
Infective Endocarditis in Diabetic Patients: A Different Profile with Prognostic Consequences
 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Methods
Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, C.J.; Chua, S.; Chung, S.Y.; Hang, C.L.; Tsai, T.H. Diabetes mellitus: An independent risk factor of in-hospital mortality in patients with infective endocarditis in a new era of clinical practice. Int. J. Environ. Res. Public Health 2019, 16, 2248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olmos, C.; Vilacosta, I.; Fernández-Pérez, C.; Bernal, J.L.; Ferrera, C.; García-Arribas, D.; Pérez-García, C.; San Román, J.A.; Maroto, L.; Macaya, C.; et al. The evolving nature of infective endocarditis in Spain. A population-based study (2003 to 2014). J. Am. Coll. Cardiol. 2017, 70, 2795–2804. [Google Scholar] [CrossRef] [PubMed]
- De Miguel-Yanes, J.M.; Jiménez-García, R.; Hernández-Barrera, V.; de Miguel-Díez, J.; Méndez-Bailón, M.; Muñoz-Rivas, N.; Pérez-Farinós, N.; López-de-Andrés, A. Infective endocarditis according to type 2 diabetes mellitus status: An observational study in Spain, 2001–2015. Cardiovasc. Diabetol. 2019, 18, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Benvenga, R.M.; De Rosa, R.; Silverio, A.; Matturro, R.; Zambrano, C.; Masullo, A.; Mastrogiovanni, G.; Soriente, L.; Ascoli, R.; Citro, R.; et al. Infective endocarditis and diabetes mellitus: Results from a single-center study from 1994 to 2017. PLoS ONE 2019, 14, e0223710. [Google Scholar] [CrossRef] [Green Version]
- Abe, T.; Eyituoyo, H.O.; De Allie, G.; Olanipekun, T.; Effoe, V.S.; Olaosebikan, K.; Mather, P. Clinical outcomes in patients with native valve infective endocarditis and diabetes mellitus. World J. Cardiol. 2021, 13, 11–20. [Google Scholar] [CrossRef]
- Frydrych, L.M.; Bian, G.; O’Lone, D.E.; Ward, P.A.; Delano, M.J. Obesity and type 2 diabetes mellitus drive immune dysfunction, infection development, and sepsis mortality. J. Leukoc. Biol. 2018, 104, 525–534. [Google Scholar] [CrossRef]
- Costantini, E.; Carlin, M.; Porta, M.; Brizzi, M.F. Type 2 diabetes mellitus and sepsis: State of the art, certainties and missing evidence. Acta Diabetol. 2021, 58, 1139–1151. [Google Scholar] [CrossRef]
- Trevelin, S.C.; Carlos, D.; Beretta, M.; da Silva, J.S.; Cunha, F.Q. Diabetes mellitus and sepsis: A challenging association. Shock 2017, 47, 276–287. [Google Scholar] [CrossRef]
- Armiñanzas, C.; Fariñas-Alvarez, C.; Zarauza, J.; Muñoz, P.; González Ramallo, V.; Martínez-Sellés, M.; Miró, J.M.; Pericás, J.M.; Goenaga, M.A.; Ojeda, G. Role of age and comorbidities in mortality of patients with infective endocarditis. Eur. J. Intern. Med. 2019, 64, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Sellés, M.; Munoz, P.; Arnáiz, A.; Moreno, M.; Gálvez, J.; Rodriguez-Roda, J.; de Alarcón, A.; García, E.; Fariñas, M.; Miró, J.M.; et al. Valve surgery in active infective endocarditis: A simple score to predict in-hospital prognosis. Int. J. Cardiol. 2014, 175, 133–137. [Google Scholar] [CrossRef]
- Mateos, R.; Boix-Palop, L.; Muñoz, P.; Mestres, C.A.; Marín, M.; Pedraz, A.; de Alarcón, A.; Gutiérrez, E.; Hernández, M.; Goenaga, M.A. Infective endocarditis in patients with cardiac implantable electronic devices: A nationwide study. Europace 2020, 22, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B. ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, J.J.; Rhinehart, A.S.; Shaefer, C.F., Jr.; Neuman, A. Diagnosis and Management of Diabetes: Synopsis of the 2016 American Diabetes Association Standards of Medical Care in Diabetes. Ann. Intern. Med. 2016, 164, 542–552. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee; American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; et al. Retinopathy, neuropathy, and foot care: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. 1), S185–S194. [Google Scholar] [CrossRef]
- Lovic, D.; Piperidou, A.; Zografou, I.; Grassos, H.; Pittaras, A.; Manolis, A. The growing epidemic of diabetes mellitus. Curr. Vasc. Pharmacol. 2020, 18, 104–109. [Google Scholar] [CrossRef]
- Ministerio de Sanidad. Consumo y Bienestar Social. Encuestas Nacionales de Salud La Diabetes en España y en el Mundo, en datos y Gráficos (epdata.es). Available online: https://www.epdata.es/datos/diabetes-espana-datos-graficos/472 (accessed on 5 March 2022).
