
Tricuspid Structural Valve Deterioration Treated with a Transcatheter Valve-in-Valve Implantation: A Single-Center Prospective Registry

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
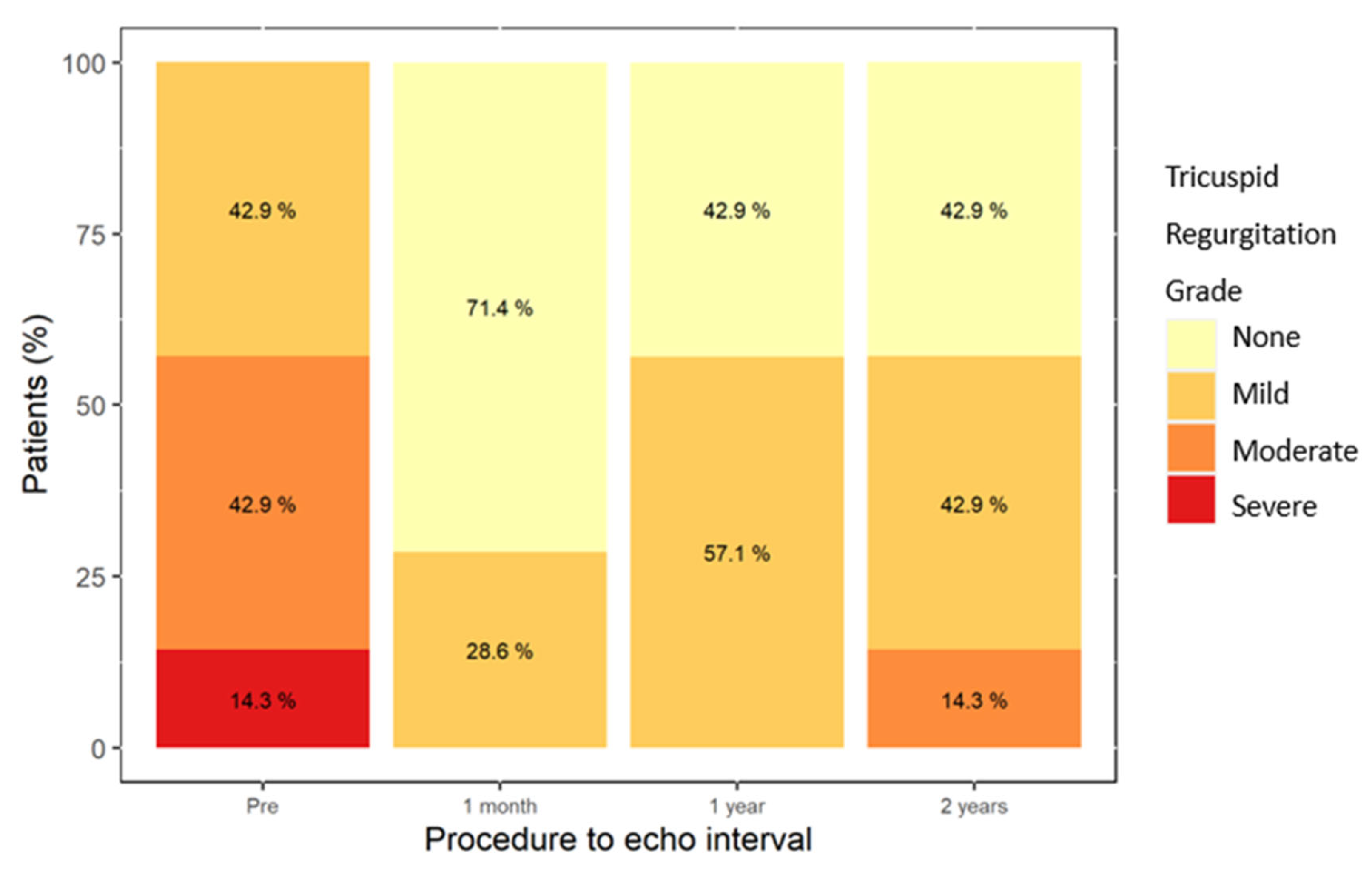
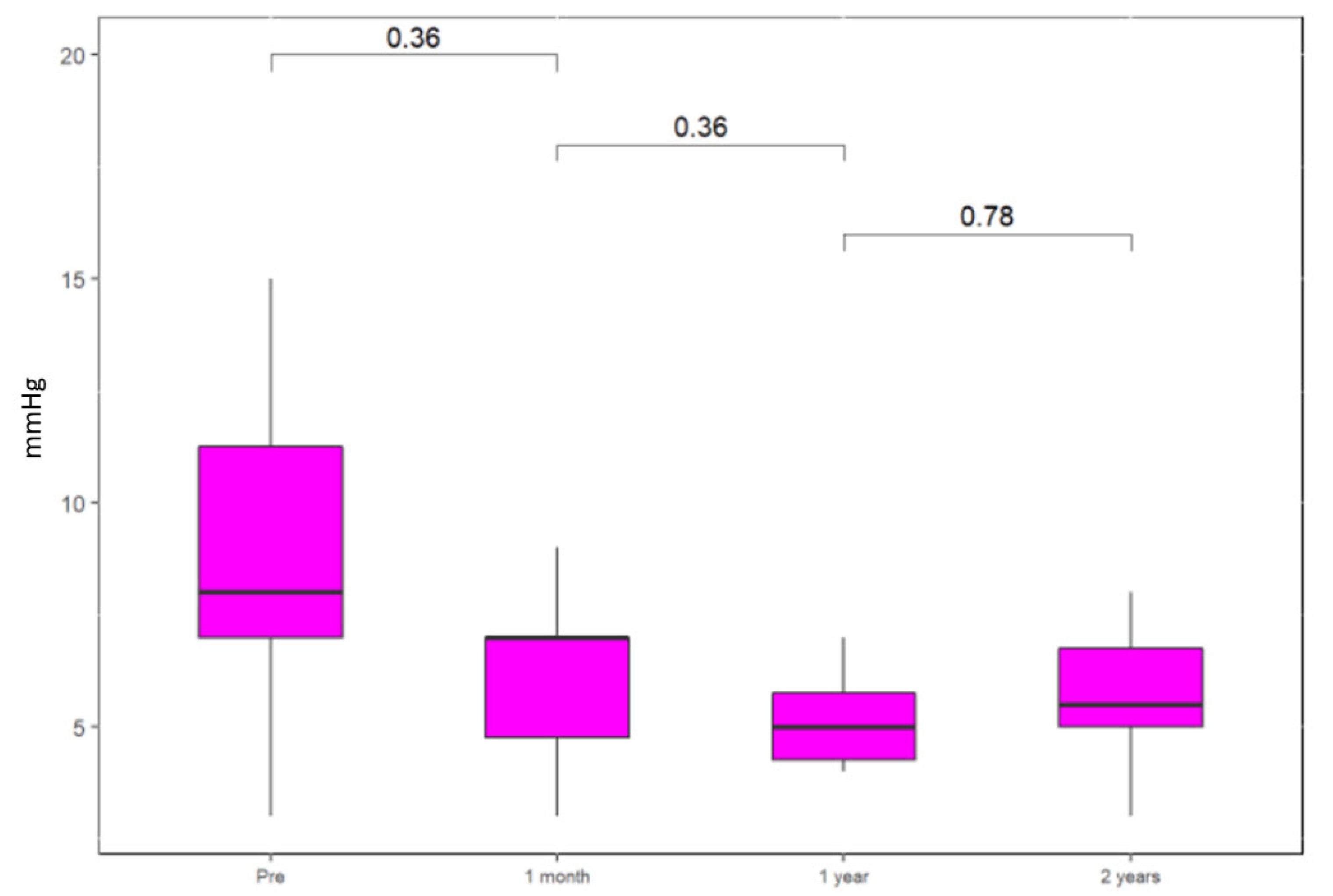
3.1. Hemodynamic Parameters
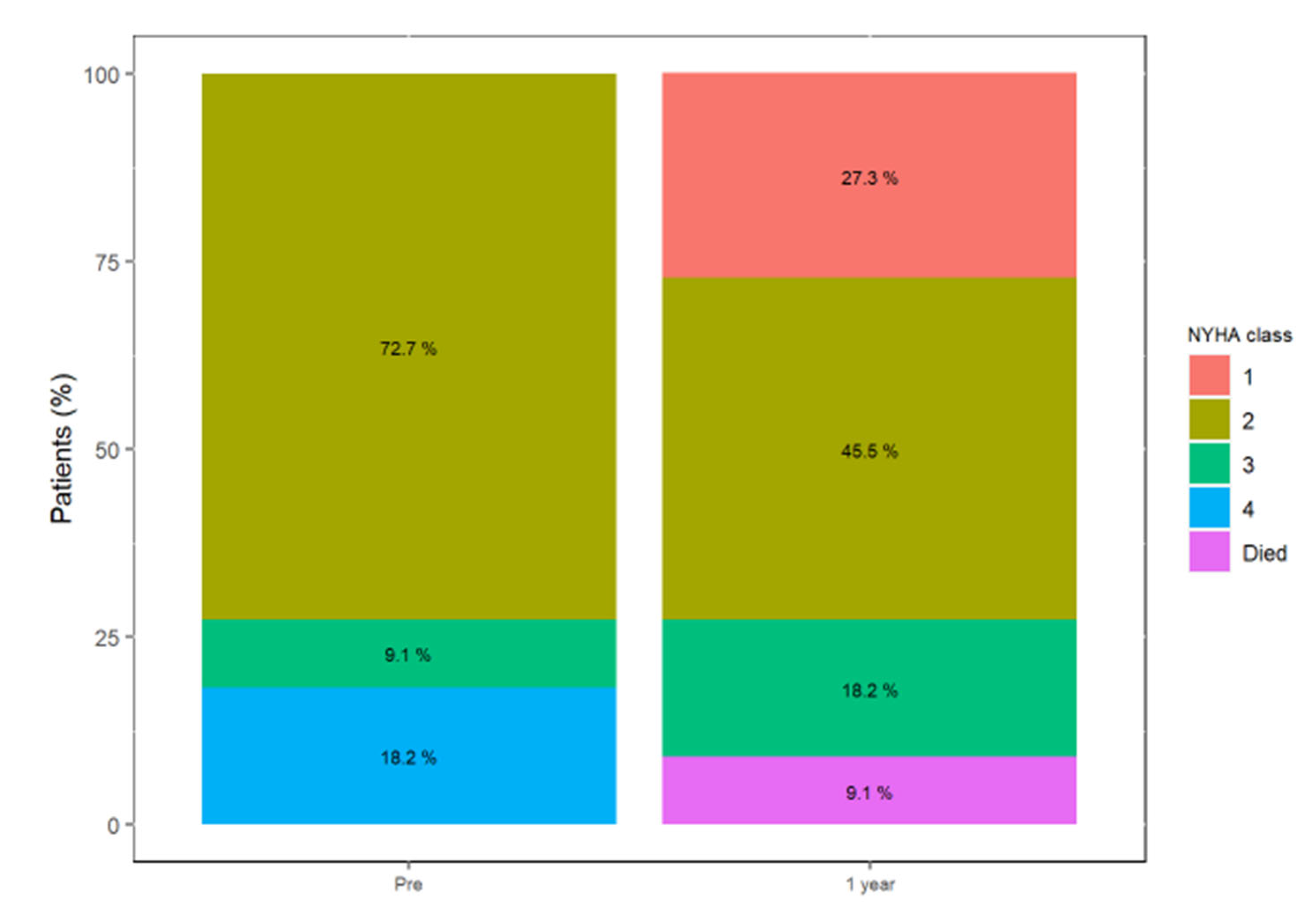
3.2. Functional Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: Executive summary: A report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Taggart, N.W.; Cabalka, A.K.; Eicken, A.; Aboulhosn, J.A.; Thomson, J.D.R.; Whisenant, B.; Bocks, M.L.; Schubert, S.; Jones, T.K.; Asnes, J.D.; et al. Outcomes of Transcatheter Tricuspid Valve-in-Valve Implantation in Patients with Ebstein Anomaly. Am. J. Cardiol. 2018, 121, 262–268. [Google Scholar] [CrossRef] [PubMed]
- McElhinney, D.B.; Aboulhosn, J.A.; Dvir, D.; Whisenant, B.; Zhang, Y.; Eicken, A.; Ribichini, F.; Tzifa, A.; Hainstock, M.R.; Martin, M.H.; et al. Mid-Term Valve-Related Outcomes After Transcatheter Tricuspid Valve-in-Valve or Valve-in-Ring Replacement. J. Am. Coll. Cardiol. 2019, 73, 148–157. [Google Scholar] [CrossRef]
- Asmarats, L.; Puri, R.; Latib, A.; Navia, J.L.; Rodés-Cabau, J. Transcatheter tricuspid valve interventions: Landscape, challenges, and future directions. J. Am. Coll. Cardiol. 2018, 71, 2935–2956. [Google Scholar] [CrossRef]
