
Characteristics of Patients Treated with JAK Inhibitors in Rheumatoid Arthritis before versus after VTE Risk Warnings

 , ,
, , 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Outcome Measure
2.3. Statistical Analyses
3. Results
3.1. Study Population
3.2. Comparison of the Baseline Characteristics of Patients Regarding VTE Risk Factors before vs. after EMA’s Warnings
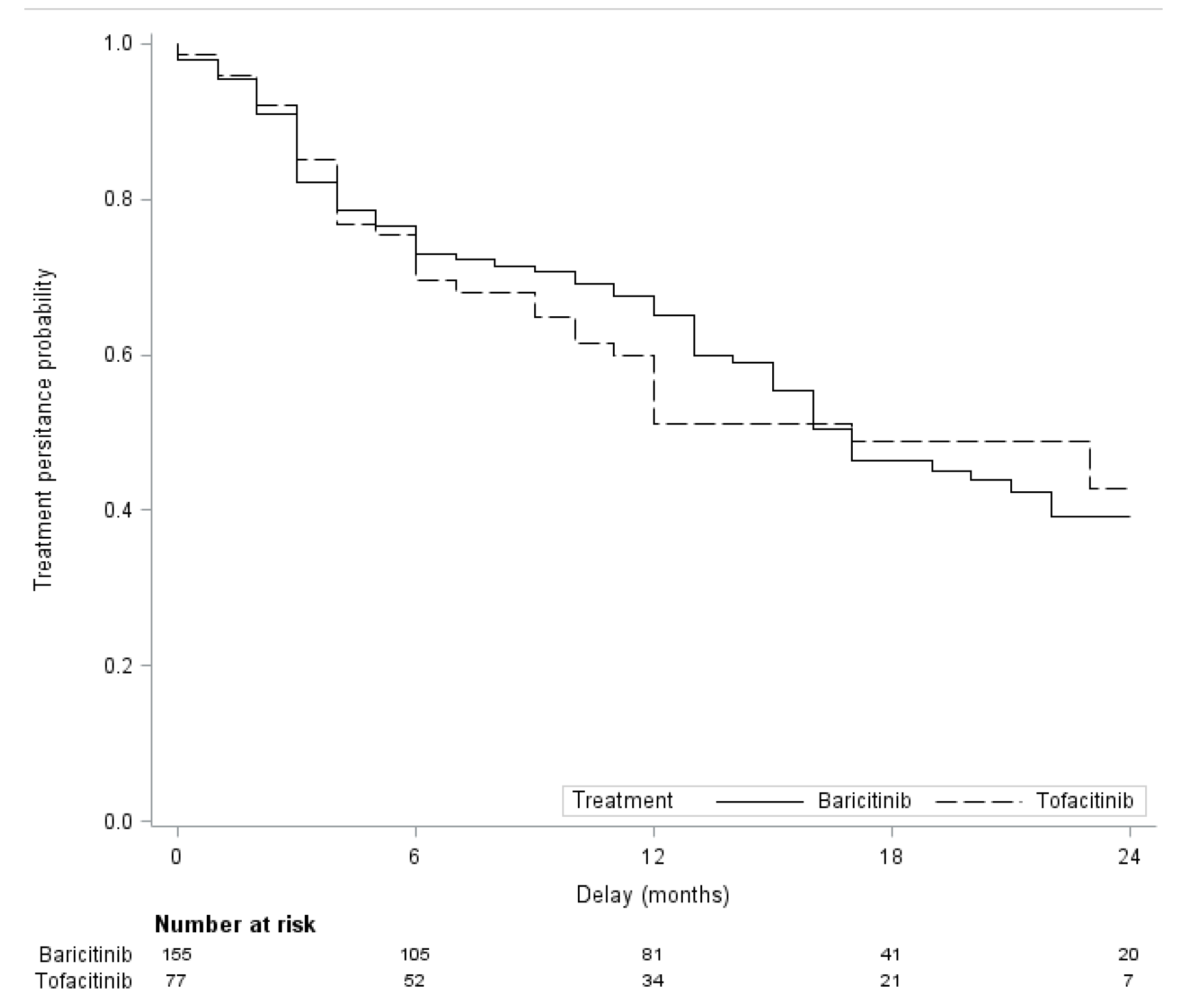
3.3. Persistence of Baricitinib and Tofacitinib
3.3.1. Overall Drug Persistence in Monotherapy vs. Combination with csDMARDs
3.3.2. Overall Drug Persistence Depending on Previous bDMARD Status
3.4. Tolerance
3.5. Focus on VTE Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burmester, G.R.; Pope, J.E. Novel treatment strategies in rheumatoid arthritis. Lancet 2017, 389, 2338–2348. [Google Scholar] [CrossRef]
- Burmester, G.R.; Bijlsma, J.W.J.; Cutolo, M.; McInnes, I.B. Managing rheumatic and musculoskeletal diseases—Past, present and future. Nat. Rev. Rheumatol. 2017, 13, 443–448. [Google Scholar] [CrossRef]
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038, Erratum in Lancet 2016, 388, 1984. [Google Scholar] [CrossRef]
- Morinobu, A. JAK inhibitors for the treatment of rheumatoid arthritis. Immunol. Med. 2020, 43, 148–155. [Google Scholar] [CrossRef]
- Malemud, C.J. The role of the JAK/STAT signal pathway in rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2018, 10, 117–127. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; van Vollenhoven, R.F.; de Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef]
- Taylor, P.C.; Keystone, E.C.; Van Der Heijde, D.; Weinblatt, M.E.; Del Carmen Morales, L.; Gonzaga, J.R.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus Placebo or Adalimumab in Rheumatoid Arthritis. N. Engl. J. Med. 2017, 376, 652–662. [Google Scholar] [CrossRef]
- Dougados, M.; Van Der Heijde, D.; Chen, Y.-C.; Greenwald, M.; Drescher, E.; Liu, J.; Beattie, S.; Witt, S.; De La Torre, I.; Gaich, C.; et al. Baricitinib in patients with inadequate response or intolerance to conventional synthetic DMARDs: Results from the RA-BUILD study. Ann. Rheum. Dis. 2016, 76, 88–95. [Google Scholar] [CrossRef]
