

Impact of Resolved Preformed, Persistent Preformed, and De Novo Anti-HLA Donor-Specific Antibodies in Kidney Transplant Recipients on Long-Term Renal Graft Outcomes

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Characteristics of Anti-HLA DSAs before and after Transplantation
3.3. Clinical Outcomes
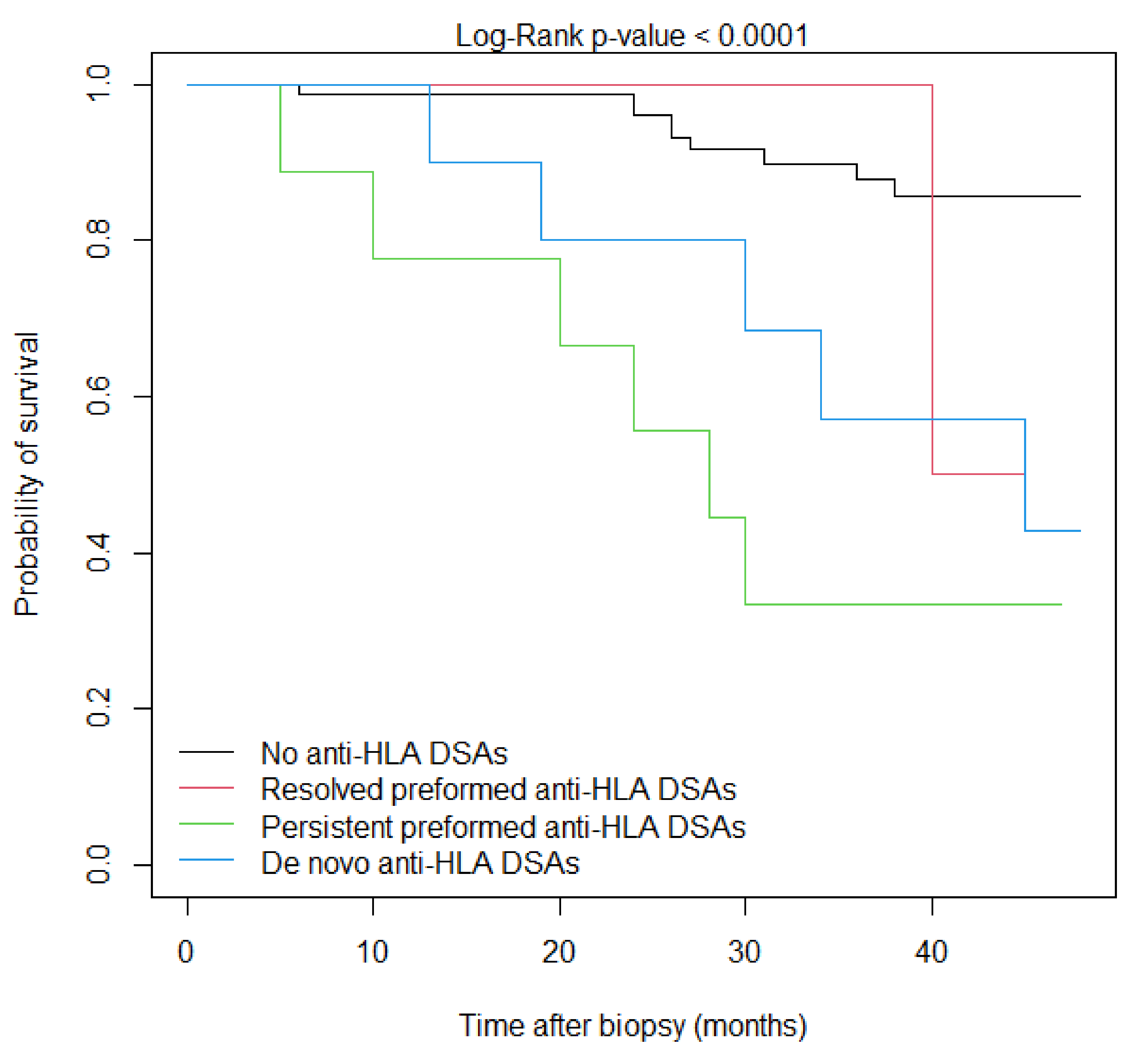
3.4. Survival Analysis
3.5. Factors Associated with DSA Status
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konvalinka, A.; Tinckam, K. Utility of HLA Antibody Testing in Kidney Transplantation. J. Am. Soc. Nephrol. 2015, 26, 1489–1502. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, H.C.; Gebel, H.M.; Bray, R.A. Understanding solid-phase HLA antibody assays and the value of MFI. Hum. Immunol. 2017, 78, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Viglietti, D.; Loupy, A.; Vernerey, D.; Bentlejewski, C.; Gosset, C.; Aubert, O.; Duong van Huyen, J.P.; Jouven, X.; Legendre, C.; Glotz, D.; et al. Value of Donor-Specific Anti-HLA Antibody Monitoring and Characterization for Risk Stratification of Kidney Allograft Loss. J. Am. Soc. Nephrol. 2017, 28, 702–715. [Google Scholar] [CrossRef]
- Muñoz-Herrera, C.M.; Gutiérrez-Bautista, J.F.; López-Nevot, M.Á. Complement Binding Anti-HLA Antibodies and the Survival of Kidney Transplantation. J. Clin. Med. 2023, 12, 2335. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R. Donor-Specific Antibodies in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2018, 13, 182–192. [Google Scholar] [CrossRef]
- Oweira, H.; Ramouz, A.; Ghamarnejad, O.; Khajeh, E.; Ali-Hasan-Al-Saegh, S.; Nikbakhsh, R.; Reißfelder, C.; Rahbari, N.; Mehrabi, A.; Sadeghi, M. Risk Factors of Rejection in Renal Transplant Recipients: A Narrative Review. J. Clin. Med. 2022, 11, 1392. [Google Scholar] [CrossRef]
- Sharma, A.; Cherukuri, A.; Mehta, R.B.; Sood, P.; Hariharan, S. High Calcineurin Inhibitor Intrapatient Variability Is Associated with Renal Allograft Inflammation, Chronicity, and Graft Loss. Transplant. Direct 2019, 5, e424. [Google Scholar] [CrossRef]
- Coti, I.; Wenda, S.; Andreeva, A.; Kocher, A.; Laufer, G.; Fischer, G.; Andreas, M. Donor-specific HLA antibodies after fresh decellularized vs cryopreserved native allograft implantation. Hla 2020, 96, 580–588. [Google Scholar] [CrossRef]
- Snanoudj, R.; Kamar, N.; Cassuto, E.; Caillard, S.; Metzger, M.; Merville, P.; Thierry, A.; Jollet, I.; Grimbert, P.; Anglicheau, D.; et al. Epitope load identifies kidney transplant recipients at risk of allosensitization following minimization of immunosuppression. Kidney Int. 2019, 95, 1471–1485. [Google Scholar] [CrossRef]
