
Perineural Invasion in Pancreatic Ductal Adenocarcinoma (PDAC): A Saboteur of Curative Intended Therapies?

 , , , ,
, , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Histopathological Records
2.3. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. PNI Correlates with Advanced Tumor Stage and Lymphatic Dissemination
3.3. Pn0 Status Is Associated with Improved Disease-Free and Long-Term Survival
3.4. PNI Occurs in the Majority of R0 Resected Patients and Diminished DFS and OS
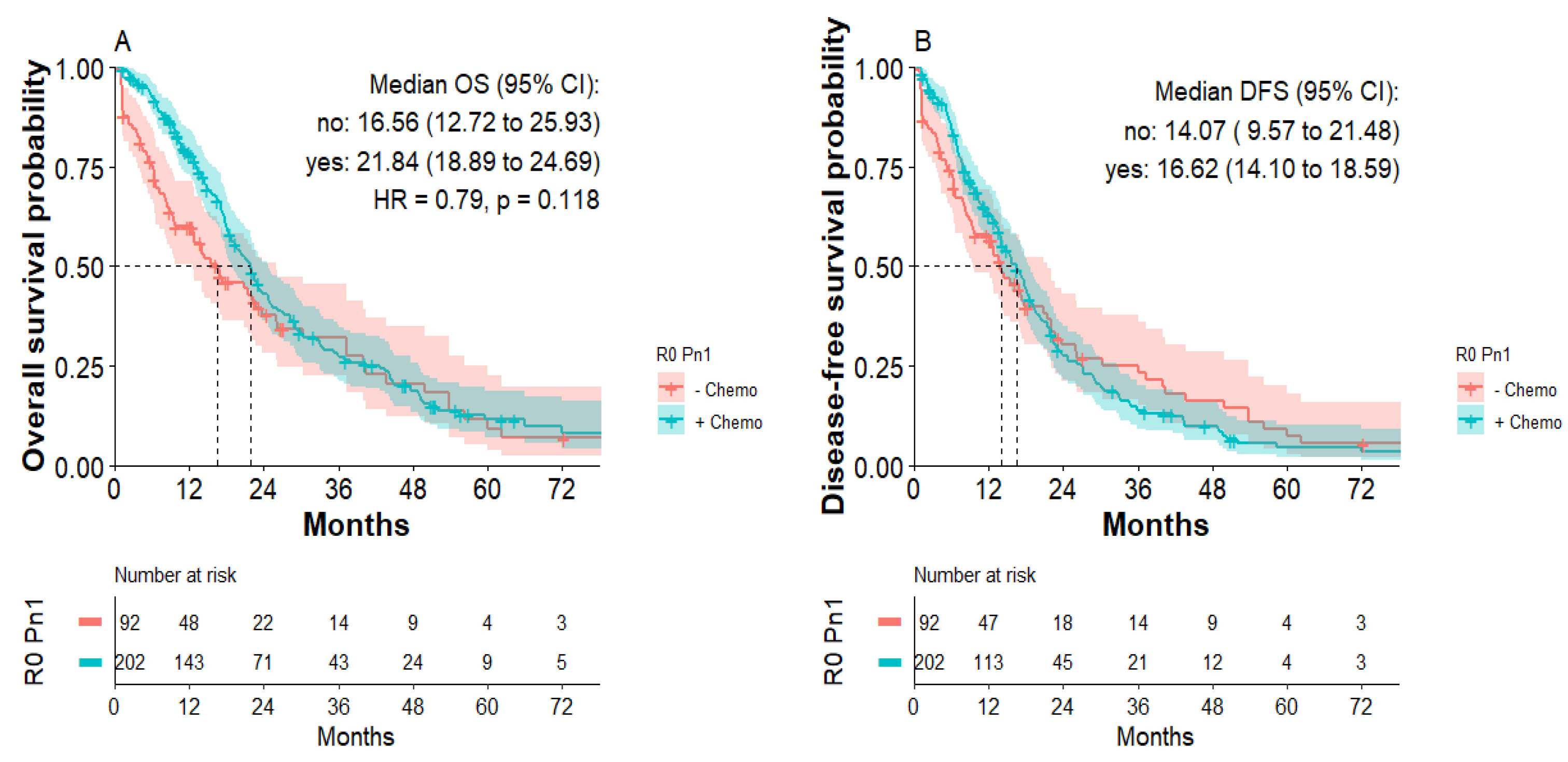
3.5. Postoperative Chemotherapy Improves OS of Pn1 Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.; Mangu, P.B.; Berlin, J.; Engebretson, A.; Hong, T.S.; Maitra, A.; Mohile, S.G.; Mumber, M.; Schulick, R.; Shapiro, M.; et al. Potentially Curable Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 2541–2556. [Google Scholar] [CrossRef]
- Isaji, S.; Mizuno, S.; Windsor, J.A.; Bassi, C.; Castillo, C.F.-D.; Hackert, T.; Hayasaki, A.; Katz, M.H.; Kim, S.-W.; Kishiwada, M.; et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma. Pancreatology 2018, 18, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Del Chiaro, M.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 439–457. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.-L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Stocken, D.D.; Bassi, C.; Ghaneh, P.; Cunningham, D.; Goldstein, D. Adjuvant chemotherapy with fluorouracil plus folinic acid vs. gemcitabine following pancreatic cancer resection: A randomized controlled trial. JAMA 2010, 304, 1073–1081. [Google Scholar] [CrossRef]
- Janssen, Q.P.; O’Reilly, E.M.; Van Eijck, C.H.J.; Koerkamp, B.G. Neoadjuvant Treatment in Patients With Resectable and Borderline Resectable Pancreatic Cancer. Front. Oncol. 2020, 10, 41. [Google Scholar] [CrossRef]
