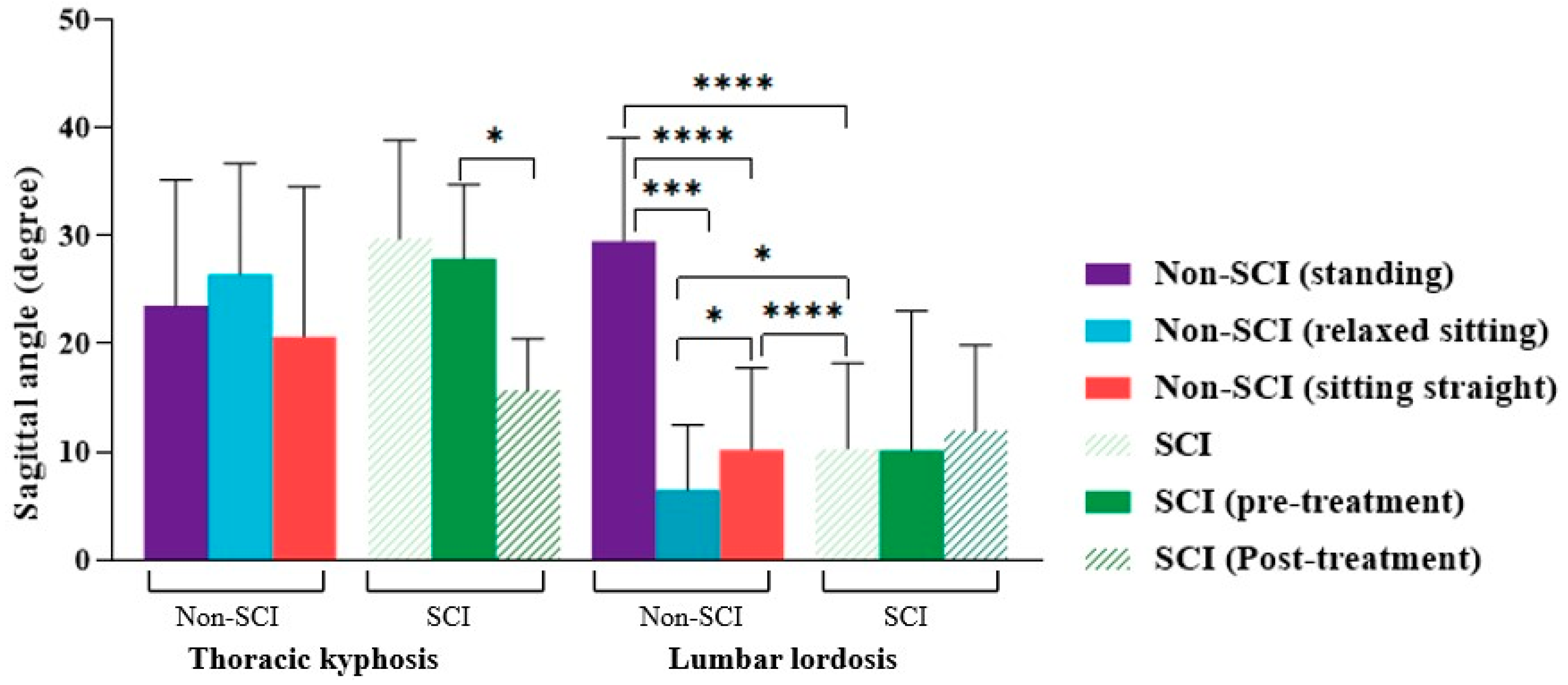
3.2. Sagittal Curvature Angle Differences for Non-SCI Subjects in Different Postures
3.3. Sagittal Curvature Angle Differences between Individuals with SCI and Non-SCI Subjects
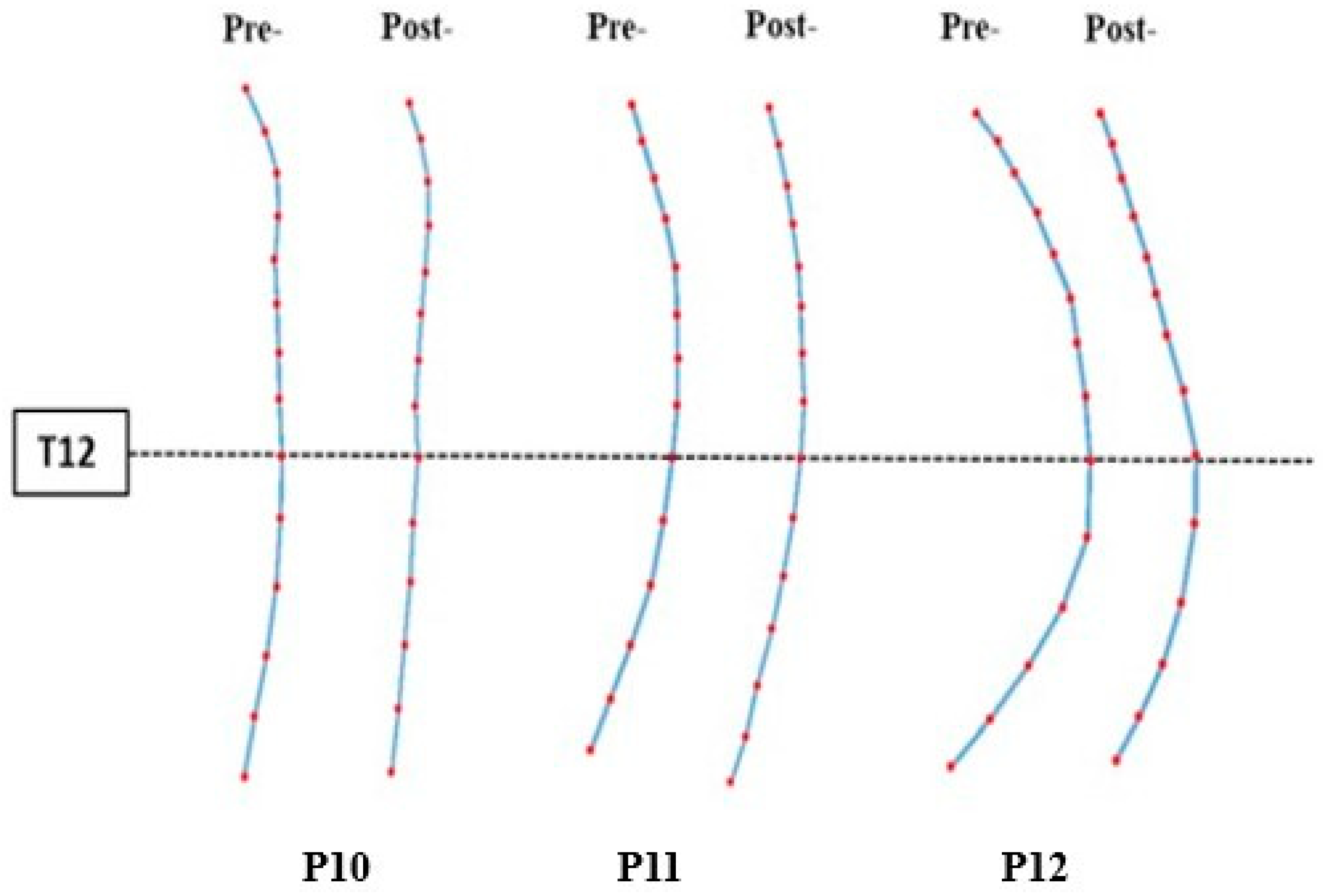
3.4. Sagittal Spinal Alignment Changed after Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Varas-Díaz, G.; Brunetti, E.P.; Rivera-Lillo, G.; Maldonado, P.E. Patients with chronic spinal cord injury exhibit reduced autonomic modulation during an emotion recognition task. Front. Hum. Neurosci. 2017, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Tharu, N.S.; Alam, M.; Bajracharya, S.; Chaudhary, G.P.; Pandey, J.; Kabir, M.A. Caregivers’ Knowledge, Attitude, and Practice towards Pressure Injuries in Spinal Cord Injury at Rehabilitation Center in Bangladesh. Adv. Orthop. 2022, 2022, 1–9. [Google Scholar] [CrossRef]
- Mataliotakis, G.I.; Tsirikos, A.I. Spinal cord trauma: Pathophysiology, classification of spinal cord injury syndromes, treatment principles and controversies. Orthop. Trauma 2016, 30, 440–449. [Google Scholar] [CrossRef]
- Sezer, N.; Akkuş, S.; Uğurlu, F.G. Chronic complications of spinal cord injury. World J. Orthop. 2015, 6, 24. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Silber, J.S. Post-traumatic Spinal Deformity. Spine 2001, 26 (Suppl. S24), S111–S118. [Google Scholar] [CrossRef] [PubMed]
- Mulcahey, M.; Gaughan, J.; Betz, R.; Samdani, A.; Barakat, N.; Hunter, L. Neuromuscular scoliosis in children with spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2013, 19, 96–103. [Google Scholar] [CrossRef]
- Negrini, S.; Aulisa, L.; Ferraro, C.; Fraschini, P.; Masiero, S.; Simonazzi, P. Italian guidelines on rehabilitation treatment of adolescents with scoliosis or other spinal deformities. Eur. Med. 2005, 41, 183–201. [Google Scholar]
- Villemure, I.; Aubin, C.; Grimard, G.; Dansereau, J.; Labelle, H. Progression of vertebral and spinal three-dimensional deformities in adolescent idiopathic scoliosis: A longitudinal study. Spine 2001, 26, 2244–2250. [Google Scholar] [CrossRef]
- Jang, J.-S.; Lee, S.-H.; Min, J.-H.; Maeng, D.H. Influence of lumbar lordosis restoration on thoracic curve and sagittal position in lumbar degenerative kyphosis patients. Spine 2009, 34, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-J.; Giambini, H.; Zhang, W.-J.; Ye, G.-H.; Zhao, C.; An, K.-N. A modified sagittal spine postural classification and its relationship to deformities and spinal mobility in a Chinese osteoporotic population. PLoS ONE 2012, 7, e38560. [Google Scholar] [CrossRef] [PubMed]