- Genovese, M.C.; Kremer, J.; Zamani, O.; Ludivico, C.; Krogulec, M.; Xie, L.; Beattie, S.D.; Koch, A.E.; Cardillo, T.E.; Rooney, T.P.; et al. Baricitinib in Patients with Refractory Rheumatoid Arthritis. N. Engl. J. Med. 2016, 374, 1243–1252. [Google Scholar] [CrossRef]
- Lee, E.B.; Fleischmann, R.; Hall, S.; Wilkinson, B.; Bradley, J.D.; Gruben, D.; Koncz, T.; Krishnaswami, S.; Wallenstein, G.V.; Zang, C.; et al. Tofacitinib versus Methotrexate in Rheumatoid Arthritis. N. Engl. J. Med. 2014, 370, 2377–2386. [Google Scholar] [CrossRef]
- Van der Heijde, D.; Strand, V.; Tanaka, Y.; Keystone, E.; Kremer, J.; Zerbini, C.A.F.; Cardiel, M.H.; Cohen, S.S.; Nash, P.; Song, Y.-W.; et al. Tofacitinib in Combination with Methotrexate in Patients with Rheumatoid Arthritis: Clinical Efficacy, Radiographic, and Safety Outcomes from a Twenty-Four–Month, Phase III Study. Arthritis Rheumatol. 2019, 71, 878–891. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.; Mysler, E.; Hall, S.; Kivitz, A.J.; Moots, R.J.; Luo, Z.; Demasi, R.; Soma, K.; Zhang, R.; Takiya, L.; et al. Efficacy and safety of tofacitinib monotherapy, tofacitinib with methotrexate, and adalimumab with methotrexate in patients with rheumatoid arthritis (ORAL Strategy): A phase 3b/4, double-blind, head-to-head, randomised controlled trial. Lancet 2017, 390, 457–468. [Google Scholar] [CrossRef]
- Sepriano, A.; Kerschbaumer, A.; Smolen, J.S.; van der Heijde, D.; Dougados, M.; van Vollenhoven, R.; McInnes, I.B.; Bijlsma, J.W.; Burmester, G.R.; de Wit, M.; et al. Safety of synthetic and biological DMARDs: A systematic literature review informing the 2019 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann. Rheum. Dis. 2020, 79, 760–770. [Google Scholar] [CrossRef]
- Harigai, M. Growing evidence of the safety of JAK inhibitors in patients with rheumatoid arthritis. Rheumatology 2019, 58, i34–i42. [Google Scholar] [CrossRef]