- Senev, A.; Lerut, E.; Van Sandt, V.; Coemans, M.; Callemeyn, J.; Sprangers, B.; Kuypers, D.; Emonds, M.P.; Naesens, M. Specificity, strength, and evolution of pretransplant donor-specific HLA antibodies determine outcome after kidney transplantation. Am. J. Transplant. 2019, 19, 3100–3113. [Google Scholar] [CrossRef]
- Redondo-Pachón, D.; Pérez-Sáez, M.J.; Mir, M.; Gimeno, J.; Llinás, L.; García, C.; Hernández, J.J.; Yélamos, J.; Pascual, J.; Crespo, M. Impact of persistent and cleared preformed HLA DSA on kidney transplant outcomes. Hum. Immunol. 2018, 79, 424–431. [Google Scholar] [CrossRef]
- Ziemann, M.; Altermann, W.; Angert, K.; Arns, W.; Bachmann, A.; Bakchoul, T.; Banas, B.; von Borstel, A.; Budde, K.; Ditt, V.; et al. Preformed Donor-Specific HLA Antibodies in Living and Deceased Donor Transplantation: A Multicenter Study. Clin. J. Am. Soc. Nephrol. 2019, 14, 1056–1066. [Google Scholar] [CrossRef]
- Aubert, O.; Loupy, A.; Hidalgo, L.; Duong van Huyen, J.-P.; Higgins, S.; Viglietti, D.; Jouven, X.; Glotz, D.; Legendre, C.; Lefaucheur, C.; et al. Antibody-Mediated Rejection Due to Preexisting versus De Novo Donor-Specific Antibodies in Kidney Allograft Recipients. J. Am. Soc. Nephrol. 2017, 28, 1912–1923. [Google Scholar] [CrossRef]
- Haas, M.; Mirocha, J.; Reinsmoen, N.L.; Vo, A.A.; Choi, J.; Kahwaji, J.M.; Peng, A.; Villicana, R.; Jordan, S.C. Differences in pathologic features and graft outcomes in antibody-mediated rejection of renal allografts due to persistent/recurrent versus de novo donor-specific antibodies. Kidney Int. 2017, 91, 729–737. [Google Scholar] [CrossRef]
- Loupy, A.; Suberbielle-Boissel, C.; Hill, G.S.; Lefaucheur, C.; Anglicheau, D.; Zuber, J.; Martinez, F.; Thervet, E.; Méjean, A.; Charron, D.; et al. Outcome of subclinical antibody-mediated rejection in kidney transplant recipients with preformed donor-specific antibodies. Am. J. Transplant. 2009, 9, 2561–2570. [Google Scholar] [CrossRef]
- Yamamoto, T.; Watarai, Y.; Takeda, A.; Tsujita, M.; Hiramitsu, T.; Goto, N.; Narumi, S.; Katayama, A.; Morozumi, K.; Uchida, K.; et al. De Novo Anti-HLA DSA Characteristics and Subclinical Antibody-Mediated Kidney Allograft Injury. Transplantation 2016, 100, 2194–2202. [Google Scholar] [CrossRef]