- Hastings, J.D.; Fanucchi, E.R.; Burns, S.P. Wheelchair configuration and postural alignment in persons with spinal cord injury. Arch. Phys. Med. Rehabil. 2003, 84, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Le Huec, J.; Thompson, W.; Mohsinaly, Y.; Barrey, C.; Faundez, A. Sagittal balance of the spine. Eur. Spine J. 2019, 28, 1889–1905. [Google Scholar] [CrossRef]
- Rath, M.; Vette, A.H.; Ramasubramaniam, S.; Li, K.; Burdick, J.; Edgerton, V.R. Trunk stability enabled by noninvasive spinal electrical stimulation after spinal cord injury. Eur. Spine J. 2018, 28, 1889–1905. [Google Scholar] [CrossRef] [PubMed]
- Mao, H.-F.; Huang, S.-L.; Lu, T.-W.; Lin, Y.-S.; Liu, H.-M.; Wang, Y.-H. Effects of lateral trunk support on scoliotic spinal alignment in persons with spinal cord injury: A radiographic study. Arch. Phys. Med. Rehabil. 2006, 87, 764–771. [Google Scholar] [CrossRef] [PubMed]
- Diebo, B.G.; Varghese, J.J.; Lafage, R.; Schwab, F.J.; Lafage, V. Sagittal alignment of the spine: What do you need to know? Clin. Neurol. Neurosurg. 2015, 139, 295–301. [Google Scholar] [CrossRef]
- Roussouly, P.; Nnadi, C. Sagittal plane deformity: An overview of interpretation and management. Eur. Spine J. 2010, 19, 1824–1836. [Google Scholar] [CrossRef]
- Harrison, D.D.; Janik, T.J.; Troyanovich, S.J.; Holland, B. Comparisons of lordotic cervical spine curvatures to a theoretical ideal model of the static sagittal cervical spine. Spine 1996, 21, 667–675. [Google Scholar] [CrossRef]
- Singla, D.; Veqar, Z. Association between forward head, rounded shoulders, and increased thoracic kyphosis: A review of the literature. J. Chiropr. Med. 2017, 16, 220–229. [Google Scholar] [CrossRef]
- El-Salam, S.M.A.; El-Din Ibrahim, M.E. The Relationship between Sagittal Curvature (Lumbar Lordosis) and Extensor Muscle Volume in Lumbar Region: A Morphological and Radiological Study. Med. J. Cairo Univ. 2019, 87, 1083–1109. [Google Scholar] [CrossRef]
- Lamartina, C.; Berjano, P. Classification of sagittal imbalance based on spinal alignment and compensatory mechanisms. Eur. Spine J. 2014, 23, 1177–1189. [Google Scholar] [CrossRef]
- Castro de Medeiros, R.; Jaccard, A.; Cliquet, A. Sagittal spinal alignment in paraplegics: A new paradigm for the rehabilitation under neuromuscular electrical stimulation. Spinal Cord 2010, 48, 251–256. [Google Scholar] [CrossRef][Green Version]