- Taylor, P.C.; Weinblatt, M.E.; Burmester, G.R.; Rooney, T.P.; Witt, S.; Walls, C.D.; Issa, M.; Salinas, C.A.; Saifan, C.; Zhang, X.; et al. Cardiovascular Safety During Treatment With Baricitinib in Rheumatoid Arthritis. Arthritis Rheumatol. 2019, 71, 1042–1055. [Google Scholar] [CrossRef]
- Mease, P.; Charles-Schoeman, C.; Cohen, S.; Fallon, L.; Woolcott, J.; Yun, H.; Kremer, J.; Greenberg, J.; Malley, W.; Onofrei, A.; et al. Incidence of venous and arterial thromboembolic events reported in the tofacitinib rheumatoid arthritis, psoriasis and psoriatic arthritis development programmes and from real-world data. Ann. Rheum. Dis. 2020, 79, 1400–1413. [Google Scholar] [CrossRef]
- EMA (European Medicines Agency). Restrictions in Use of Xeljanz While EMA Reviews Risk Blood Clots Lungs. 2019. Available online: https://www.ema.europa.eu/en/news/restrictions-use-xeljanz-while-ema-reviews-risk-blood-clots-lungs (accessed on 3 February 2021).
- Desai, R.J.; Pawar, A.; Weinblatt, M.E.; Kim, S.C. Comparative Risk of Venous Thromboembolism in Rheumatoid Arthritis Patients Receiving Tofacitinib Versus Those Receiving Tumor Necrosis Factor Inhibitors: An Observational Cohort Study. Arthritis Rheumatol. 2018, 71, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Deprez, V.; Le Monnier, L.; Sobhy-Danial, J.-M.; Grados, F.; Henry-Desailly, I.; Salomon-Goëb, S.; Rabin, T.; Ristic, S.; Fumery, M.; Fardellone, P.; et al. Therapeutic Maintenance of Baricitinib and Tofacitinib in Real Life. J. Clin. Med. 2020, 9, 3319. [Google Scholar] [CrossRef] [PubMed]
- Daien, C.; Hua, C.; Gaujoux-Viala, C.; Cantagrel, A.; Dubremetz, M.; Dougados, M.; Fautrel, B.; Mariette, X.; Nayral, N.; Richez, C.; et al. Actualisation des Recommandations de la Société française de rhumatologie pour la prise en charge de la polyarthrite rhumatoïde. Rev. Rhum. 2018, 86, 8–24. (In French) [Google Scholar] [CrossRef]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Lee, E.T.; Wang, J. Statistical Methods for Survival Data Analysis, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2003; Available online: https://onlinelibrary.wiley.com/doi/book/10.1002/0471458546 (accessed on 14 December 2022).