- Sy, R.W.; Kritharides, L. Health care exposure and age in infective endocarditis: Results of a contemporary population-based profile of 1536 patients in Australia. Eur. Heart J. 2010, 31, 1890–1897. [Google Scholar] [CrossRef] [Green Version]
- Olmos, C.; Vilacosta, I.; Pozo, E.; Fernández, C.; Sarriá, C.; López, J.; Ferrera, C.; Maroto, L.; González, I.; Vivas, D. Prognostic implications of diabetes in patients with left-sided endocarditis: Findings from a large cohort study. Medicine 2014, 93, 114–119. [Google Scholar] [CrossRef]
- Leone, S.; Ravasio, V.; Durante-Mangoni, E.; Crapis, M.; Carosi, G.; Scotton, P.G.; Barzaghi, N.; Falcone, M.; Chinello, P.; Pasticci, M.B. Epidemiology, characteristics, and outcome of infective endocarditis in Italy: The Italian Study on Endocarditis. Infection 2012, 40, 527–535. [Google Scholar] [CrossRef]
- Fedeli, U.; Schievano, E.; Buonfrate, D.; Pellizzer, G.; Spolaore, P. Increasing incidence and mortality of infective endocarditis: A population-based study through a record-linkage system. BMC Infect. Dis. 2011, 11, 48. [Google Scholar] [CrossRef] [Green Version]
- Duval, X.; Alla, F.; Doco-Lecompte, T.; Le Moing, V.; Delahaye, F.; Mainardi, J.L.; Plesiat, P.; Célard, M.; Hoen, B.; Leport, C. Association pour l’Etude et la Prévention de l’Endocardite Infectieuse (AEPEI). Diabetes mellitus and infective endocarditis: The insulin factor in patient morbidity and mortality. Eur. Heart J. 2007, 28, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.C.P.; Guimarães-Júnior, M.H.; Murta Pinto, P.H.O.; Coelho, R.M.P.; Souza Barros, T.L.; Faleiro Maia, N.P.A.; Madureira, D.A.; Padilha Reis, R.C.; Costa, P.H.N.; Bráulio, R. Outcomes of infective endocarditis in the current era: Early predictors of a poor prognosis. Int. J. Infect. Dis. 2018, 68, 102–107. [Google Scholar] [CrossRef] [Green Version]