- Czaprowski, D.; Pawłowska, P.; Kolwicz-Gańko, A.; Sitarski, D.; Kędra, A. The influence of the “straighten your back” command on the sagittal spinal curvatures in children with generalized joint hypermobility. BioMed Res. Int. 2017, 2017, 9724021. [Google Scholar] [CrossRef] [PubMed]
- Scheer, J.K.; Tang, J.A.; Smith, J.S.; Acosta, F.L.; Protopsaltis, T.S.; Blondel, B. Cervical spine alignment, sagittal deformity, and clinical implications: A review. J. Neurosurg. Spine 2013, 19, 141–159. [Google Scholar] [CrossRef] [PubMed]
- Yazici, A.G.; Mohammadi, M. The effect of corrective exercises on the thoracic kyphosis and lumbar lordosis of boy students. Turk. J. Sport Exerc. 2017, 19, 177–181. [Google Scholar] [CrossRef]
- López-Miñarro, P.A.; Vaquero-Cristóbal, R.; Alacid, F.; Isorna, M.M.; Muyor, J. Comparison of sagittal spinal curvatures and pelvic tilt in highly trained athletes from different sport disciplines. Kinesiology 2017, 49, 109–116. [Google Scholar] [CrossRef]
- Asai, Y.; Tsutsui, S.; Oka, H.; Yoshimura, N.; Hashizume, H.; Yamada, H.; Akune, T.; Muraki, S.; Matsudaira, K.; Kawaguchi, H.; et al. Sagittal spino-pelvic alignment in adults: The Wakayama Spine Study. PLoS ONE 2017, 12, e0178697. [Google Scholar] [CrossRef] [PubMed]
- Jentzsch, T.; Geiger, J.; König, M.A.; Werner, C.M. Hyperlordosis is associated with facet joint pathology at the lower lumbar spine. Clin. Spine Surg. 2017, 30, 129–135. [Google Scholar] [CrossRef]
- Gao, K.L.; Chan, K.; Purves, S.; Tsang, W.W. Reliability of dynamic sitting balance tests and their correlations with functional mobility for wheelchair users with chronic spinal cord injury. J. Orthop. Transl. 2015, 3, 44–49. [Google Scholar] [CrossRef]
- Chen, C.-L.; Yeung, K.-T.; Bih, L.-I.; Wang, C.-H.; Chen, M.-I.; Chien, J.-C. The relationship between sitting stability and functional performance in patients with paraplegia. Arch. Phys. Med. Rehabil. 2003, 84, 1276–1281. [Google Scholar] [CrossRef]
- Shirado, O.; Kawase, M.; Minami, A.; Strax, T.E. Quantitative evaluation of long sitting in paraplegic patients with spinal cord injury. Arch. Phys. Med. Rehabil. 2004, 85, 1251–1256. [Google Scholar] [CrossRef]
- Minkel, J.L. Seating and mobility considerations for people with spinal cord injury. Phys. Ther. 2000, 80, 701–709. [Google Scholar] [CrossRef]