- Madill-Thomsen, K.S.; Böhmig, G.A.; Bromberg, J.; Einecke, G.; Eskandary, F.; Gupta, G.; Hidalgo, L.G.; Myslak, M.; Viklicky, O.; Perkowska-Ptasinska, A.; et al. Donor-Specific Antibody Is Associated with Increased Expression of Rejection Transcripts in Renal Transplant Biopsies Classified as No Rejection. J. Am. Soc. Nephrol. 2021, 32, 2743–2758. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Louis, K.; Morris, A.B.; Taupin, J.L.; Nickerson, P.; Tambur, A.R.; Gebel, H.M.; Reed, E.F. Clinical recommendations for posttransplant assessment of anti-HLA (Human Leukocyte Antigen) donor-specific antibodies: A Sensitization in Transplantation: Assessment of Risk consensus document. Am. J. Transplant. 2023, 23, 115–132. [Google Scholar] [CrossRef]
- Gniewkiewicz, M.; Czerwinska, K.; Zielniok, K.; Durlik, M. Association of Circulating Anti-HLA Donor-Specific Antibodies and Their Characteristics, including C1q-Binding Capacity, in Kidney Transplant Recipients with Long-Term Renal Graft Outcomes. J. Clin. Med. 2023, 12, 1312. [Google Scholar] [CrossRef]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef]
- Bestard, O.; Thaunat, O.; Bellini, M.I.; Böhmig, G.A.; Budde, K.; Claas, F.; Couzi, L.; Furian, L.; Heemann, U.; Mamode, N.; et al. Alloimmune Risk Stratification for Kidney Transplant Rejection. Transplant. Int. 2022, 35, 10138. [Google Scholar] [CrossRef] [PubMed]
- Markkinen, S.; Helanterä, I.; Lauronen, J.; Lempinen, M.; Partanen, J.; Hyvärinen, K. Mismatches in Gene Deletions and Kidney-related Proteins as Candidates for Histocompatibility Factors in Kidney Transplantation. Kidney Int. Rep. 2022, 7, 2484–2494. [Google Scholar] [CrossRef] [PubMed]
- Schinstock, C.A.; Gandhi, M.J.; Stegall, M.D. Interpreting Anti-HLA Antibody Testing Data: A Practical Guide for Physicians. Transplantation 2016, 100, 1619–1628. [Google Scholar] [CrossRef] [PubMed]
- Caillard, S.; Becmeur, C.; Gautier-Vargas, G.; Olagne, J.; Muller, C.; Cognard, N.; Perrin, P.; Braun, L.; Heibel, F.; Lefebre, F.; et al. Pre-existing donor-specific antibodies are detrimental to kidney allograft only when persistent after transplantation. Transplant. Int. 2017, 30, 29–40. [Google Scholar] [CrossRef]
- Kimball, P.M.; Baker, M.A.; Wagner, M.B.; King, A. Surveillance of alloantibodies after transplantation identifies the risk of chronic rejection. Kidney Int. 2011, 79, 1131–1137. [Google Scholar] [CrossRef]
- Kenta, I.; Takaaki, K. Molecular Mechanisms of Antibody-Mediated Rejection and Accommodation in Organ Transplantation. Nephron 2020, 144 (Suppl. 1), 2–6. [Google Scholar] [CrossRef]
- Irving, C.A.; Carter, V.; Gennery, A.R.; Parry, G.; Griselli, M.; Hasan, A.; Kirk, C.R. Effect of persistent versus transient donor-specific HLA antibodies on graft outcomes in pediatric cardiac transplantation. J. Heart Lung Transplant. 2015, 34, 1310–1317. [Google Scholar] [CrossRef]