- Guenther, T.; Noebauer, C.; Mazzitelli, D.; Busch, R.; Tassani-Prell, P.; Lange, R. Tricuspid valve surgery: A thirty-year assessment of early and late outcome. Eur. J. Cardiothorac. Surg. 2008, 34, 402–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dreyfus, J.; Flagiello, M.; Bazire, B.; Eggenspieler, F.; Viau, F.; Riant, E.; Mbaki, Y.; Bohbot, Y.; Eyharts, D.; Sénage, T.; et al. Isolated tricuspid valve surgery: Impact of aetiology and clinical presentation on outcomes. Eur. Heart J. 2020, 41, 4304–4317. [Google Scholar] [CrossRef] [PubMed]
- Dannenberg, V.; Donà, C.; Koschutnik, M.; Winter, M.-P.; Nitsche, C.; Kammerlander, A.A.; Bartko, P.E.; Hengstenberg, C.; Mascherbauer, J.; Goliasch, G.; et al. Transcatheter treatment by valve-in-valve and valve-in-ring implantation for prosthetic tricuspid valve dysfunction. Wien. Klin. Wochenschr. 2021, 133, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.-L.; An, Z.; Ma, Y.; Song, Z.-G.; Cai, C.-L.; Li, B.-L.; Zhou, G.W.; Han, L.; Wang, J.; Bai, Y.F.; et al. Transcatheter tricuspid valve replacement in patients with severe tricuspid regurgitation. Heart 2021, 107, 1664–1670. [Google Scholar] [CrossRef] [PubMed]
- Panaich, S.S.; Eleid, M.F. Tricuspid valve-in-valve implantation for failing bioprosthetic valves: An evolving standard of care. Ann. Transl. Med. 2016, 4, 410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McElhinney, D.B.; Cabalka, A.K.; Aboulhosn, J.A.; Eicken, A.; Boudjemline, Y.; Schubert, S.; Himbert, D.; Asnes, J.D.; Salizzoni, S.; Bocks, M.L.; et