- Triolo, R.J.; Bailey, S.N.; Miller, M.E.; Lombardo, L.M.; Audu, M.L. Effects of stimulating hip and trunk muscles on seated stability, posture, and reach after spinal cord injury. Arch. Phys. Med. Rehabil. 2013, 94, 1766–1775. [Google Scholar] [CrossRef] [PubMed]
- Bolin, I.; Bodin, P.; Kreuter, M. Sitting position–posture and performance in C5–C6 tetraplegia. Spinal Cord 2000, 38, 425–434. [Google Scholar] [CrossRef][Green Version]
- Kuo, Y.-L.; Chung, C.-H.; Huang, T.-W.; Tsao, C.-H.; Chang, S.-Y.; Peng, C.-K. Association between spinal curvature disorders and injury: A nationwide population-based retrospective cohort study. BMJ Open 2019, 9, e023604. [Google Scholar] [CrossRef] [PubMed]
- Yeramaneni, S.; Robinson, C.; Hostin, R. Impact of spine surgery complications on costs associated with management of adult spinal deformity. Curr. Rev. Musculoskelet. Med. 2016, 9, 327–332. [Google Scholar] [CrossRef]
- Palazzo, C.; Montigny, J.-P.; Barbot, F.; Bussel, B.; Vaugier, I.; Fort, D. Effects of bracing in adult with scoliosis: A retrospective study. Arch. Phys. Med. Rehabil. 2017, 98, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.A.; Tharu, N.S.; Gustin, S.M.; Zheng, Y.-P.; Alam, M. Trans-Spinal Electrical Stimulation Therapy for Functional Rehabilitation after Spinal Cord Injury. J. Clin. Med. 2022, 11, 1550. [Google Scholar] [CrossRef]
- McGeady, C.; Vučković, A.; Tharu, N.S.; Zheng, Y.-P.; Alam, M. Brain-Computer Interface Priming for Cervical Transcutaneous Spinal Cord Stimulation Therapy: An Exploratory Case Study. Front. Rehabil. Sci. 2022, 3, 896766. [Google Scholar] [CrossRef]
- Tharu, N.S.; Alam, M.; Ling, Y.T.; Wong, A.Y.; Zheng, Y.-P. Combined Transcutaneous Electrical Spinal Cord Stimulation and Task-Specific Rehabilitation Improves Trunk and Sitting Functions in People with Chronic Tetraplegia. Biomedicines 2022, 11, 34. [Google Scholar] [CrossRef]
- Keller, A.; Singh, G.; Sommerfeld, J.H.; King, M.; Parikh, P.; Ugiliweneza, B. Noninvasive spinal stimulation safely enables upright posture in children with spinal cord injury. Nat. Commun. 2021, 12, 5850. [Google Scholar] [CrossRef]
- Zheng, Y.-P.; Lee, T.T.-Y.; Lai, K.K.-L.; Yip, B.H.-K.; Zhou, G.-Q.; Jiang, W.-W.; Cheung, J.C.-W.; Wong, M.-S.; Ng, B.K.-W.; Cheng, J.C.-Y.; et al. A reliability and validity study for Scolioscan: A radiation-free scoliosis assessment system using 3D ultrasound imaging. Scoliosis 2016, 11, 13. [Google Scholar] [CrossRef]