- Li, F.; Thomas, L.E. Addressing Extreme Propensity Scores via the Overlap Weights. Am. J. Epidemiol. 2018, 188, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. A comparison of 12 algorithms for matching on the propensity score. Stat. Med. 2013, 33, 1057–1069. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Wakounig, S.; Heinze, G. The estimation of average hazard ratios by weighted Cox regression. Stat. Med. 2009, 28, 2473–2489. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.Y. Cox regression analysis of multivariate failure time data: The marginal approach. Stat. Med. 1994, 13, 2233–2247. [Google Scholar] [CrossRef]
- Mattei, A. Estimating and using propensity score in presence of missing background data: An application to assess the impact of childbearing on wellbeing. Stat. Methods Appl. 2008, 18, 257–273. [Google Scholar] [CrossRef]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- Li, K.-H.; Meng, X.-L.; Raghunathan, T.E.; Rubem, D.B. Significance levels from repeated p-values with multiply-imputed data. Stat Sin. 1991, 1, 65–92. [Google Scholar]
- Bender, R.; Augustin, T.; Blettner, M. Generating survival times to simulate Cox proportional hazards models. Stat. Med. 2005, 24, 1713–1723. [Google Scholar] [CrossRef] [PubMed]
- Burmester, G.R.; Blanco, R.; Charles-Schoeman, C.; Wollenhaupt, J.; Zerbini, C.; Benda, B.; Gruben, D.; Wallenstein, G.; Krishnaswami, S.; Zwillich, S.H.; et al. Tofacitinib (CP-690,550) in combination with methotrexate in patients with active rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitors: A randomised phase 3 trial. Lancet 2013, 381, 451–460. [Google Scholar] [CrossRef]
- Finckh, A.; Tellenbach, C.; Herzog, L.; Scherer, A.; Moeller, B.; Ciurea, A.; Von Muehlenen, I.; Gabay, C.; Kyburz, D.; Brulhart, L.; et al. Comparative effectiveness of antitumour necrosis factor agents, biologics with an alternative mode of action and tofacitinib in an observational cohort of patients with rheumatoid arthritis in Switzerland. RMD Open 2020, 6, e001174. [Google Scholar] [CrossRef]
- Reed, G.W.; Gerber, R.A.; Shan, Y.; Takiya, L.; Dandreo, K.J.; Gruben, D.; Kremer, J.; Wallenstein, G. Real-World Comparative Effectiveness of Tofacitinib and Tumor Necrosis Factor Inhibitors as Monotherapy and Combination Therapy for Treatment of Rheumatoid Arthritis. Rheumatol. Ther. 2019, 6, 573–586. [Google Scholar] [CrossRef] [PubMed]
- Fitton, J.; Melville, A.R.; Emery, P.; Nam, J.L.; Buch, M.H. Real-world single centre use of JAK inhibitors across the rheumatoid arthritis pathway. Rheumatology 2020, 60, 4048–4054. [Google Scholar] [CrossRef]
- Mueller, R.B.; Hasler, C.; Popp, F.; Mattow, F.; Durmisi, M.; Souza, A.; Rubbert-Roth, A.; Schulze-Koops, H.; von Kempis, J. Effectiveness, Tolerability, and Safety of Tofacitinib in Rheumatoid Arthritis: A Retrospective Analysis of Real-World Data from the St. Gallen and Aarau Cohorts. J. Clin. Med. 2019, 8, 1548. [Google Scholar] [CrossRef]
- Caporali, R.; Zavaglia, D. Real-world experience with tofacitinib for the treatment of rheumatoid arthritis. Clin. Exp. Rheumatol. 2018, 37, 485–495. [Google Scholar]
- Doria, A.; Zavaglia, D. Monotherapy is a relevant option in rheumatoid arthritis treatment: A literature review. Clin. Exper. Rheumatol 2019, 37, 862–871. [Google Scholar]
- Desai, R.J.; Pawar, A.; Khosrow-Khavar, F.; Weinblatt, M.E.; Kim, S.C. Risk of venous thromboembolism associated with tofacitinib in patients with rheumatoid arthritis: A population-based cohort study. Rheumatology 2021, 61, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Charles-Schoeman, C.; Fleischmann, R.M.; Mysler, E.; Greenwald, M.; Wang, C.; Chen, A.S.; Connell, C.A.; Woolcott, J.; Menon, S.; Chen, Y.; et al. The Risk of Venous Thromboembolic Events in Patients with RA Aged ≥ 50 Years with ≥ 1 Cardiovascular Risk Factor: Results from a Phase 3b/4 Randomized Safety Study of Tofacitinib vs. TNF Inhibitors. Ann. Rheum. Dis. 2022, 81, 358–359. Available online: https://acrabstracts.org/abstract/the-risk-of-venous-thromboembolic-events-in-patients-with-ra-aged-≥-50-years-with-≥-1-cardiovascular-risk-factor-results-from-a-phase-3b-4-randomized-safety-study-of-tofacitinib-vs-tn/ (accessed on 15 February 2021). [CrossRef]
