
Systemic Complement Activation Profiles in Nonexudative Age-Related Macular Degeneration: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
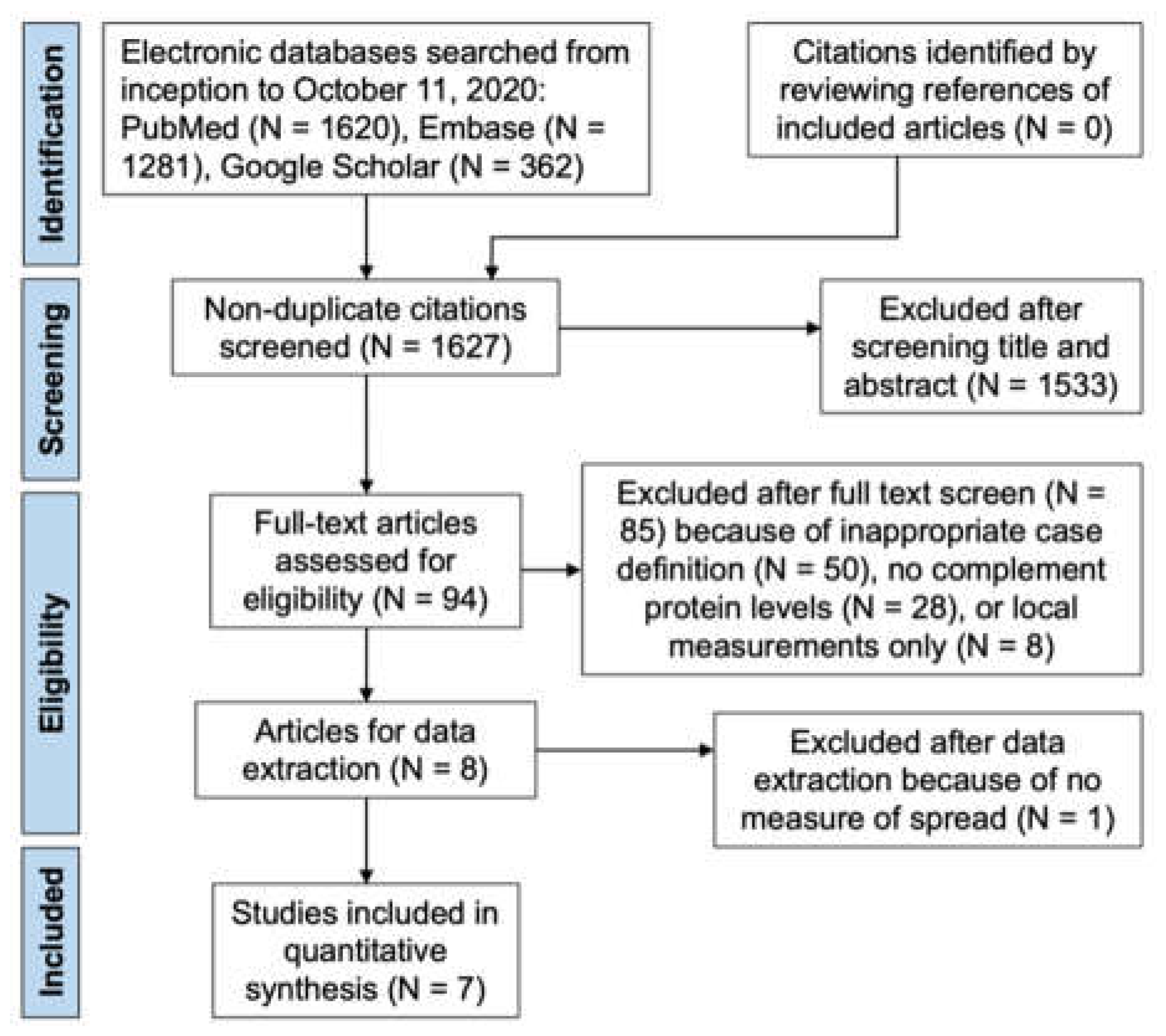
2.2. Search Strategy and Study Selection
2.3. Summary Measures and Synthesis of the Results
2.4. Assessment of Heterogeneity, Outliers, and Publication Bias
2.5. Data and Code Sharing
3. Results
3.1. Study Characteristics
3.2. Quality Assessment
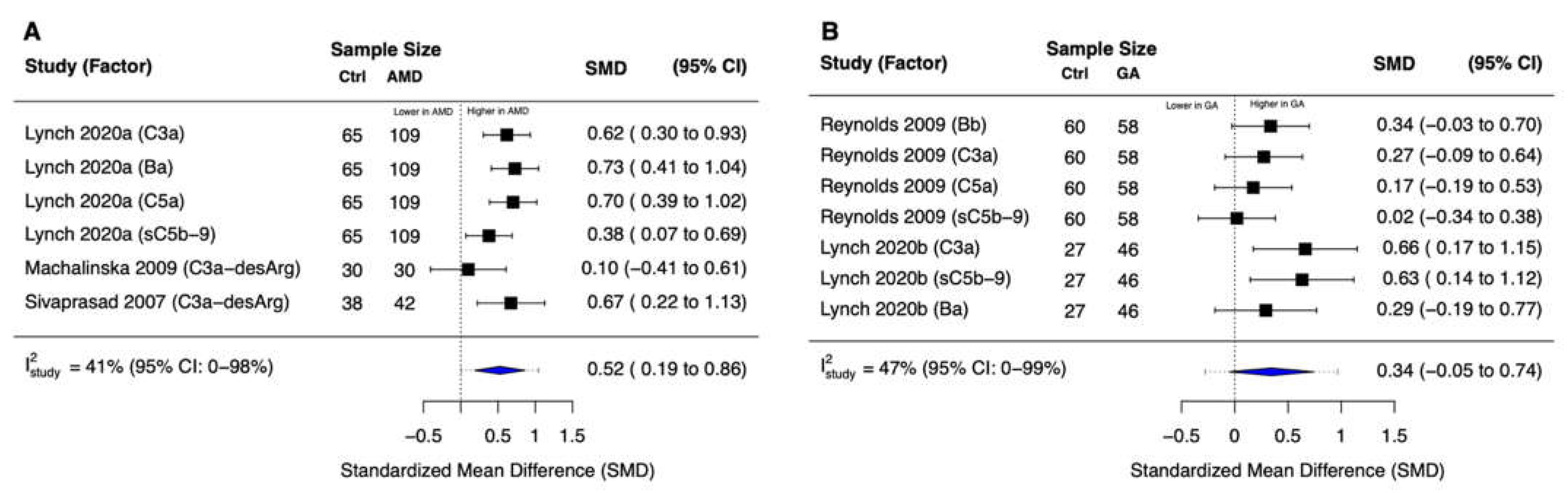
3.3. Complement Common Pathway Activation
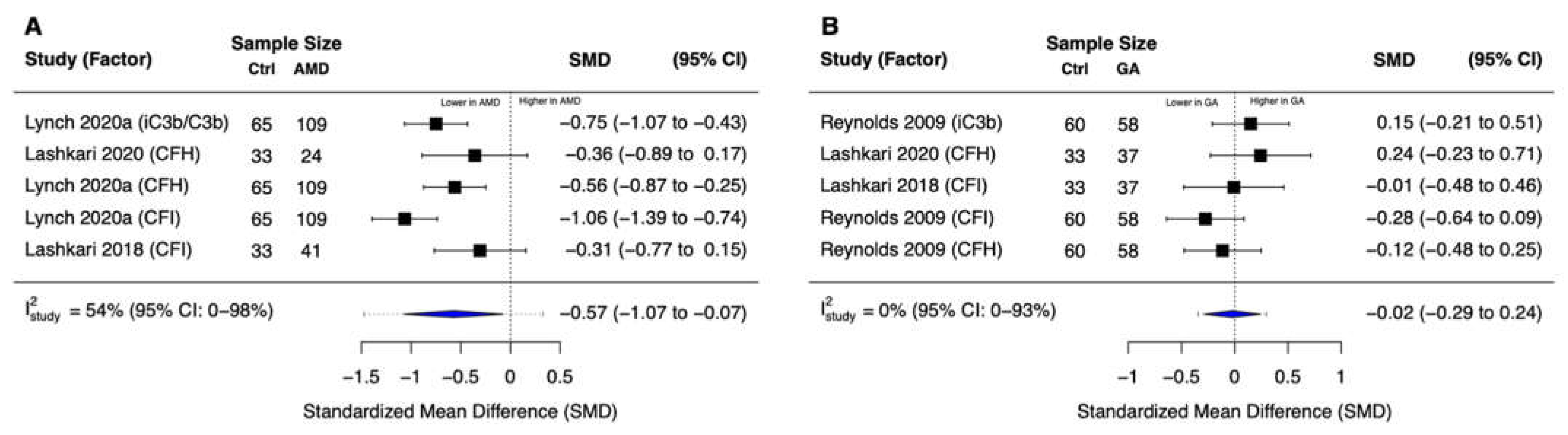
3.4. Complement Inhibition
3.5. Risk of Influential Outliers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.-Y.; Wong, T.Y. Global Prevalence of Age-Related Macular Degeneration and Disease Burden Projection for 2020 and 2040: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Chew, E.Y.; Clemons, T.E.; SanGiovanni, J.P.; Danis, R.P.; Ferris, F.L.; Elman, M.J.; Antoszyk, A.N.; Ruby, A.J.; Orth, D.; Bressler, S.B.; et al. Secondary Analyses of the Effects of Lutein/Zeaxanthin on Age-Related Macular Degeneration Progression: AREDS2 Report No. 3. JAMA Ophthalmol. 2014, 132, 142. [Google Scholar] [CrossRef] [PubMed]
- Lutein + Zeaxanthin and Omega-3 Fatty Acids for Age-Related Macular Degeneration: The Age-Related Eye Disease Study 2 (AREDS2) Randomized Clinical Trial. JAMA 2013, 309, 2005. [CrossRef] [PubMed]
- Vavvas, D.G.; Small, K.W.; Awh, C.C.; Zanke, B.W.; Tibshirani, R.J.; Kustra, R. CFH and ARMS2 Genetic Risk Determines Progression to Neovascular Age-Related Macular Degeneration after Antioxidant and Zinc Supplementation. Proc. Natl. Acad. Sci. USA 2018, 115, E696–E704. [Google Scholar] [CrossRef] [Green Version]
- Age-Related Eye Disease Study Research Group A Randomized, Placebo-Controlled, Clinical Trial of High-Dose Supplementation with Vitamins C and E, Beta Carotene, and Zinc for Age-Related Macular Degeneration and Vision Loss: AREDS Report No. 8. Arch. Ophthalmol. 2001, 119, 1417–1436. [CrossRef] [Green Version]