- Lai, K.K.-L.; Lee, T.T.-Y.; Lee, M.K.-S.; Hui, J.C.-H.; Zheng, Y.-P. Validation of scolioscan air-portable radiation-free three-dimensional ultrasound imaging assessment system for scoliosis. Sensors 2021, 21, 2858. [Google Scholar] [CrossRef]
- Lee, T.T.-Y.; Jiang, W.W.; Cheng, C.L.K.; Lai, K.K.-L.; To, M.K.T.; Castelein, R.M. A novel method to measure the sagittal curvature in spinal deformities: The reliability and feasibility of 3-D ultrasound imaging. Ultrasound Med. Biol. 2019, 45, 2725–2735. [Google Scholar] [CrossRef]
- Lee, T.T.-Y.; Cheung, J.C.-W.; Law, S.-Y.; To, M.K.T.; Cheung, J.P.Y.; Zheng, Y.-P. Analysis of sagittal profile of spine using 3D ultrasound imaging: A phantom study and preliminary subject test. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2020, 8, 232–244. [Google Scholar] [CrossRef]
- Schmid, S.; Bruhin, B.; Ignasiak, D.; Romkes, J.; Taylor, W.R.; Ferguson, S.J. Spinal kinematics during gait in healthy individuals across different age groups. Hum. Mov. Sci. 2017, 54, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Hey, H.W.D.; Teo, A.Q.A.; Tan, K.-A.; Ng, L.W.N.; Lau, L.-L.; Liu, K.-P.G. How the spine differs in standing and in sitting—Important considerations for correction of spinal deformity. Spine J. 2017, 17, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Habibi, Z.; Maleki, F.; Meybodi, A.T.; Mahdavi, A.; Saberi, H. Lumbosacral sagittal alignment in association to intervertebral disc diseases. Asian Spine J. 2014, 8, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Hey, H.W.D.; Wong, C.G.; Lau, E.T.-C.; Tan, K.-A.; Lau, L.-L.; Liu, K.-P.G. Differences in erect sitting and natural sitting spinal alignment—Insights into a new paradigm and implications in deformity correction. Spine J. 2017, 17, 183–189. [Google Scholar] [CrossRef]
- Alm, M.; Gutierrez, E.; Hultling, C.; Saraste, H. Clinical evaluation of seating in persons with complete thoracic spinal cord injury. Spinal Cord 2003, 41, 563–571. [Google Scholar] [CrossRef]
- Hobson, D.A.; Tooms, R.E. Seated lumbar/pelvic alignment. A comparison between spinal cord-injured and noninjured groups. Spine 1992, 17, 293–298. [Google Scholar] [CrossRef]
- Schwab, F.; Patel, A.; Ungar, B.; Farcy, J.-P.; Lafage, V. Adult spinal deformity—Postoperative standing imbalance: How much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine 2010, 35, 2224–2231. [Google Scholar] [CrossRef] [PubMed]