- Le Pavec, J.; Suberbielle, C.; Lamrani, L.; Feuillet, S.; Savale, L.; Dorfmüller, P.; Stephan, F.; Mussot, S.; Mercier, O.; Fadel, E. De-novo donor-specific anti-HLA antibodies 30 days after lung transplantation are associated with a worse outcome. J. Heart Lung Transplant. 2016, 35, 1067–1077. [Google Scholar] [CrossRef]
- Abu-Elmagd, K.M.; Wu, G.; Costa, G.; Lunz, J.; Martin, L.; Koritsky, D.A.; Murase, N.; Irish, W.; Zeevi, A. Preformed and de novo donor specific antibodies in visceral transplantation: Long-term outcome with special reference to the liver. Am. J. Transplant. 2012, 12, 3047–3060. [Google Scholar] [CrossRef]
- Fujiyama, N.; Satoh, S.; Saito, M.; Numakura, K.; Inoue, T.; Yamamoto, R.; Saito, T.; Kanda, S.; Narita, S.; Mitobe, Y.; et al. Impact of persistent preformed and de novo donor-specific antibodies detected at 1 year after kidney transplantation on long-term graft survival in Japan: A retrospective study. Clin. Exp. Nephrol. 2019, 23, 1398–1406. [Google Scholar] [CrossRef]
- Betjes, M.G.H.; Sablik, K.S.; Otten, H.G.; Roelen, D.L.; Claas, F.H.; de Weerd, A. Pretransplant Donor-Specific Anti-HLA Antibodies and the Risk for Rejection-Related Graft Failure of Kidney Allografts. J. Transplant. 2020, 2020, 5694670. [Google Scholar] [CrossRef]
- Del Bello, A.; Congy-Jolivet, N.; Muscari, F.; Lavayssière, L.; Esposito, L.; Cardeau-Desangles, I.; Guitard, J.; Dörr, G.; Suc, B.; Duffas, J.P.; et al. Prevalence, Incidence and Risk Factors for Donor-Specific Anti-HLA Antibodies in Maintenance Liver Transplant Patients. Am. J. Transplant. 2014, 14, 867–875. [Google Scholar] [CrossRef]
- Grimaldi, V.; Pagano, M.; Moccia, G.; Maiello, C.; De Rosa, P.; Napoli, C. Novel insights in the clinical management of hyperimmune patients before and after transplantation. Curr. Res. Immunol. 2023, 4, 100056. [Google Scholar] [CrossRef]
- Leal, R.; Pardinhas, C.; Martinho, A.; Sá, H.O.; Figueiredo, A.; Alves, R. Strategies to Overcome HLA Sensitization and Improve Access to Retransplantation after Kidney Graft Loss. J. Clin. Med. 2022, 11, 5753. [Google Scholar] [CrossRef]


{kind=link}
| No Anti-HLA DSAs (N = 80) | Resolved Preformed Anti-HLA DSAs (N = 9) | Persistent Preformed Anti-HLA DSAs (N = 9) | De Novo Anti-HLA DSAs (N = 10) | p-Value | |
|---|---|---|---|---|---|
| Recipient characteristic | |||||
| Age at biopsy, years, median (Q1–Q3) | 45.0 (38.0–62.0) | 49.0 (45.0–54.0) | 54.0 (44.0–61.0) | 51.0 (45.3–55.0) | 0.9637 |
| Male, n (%) | 53 (66.3) | 5 (55.6) | 4 (44.4) | 7 (70.0) | 0.5517 |
| Body mass index at biopsy, kg/m2, mean ± SD | 24.9 ± 4.03 | 26.6 ± 3.15 | 24.2 ± 2.82 | 24.3 ± 3.56 | 0.1589 |