- Chew, E.Y.; Clemons, T.E.; Agrón, E.; Sperduto, R.D.; Sangiovanni, J.P.; Kurinij, N.; Davis, M.D. Age-Related Eye Disease Study Research Group Long-Term Effects of Vitamins C and E, β-Carotene, and Zinc on Age-Related Macular Degeneration: AREDS Report No. 35. Ophthalmology 2013, 120, 1604–1611. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.B.; Halawa, O.A.; Miller, J.W.; Vavvas, D.G. Complement Inhibition for Geographic Atrophy: A Tempting Target with Mixed Results. J. Clin. Med. 2021, 10, 2890. [Google Scholar] [CrossRef]
- Halawa, O.A.; Lin, J.B.; Miller, J.W.; Vavvas, D.G. A Review of Completed and Ongoing Complement Inhibitor Trials for Geographic Atrophy Secondary to Age-Related Macular Degeneration. J. Clin. Med. 2021, 10, 2580. [Google Scholar] [CrossRef]
- Lin, J.B.; Serghiou, S.; Miller, J.W.; Vavvas, D.G. Systemic Complement Activation Profiles in Nonexudative Age-Related Macular Degeneration: A Systematic Review. Ophthalmol. Sci. 2022, 2, 100118. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.; Bossuyt, P.; Boutron, I.; Hoffmann, T.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.; Akl, E.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-Analysis of Observational Studies in Epidemiology: A Proposal for Reporting. Meta-Analysis Of Observational Studies in Epidemiology (MOOSE) Group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Lin, L. Bias Caused by Sampling Error in Meta-Analysis with Small Sample Sizes. PLoS ONE 2018, 13, e0204056. [Google Scholar] [CrossRef] [Green Version]
- Lynch, A.M.; Palestine, A.G.; Wagner, B.D.; Patnaik, J.L.; Frazier-Abel, A.A.; Mathias, M.T.; Siringo, F.S.; Holers, V.M.; Mandava, N. Complement Factors and Reticular Pseudodrusen in Intermediate Age-Related Macular Degeneration Staged by Multimodal Imaging. BMJ Open Ophthalmol. 2020, 5, e000361. [Google Scholar] [CrossRef] [Green Version]