- Ytterberg, S.R.; Bhatt, D.L.; Mikuls, T.R.; Koch, G.G.; Fleischmann, R.; Rivas, J.L.; Germino, R.; Menon, S.; Sun, Y.; Wang, C.; et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N. Engl. J. Med. 2022, 386, 316–326. [Google Scholar] [CrossRef]
- Yates, M.; Mootoo, A.; Adas, M.; Bechman, K.; Rampes, S.; Patel, V.; Qureshi, S.; Cope, A.P.; Norton, S.; Galloway, J.B. Venous Thromboembolism Risk with JAK Inhibitors: A Meta-Analysis. Arthritis Rheumatol. 2020, 73, 779–788. [Google Scholar] [CrossRef]
- Taylor, P.C.; Takeuchi, T.; Burmester, G.; Durez, P.; Smolen, J.; Deberdt, W.; Zhong, J.; Terres, J.R.; Bello, N.; Winthrop, K. Safety Profile of Baricitinib for the Treatment of Rheumatoid Arthritis up to 9.3 Years: An Updated Integrated Safety Analysis. In Proceedings of the ACR Convergence 2021, Virtual, 5–9 November 2021; Abstract Number 1688. Available online: https://acrabstracts.org/abstract/safety-profile-of-baricitinib-for-the-treatment-of-rheumatoid-arthritis-up-to-9-3-years-an-updated-integrated-safety-analysis/ (accessed on 15 November 2021).
- Cohen, S.B. JAK inhibitors and VTE risk: How concerned should we be? Nat. Rev. Rheumatol. 2021, 17, 133–134. [Google Scholar] [CrossRef] [PubMed]
- Scott, I.C.; Hider, S.L.; Scott, D.L. Thromboembolism with Janus Kinase (JAK) Inhibitors for Rheumatoid Arthritis: How Real is the Risk? Drug Saf. 2018, 41, 645–653. [Google Scholar] [CrossRef]
- Ketfi, C.; Boutigny, A.; Mohamedi, N.; Bouajil, S.; Magnan, B.; Amah, G.; Dillinger, J.-G. Risk of venous thromboembolism in rheumatoid arthritis. Jt. Bone Spine 2020, 88, 105122. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Lu, N.; Avina-Galindo, A.M.; Zheng, Y.; Lacaille, D.; Esdaile, J.M.; Choi, H.K.; Aviña-Zubieta, J.A. The risk and trend of pulmonary embolism and deep vein thrombosis in rheumatoid arthritis: A general population-based study. Rheumatology 2020, 60, 188–195. [Google Scholar] [CrossRef]
- Molander, V.; Bower, H.; Frisell, T.; Askling, J. Risk of venous thromboembolism in rheumatoid arthritis, and its association with disease activity: A nationwide cohort study from Sweden. Ann. Rheum. Dis. 2020, 80, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Samuelson, B.T.; Vesely, S.; Chai-Adisaksopha, C.; Scott, B.L.; Crowther, M.; Garcia, D. The impact of ruxolitinib on thrombosis in patients with polycythemia vera and myelofibrosis. Blood Coagul. Fibrinolysis 2016, 27, 648–652. [Google Scholar] [CrossRef]
- Cohen, S.B.; van Vollenhoven, R.F.; Winthrop, K.L.; Zerbini, C.A.F.; Tanaka, Y.; Bessette, L.; Zhang, Y.; Khan, N.; Hendrickson, B.; Enejosa, J.V.; et al. Safety profile of upadacitinib in rheumatoid arthritis: Integrated analysis from the SELECT phase III clinical programme. Ann. Rheum. Dis. 2020, 80, 304–311. [Google Scholar] [CrossRef]
- Winthrop, K.; Tanaka, Y.; Takeuchi, T.; Kivitz, A.; Genovese, M.; Pechonkina, A.; Matzkies, F.; Bartok, B.; Chen, K.; Jiang, D.; et al. Integrated Safety Analysis Update for Filgotinib in Patients with Moderately to Severely Active Rheumatoid Arthritis Receiving Treatment over a Median of 2.2 Years. In Proceedings of the ACR Convergence 2021, Virtual, 5–9 November 2021; Abstract Number 1698. pp. 354–355. Available online: https://acrabstracts.org/abstract/integrated-safety-analysis-update-for-filgotinib-in-patients-with-moderately-to-severely-active-rheumatoid-arthritis-receiving-treatment-over-a-median-of-2-2-years/ (accessed on 15 November 2021).