| Previous transplantation, n (%) | 2 (2.5) | 2 (22.2) | 7 (77.8) | 8 (80.0) | <0.0001 |
| Renal replacement therapy, n (%) | 0.9640 | ||||
| Pre-emptive transplantation | 10 (12.5) | 1 (11.1) | 0 | 1 (10.0) | |
| Hemodialysis | 60 (75.0) | 7 (77.8) | 8 (88.9) | 8 (80.0) | |
| Peritoneal dialysis | 10 (12.5) | 1 (11.1) | 1 (11.1) | 1 (10.0) | |
| Cause of ESRD, n (%) | 0.6475 | ||||
| Glomerulonephritis | 31 (38.8) | 5 (55.6) | 5 (55.6) | 7 (70.0) | |
| ADPKD | 13 (16.3) | 2 (22.2) | 2 (22.2) | 2 (20.0) | |
| Diabetes | 14 (17.5) | 0 | 1 (11.1) | 1 (10.0) | |
| Congenital anomaly | 4 (5.0) | 1 (11.1) | 0 | 0 | |
| Other | 18 (22.4) | 1 (11.1) | 1 (11.1) | 0 | |
| Diabetes, n (%) | 24 (30.0) | 2 (22.2) | 2 (22.2) | 3 (30.0) | 0.9311 |
| Donor characteristics | |||||
| Age, years, mean ± SD | 44.8 ± 15.04 | 46.9 ± 14.07 | 57.9 ± 9.24 | 46.7 ± 15.44 | 0.1306 |
| Male, n (%) | 53 (66.3) | 5 (55.6) | 5 (55.6) | 5 (50.0) | 0.6789 |
| Transplant characteristics | |||||
| Cold ischemia time, minutes, mean ± SD | 1239 ± 607.1 | 1242 ± 450.9 | 1271 ± 390.3 | 1562 ± 753.3 | 0.4476 |
| Induction therapy, n (%) | <0.0001 | ||||
| None | 68 (85.0) | 2 (22.2) | 1 (11.1) | 4 (40.0) | |
| Basiliximab | 8 (10.0) | 2 (22.2) | 3 (33.3) | 5 (50.0) | |
| ATG | 4 (5.0) | 5 (55.6) | 5 (55.6) | 1 (10.0) | |
| HLA mismatches, median, (Q1–Q3) | |||||
| A | 1.0 (1.0–2.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.8) | 0.3588 |
| B | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.5407 |
| DR | 1.0 (0.8–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 0.3914 |
| Total | 3.0 (3.0–4.0) | 3.0 (3.0–4.0) | 3.0 (3.0–4.0) | 4.0 (3.0–4.0) | 0.7966 |
| Panel-reactive antibody >5%, n (%) | 7 (8.8) | 1 (11.1) | 5 (55.6) | 2 (20.0) | 0.0017 |
| Panel-reactive antibody, median (Q1–Q3) | 0 (0–0) | 0 (0–0) | 57 (0–33) | 0 (0–0) | 0.0015 |
| Clinical characteristics | |||||
| Immunosuppression, n (%) | 0.2455 | ||||
| Tacrolimus | 79 (98.7) | 9 (100.0) | 9 (100.0) | 9 (90.0) | |
| Cyclosporine | 1 (1.3) | 0 | 0 | 1 (10.0) | |
| eGFR at biopsy, mL/min/1.73 m2, mean ± SD | 54.4 ± 21.78 | 56.8 ± 16.47 | 40.9 ± 16.23 | 51.1 ± 17.39 | 0.2406 |
| Proteinuria at biopsy ≥50 mg/dL, n (%) | 10 (12.5) | 1 (11.1) | 3 (33.3) | 2 (20.0) | 0.3770 |
| Proteinuria at biopsy, median (Q1–Q3) | 0 (0–10) | 0 (0–0) | 0 (0–50) | 5 (0–10) | 0.4762 |
| Protocol biopsy n (%) | 45 (56.3) | 7 (77.8) | 5 (55.6) | 4 (40.0) | 0.4284 |
| Time from transplantation to biopsy, months, median (Q1–Q3) | 5 (3–12) | 4 (3–12) | 4 (3–7) | 4 (3–11) | 0.8841 |