- Joffre, J.; Dumas, G.; Aegerter, P.; Dubée, V.; Bigé, N.; Preda, G.; Baudel, J.L.; Maury, E.; Guidet, B.; Ait-Oufella, H. CUB-Réa Network. Epidemiology of infective endocarditis in French intensive care units over the 1997–2014 period-from CUB-Réa Network. Crit. Care 2019, 23, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, X.B.; Liu, Y.H.; Huang, J.L.; Chen, X.L.; Yu, D.Q.; Tan, N.; Chen, J.Y.; He, P.C. Prediabetes and diabetes are both risk factors for adverse outcomes in infective endocarditis. Diabet. Med. 2018, 35, 1499–1507. [Google Scholar] [CrossRef] [PubMed]
- Moreno, R.; Zamorano, J.; Almería, C.; Villate, A.; Rodrigo, J.L.; Herrera, D.; Alvarez, L.; Morán, J.; Aubele, A.; Mataix, L. Influence of diabetes mellitus on short- and long-term outcome in patients with active infective endocarditis. J. Heart Valve Dis. 2002, 11, 651–659. [Google Scholar] [PubMed]
- Østergaard, L.; Mogensen, U.M.; Bundgaard, J.S.; Dahl, A.; Wang, A.; Torp-Pedersen, C.; Gislason, G.; Køber, L.; Køber, N.; Dejgaard, T.F. Duration and complications of diabetes mellitus and the associated risk of infective endocarditis. Int. J. Cardiol. 2019, 278, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Tousoulis, D.; Kampoli, A.M.; Stefanadis, C. Diabetes mellitus and vascular endothelial dysfunction: Current perspectives. Curr. Vasc. Pharmacol. 2012, 10, 19–32. [Google Scholar] [CrossRef]
- Eringa, E.C.; Serne, E.H.; Meijer, R.I.; Schalkwijk, C.G.; Houben, A.J.; Stehouwer, C.D.; Smulders, Y.M.; van Hinsbergh, V.W. Endothelial dysfunction in (pre)diabetes: Characteristics, causative mechanisms and pathogenic role in type 2 diabetes. Rev. Endocr. Metab. Disord. 2013, 14, 39–48. [Google Scholar] [CrossRef]
- Delamaire, M.; Maugendre, D.; Moreno, M.; Le Gof, M.C.; Allannic, H.; Genetet, B. Impaired leucocyte functions in diabetic patients. Diabet. Med. 1997, 14, 29–34. [Google Scholar] [CrossRef]
- Chirillo, F.; Bacchion, F.; Pedrocco, A.; Scotton, P.; De Leo, A.; Rocco, F.; Valfrè, C.; Olivari, Z. Infective endocarditis in patients with diabetes mellitus. J. Heart Valve Dis. 2010, 19, 312–320. [Google Scholar]