- Kulshrestha, R.; Kuiper, J.; Masri, W.E.; Chowdhury, J.; Kaur, S.; Kumar, N. Scoliosis in paediatric onset spinal cord injuries. Spinal Cord 2020, 58, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Beltsios, M.; Savvidou, O.; Mitsiokapa, E.A.; Mavrogenis, A.F.; Kaspiris, A.; Efstathopoulos, N. Sagittal alignment of the cervical spine after neck injury. Eur. J. Orthop. Surg. Traumatol. 2013, 23, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.C.; van Rhijn, L.W.; van Ooij, A. Predictable correction of the unfused lumbar lordosis after thoracic correction and fusion in Scheuermann kyphosis. Spine 2006, 31, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Zidek, K.; Srinivasan, R. Rehabilitation of a child with a spinal cord injury. In Seminars in Pediatric Neurology; Elsevier: Amsterdam, The Netherlands, 2003. [Google Scholar] [CrossRef]
- Keorochana, G.; Taghavi, C.E.; Lee, K.-B.; Yoo, J.H.; Liao, J.-C.; Fei, Z. Effect of sagittal alignment on kinematic changes and degree of disc degeneration in the lumbar spine: An analysis using positional MRI. Spine 2011, 36, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Triolo, R.J.; Boggs, L.; Miller, M.E.; Nemunaitis, G.; Nagy, J.; Bailey, S.N. Implanted electrical stimulation of the trunk for seated postural stability and function after cervical spinal cord injury: A single case study. Arch. Phys. Med. Rehabil. 2009, 90, 340–347. [Google Scholar] [CrossRef]
- Crytzer, T.M.; Hong, E.-K.; Dicianno, B.E.; Pearlman, J.; Schmeler, M.; Cooper, R.A. Identifying characteristic back shapes from anatomical scans of wheelchair users to improve seating design. Med. Eng. Phys. 2016, 38, 999–1007. [Google Scholar] [CrossRef]
- Bergström, E.; Short, D.; Frankel, H.; Henderson, N.; Jones, P. The effect of childhood spinal cord injury on skeletal development: A retrospective study. Spinal Cord 1999, 37, 838–846. [Google Scholar] [CrossRef][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Gender | Age (yr) | BMI (kg/m2) | ASIA | NLI | Post-SCI (yr) | |
|---|---|---|---|---|---|---|---|
| SCI group | |||||||
| P1 | M | 44 | 18.2 | C | C8 | 20 | |
| P2 | F | 39 | 24.8 | B | C7 | 13 | |
| P3 | M | 36 | 20.2 | B | T1 | 11 | |
| P4 | M | 58 | 20.8 | C | C6 | 18 | |
| P5 | M | 31 | 26.7 | B | C7 | 12 | |
| P6 | F | 48 | 18.0 | C | T6 | 22 | |
| P7 | M | 50 | 23.0 | B | T2 | 13 | |
| P8 | F | 61 | 25.0 | C | C8 | 26 | |
| P9 | M | 38 | 22.9 | D | T8 | 23 | |
| 28.1 (Mean) 13.3 (SD) | 21.9 (Mean) 2.9 (SD) | 15.9 (Mean) 6.6 (SD) | |||||
| Received TSCS | P10 | F | 57 | 24.8 | A | C6 | 2 |