| ABMR at the time of biopsy, n (%) | 3 (3.8) | 2 (22.2) | 2 (22.2) | 2 (20.0) | 0.0363 |
| C4d in biopsy, n (%) | 10 (12.5) | 0 | 2 (22.2) | 2 (20.0) | 0.4792 |
| Resolved Preformed Anti-HLA DSAs (N = 9) | Persistent Preformed Anti-HLA DSAs (N = 9) | p-Value | |
|---|---|---|---|
| All anti-HLA DSAs | |||
| Number, median (Q1–Q3) | 1.0 (1.0–1.0) | 1 (1.0–2.0) | 0.5008 |
| HLA class specificity, n (%) | 0.5796 | ||
| I | 6 (66.7) | 5 (55.6) | |
| II | 3 (33.3) | 3 (33.3) | |
| I + II | 0 | 1 (11.1) | |
| DSAs with the highest MFI | |||
| HLA class specificity, n (%) | 1 | ||
| I | 6 (66.7) | 5 (55.6) | |
| II | 3 (33.3) | 4 (44.4) | |
| MFI, median (Q1–Q3) | 983 (786–3110) | 1905 (1381–2889) | 0.4363 |
| Persistent Preformed Anti-HLA DSAs (N = 9) | De Novo Anti-HLA DSAs (N = 10) | p-Value | |
|---|---|---|---|
| All anti-HLA DSAs | |||
| Number, median (Q1–Q3) | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 0.1457 |
| HLA class specificity, n (%) | 0.1572 | ||
| I | 4 (44.5) | 3 (30.0) | |
| II | 3 (33.3) | 7 (70.0) | |
| I + II | 2 (22.2) | 0 | |
| DSAs with the highest MFI | |||
| HLA class specificity, n (%) | 0.5085 | ||
| I | 5 (55.5) | 3 (30.0) | |
| II | 4 (44.5) | 7 (70.0) | |
| MFI, median (Q1–Q3) | 3843 (2900–6206) | 1693 (903–3832) | 0.1564 |
| C1q binding, n (%) | 6 (66.7) | 4 (40.0) | 0.4825 |
| IgG subclasses, n (%) | |||
| IgG1 | 7 (77.8) | 7 (70.0) | 1 |
| IgG2 | 1 (11.1) | 1 (10.0) | 1 |
| IgG3 | 3 (33.3) | 4 (40.0) | 1 |
| IgG4 | 1 (11.1) | 3 (30.0) | 0.6564 |
| No Anti-HLA DSAs (N = 80) | Resolved Preformed Anti-HLA DSAs (N = 9) | Persistent Preformed Anti-HLA DSAs (N = 9) | De Novo Anti-HLA DSAs (N = 10) | p-Value | |
|---|---|---|---|---|---|
| Follow-up after biopsy, months, median (Q1–Q3) | 38.5 (28.0–44.3) | 33.0 (29.0–39.0) | 45.0 (41.0–47.0) | 41.5 (36.3–46.5) | 0.1969 |
| eGFR at the end of follow-up, mL/min/1.73 m2, median (Q1–Q3) | 51.0 (34.5–64.5) | 54.0 (45.0–62.0) | 23.5 (17.8–36.3) | 40.0 (32.0–50.0) | 0.0188 |
| Proteinuria at the end of follow-up ≥50 mg/dL, n (%) | 2 (2.5) | 1 (12.5) | 3 (42.9) | 0 | 0.0001 |
| Proteinuria at the end of follow-up, median (Q1–Q3) | 0 (0–0) | 0 (0–0) | 0 (0–51.5) | 0 (0–0) | 0.2471 |
| >30% decline in eGFR, n (%) | 8 (10.0) | 1 (11.1) | 6 (66.7) | 5 (50.0) | <0.0001 |
| Death-censored graft loss, n (%) | 1 (1.3) | 0 | 2 (22.2) | 1 (10.0) | 0.0095 |
| Combined endpoint: >30% decline in eGFR or graft loss, n (%) | 9 (11.3) | 1 (11.1) | 6 (66.7) | 5 (50.0) | <0.0001 |
| Time from biopsy to combined endpoint, months, mean ± SD | 25.3 ± 9.05 | 40 | 19.5 ± 10.03 | 28.2 ± 12.60 | 0.2714 |
| Death event, n (%) | 4 (5.0) | 0 | 2 (22.2) | 0 | 0.1151 |