- Lynch, A.M.; Mandava, N.; Patnaik, J.L.; Frazer-Abel, A.A.; Wagner, B.D.; Palestine, A.G.; Mathias, M.T.; Siringo, F.S.; Cathcart, J.N.; Holers, V.M. Systemic Activation of the Complement System in Patients with Advanced Age-Related Macular Degeneration. Eur. J. Ophthalmol. 2020, 30, 1061–1068. [Google Scholar] [CrossRef]
- Machalińska, A.; Dziedziejko, V.; Mozolewska-Piotrowska, K.; Karczewicz, D.; Wiszniewska, B.; Machaliński, B. Elevated Plasma Levels of C3a Complement Compound in the Exudative Form of Age-Related Macular Degeneration. Ophthalmic Res. 2009, 42, 54–59. [Google Scholar] [CrossRef]
- Reynolds, R.; Hartnett, M.E.; Atkinson, J.P.; Giclas, P.C.; Rosner, B.; Seddon, J.M. Plasma Complement Components and Activation Fragments: Associations with Age-Related Macular Degeneration Genotypes and Phenotypes. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5818. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally Estimating the Sample Mean from the Sample Size, Median, Mid-Range, and/or Mid-Quartile Range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the Sample Mean and Standard Deviation from the Sample Size, Median, Range and/or Interquartile Range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Sivaprasad, S.; Adewoyin, T.; Bailey, T.A.; Dandekar, S.S.; Jenkins, S.; Webster, A.R.; Chong, N.V. Estimation of Systemic Complement C3 Activity in Age-Related Macular Degeneration. Arch. Ophthalmol. 2007, 125, 515–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lashkari, K.; Teague, G.C.; Beattie, U.; Betts, J.; Kumar, S.; McLaughlin, M.M.; López, F.J. Plasma Biomarkers of the Amyloid Pathway Are Associated with Geographic Atrophy Secondary to Age-Related Macular Degeneration. PLoS ONE 2020, 15, e0236283. [Google Scholar] [CrossRef] [PubMed]