al. Transcatheter Tricuspid Valve-in-Valve Implantation for the Treatment of Dysfunctional Surgical Bioprosthetic Valves: An International, Multicenter Registry Study. Circulation 2016, 133, 1582–1593. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TT-ViV (n = 12) | Mean/Percentage |
|---|---|
| Age (years ± SD) | 65.4 ± 11.9 |
| Male (%) | 10 (83.3) |
| BMI (units) | 26.6 ± 7.1 |
| STS | 4.1 ± 3.1 |
| Euroscore II | 5.4 ± 3.4 |
| Coronary artery disease (%) | 1 (8.3) |
| Prior coronary artery bypass surgery (%) | 0 |
| Prior PCI (%) | 1 (9.1) |
| Diabetes mellitus | 6 (50) |
| Hypertension | 7 (58.3) |
| Chronic dialysis | 0 (0) |
| Chronic obstructive pulmonary disease | 2 (16.7) |
| Atrial fibrillation/flutter | 10 (83.3) |
| Permanent pacemaker/defibrillator | 5 (41.7) |
| NYHA functional class III/IV | 4 (33.3) |
| Hemoglobin (g/dL) | 11.6 ± 2.3 |
| GFR (MDRD) | 62.6 ± 24.3 |
| Albumin | 4.2 ± 0.4 |
| Systolic pulmonary artery pressure (mmHg) | 24.5 ± 27.4 |
| Size of valve treated (mm) | |
| 27 | 2 (18.2) |
| 29 | 2 (18.2) |
| 31 | 2 (18.2) |
| 33 | 5 (45.5) |
| LV systolic function | |
| Normal (>50%) | 11 (91.7) |
| Mild (40–49%) | 1 (8.3) |
| Moderate or more tricuspid regurgitation | 4 (33.3) |
| Valve pathology | |
| Stenosis | 4 (33.3) |
| Regurgitation | 5 (41.7) |
| Combined | 3 (25.0) |
| TT-ViV (n = 12) | Number (%) |
|---|---|
| Urgent procedure, n (%) | 1 (8.3) |
| Conscious sedation or local anesthesia only | 7 (58.3) |
| General anesthesia | 5 (41.5) |
| TEE guidance | 7 (58.3) |
| Vascular access via femoral vein | 12 (100) |
| Size of ViV used (mm) | |
| 26 | 2 (16.7) |
| 29 | 10 (83.3) |
| Balloon-expandable valve | 12 (100) |
| Fluoroscopy time (min) | 17.6 ± 14.8 |
| Contrast volume (mL) | 10.0 ± 14.1 |
| Tradename Surgical Valve | Surgical Valve Size | Number of Previous Tricuspid Interventions Prior to TT-ViV | TT-ViV Valve | TT-ViV Size |
|---|---|---|---|---|
| Xenograft | 29 | 2 | Edwards SAPIEN XT | 29 |
| Carpentier Edwards | 33 | 1 | Edwards SAPIEN 3 | 29 |
| Hancock II | 33 | 1 | Edwards SAPIEN 3 | 29 |
| Epic | 33 | 1 | Edwards SAPIEN 3 | 29 |
| Hancock II | 33 | 1 | Edwards SAPIEN 3 | 29 |
| Carpentier Edwards | 27 | 1 | Edwards SAPIEN 3 | 26 |
| Hancock II 29 | 29 | 1 | Edwards SAPIEN 3 | 29 |
| Carpentier Edwards | 31 | 1 | Edwards SAPIEN 3 | 29 |
| Carpentier Edwards | 33 | 2 | Edwards SAPIEN 3 | 29 |
| Hancock II | 27 | 1 | Edwards SAPIEN 3 | 26 |
| Carpentier Edwards | 31 | 1 | Edwards SAPIEN 3 | 29 |
| Xenograft | Not known | 2 | Edwards SAPIEN 3 | 29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schamroth Pravda, N.; Vaknin Assa, H.; Levi, A.; Witberg, G.; Shapira, Y.; Vaturi, M.; Orvin, K.; Talmor Barkan, Y.; Hamdan, A.; Mishaev, R.; et al. Tricuspid Structural Valve Deterioration Treated with a Transcatheter Valve-in-Valve Implantation: A Single-Center Prospective Registry. J. Clin. Med. 2022, 11, 2667. https://doi.org/10.3390/jcm11092667