- Finckh, A.; Herzog, L.; Scherer, A.; Dudler, J.; Moeller, B.; Ciurea, A.; Mueller, R.; Hasler, P.; Exer, P.; von Muehlenen, I.; et al. THU0174 Drug retention of tofacitinib versus biologic antirheumatic agents in rheumatoid arthritis: Observational data from the swiss scqm registry. Ann. Rheum. Dis. 2017, 76, 267. [Google Scholar] [CrossRef]
- Schneeberger, E.; Salas, A.; Medina, L.; Zacariaz, J.; Mantilla, R.; Sarmiento-Monroy, J.; Elizondo, L.; Garro, B.; Madariaga, H.; Gόrriz, L.; et al. AB0419 Real world use of tofacitinib in rheumatoid arthritis: Data from Latin America. BMJ 2017, 76, 1196–1197. [Google Scholar] [CrossRef]
- Cohen, S.; Curtis, J.R.; DeMasi, R.; Chen, Y.; Fan, H.; Soonasra, A.; Fleischmann, R. Worldwide, 3-Year, Post-Marketing Surveillance Experience with Tofacitinib in Rheumatoid Arthritis. Rheumatol. Ther. 2018, 5, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Khosrow-Khavar, F.; Desai, R.; Lee, H.; Lee, S.; Kim, S. Risk of Malignancy in Patients Treated with Tofacitinib: Results from the Safety of TofAcitinib in Routine Care Patients with Rheumatoid Arthritis (STAR-RA) Study. In Proceedings of the ACR Convergence 2021, Virtual, 5–9 November 2021; Available online: https://acrabstracts.org/abstract/risk-of-malignancy-in-patients-treated-with-tofacitinib-results-from-the-safety-of-tofacitinib-in-routine-care-patients-with-rheumatoid-arthritis-star-ra-study (accessed on 15 November 2021). Abstract Number 1675.
- Khosrow-Khavar, F.; Kim, S.; Lee, H.; Lee, S.; Desai, R. Risk of Cardiovascular Outcomes in Patients Treated with Tofacitinib: First Results from the Safety of TofAcitinib in Routine Care Patients with Rheumatoid Arthritis (STAR-RA) Study. In Proceedings of the ACR Convergence 2021, 5–9 November 2021; Abstract Number 1939. Available online: https://acrabstracts.org/abstract/risk-of-cardiovascular-outcomes-in-patients-treated-with-tofacitinib-first-results-from-the-safety-of-tofacitinib-in-routine-care-patients-with-rheumatoid-arthritis-star-ra-study (accessed on 15 November 2021).
- European Medicines Agency. Janus Kinase Inhibitors (JAKi) Article-20 referral-EMA recommends measures to minimise risk of serious side effects with Janus kinase inhibitors for chronic inflammatory disorders. Eur. Med. Agency. 2020. Available online: https://www.ema.europa.eu/en/medicines/human/referrals/janus-kinase-inhibitors-jaki. (accessed on 7 November 2022).