- Lashkari, K.; Teague, G.; Chen, H.; Lin, Y.-Q.; Kumar, S.; McLaughlin, M.M.; López, F.J. A Monoclonal Antibody Targeting Amyloid β (Aβ) Restores Complement Factor I Bioactivity: Potential Implications in Age-Related Macular Degeneration and Alzheimer’s Disease. PLoS ONE 2018, 13, e0195751. [Google Scholar] [CrossRef] [PubMed]
- Sitnilska, V.; Enders, P.; Cursiefen, C.; Fauser, S.; Altay, L. Association of Imaging Biomarkers and Local Activation of Complement in Aqueous Humor of Patients with Early Forms of Age-Related Macular Degeneration. Graefe Arch. Clin. Exp. Ophthalmol. 2020, 259, 623–632. [Google Scholar] [CrossRef]
- Altay, L.; Sitnilska, V.; Schick, T.; Widmer, G.; Duchateau-Nguyen, G.; Piraino, P.; Jayagopal, A.; Drawnel, F.M.; Fauser, S. Early Local Activation of Complement in Aqueous Humour of Patients with Age-Related Macular Degeneration. Eye 2019, 33, 1859–1864. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Study (Country) | Year | Study Design | Number of Participants | Controls | AMD Classification Methodology | ||
|---|---|---|---|---|---|---|---|
| neAMD a | GA | Non-AMD | |||||
| Sivaprasad et al. (England) | 2007 | Cross-sectional | 42 | 0 | 38 | Likely clinic-based; healthy without AMD | International ARM Epidemiological Study Group |
| Reynolds et al. (USA) | 2009 | Case-control from registry | 0 | 58 | 60 | Registry-based; no AMD, CARMS grade 1 | Clinical Age-Related Maculopathy Staging |
| Machalińska et al. (Poland) | 2009 | Cross-sectional | 30 | 0 | 30 | Clinic-based; no AMD | Study-specific clinical definition |
| Lashkari et al. (USA) | 2018 | Hybrid | 41 | 37 | 33 | Clinic-based; no AMD, AREDS stage 0 | Age-Related Eye Disease Study |
| Lynch et al. (USA) ref. [18] | 2020b | Case-control from registry | 0 | 46 | 27 | Registry-based; cataract controls without AMD | Study-specific clinical definition |