- Alba-Loureiro, T.C.; Munhoz, C.D.; Martins, J.O.; Cerchiaro, G.A.; Scavone, C.; Curi, R.; Sannomiya, P. Neutrophils function and metabolism in individuals with diabetes mellitus. Braz. J. Med. Res. 2007, 40, 1037–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonidou, L.; Mouzaki, A.; Michalaki, M.; DeLastic, A.L.; Kyriazopoulou, V.; Bassaris, H.P.; Gogos, C.A. Cytokine production and hospital mortality in patients with sepsis-induced stress hyperglycemia. J. Infect. 2007, 55, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, R.; Haque, M. Oral health messiers: Diabetes mellitus relevance. Diabetes Metab. Syndr. Obes. 2021, 14, 3001–3015. [Google Scholar] [CrossRef] [PubMed]
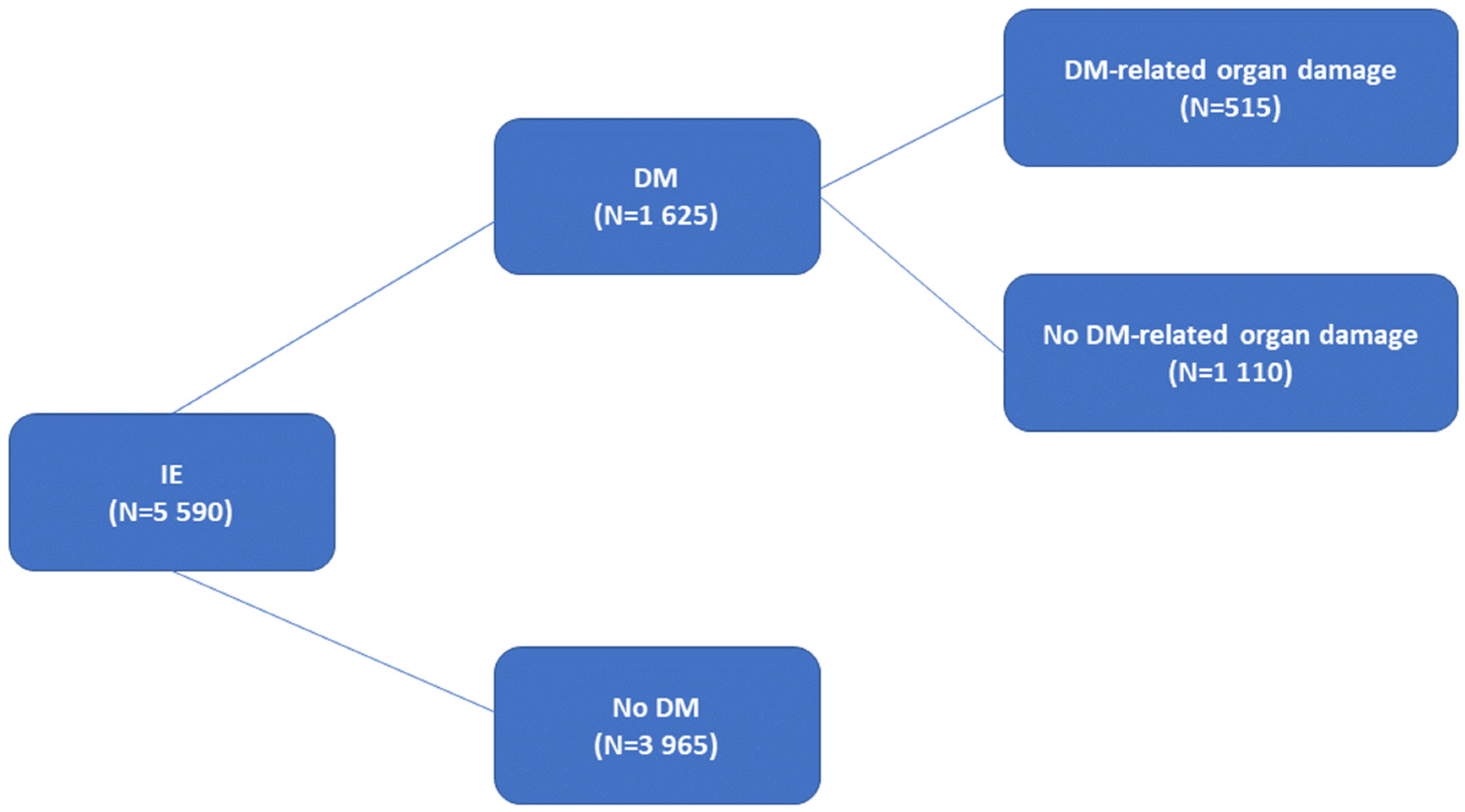

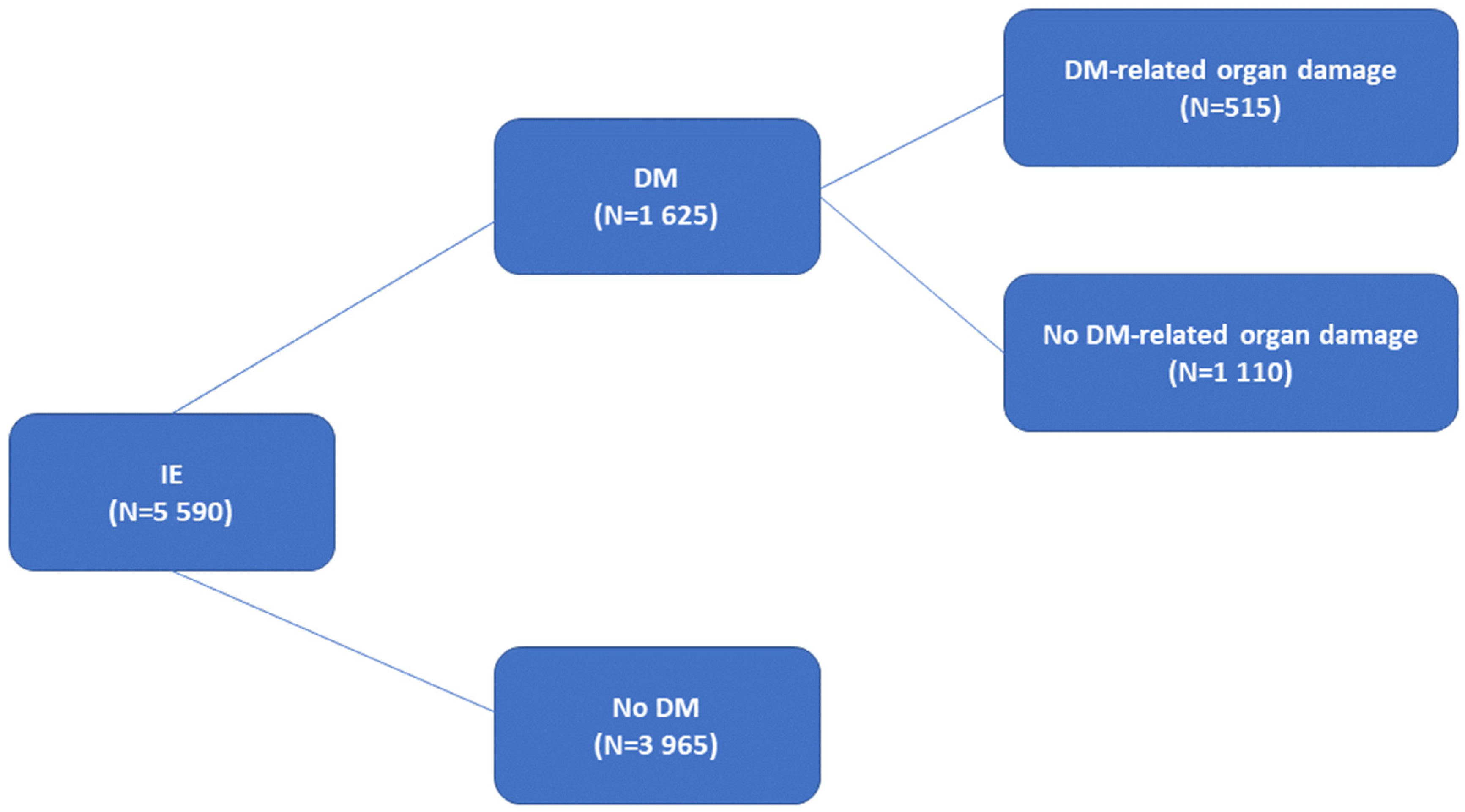{kind=link}
{kind=link}
{kind=link}
| No DM (3965) | DM (1625) | p | |
|---|---|---|---|
| Age, years, median (IQR) | 67 (54–77) | 72 (64–78) | <0.001 |
| Male Gender (%) | 2679 (67.5) | 1085 (66.7) | 0.564 |
| Nosocomial IE (%) | 1041 (26.3) | 535 (32.9) | <0.001 |
| Health care-associated IE (%) | 306 (7.7) | 158 (9.7) | 0.014 |
| Vegetation present (%) | 2893 (73.0) | 1150 (70.8) | 0.096 |
| New heart murmur (%) | 1349 (34.0) | 477 (29.3) | 0.001 |
| Location (%) | |||
| Aortic | 2060 (52.0) | 830 (51.1) | 0.551 |
| Mitral | 1688 (42.6) | 670 (41.2) | 0.356 |
| Tricuspid | 215 (5.4) | 79 (4.9) | 0.394 |
| Pulmonary | 71 (1.8) | 8 (0.5) | <0.001 |
| PM/ICD | 349 (8.8) | 213 (13.1) | <0.001 |
| Others | 113 (2.8) | 37 (2.3) | 0.229 |
| Multiple | 570 (14.4) | 227 (14.0) | 0.693 |
| Unknown | 66 (1.7) | 24 (1.5) | 0.613 |
| Native IE | 2459 (62.0) | 941 (57.9) | 0.004 |
| Prosthetic IE | 1213 (30.6) | 528 (32.5) | 0.164 |
| Comorbidities (%) | |||
| Respiratory disease | 668 (16.8) | 379 (23.3) | <0.001 |
| Coronary artery disease | 877 (22.1) | 625 (38.4) | <0.001 |
| Heart failure | 1179 (29.7) | 691 (42.5) | <0.001 |
| Peripheral arterial disease | 286 (7.2) | 315 (19.3) | <0.001 |
| Stroke | 441 (11.1) | 277 (17.0) | <0.001 |