| P11 | F | 55 | 18.8 | A | C7 | 19 | |
| P12 | F | 26 | 20.4 | A | C5 | 12 | |
| 46.0 (Mean) 17.3 (SD) | 21.3 (Mean) 3.1 (SD) | 10.8 (Mean) 8.8 (SD) | |||||
| Non-SCI group | |||||||
| S1 | M | 28 | 20.2 | - | - | - | |
| S2 | M | 57 | 19.7 | - | - | - | |
| S3 | F | 47 | 26.6 | - | - | - | |
| S4 | F | 40 | 22.0 | - | - | - | |
| S5 | M | 16 | 19.5 | - | - | - | |
| S6 | M | 25 | 24.7 | - | - | - | |
| S7 | M | 32 | 20.4 | - | - | - | |
| S8 | M | 28 | 25.0 | - | - | - | |
| S9 | M | 29 | 25.9 | - | - | - | |
| S10 | M | 33 | 22.6 | - | - | - | |
| 33.5 (Mean) 11.7 (SD) | 22.6 (Mean) 2.7 (SD) | ||||||
| Sagittal Angle (Degree) | SCI | Non-SCI | ||
|---|---|---|---|---|
| Standing | Sitting Straight | Relaxed Sitting | ||
| TK (mean ± SD) | 29.6 ± 9.5 | 23.5 ± 11.6 | 20.3 ± 14.5 | 26.4 ± 10.3 |
| LL (mean ± SD) | 7.2 ± 9.7 | 29.5 ± 9.6 | 10.0 ± 7.9 | 6.1 ± 9.1 |
| P10 (Mean in Degree) | P11 (Mean in Degree) | P12 (Mean in Degree) | Average (Mean ± SD) | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post |
| (TK) 27.6 | 16.4 | 21.2 | 20.1 | 34.9 | 10.6 | 26.6 ± 7.3 | 16.3 ± 5.0 |
| (LL) 0.5 | 4.4 | 5.1 | 11.2 | 24.8 | 20.2 | 9.3 ± 13.9 | 11.7 ± 8.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tharu, N.S.; Lee, T.T.-Y.; Lai, K.K.-L.; Lau, T.-E.; Chan, C.-Y.; Zheng, Y.-P. Sagittal Spinal Alignment in People with Chronic Spinal Cord Injury and Normal Individual: A Comparison Study Using 3D Ultrasound Imaging. J. Clin. Med. 2023, 12, 3854. https://doi.org/10.3390/jcm12113854
Tharu NS, Lee TT-Y, Lai KK-L, Lau T-E, Chan C-Y, Zheng Y-P. Sagittal Spinal Alignment in People with Chronic Spinal Cord Injury and Normal Individual: A Comparison Study Using 3D Ultrasound Imaging. Journal of Clinical Medicine. 2023; 12(11):3854. https://doi.org/10.3390/jcm12113854
Chicago/Turabian StyleTharu, Niraj Singh, Timothy Tin-Yan Lee, Kelly Ka-Lee Lai, Ting-Er Lau, Chui-Yi Chan, and Yong-Ping Zheng. 2023. "Sagittal Spinal Alignment in People with Chronic Spinal Cord Injury and Normal Individual: A Comparison Study Using 3D Ultrasound Imaging" Journal of Clinical Medicine 12, no. 11: 3854. https://doi.org/10.3390/jcm12113854
APA StyleTharu, N. S., Lee, T. T.-Y., Lai, K. K.-L., Lau, T.-E., Chan, C.-Y., & Zheng, Y.-P. (2023). Sagittal Spinal Alignment in People with Chronic Spinal Cord Injury and Normal Individual: A Comparison Study Using 3D Ultrasound Imaging. Journal of Clinical Medicine, 12(11), 3854. https://doi.org/10.3390/jcm12113854