| DSA Status | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| No anti-HLA DSAs | Ref. | ||
| Resolved preformed anti-HLA DSAs | 1.07 | 0.136–8.481 | 0.9470 |
| Persistent preformed anti-HLA DSAs | 8.18 | 2.902–23.03 | <0.0001 |
| De novo anti-HLA DSAs | 4.61 | 1.541–13.793 | 0.0063 |
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Donor’s age (per 1-year increase) | 1.03 | 0.999–1.066 | 0.0530 |
| Proteinuria at biopsy ≥50 mg/dL (vs. <50 mg/dL) | 1.02 | 1.001–1.036 | 0.0428 |
| DSA status | |||
| No anti-HLA DSAs | Ref. | ||
| Resolved preformed anti-HLA DSAs | 1.10 | 0.139–8.676 | 0.9305 |
| Persistent preformed anti-HLA DSAs | 5.96 | 2.041–17.431 | 0.0011 |
| De novo anti-HLA DSAs | 4.48 | 1.483–13.520 | 0.0079 |
| Variable | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Resolved preformed anti-HLA DSAs | |||
| Induction therapy (ATG vs. None) | 18.25 | 7.40–44.97 | 0.0013 |
| Induction therapy (Basiliximab vs. None) | 4.56 | 1.61–12.87 | 0.1434 |
| Persistent preformed anti-HLA DSAs | |||
| Previous transplantation (yes vs. no) | 25.77 | 10.34–64.23 | 0.0004 |
| Donor’s age (per 1-year increase) | 1.08 | 1.04–1.13 | 0.0424 |
| De novo anti-HLA DSAs | |||
| Previous transplantation (yes vs. no) | 31.64 | 13.48–74.23 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gniewkiewicz, M.; Czerwinska, K.; Zielniok, K.; Durlik, M. Impact of Resolved Preformed, Persistent Preformed, and De Novo Anti-HLA Donor-Specific Antibodies in Kidney Transplant Recipients on Long-Term Renal Graft Outcomes. J. Clin. Med. 2023, 12, 3361. https://doi.org/10.3390/jcm12103361
Gniewkiewicz M, Czerwinska K, Zielniok K, Durlik M. Impact of Resolved Preformed, Persistent Preformed, and De Novo Anti-HLA Donor-Specific Antibodies in Kidney Transplant Recipients on Long-Term Renal Graft Outcomes. Journal of Clinical Medicine. 2023; 12(10):3361. https://doi.org/10.3390/jcm12103361
Chicago/Turabian StyleGniewkiewicz, Michal, Katarzyna Czerwinska, Katarzyna Zielniok, and Magdalena Durlik. 2023. "Impact of Resolved Preformed, Persistent Preformed, and De Novo Anti-HLA Donor-Specific Antibodies in Kidney Transplant Recipients on Long-Term Renal Graft Outcomes" Journal of Clinical Medicine 12, no. 10: 3361. https://doi.org/10.3390/jcm12103361
APA StyleGniewkiewicz, M., Czerwinska, K., Zielniok, K., & Durlik, M. (2023). Impact of Resolved Preformed, Persistent Preformed, and De Novo Anti-HLA Donor-Specific Antibodies in Kidney Transplant Recipients on Long-Term Renal Graft Outcomes. Journal of Clinical Medicine, 12(10), 3361. https://doi.org/10.3390/jcm12103361