{kind=link}
| Before Propensity Score-Matching | After Propensity Score-Matching | |||||
|---|---|---|---|---|---|---|
| Parameters | Baricitinib n = 155 | Tofacitinib n = 77 | ASD (%) | Baricitinib n = 116 | Tofacitinib n = 70 | ASD (%) |
| Women | 118 (76.1) | 51 (66.2) | 21.7 | 82 (70.8) | 49 (69.6) | 2.7 |
| Age (years), mean ± SD | 59.6 ± 14.2 | 56.7 ± 13.4 | 20.9 | 58.7 ± 15.3 | 57.6 ± 13.1 | 7.8 |
| BMI (kg/m2), mean ± SD | 27.0 ± 6.3 | 27.0 ± 6.8 | 4.2 | 26.8 ± 6.6 | 27.0 ± 6.5 | 3.0 |
| Smoking status | 31.5 | 14.3 | ||||
| Non-smoker | 94 (60.7) | 33 (43.4) | 60 (51.2) | 32 (46.1) | ||
| Former smoker | 31 (20.1) | 19 (24.9) | 28 (23.9) | 18 (24.9) | ||
| Current smoker | 30 (19.2) | 24 (31.7) | 28 (24.5) | 20 (29.0) | ||
| RA duration (years), median (IQR) | 11 (4 to 20) | 11 (6 to 19) | 10.1 * | 12 (6 to 20) | 12 (5 to 19) | 3.0 * |
| Seropositivity status | 21.7 | 8.5 | ||||
| RF +/ACPA + | 123 (79.4) | 55 (70.6) | 89 (76.6) | 53 (75.6) | ||
| RF +/ACPA − | 11 (7.1) | 8 (10.6) | 10 (8.3) | 7 (9.3) | ||
| RF −/ACPA + | 8 (5.2) | 7 (9.5) | 7 (6.4) | 4 (6.3) | ||
| RF −/ACPA − | 13 (8.4) | 7 (9.2) | 10 (8.8) | 6 (8.9) | ||
| Erosion | 106 (68.6) | 58 (75.7) | 15.7 | 86 (74.3) | 53 (75.7) | 3.3 |
| Baseline CRP (mg/L), median (IQR) | 7.0 (1.1 to 25.6) | 9.9 (2.6 to 27.0) | 12.5 * | 7.7 (1.8 to 26.8) | 10.0 (2.7 to 27.2) | 4.0 * |
| Prior bDMARD | 27.7 | 7.8 | ||||
| Naïve (0) | 23 (14.8) | 7 (9.1) | 12 (10.7) | 7 (10.0) | ||
| 1 or 2 | 50 (32.3) | 34 (44.2) | 45 (38.8) | 29 (42.0) | ||
| 3 or more | 82 (52.9) | 36 (46.8) | 59 (50.6) | 34 (48.0) | ||
| Concomitant csDMARD | 62 (38.7) | 29 (37.4) | 5.5 | 43 (37.1) | 27 (38.7) | 3.4 |
| Before May 2019 n = 161 | After May 2019 n = 71 | p-Value | |
|---|---|---|---|
| Age (years), mean ± SD | 59.1 ± 13.6 | 57.5 ± 14.8 | 0.40 |
| BMI (kg/m2), mean ± SD | 27.4 ± 6.2 | 26.0 ± 5.1 | 0.17 |
| Smoking status | 0.65 | ||
| Non-smoker | 62/110 (56.4) | 22/43 (51.2) | |
| Former smoker | 25/110 (22.7) | 9/43 (20.9) | |
| Current smoker | 23/110 (20.9) | 12/43 (27.9) | |
| Personal history of DVT | 10/161 (6.2) | 1/71 (1.4) | 0.18 |
| Personal history of PE | 7/161 (4.3) | 2/71 (2.8) | 0.73 |
| Neoplastic history | 12/161 (7.5) | 5/71 (7.0) | 0.91 |
| n | Baricitinib Rate, % | n | Tofacitinib Rate,% | HR (95%CI) | p-Value | |
|---|---|---|---|---|---|---|
| Unadjusted analysis | 155 | 60.7 | 77 | 57.2 | 1.02 (0.68 to 1.53) | 0.93 |
| PSOW analysis | 155 | 60.9 | 77 | 56.4 | 0.96 (0.52 to 1.74) | 0.89 |
| PS-matched analysis | 116 | 61.8 | 70 | 56.1 | 0.93 (0.59 to 1.45) | 0.75 |
| Gender/Age | RA Characteristics | Molecule/Dose/Line JAK | Comorbidities | MTEV Type | Delay of Occurring | Management Death | Treatment Discontinuation |
|---|---|---|---|---|---|---|---|