| Cancer | 642 (16.1) | 254 (15.6) | 0.604 |
| Renal disease | 844 (21.3) | 586 (36.1) | <0.001 |
| Liver disease | 370 (9.4) | 163 (10.1) | 0.443 |
| Congenital heart disease | 303 (7.6) | 38 (2.3) | <0.001 |
| Native heart valve disease | 1794 (45.2) | 773 (47.5) | 0.113 |
| Age-adjusted Charlson score, median (IQR) | 4 (2–6) | 6 (5–8) | <0.001 |
| Etiology (%) | No DM (3965) | DM (1625) | p |
|---|---|---|---|
| Staphylococcus aureus | 836 (21.1) | 413 (25.4) | <0.001 |
| Coagulase-negative staphylococcus | 680 (17.2) | 322 (19.8) | 0.018 |
| Enterococcus | 519 (13.1) | 268 (16.5) | 0.001 |
| Streptococcus | 1081 (27.3) | 346 (21.3) | <0.001 |
| Candida | 68 (1.7) | 20 (1.2) | 0.187 |
| Other Fungi | 11 (0.3) | 4 (0.2) | 0.837 |
| Unknown | 345 (8.7) | 112 (6.9) | 0.025 |
| Anaerobe | 52 (1.3) | 16 (1.0) | 0.311 |
| Polymicrobial | 65 (1.6) | 21 (1.3) | 0.338 |
| Gram-negative bacteria | 167 (4.2) | 60 (3.7) | 0.372 |
| Other etiologies | 112 (2.8) | 34 (2.1) | 0.119 |
| No DM (3965) | DM (1625) | p | |
|---|---|---|---|
| Intracardiac complications (%) | 1264 (31.9) | 500 (30.8) | 0.715 |
| Valve perforation | 581 (14.6) | 203 (12.4) | 0.035 |
| Pseudoaneurysm | 248 (6.2) | 90 (5.5) | 0.308 |
| Abscess | 639 (16.1) | 283 (17.4) | 0.235 |
| Fistula | 105 (2.6) | 35 (2.1) | 0.283 |
| Vascular events (%) | 340 (8.5) | 98 (6.0) | 0.001 |
| Heart Failure (%) | 1554 (39.1) | 699 (43.0) | 0.008 |
| Persistent bacteremia (%) | 402 (10.1) | 204 (12.5) | 0.008 |
| Central nervous system involvement (%) | 750 (18.1) | 350 (21.5) | 0.025 |
| Embolism (%) | 888 (22.3) | 316 (19.4) | 0.015 |
| Renal Failure, new or worsening (%) | 1341 (33.8) | 654 (40.2) | <0.001 |
| Sepsis (%) | 632 (15.9) | 300 (18.4) | 0.022 |
| Septic shock (%) | 468 (11.8) | 226 (13.9) | 0.03 |
| Cardiac Surgery (%) | 1905 (48.0) | 707 (43.5) | 0.002 |
| In-hospital mortality (%) | 924 (23.3) | 521 (32.1) | <0.001 |
| One-year mortality (%) | 1131 (28.5) | 640 (39.4) | <0.001 |