| Lynch et al. (USA) ref. [17] | 2020a | Case-control form registry | 109 | 0 | 65 | Registry-based; cataract controls without AMD | Study-specific clinical definition |
| Lashkari et al. (USA) | 2020 | Hybrid | 24 | 37 | 33 | Clinic-based; no AMD, AREDS stage 0 | Age-Related Eye Disease Study |
| Study | Year | Activation Products | Inhibition | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| C3a | C3a-desArg | Ba | Bb | C5a | sC5b-9 | CFH | CFI | iC3b/C3b | ||
| Sivaprasad et al. | 2007 | ✗ | ||||||||
| Reynolds et al. | 2009 | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ||
| Machalińska et al. | 2009 | ✗ | ||||||||
| Lashkari et al. | 2018 | ✗ | ||||||||
| Lynch et al. ref. [18] | 2020b | ✗ | ✗ | ✗ | ||||||
| Lynch et al. ref. [17] | 2020a | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ✗ | ||
| Lashkari et al. | 2020 | ✗ | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.B.; Serghiou, S.; Miller, J.W.; Vavvas, D.G. Systemic Complement Activation Profiles in Nonexudative Age-Related Macular Degeneration: A Meta-Analysis. J. Clin. Med. 2022, 11, 2371. https://doi.org/10.3390/jcm11092371
Lin JB, Serghiou S, Miller JW, Vavvas DG. Systemic Complement Activation Profiles in Nonexudative Age-Related Macular Degeneration: A Meta-Analysis. Journal of Clinical Medicine. 2022; 11(9):2371. https://doi.org/10.3390/jcm11092371
Chicago/Turabian StyleLin, Jonathan B., Stylianos Serghiou, Joan W. Miller, and Demetrios G. Vavvas. 2022. "Systemic Complement Activation Profiles in Nonexudative Age-Related Macular Degeneration: A Meta-Analysis" Journal of Clinical Medicine 11, no. 9: 2371. https://doi.org/10.3390/jcm11092371
APA StyleLin, J. B., Serghiou, S., Miller, J. W., & Vavvas, D. G. (2022). Systemic Complement Activation Profiles in Nonexudative Age-Related Macular Degeneration: A Meta-Analysis. Journal of Clinical Medicine, 11(9), 2371. https://doi.org/10.3390/jcm11092371