
Pre- and Post-Operative Hamstring Autograft ACL Reconstruction Isokinetic Knee Strength Assessments of Recreational Athletes
 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Approach of the Study
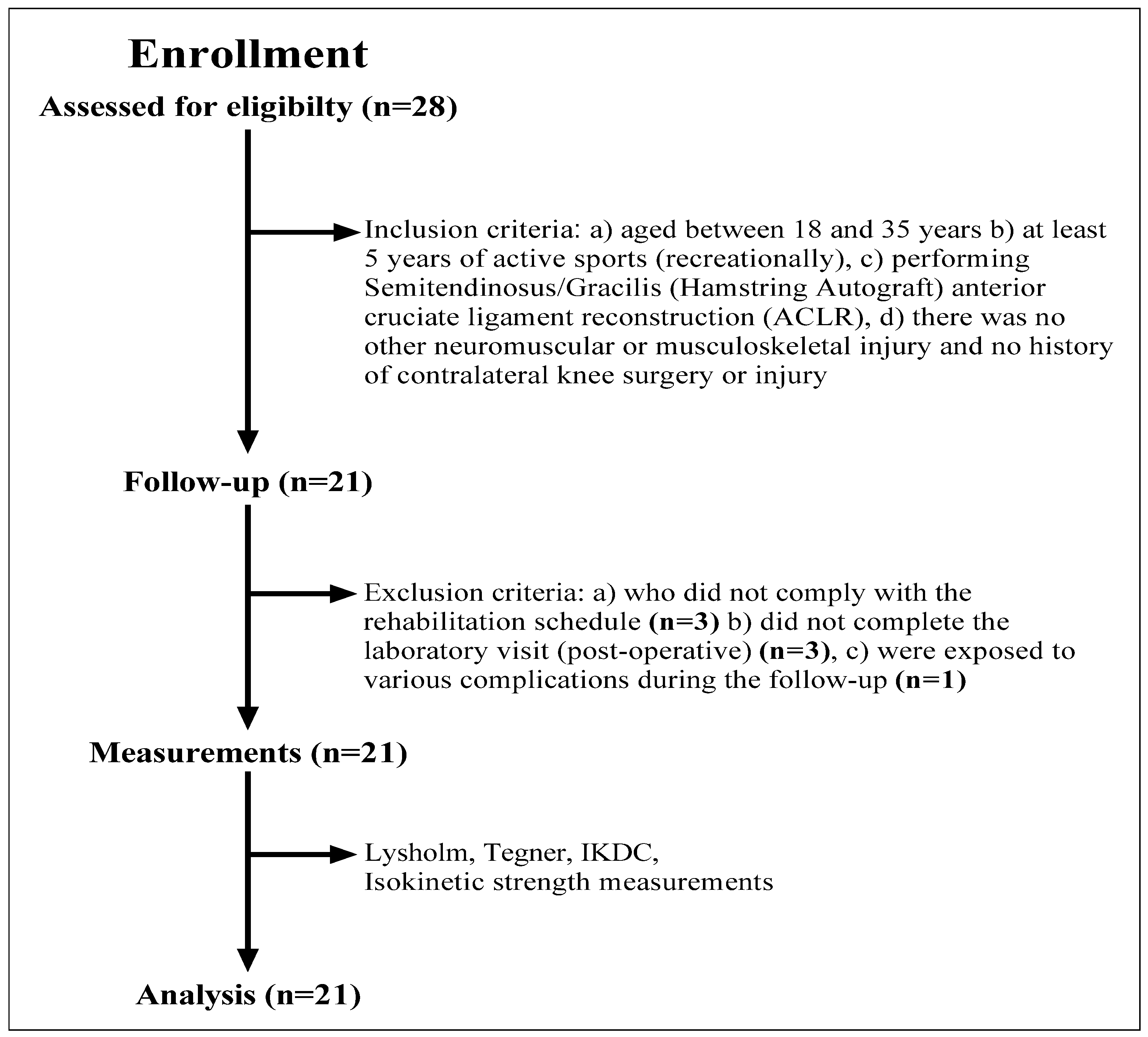
2.2. Patients
2.3. Surgical Treatment (Semitendinosus/Gracilis Autograft)
2.4. Procedures
2.4.1. Anthropometric Measures
2.4.2. Isokinetic Strength Measurement
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sport following anterior cruciate ligament reconstruction surgery: A systematic review and meta-analysis of the state of play. Br. J. Sports Med. 2011, 45, 596–606. [Google Scholar] [CrossRef]
- Petersen, W.; Fink, C.; Kopf, S. Return to sports after ACL reconstruction: A paradigm shift from time to function. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1353–1355. [Google Scholar] [CrossRef] [PubMed]
- Hart, J.M.; Pietrosimone, B.; Hertel, J.; Ingersoll, C.D. Quadriceps activation following knee injuries: A systematic review. J. Athl. Train. 2010, 45, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Nicoletti, P.; Baldin, G.; Bragazzi, N.L.; Crimì, A.; Ruggieri, P. Hamstring Strain Injury (HSI) Prevention in Professional and Semi-Professional Football Teams: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8272. [Google Scholar] [CrossRef] [PubMed]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebresten, L.; Bahr, R.; Krosshaug, T. Mechanisms for noncontact anterior cruciate ligament injuries: Knee joint kinematics in 10 injury situations from female team handball and basketball. Am. J. Sports Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef] [PubMed]
- Pua, Y.H.; Bryant, A.L.; Steele, J.R.; Newton, R.U.; Wrigley, T.V. Isokinetic dynamometry in anterior cruciate ligament injury and reconstruction. Ann. Acad. Med. 2008, 37, 330. [Google Scholar]
- Middleton, K.K.; Hamilton, T.; Irrgang, J.J.; Karlsson, J.; Harner, C.D.; Fu, F.H. Anatomic anterior cruciate ligament (ACL) reconstruction: A global perspective. Part 1. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1467–1482. [Google Scholar] [CrossRef]
- Abrams, G.D.; Harris, J.D.; Gupta, A.K.; McCormick, F.M.; Bush-Joseph, C.A.; Verma, N.N.; Cole, B.J.; Bach, B.R., Jr. Functional performance testing after anterior cruciate ligament reconstruction: A systematic review. Orthop. J. Sports Med. 2014, 2, 2325967113518305. [Google Scholar] [CrossRef]
- Myer, G.D.; Paterno, M.V.; Ford, K.R.; Quatman, C.E.; Hewett, T.E. Rehabilitation after anterior cruciate ligament reconstruction: Criteria-based progression through the return-to-sport phase. J. Orthop. Sports Phys. Ther. 2006, 36, 385–402. [Google Scholar] [CrossRef]
- Rivera-Brown, A.M.; Frontera, W.R.; Fontanez, R.; Micheo, W.F. Evidence for isokinetic and functional testing in return to sport decisions following ACL surgery. PMR 2022, 14, 678–690. [Google Scholar]
- Ohji, S.; Aizawa, J.; Hirohata, K.; Ohmi, T.; Mitomo, S.; Koga, H.; Yagishita, K. Single-leg hop can result in higher limb symmetry index than isokinetic strength and single-leg vertical jump following anterior cruciate ligament reconstruction. Knee 2021, 29, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Herbawi, F.; Lozano-Lozano, M.; Lopez-Garzon, M.; Postigo-Martin, P.; Ortiz-Comino, L.; Martin-Alguacil, J.L.; Fernandez-Lao, C. A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts. Int. J. Environ. Res. Public Health 2022, 19, 6764. [Google Scholar] [CrossRef] [PubMed]
- Kehribar, L.; Yılmaz, A.K.; Karaduman, E.; Kabadayı, M.; Bostancı, Ö.; Sürücü, S.; Mahiroğulları, M. Post-Operative Results of ACL Reconstruction Techniques on Single-Leg Hop Tests in Athletes: Hamstring Autograft vs. Hamstring Grafts Fixed Using Adjustable Cortical Suspension in Both the Femur and Tibia. Medicina 2022, 58, 435. [Google Scholar] [CrossRef]
- Ermiş, E.; Yilmaz, A.K.; Kabadayi, M.; Bostanci, Ö.; Mayda, M.H. Bilateral and ipsilateral peak torque of quadriceps and hamstring muscles in elite judokas. J. Musculoskelet. Neuronal Interact. 2019, 19, 286. [Google Scholar] [PubMed]
- Yılmaz, A.K.; Kabadayı, M. Electromyographic responses of knee isokinetic and single-leg hop tests in athletes: Dominant vs. non-dominant sides. Res. Sport. Med. 2020, 30, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Kellis, E.; Baltzopoulos, V. Isokinetic eccentric exercise. Sports Med. 1995, 19, 202–222. [Google Scholar] [CrossRef] [PubMed]
- Lepley, L.K.; Palmieri-Smith, R.M. Pre-operative quadriceps activation is related to post-operative activation, not strength, in patients post-ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Logerstedt, D.S.; Hunter-Giordano, A.; Axe, M.J.; Snyder-Mackler, L. Current concepts for anterior cruciate ligament reconstruction: A criterionbased rehabilitation progression. J. Orthop. Sports Phys Ther. 2012, 42, 601–614. [Google Scholar] [CrossRef]
- Fukuda, T.Y.; Fingerhut, D.; Moreira, V.C.; Camarini, P.M.; Scodeller, N.F.; Duarte, A., Jr.; Martinelli, M.; Bryk, F.F. Open kinetic chain exercises in a restricted range of motion after anterior cruciate ligament reconstruction: A randomized controlled clinical trial. Am. J. Sports Med. 2013, 41, 788–794. [Google Scholar] [CrossRef]
- Riesterer, J.; Mauch, M.; Paul, J.; Gehring, D.; Ritzmann, R.; Wenning, M. Relationship between pre-and post-operative isokinetic strength after ACL reconstruction using hamstring autograft. BMC Sports Sci. Med. Rehabil. 2020, 12, 68. [Google Scholar] [CrossRef]
- Biz, C.; Cigolotti, A.; Zonta, F.; Belluzzi, E.; Ruggieri, P. ACL reconstruction using a bone patellar tendon bone (BPTB) allograft or a hamstring tendon autograft (GST): A single-center comparative study. Acta Bio Med. 2019, 90 (Suppl. 12), 109. [Google Scholar]
- Roger, J.; Bertani, A.; Vigouroux, F.; Mottier, F.; Gaillard, R.; Have, L.; Rongièras, F. ACL reconstruction using a quadruple semitendinosus graft with cortical fixations gives suitable isokinetic and clinical outcomes after 2 years. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2468–2477. [Google Scholar] [CrossRef] [PubMed]
- Keays, S.L.; Bullock-Saxton, J.; Keays, A.C.; Newcombe, P. Muscle strength and function before and after anterior cruciate ligament reconstruction using semitendonosus and gracilis. Knee 2001, 8, 229–234. [Google Scholar] [CrossRef]
- Keays, S.L.; Bullock-Saxton, J.E.; Newcombe, P.; Keays, A.C. The relationship between knee strength and functional stability before and after anterior cruciate ligament reconstruction. J. Orthop. Res. 2003, 21, 231–237. [Google Scholar] [CrossRef]
- Eitzen, I.; Holm, I.; Risberg, M.A. Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2009, 43, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Barber-Westin, S.D.; Noyes, F.R. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. J. Arthrosc. Relat. Surg. 2011, 27, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Webster, K.E. Knee flexor strength recovery following hamstring tendon harvest for anterior cruciate ligament reconstruction: A systematic review. Orthop. Rev. 2009, 1, e12. [Google Scholar] [CrossRef]
- Kyung, H.S.; Lee, H.J.; Oh, C.W.; Hong, H.P. Comparison of results after anterior cruciate ligament reconstruction using a four-strand single semitendinosus or a semitendinosus and gracilis tendon. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 3238–3243. [Google Scholar] [CrossRef]
- Sharma, A.; Flanigan, D.C.; Randall, K.; Magnussen, R.A. Does gracilis preservation matter in anterior cruciate ligament reconstruction? A systematic review. J. Arthrosc. Relat. Surg. 2016, 32, 1165–1173. [Google Scholar] [CrossRef]
- Yosmaoglu, H.B.; Baltaci, G.; Ozer, H.; Atay, A. Efects of additional gracilis tendon harvest on muscle torque, motor coordination, and knee laxity in ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 1287–1292. [Google Scholar] [CrossRef]
- Barenius, B.; Webster, W.K.; McClelland, J.; Feller, J. Hamstring tendon anterior cruciate ligament reconstruction: Does gracilis tendon harvest matter? Int. Orthop. 2013, 37, 207–212. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients Demographics | Mean ± SD | Median (Min–Max) |
|---|---|---|
| Age (years) | 25.6 ± 5.8 | 25 (18–36) |
| Heigh (cm) | 177.9 ± 6.4 | 177 (170–193) |
| Weigh (kg) | 77.9 ± 13.5 | 77 (58–114) |
| BMI (kg/m2) | 24.6 ± 4.3 | 24.3 (18.3–35.2) |
| Follow-up (months) | 6.6 ± 0.5 | 7 (6–7) |
| Surgical side, n (%) | ||
| Right | 12 (64.3) | |
| Left | 9 (35.7) |
| Mean ± SD | Median (Min–Max) | 95% Confidence Interval | Test Statistical | p Value | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Lysholm score | ||||||
| Pre-operation | 73.2 ± 5.8 | 73.5 (65–84) | −28.439 | −21.847 | −3.297 | 0.001 1 |
| Post-operation | 98.4 ± 3 | 100 (90–100) | ||||
| IKDC score | ||||||
| Pre-operation | 48.4 ± 9.2 | 47.5 (36–65) | −45.640 | −30.788 | −11.117 | <0.001 2 |
| Post-operation | 86.6 ± 6.7 | 87 (77–98) | ||||
| Tegner score | ||||||
| Pre-operation | 5.8 ± 1.2 | 6 (4–9) | 0.200 | 0.800 | −2.646 | 0.008 1 |
| Post-operation | 5.3 ± 1.1 | 5 (4–8) | ||||
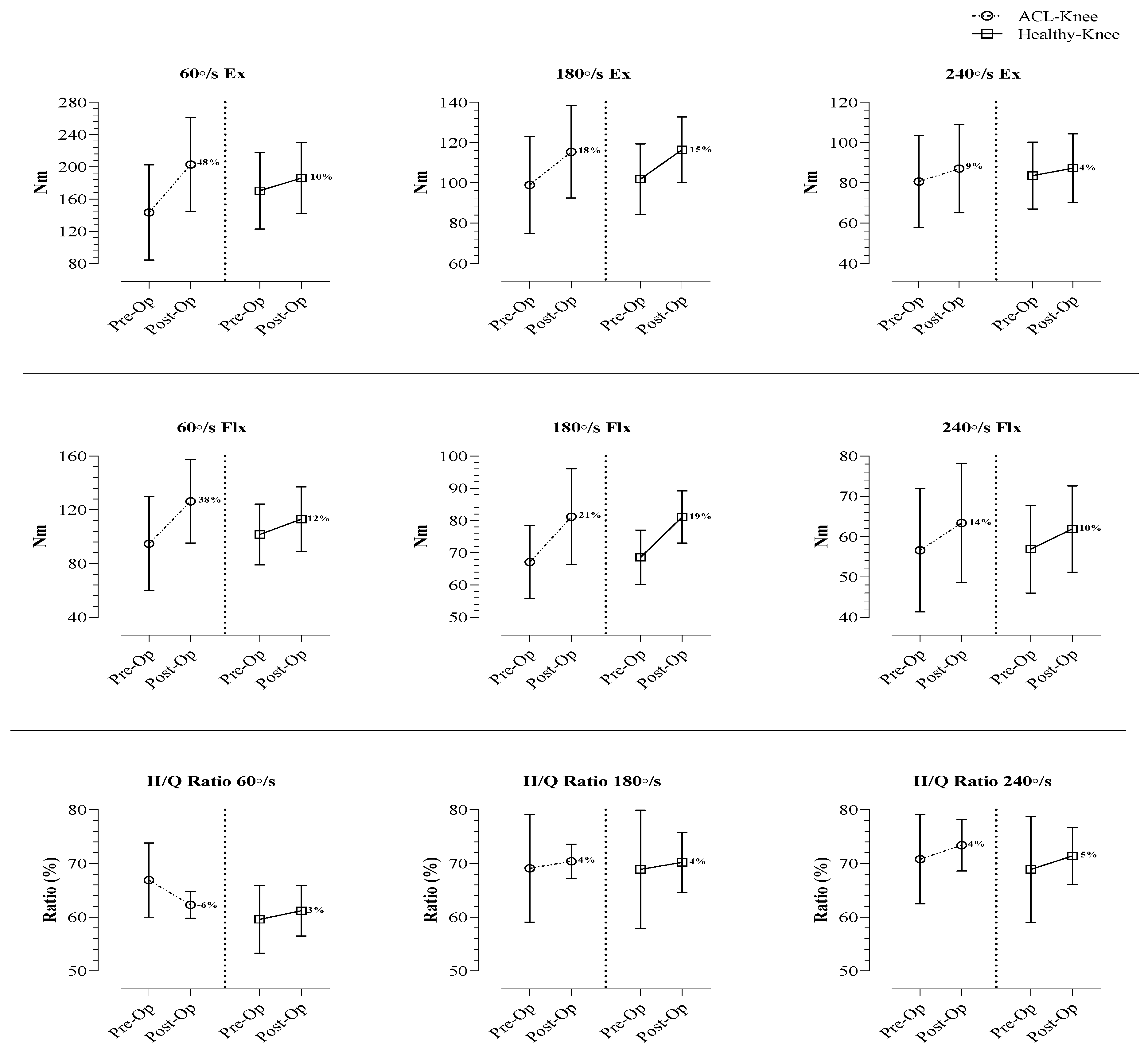
| ACL-Knee | Healthy-Knee | Between Groups | Within Subjects Effects | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Op | Post-Op | Pre-Op | Post-Op | Pre-Op | Post-Op | Time | Group | Time × Group | |||
| Mean ± SD | Mean ± SD | p Value | Mean ± SD | Mean ± SD | p Value | p Value | p Value | p Value | p Value | p Value | |
| Knee peak torque (Nm) | |||||||||||
| 60°/s Ex | 143.4 ± 59.1 | 202.9 ± 58.1 | <0.001 | 170.4 ± 47.6 | 186.1 ± 44.1 | <0.001 | 0.012 | 0.126 | <0.001 | 0.607 | <0.001 |
| 180°/s Ex | 98.9 ± 24 | 115.4 ± 22.9 | <0.001 | 101.8 ± 17.6 | 116.4 ± 16.3 | <0.001 | 0.553 | 0.856 | <0.001 | 0.697 | 0.525 |
| 240°/s Ex | 80.6 ± 22.8 | 87.1 ± 21.9 | <0.001 | 83.6 ± 16.6 | 87.3 ± 17 | <0.001 | 0.507 | 0.972 | <0.001 | 0.709 | 0.047 |
| 60°/s Flx | 94.7 ± 35 | 126.3 ± 35.7 | <0.001 | 101.6 ± 22.6 | 113.1 ± 23.9 | <0.001 | 0.258 | 0.044 | <0.001 | 0.588 | <0.001 |
| 180°/s Flx | 67.1 ± 11.3 | 81.2 ± 14.9 | <0.001 | 68.6 ± 8.4 | 81.1 ± 8.1 | <0.001 | 0.636 | 0.984 | <0.001 | 0.828 | 0.522 |
| 240°/s Flx | 56.6 ± 15.3 | 63.4 ± 14.8 | <0.001 | 56.9 ± 10.9 | 61.9 ± 10.7 | 0.002 | 0.946 | 0.628 | <0.001 | 0.860 | 0.295 |
| H/Q Ratio (%) | |||||||||||
| 60°/s | 66.9 ± 6.9 | 62.3 ± 2.5 | 0.007 | 59.6 ± 6.3 | 61.2 ± 4.7 | 0.014 | 0.001 | 0.168 | 0.091 | 0.002 | <0.001 |
| 180°/s | 69.1 ± 10 | 70.4 ± 3.2 | 0.552 | 68.9 ± 12.1 | 70.2 ± 5.6 | 0.552 | 0.957 | 0.901 | 0.488 | 0.926 | 0.975 |
| 240°/s | 70.8 ± 8.3 | 73.4 ± 4.8 | 0.085 | 68.9 ± 9.9 | 71.4 ± 5.3 | 0.162 | 0.508 | 0.253 | 0.054 | 0.364 | 0.942 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Güzel, N.; Yılmaz, A.K.; Genç, A.S.; Karaduman, E.; Kehribar, L. Pre- and Post-Operative Hamstring Autograft ACL Reconstruction Isokinetic Knee Strength Assessments of Recreational Athletes. J. Clin. Med. 2023, 12, 63. https://doi.org/10.3390/jcm12010063
Güzel N, Yılmaz AK, Genç AS, Karaduman E, Kehribar L. Pre- and Post-Operative Hamstring Autograft ACL Reconstruction Isokinetic Knee Strength Assessments of Recreational Athletes. Journal of Clinical Medicine. 2023; 12(1):63. https://doi.org/10.3390/jcm12010063
Chicago/Turabian StyleGüzel, Nizamettin, Ali Kerim Yılmaz, Ahmet Serhat Genç, Emre Karaduman, and Lokman Kehribar. 2023. "Pre- and Post-Operative Hamstring Autograft ACL Reconstruction Isokinetic Knee Strength Assessments of Recreational Athletes" Journal of Clinical Medicine 12, no. 1: 63. https://doi.org/10.3390/jcm12010063
APA StyleGüzel, N., Yılmaz, A. K., Genç, A. S., Karaduman, E., & Kehribar, L. (2023). Pre- and Post-Operative Hamstring Autograft ACL Reconstruction Isokinetic Knee Strength Assessments of Recreational Athletes. Journal of Clinical Medicine, 12(1), 63. https://doi.org/10.3390/jcm12010063