| No Organ Damage (1110) | Organ Damage (515) | p | |
|---|---|---|---|
| Nosocomial IE (%) | 330 (29.7) | 205 (39.8) | <0.001 |
| Health care-associated IE (%) | 67 (6.0) | 91 (17.7) | <0.001 |
| Native IE (%) | 617 (55.6) | 324 (62.9) | 0.005 |
| Prosthetic IE (%) | 392 (35.3) | 136 (26.4) | <0.001 |
| Coronary artery disease (%) | 394 (35.4) | 231 (44.8) | <0.001 |
| Heart failure (%) | 428 (38.5) | 263 (51.0) | <0.001 |
| Peripheral arterial disease (%) | 116 (10.4) | 199 (38.4) | <0.001 |
| Stroke (%) | 168 (15.1) | 109 (21.1) | 0.003 |
| Cancer (%) | 197 (17.7) | 57 (11.0) | 0.001 |
| Renal disease (%) | 267 (24.1) | 319 (61.9) | <0.001 |
| Age-adjusted Charlson score, median (IQR) | 6 (4–7) | 8 (6–9) | <0.001 |
| Staphylococcus aureus (%) | 219 (19.7) | 194 (37.7) | <0.001 |
| Streptococcus (%) | 278 (25.0) | 68 (13.2) | <0.001 |
| Cardiac Surgery (%) | 523 (47.1) | 184 (35.7) | <0.001 |
| In-hospital mortality (%) | 321 (28.9) | 200 (38.8) | <0.001 |
| One-year mortality (%) | 393 (35.4) | 247 (48.0) | <0.001 |
| (A) | ||
| OR (95% CI) | p | |
| Diabetes | 1.4 (1.2–1.6) | <0.001 |
| Age (years) | 1.02 (1.02–1.03) | <0.001 |
| Female sex | 1.3 (1.1–1.5) | 0.001 |
| Heart failure | 2.6 (2.3–3.0) | <0.001 |
| Renal disease | 2.2 (1.9–2.5) | <0.001 |
| Sepsis | 2.1 (1.7–2.5) | 0.005 |
| S. aureus | 1.4 (1.2–1.7) | 0.002 |
| (B) | ||
| OR (95% CI) | p | |
| Diabetes | 1.4 (1.2–1.6) | <0.001 |
| Age (years) | 1.02 (1.02–1.03) | <0.001 |
| Female sex | 1.17 (1.02–1.34) | 0.027 |
| Heart failure | 2.4 (2.1–2.8) | <0.001 |
| Renal disease | 2.0 (1.8–2.3) | <0.001 |
| Sepsis | 2.0 (1.7–2.4) | <0.001 |
| Cardiac surgery not done | 1.3 (1.1–1.5) | 0.005 |
| S. aureus | 1.3 (1.1–1.5) | 0.002 |
| (C) | ||
| OR (95% CI) | p | |
| Diabetes-related organ damage | 1.4 (1.1–1.8) | 0.01 |
| Age (years) | 1.02 (1.01–1.03) | 0.007 |
| Female sex | 1.4 (1.1–1.8) | 0.01 |
| Heart failure | 3.2 (2.5–4.1) | <0.001 |
| Renal disease | 2.3 (1.8–2.9) | <0.001 |
| Sepsis | 1.8 (1.3–2.4) | <0.001 |