| Patient 1 F. 77 yo | 9 years of evolution RF+/ACPA+ Introduction BEFORE May 2019 | BARI 4 mg/day Monotherapy + prednisone 10 mg/day 4th line or more | BMI 35.2 Former smoker | PE | 23 months | Ambulatory DOAC No death | No Dose reduction (BARI 4 to BARI 2 mg) Discontinuation 6 months later due to secondary inefficacy |
| Patient 2 F. 72 yo | Unknown years of evolution RF+/ACPA+ Introduction BEFORE May 2019 | BARI 4 mg/day Monotherapy + prednisone 10 mg/day 4th line or more + | BMI 35.6 Smoking status unknown AHT FA (DOAC) Stroke 2 DVT (oral contraception) | PE + DVT | 13 months | Hospitalization IV anticoagulant then DOAC No death | Yes |
| Patient 3 F. 82 yo | 34 years of evolution RF+/ACPA+ Introduction BEFORE May 2019 | BARI 2 mg/day Monotherapy + prednisone 5 mg/day 4th line or more | BMI 22.2 Smoking status unknown AHT 2 EP (surgery) | PE | 9 months | Hospitalization IV anticoagulant then DOAC No death | Yes |
| Patient 4 F. 42 yo | 5 years of evolution RF+/ACPA+ Introduction AFTER May 2019 | TOFA 5 mg BID Monotherapy + prednisone (unknown posology) 4th line or more | Unknown BMI Former smoker AHT | DVT | 9 months | Ambulatory No information available about AC treatment No death | Yes |
| Patient 5 F. 66 yo | 15 years of evolution RF+/ACPA- Introduction BEFORE May 2019 | BARI 4 mg/day Monotherapy + prednisone 5 mg/day 4th line or more | BMI 31.3 Never smoked | DVT + PE | 20 months | Ambulatory DOAC No death | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Philippoteaux, C.; Deprez, V.; Nottez, A.; Cailliau, E.; Houvenagel, E.; Deprez, X.; Philippe, P.; Pascart, T.; Flipo, R.-M.; Goëb, V.; et al. Characteristics of Patients Treated with JAK Inhibitors in Rheumatoid Arthritis before versus after VTE Risk Warnings. J. Clin. Med. 2023, 12, 207. https://doi.org/10.3390/jcm12010207
Philippoteaux C, Deprez V, Nottez A, Cailliau E, Houvenagel E, Deprez X, Philippe P, Pascart T, Flipo R-M, Goëb V, et al. Characteristics of Patients Treated with JAK Inhibitors in Rheumatoid Arthritis before versus after VTE Risk Warnings. Journal of Clinical Medicine. 2023; 12(1):207. https://doi.org/10.3390/jcm12010207
Chicago/Turabian StylePhilippoteaux, Cécile, Valentine Deprez, Aurore Nottez, Emeline Cailliau, Eric Houvenagel, Xavier Deprez, Peggy Philippe, Tristan Pascart, René-Marc Flipo, Vincent Goëb, and et al. 2023. "Characteristics of Patients Treated with JAK Inhibitors in Rheumatoid Arthritis before versus after VTE Risk Warnings" Journal of Clinical Medicine 12, no. 1: 207. https://doi.org/10.3390/jcm12010207
APA StylePhilippoteaux, C., Deprez, V., Nottez, A., Cailliau, E., Houvenagel, E., Deprez, X., Philippe, P., Pascart, T., Flipo, R.-M., Goëb, V., & Letarouilly, J.-G. (2023). Characteristics of Patients Treated with JAK Inhibitors in Rheumatoid Arthritis before versus after VTE Risk Warnings. Journal of Clinical Medicine, 12(1), 207. https://doi.org/10.3390/jcm12010207