Schamroth Pravda N, Vaknin Assa H, Levi A, Witberg G, Shapira Y, Vaturi M, Orvin K, Talmor Barkan Y, Hamdan A, Mishaev R, et al. Tricuspid Structural Valve Deterioration Treated with a Transcatheter Valve-in-Valve Implantation: A Single-Center Prospective Registry. Journal of Clinical Medicine. 2022; 11(9):2667. https://doi.org/10.3390/jcm11092667
Chicago/Turabian StyleSchamroth Pravda, Nili, Hana Vaknin Assa, Amos Levi, Guy Witberg, Yaron Shapira, Mordechai Vaturi, Katia Orvin, Yeela Talmor Barkan, Ashraf Hamdan, Raffael Mishaev, and et al. 2022. "Tricuspid Structural Valve Deterioration Treated with a Transcatheter Valve-in-Valve Implantation: A Single-Center Prospective Registry" Journal of Clinical Medicine 11, no. 9: 2667. https://doi.org/10.3390/jcm11092667
APA StyleSchamroth Pravda, N., Vaknin Assa, H., Levi, A., Witberg, G., Shapira, Y., Vaturi, M., Orvin, K., Talmor Barkan, Y., Hamdan, A., Mishaev, R., Sharoni, R., Perl, L., Sagie, A., Kornowski, R., & Codner, P. (2022). Tricuspid Structural Valve Deterioration Treated with a Transcatheter Valve-in-Valve Implantation: A Single-Center Prospective Registry. Journal of Clinical Medicine, 11(9), 2667. https://doi.org/10.3390/jcm11092667