- Sohal, D.P.; Duong, M.; Ahmad, S.A.; Gandhi, N.S.; Beg, M.S.; Wang-Gillam, A. Efficacy of Perioperative Chemotherapy for Resectable Pancreatic Adenocarcinoma: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Jiang, W.; Yeap, B.Y.; Drapek, L.C. Total Neoadjuvant Therapy with FOLFIRINOX Followed by Individualized Chemoradiotherapy for Borderline Resectable Pancreatic Adenocarcinoma: A Phase 2 Clinical Trial. JAMA Oncol. 2018, 4, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Chawla, A.; Molina, G.; Pak, L.M.; Rosenthal, M.; Mancias, J.D.; Clancy, T.E.; Wolpin, B.M.; Wang, J. Neoadjuvant Therapy is Associated with Improved Survival in Borderline-Resectable Pancreatic Cancer. Ann. Surg. Oncol. 2019, 27, 1191–1200. [Google Scholar] [CrossRef]
- Groot, V.P.; Rezaee, N.; Wu, W.; Cameron, J.L.; Fishman, E.; Hruban, R.H.; Weiss, M.J.; Zheng, L.; Wolfgang, C.L.; He, J. Patterns, Timing, and Predictors of Recurrence Following Pancreatectomy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2018, 267, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Gnerlich, J.L.; Luka, S.R.; Deshpande, A.D.; Dubray, B.J.; Weir, J.S.; Carpenter, D.H. Microscopic margins and patterns of treatment failure in resected pancreatic adenocarcinoma. Arch Surg. 2012, 147, 753–760. [Google Scholar] [CrossRef]
- Allen, P.J.; Kuk, D.; Castillo, C.F.-D.; Basturk, O.; Wolfgang, C.L.; Cameron, J.L.; Lillemoe, K.D.; Ferrone, C.R.; Morales-Oyarvide, V.; He, J.; et al. Multi-institutional Validation Study of the American Joint Commission on Cancer (8th Edition) Changes for T and N Staging in Patients with Pancreatic Adenocarcinoma. Ann. Surg. 2017, 265, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Saka, B.; Balci, S.; Basturk, O.; Bagci, P.; Postlewait, L.M.; Maithel, S. Pancreatic Ductal Adenocarcinoma is Spread to the Peripancreatic Soft Tissue in the Majority of Resected Cases, Rendering the AJCC T-Stage Protocol (7th Edition) Inapplicable and Insignificant: A Size-Based Staging System (pT1: 2-4 cm) is More Valid and Clinically Relevant. Ann. Surg. Oncol. 2016, 23, 2010–2018. [Google Scholar] [PubMed]
- Basturk, O.; Saka, B.; Balci, S.; Postlewait, L.M.; Knight, J.; Goodman, M.; Kooby, D.; Sarmiento, J.M.; El-Rayes, B.; