
Prediction Model of Extubation Outcomes in Critically Ill Patients: A Multicenter Prospective Cohort Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
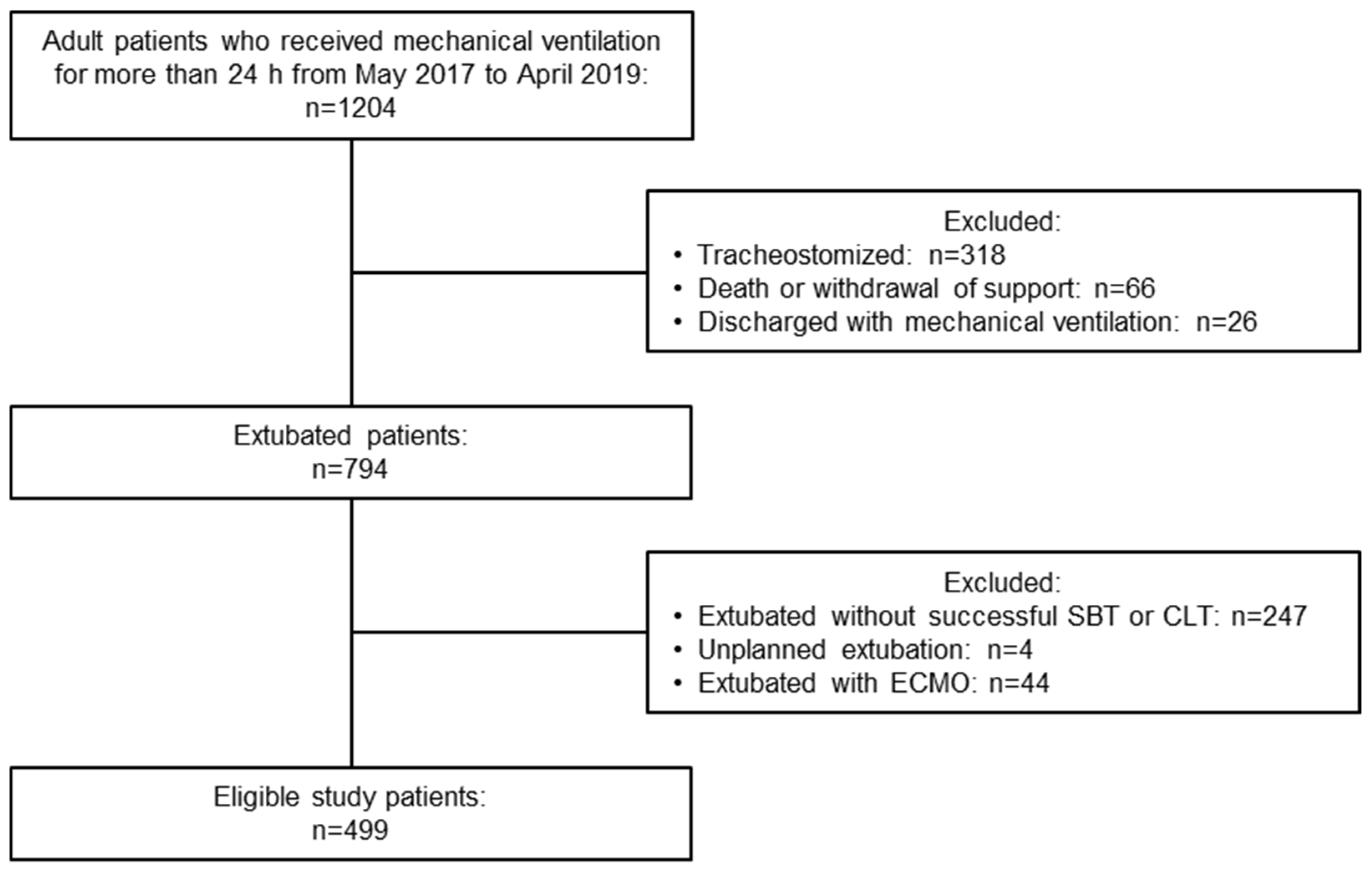
2.1. Study Population and Eligibility Criteria
2.2. Weaning and Extubation Procedures
2.3. Study Endpoints: The Outcomes That Were Predicted by the Prediction Model
2.4. Parameters for Developing the Prediction Model and Data Collection
2.5. Statistical Analysis
3. Results
3.1. Study Population and Clinical Characteristics
3.2. Prediction Model and Online Calculator
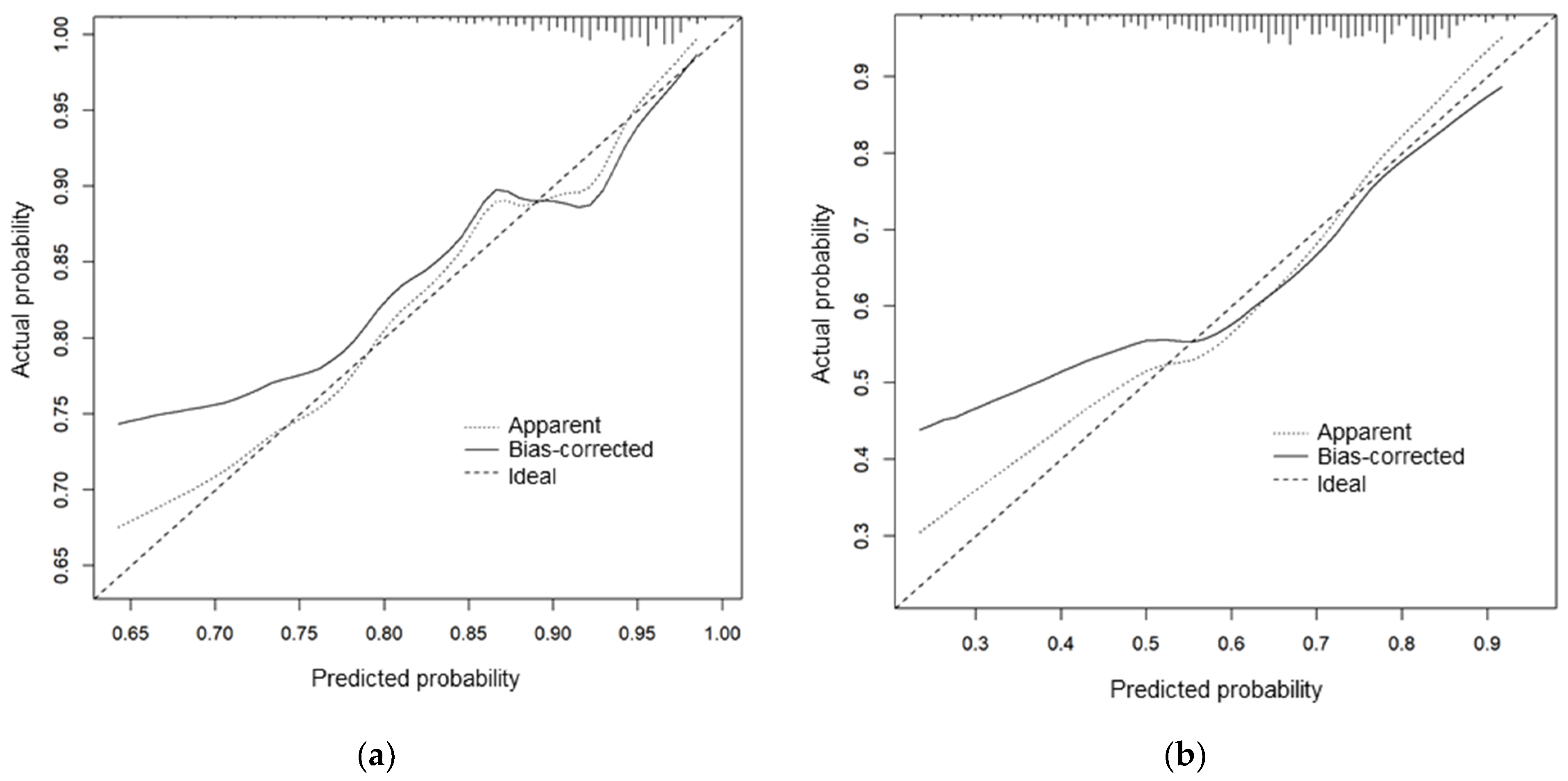
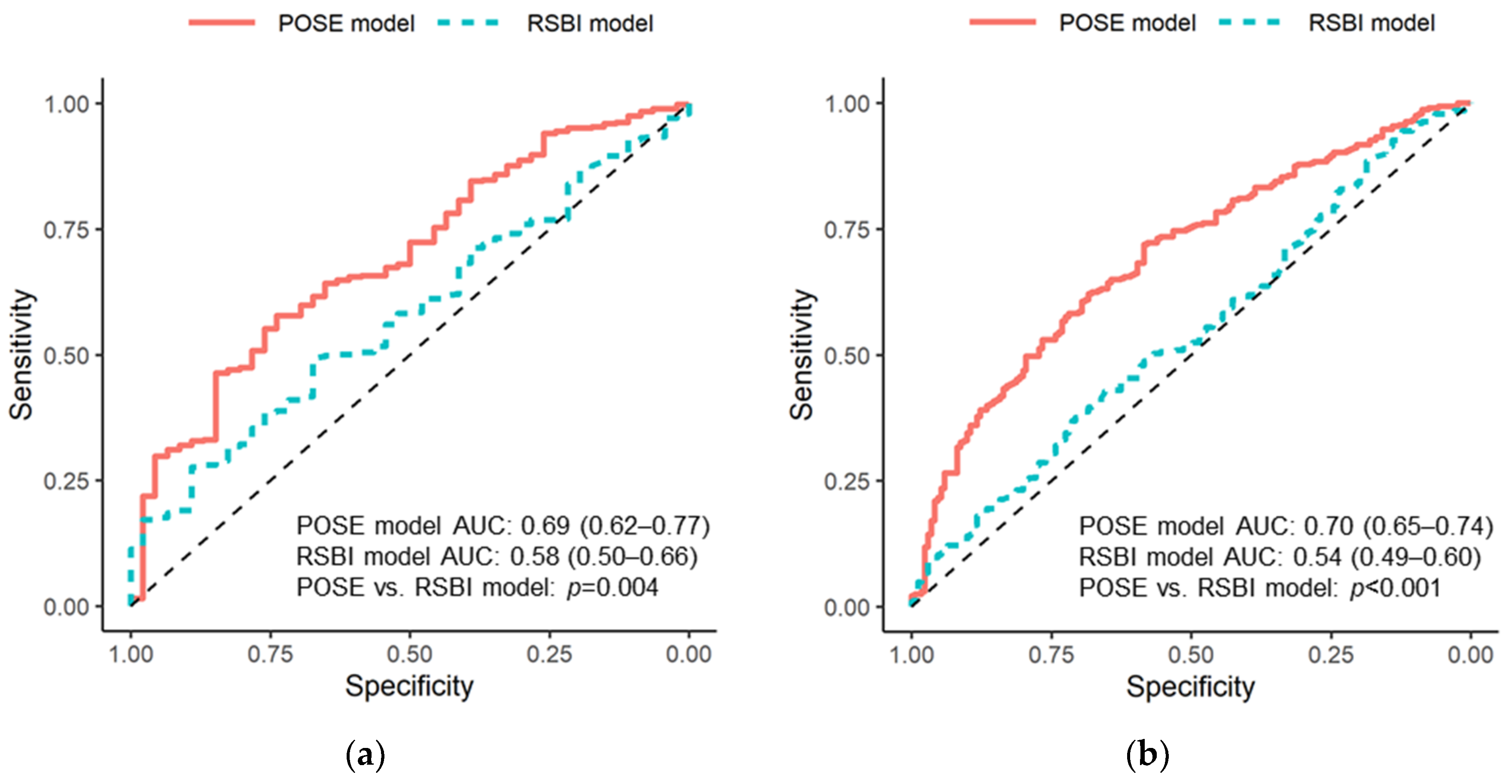
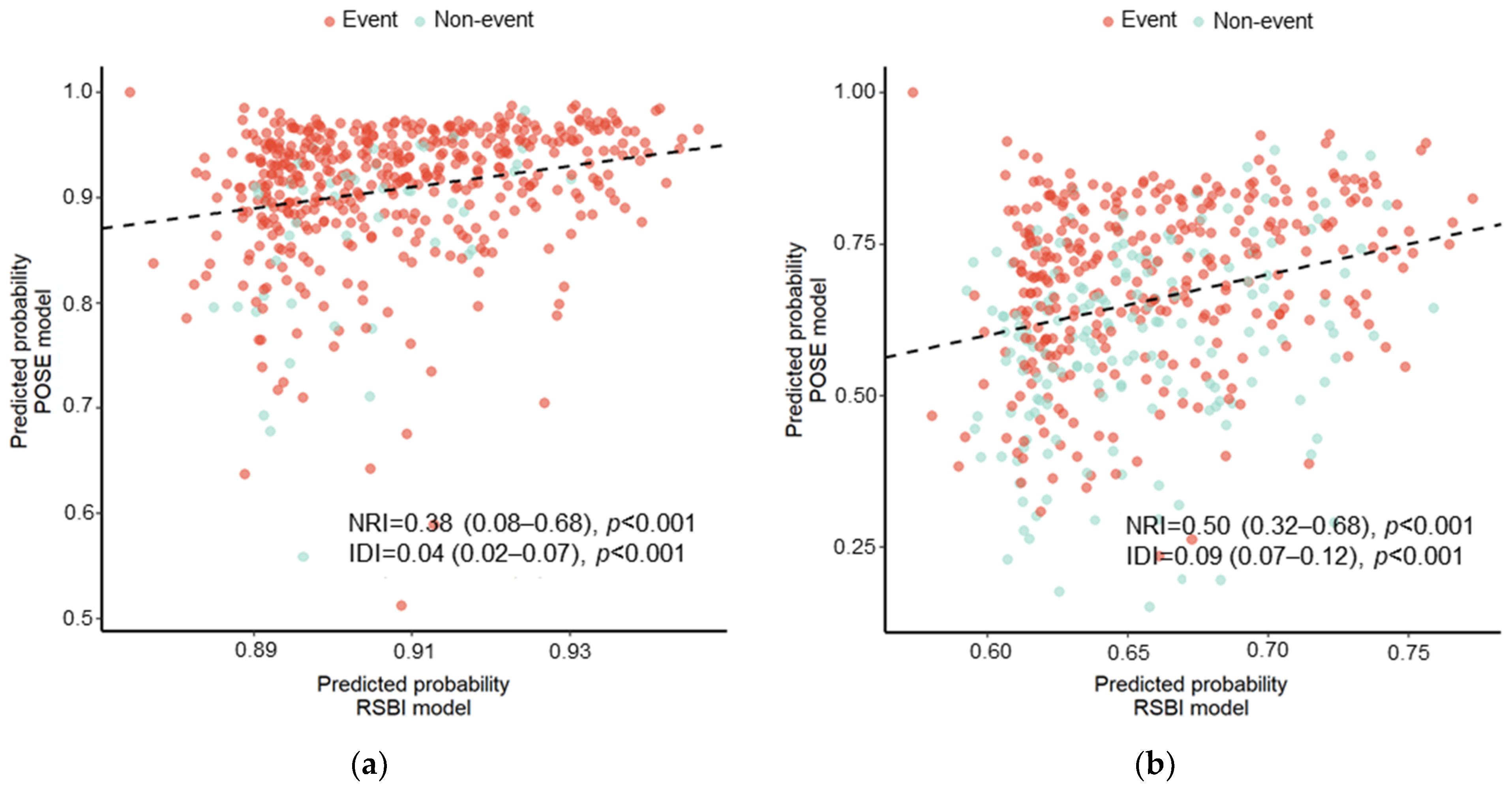
3.3. Predictive Performance of the POSE Model
4. Discussion
4.1. Key Findings
4.2. Prediction of Extubation Outcome
4.3. Implications of Study Findings
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morandi, A.; Piva, S.; Ely, E.W.; Myatra, S.N.; Salluh, J.I.F.; Amare, D.; Azoulay, E.; Bellelli, G.; Csomos, A.; Fan, E.; et al. Worldwide Survey of the “Assessing Pain, Both Spontaneous Awakening and Breathing Trials, Choice of Drugs, Delirium Monitoring/Management, Early Exercise/Mobility, and Family Empowerment” (Abcdef) Bundle. Crit. Care Med. 2017, 45, e1111–e1122. [Google Scholar] [CrossRef] [PubMed]
- Ouellette, D.R.; Patel, S.; Girard, T.D.; Morris, P.E.; Schmidt, G.A.; Truwit, J.D.; Alhazzani, W.; Burns, S.M.; Epstein, S.K.; Esteban, A.; et al. Liberation from Mechanical Ventilation in Critically Ill Adults: An Official American College of Chest Physicians/American Thoracic Society Clinical Practice Guideline: Inspiratory Pressure Augmentation during Spontaneous Breathing Trials, Protocols Minimizing Sedation, and Noninvasive Ventilation Immediately after Extubation. Chest 2017, 151, 166–180. [Google Scholar] [CrossRef] [Green Version]
- Quintard, H.; l’Her, E.; Pottecher, J.; Adnet, F.; Constantin, J.M.; De Jong, A.; Diemunsch, P.; Fesseau, R.; Freynet, A.; Girault, C.; et al. Experts’ Guidelines of Intubation and Extubation of the Icu Patient of French Society of Anaesthesia and Intensive Care Medicine (Sfar) and French-Speaking Intensive Care Society (Srlf): In Collaboration with the Pediatric Association of French-Speaking Anaesthetists and Intensivists (Adarpef), French-Speaking Group of Intensive Care and Paediatric Emergencies (Gfrup) and Intensive Care Physiotherapy Society (Skr). Ann. Intensive Care 2019, 9, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.C.; Chen, C.M.; Chiang, S.R.; Liu, W.L.; Weng, S.F.; Sung, M.I.; Hsing, S.C.; Cheng, K.C. Establishing Predictors for Successfully Planned Endotracheal Extubation. Medicine 2016, 95, e4852. [Google Scholar] [CrossRef] [PubMed]
- Esteban, A.; Alía, I.; Gordo, F.; Fernández, R.; Solsona, J.F.; Vallverdú, I.; Macías, S.; Allegue, J.M.; Blanco, J.; Carriedo, D.; et al. Extubation Outcome after Spontaneous Breathing Trials with T-Tube or Pressure Support Ventilation. The Spanish Lung Failure Collaborative Group. Am. J. Respir. Crit. Care Med. 1997, 156, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Frutos-Vivar, F.; Esteban, A.; Apezteguia, C.; González, M.; Arabi, Y.; Restrepo, M.I.; Gordo, F.; Santos, C.; Alhashemi, J.A.; Pérez, F.; et al. Outcome of Reintubated Patients after Scheduled Extubation. J. Crit. Care 2011, 26, 502–509. [Google Scholar] [CrossRef]
- Thille, A.W.; Harrois, A.; Schortgen, F.; Brun-Buisson, C.; Brochard, L. Outcomes of Extubation Failure in Medical Intensive Care Unit Patients. Crit. Care Med. 2011, 39, 2612–2618. [Google Scholar] [CrossRef]
- Epstein, S.K.; Ciubotaru, R.L.; Wong, J.B. Effect of Failed Extubation on the Outcome of Mechanical Ventilation. Chest 1997, 112, 186–192. [Google Scholar] [CrossRef]
- Frutos-Vivar, F.; Ferguson, N.D.; Esteban, A.; Epstein, S.K.; Arabi, Y.; Apezteguía, C.; González, M.; Hill, N.S.; Nava, S.; D’Empaire, G.; et al. Risk Factors for Extubation Failure in Patients Following a Successful Spontaneous Breathing Trial. Chest 2006, 130, 1664–1671. [Google Scholar] [CrossRef] [Green Version]
- Namen, A.M.; Ely, E.W.; Tatter, S.B.; Case, L.D.; Lucia, M.A.; Smith, A.; Landry, S.; Wilson, J.A.; Glazier, S.S.; Branch, C.L.; et al. Predictors of Successful Extubation in Neurosurgical Patients. Am. J. Respir. Crit. Care Med. 2001, 163, 658–664. [Google Scholar] [CrossRef]
- Mokhlesi, B.; Tulaimat, A.; Gluckman, T.J.; Wang, Y.; Evans, A.T.; Corbridge, T.C. Predicting Extubation Failure after Successful Completion of a Spontaneous Breathing Trial. Respir. Care 2007, 52, 1710–1717. [Google Scholar] [PubMed]
- Tanaka, A.; Yamashita, T.; Koyama, Y.; Uchiyama, A.; Fujino, Y. Predictors of Successful Extubation in Reintubated Patients: The Impact of Fluid Balance During the 24 Hours Prior to Extubation. Indian J. Crit. Care Med. 2019, 23, 344–345. [Google Scholar] [CrossRef] [PubMed]
- Khamiees, M.; Raju, P.; DeGirolamo, A.; Amoateng-Adjepong, Y.; Manthous, C.A. Predictors of Extubation Outcome in Patients Who Have Successfully Completed a Spontaneous Breathing Trial. Chest 2001, 120, 1262–1270. [Google Scholar] [CrossRef] [Green Version]
- Karthika, M.; Al Enezi, F.A.; Pillai, L.V.; Arabi, Y.M. Rapid Shallow Breathing Index. Ann. Thorac. Med. 2016, 11, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, A.P.; Agarwal, V. Extubation Failure in Intensive Care Unit: Predictors and Management. Indian J. Crit. Care Med. 2008, 12, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, H.J.; Chiu, H.W.; Lee, C.N.; Chen, T.T.; Chang, C.C.; Bien, M.Y. Improvement in the Prediction of Ventilator Weaning Outcomes by an Artificial Neural Network in a Medical Icu. Respir. Care 2015, 60, 1560–1569. [Google Scholar] [CrossRef] [Green Version]
- Baptistella, A.R.; Mantelli, L.M.; Matte, L.; Carvalho, M.E.D.R.U.; Fortunatti, J.A.; Costa, I.Z.; Haro, F.G.; Turkot, V.L.O.; Baptistella, S.F.; de Carvalho, D.; et al. Prediction of Extubation Outcome in Mechanically Ventilated Patients: Development and Validation of the Extubation Predictive Score (Expres). PLoS ONE 2021, 16, e0248868. [Google Scholar] [CrossRef]
- Frat, J.P.; Coudroy, R.; Thille, A.W. Non-invasive ventilation or high-flow oxygen therapy: When to choose one over the other? Respirology 2019, 24, 724–731. [Google Scholar] [CrossRef]
- Casey, J.D.; Vaughan, E.M.; Lloyd, B.D.; Billas, P.A.; Jackson, K.E.; Hall, E.J.; Toporek, A.H.; Buell, K.G.; Brown, R.M.; Richardson, R.K.; et al. Protocolized Post-Extubation Respiratory Support to Prevent Reintubation: A Randomized Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 294–302. [Google Scholar] [CrossRef]
- Glossop, A.J.; Shephard, N.; Bryden, D.C.; Mills, G.H. Non-Invasive Ventilation for Weaning, Avoiding Reintubation after Extubation and in the Postoperative Period: A Meta-Analysis. Br. J. Anaesth. 2012, 109, 305–314. [Google Scholar] [CrossRef] [Green Version]
- Xu, Z.; Li, Y.; Zhou, J.; Li, X.; Huang, Y.; Liu, X.; Burns, K.E.A.; Zhong, N.; Zhang, H. High-Flow Nasal Cannula in Adults with Acute Respiratory Failure and after Extubation: A Systematic Review and Meta-Analysis. Respir. Res. 2018, 19, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, A.; Uchiyama, A.; Horiguchi, Y.; Higeno, R.; Sakaguchi, R.; Koyama, Y.; Ebishima, H.; Yoshida, T.; Matsumoto, A.; Sakai, K.; et al. Predictors of Post-Extubation Stridor in Patients on Mechanical Ventilation: A Prospective Observational Study. Sci. Rep. 2021, 11, 19993. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.L.; Cole, R.P. Association between Reduced Cuff Leak Volume and Postextubation Stridor. Chest 1996, 110, 1035–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandhu, R.S.; Pasquale, M.D.; Miller, K.; Wasser, T.E. Measurement of Endotracheal Tube Cuff Leak to Predict Postextubation Stridor and Need for Reintubation. J. Am. Coll. Surg. 2000, 190, 682–687. [Google Scholar] [CrossRef]
- Thille, A.W.; Richard, J.C.; Brochard, L. The Decision to Extubate in the Intensive Care Unit. Am. J. Respir. Crit. Care Med. 2013, 187, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr. Regression Modeling Strategies with Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis, 2nd ed.; Springer: New York, NY, USA, 2015. [Google Scholar]
- Yang, K.L.; Tobin, M.J. A Prospective Study of Indexes Predicting the Outcome of Trials of Weaning from Mechanical Ventilation. N. Engl. J. Med. 1991, 324, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- El-Khatib, M.F.; Zeineldine, S.M.; Jamaleddine, G.W. Effect of Pressure Support Ventilation and Positive End Expiratory Pressure on the Rapid Shallow Breathing Index in Intensive Care Unit Patients. Intensive Care Med. 2008, 34, 505–510. [Google Scholar] [CrossRef]
- Segal, L.N.; Oei, E.; Oppenheimer, B.W.; Goldring, R.M.; Bustami, R.T.; Ruggiero, S.; Berger, K.I.; Fiel, S.B. Evolution of Pattern of Breathing during a Spontaneous Breathing Trial Predicts Successful Extubation. Intensive Care Med. 2010, 36, 487–495. [Google Scholar] [CrossRef]
- El Khoury, M.Y.; Panos, R.J.; Ying, J.; Almoosa, K.F. Value of the PaO2:FiO2 Ratio and Rapid Shallow Breathing Index in Predicting Successful Extubation in Hypoxemic Respiratory Failure. Heart Lung 2010, 39, 529–536. [Google Scholar] [CrossRef]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, M.Z.I.; Turin, T.C. Variable selection strategies and its importance in clinical prediction modelling. Fam. Med. Community Health 2020, 8, e000262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, S.N.; Osaku, E.F.; Costa, C.R.; Toccolini, B.F.; Costa, N.L.; Cândia, M.F.; Leite, M.A.; Jorge, A.C.; Duarte, P.A.D. Comparison of Proportional Assist Ventilation Plus, T-Tube Ventilation, and Pressure Support Ventilation as Spontaneous Breathing Trials for Extubation: A Randomized Study. Respir. Care 2015, 60, 1527–1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keyal, N.K.; Amatya, R.; Shrestha, G.S.; Acharya, S.P.; Shrestha, P.S.; Marhatta, M.N. Influence of Arterial Blood Gas to Guide Extubation in Intensive Care Unit Patients after Spontaneous Breathing Trial. J. Nepal Health Res. Counc. 2020, 18, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Demoule, A.; Chevret, S.; Carlucci, A.; Kouatchet, A.; Jaber, S.; Meziani, F.; Schmidt, M.; Schnell, D.; Clergue, C.; Aboab, J.; et al. Changing Use of Noninvasive Ventilation in Critically Ill Patients: Trends Over 15 Years in Francophone Countries. Intensive Care Med. 2016, 42, 82–92. [Google Scholar] [CrossRef]
- Dhillon, N.K.; Smith, E.J.T.; Ko, A.; Harada, M.Y.; Polevoi, D.; Liang, R.; Barmparas, G.; Ley, E.J. Extubation to High-Flow Nasal Cannula in Critically Ill Surgical Patients. J. Surg. Res. 2017, 217, 258–264. [Google Scholar] [CrossRef]
- Hsiung Lee, E.S.; Jiann Lim, D.T.; Taculod, J.M.; Sahagun, J.T.; Otero, J.P.; Teo, K.; Loh, W.N.; Hui Tan, A.Y. Factors Associated with Reintubation in an Intensive Care Unit: A Prospective Observational Study. Indian J. Crit. Care Med. 2017, 21, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Jaber, S.; Quintard, H.; Cinotti, R.; Asehnoune, K.; Arnal, J.M.; Guitton, C.; Paugam-Burtz, C.; Abback, P.; Mekontso Dessap, A.; Lakhal, K.; et al. Risk Factors and Outcomes for Airway Failure versus Non-Airway Failure in the Intensive Care Unit: A Multicenter Observational Study of 1514 Extubation Procedures. Crit. Care 2018, 22, 236. [Google Scholar] [CrossRef] [Green Version]
- Meredith, W.; Rutledge, R.; Fakhry, S.M.; Emery, S.; Kromhout-Schiro, S. The conundrum of the Glasgow Coma Scale in intubated patients: A linear regression prediction of the Glasgow verbal score from the Glasgow eye and motor scores. J. Trauma 1998, 44, 839–844. [Google Scholar] [CrossRef] [Green Version]
- Brennan, P.M.; Murray, G.D.; Teasdale, G.M. A practical method for dealing with missing Glasgow Coma Scale verbal component scores. J. Neurosurg. 2020, 135, 214–219. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort (n = 499) | Uneventful Extubation (n = 328) a | Noninvasive Respiratory Support (n = 125) b | Reintubation (n = 46) | p Value | Missing (%) |
|---|---|---|---|---|---|---|
| Age, years | 69 (55–77) | 69 (55–77) | 69 (54–78) | 70 (63–76) | 0.913 | 0 |
| Male sex, n (%) | 311 (62.3%) | 201 (61.3%) | 79 (63.2%) | 31 (67.4%) | 0.706 | 0 |
| Body mass index, kg/m2 | 22.5 (19.8–25.4) | 22.2 (19.8–25.2) | 23.7 (20.1–26.7) | 21.0 (19.0–24.0) | 0.025 | 0 |
| APACHE II score | 19 (14–24) | 19 (14–23) | 19 (14–25) | 18 (14–22) | 0.386 | 0 |
| Comorbidity, n (%) | ||||||
| Heart failure | 151 (30.3%) | 94 (28.7%) | 45 (36.0%) | 12 (26.1%) | 0.194 | 0 |
| COPD | 33 (6.6%) | 18 (5.5%) | 11 (8.8%) | 4 (8.7%) | 0.375 | 0 |
| Asthma | 23 (4.6%) | 15 (4.6%) | 6 (4.8%) | 2 (4.3%) | 0.991 | 0 |
| Other respiratory diseases | 66 (13.2%) | 37 (11.3%) | 18 (14.4%) | 11 (23.9%) | 0.300 | 0 |
| Diabetes mellitus | 130 (26.1%) | 82 (25.0%) | 33 (26.4%) | 15 (32.6%) | 0.543 | 0 |
| Chronic kidney disease | 101 (20.2%) | 66 (20.1%) | 23 (18.4%) | 12 (26.1%) | 0.538 | 0 |
| Surgical ICU admission, n (%) | 355 (71.1%) | 224 (68.3%) | 93 (74.4%) | 38 (82.6%) | 0.087 | 0 |
| Reason for mechanical ventilation, n (%) | ||||||
| Asthma | 2 (0.4%) | 2 (0.6%) | 0 (0.0%) | 0 (0.0%) | 0.096 | 0 |
| COPD | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| Pneumonia | 50 (10.0%) | 33 (10.0%) | 9 (7.2%) | 8 (17.4%) | ||
| ARDS | 4 (0.8%) | 3 (0.9%) | 1 (0.8%) | 0 (0.0%) | ||
| Postoperative acute respiratory failure | 329 (65.9%) | 207 (63.1%) | 88 (70.4%) | 34 (73.9%) | ||
| Upper airway obstruction | 4 (0.8%) | 3 (0.9%) | 1 (0.8%) | 0 (0.0%) | ||
| Other causes of respiratory failure | 17 (3.4%) | 10 (3.0%) | 6 (4.8%) | 1 (2.2%) | ||
| Sepsis | 23 (4.6%) | 17 (5.2%) | 4 (3.2%) | 2 (4.3%) | ||
| Heart failure | 29 (5.8%) | 21 (6.4%) | 8 (6.4%) | 0 (0.0%) | ||
| Coma | 12 (2.4%) | 8 (2.4%) | 3 (2.4%) | 1 (2.2%) | ||
| Neurological disease | 10 (2.0%) | 9 (2.7%) | 1 (0.8%) | 0 (0.0%) | ||
| Trauma | 1 (0.2%) | 0 (0.0%) | 1 (0.8%) | 0 (0.0%) | ||
| Cardiac arrest | 18 (3.6%) | 15 (4.6%) | 3 (2.4%) | 0 (0.0%) | ||
| Variables | Total Cohort | Uneventful Extubation a | Noninvasive Respiratory Support b | Reintubation | p Value | Missing (%) |
|---|---|---|---|---|---|---|
| Duration of mechanical ventilation, h | 83.5 (45.8–139.2) | 68.9 (44.1–119.9) | 92.4 (49.3–184.8) | 99.7 (66.2–164.6) | <0.001 | 0 |
| Cardiopulmonary disorders prior to extubation, n (%) | ||||||
| Underlying or new occurrence of heart failure c | 159 (31.9%) | 100 (30.5%) | 47 (37.6%) | 12 (26.1%) | 0.236 | 0 |
| Underlying respiratory disease or occurrence of pneumonia c | 183 (36.7%) | 111 (33.8%) | 48 (38.4%) | 24 (52.2%) | 0.049 | 0 |
| ABG levels and respiratory data during successful SBT | ||||||
| pH | 7.43 (7.40–7.46) | 7.43 (7.40–7.46) | 7.44 (7.41–7.48) | 7.45 (7.41–7.46) | 0.165 | 0 |
| PaCO2, mmHg | 40.5 (36.8–44.2) | 40.5 (36.9–43.8) | 40.0 (36.1–44.0) | 43.3 (38.4–46.1) | 0.050 | 0 |
| PaO2/FIO2, mmHg | 300 (242–367) | 311 (259–381) | 260 (220–340) | 314 (227–354) | <0.001 | 0 |
| SpO2, % | 98 (97–100) | 99 (98–100) | 98 (97–99) | 98 (96–99) | 0.007 | 0 |
| RSBI, breaths/min/L | 41.8 (31.3–55.7) | 40.3 (30.7–55.0) | 41.8 (31.1–56.9) | 45.1 (36.5–56.3) | 0.141 | 0 |
| Parameters at extubation | ||||||
| SOFA score | 8 (6–10) | 8 (6–10) | 9 (7–11) | 8 (5–10) | 0.002 | 0 |
| Fluid balance during the previous 24 h, mL | −296 (−1053–400) | −313 (−1032–498) | −247 (−1059–343) | −412 (−1198–276) | 0.659 | 0 |
| GCS score, point | 11 (10–11) | 11 (10–11) | 11 (10–11) | 10 (10–11) | 0.314 | 0 |
| Number of endotracheal suctioning episodes during the previous 24 h | 12 (9–16) | 12 (9–14) | 13 (9–16) | 15 (11–18) | 0.659 | 0 |
| Patient outcomes | ||||||
| ICU length of stay, d | 8 (5–14) | 7 (4–11) | 10 (6–17) | 17 (13–27) | <0.001 | 0 |
| Hospital length of stay, d | 46 (28–83) | 40 (27–77) | 48 (29–87) | 75 (49–127) | <0.001 | 0 |
| 28-day mortality, n (%) | 9 (1.8%) | 5 (1.5%) | 3 (2.4%) | 1 (2.2%) | 0.806 | 0 |
| ICU mortality, n (%) | 13 (2.6%) | 5 (1.5%) | 7 (5.6%) | 1 (2.2%) | 0.051 | 0 |
| Hospital mortality, n (%) | 43 (8.6%) | 23 (7.0%) | 14 (11.2%) | 6 (13.0%) | 0.194 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, A.; Kabata, D.; Hirao, O.; Kosaka, J.; Furushima, N.; Maki, Y.; Uchiyama, A.; Egi, M.; Shintani, A.; Morimatsu, H.; et al. Prediction Model of Extubation Outcomes in Critically Ill Patients: A Multicenter Prospective Cohort Study. J. Clin. Med. 2022, 11, 2520. https://doi.org/10.3390/jcm11092520
Tanaka A, Kabata D, Hirao O, Kosaka J, Furushima N, Maki Y, Uchiyama A, Egi M, Shintani A, Morimatsu H, et al. Prediction Model of Extubation Outcomes in Critically Ill Patients: A Multicenter Prospective Cohort Study. Journal of Clinical Medicine. 2022; 11(9):2520. https://doi.org/10.3390/jcm11092520
Chicago/Turabian StyleTanaka, Aiko, Daijiro Kabata, Osamu Hirao, Junko Kosaka, Nana Furushima, Yuichi Maki, Akinori Uchiyama, Moritoki Egi, Ayumi Shintani, Hiroshi Morimatsu, and et al. 2022. "Prediction Model of Extubation Outcomes in Critically Ill Patients: A Multicenter Prospective Cohort Study" Journal of Clinical Medicine 11, no. 9: 2520. https://doi.org/10.3390/jcm11092520
APA StyleTanaka, A., Kabata, D., Hirao, O., Kosaka, J., Furushima, N., Maki, Y., Uchiyama, A., Egi, M., Shintani, A., Morimatsu, H., Mizobuchi, S., Kotake, Y., & Fujino, Y. (2022). Prediction Model of Extubation Outcomes in Critically Ill Patients: A Multicenter Prospective Cohort Study. Journal of Clinical Medicine, 11(9), 2520. https://doi.org/10.3390/jcm11092520