| S. aureus | 1.4 (1.1–1.9) | 0.01 |
| (D) | ||
| OR (95% CI) | p | |
| Diabetes-related organ damage | 1.6 (1.3–2.0) | <0.001 |
| Age (years) | 1.02 (1.01–1.03) | <0.001 |
| Female sex | 1.32 (1.04–1.67) | 0.024 |
| Heart failure | 2.7 (2.1–3.3) | <0.001 |
| Renal disease | 2.1 (1.7–2.6) | <0.001 |
| Sepsis | 1.7 (1.3–2.3) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biezma, M.I.; Muñoz, P.; De la Villa, S.; Fariñas-Álvarez, M.C.; Arnáiz de las Revillas, F.; Gutierrez-Carretero, E.; De Alarcón, A.; Rodríguez-García, R.; Llopis, J.; Goenaga, M.Á.; et al. Infective Endocarditis in Diabetic Patients: A Different Profile with Prognostic Consequences. J. Clin. Med. 2022, 11, 2651. https://doi.org/10.3390/jcm11092651
Biezma MI, Muñoz P, De la Villa S, Fariñas-Álvarez MC, Arnáiz de las Revillas F, Gutierrez-Carretero E, De Alarcón A, Rodríguez-García R, Llopis J, Goenaga MÁ, et al. Infective Endocarditis in Diabetic Patients: A Different Profile with Prognostic Consequences. Journal of Clinical Medicine. 2022; 11(9):2651. https://doi.org/10.3390/jcm11092651
Chicago/Turabian StyleBiezma, María Isabel, Patricia Muñoz, Sofía De la Villa, Mª Carmen Fariñas-Álvarez, Francisco Arnáiz de las Revillas, Encarnación Gutierrez-Carretero, Arístides De Alarcón, Raquel Rodríguez-García, Jaume Llopis, Miguel Ángel Goenaga, and et al. 2022. "Infective Endocarditis in Diabetic Patients: A Different Profile with Prognostic Consequences" Journal of Clinical Medicine 11, no. 9: 2651. https://doi.org/10.3390/jcm11092651
APA StyleBiezma, M. I., Muñoz, P., De la Villa, S., Fariñas-Álvarez, M. C., Arnáiz de las Revillas, F., Gutierrez-Carretero, E., De Alarcón, A., Rodríguez-García, R., Llopis, J., Goenaga, M. Á., Gutierrez-Villanueva, A., Plata, A., Vidal, L., Martínez-Sellés, M., & on behalf of GAMES. (2022). Infective Endocarditis in Diabetic Patients: A Different Profile with Prognostic Consequences. Journal of Clinical Medicine, 11(9), 2651. https://doi.org/10.3390/jcm11092651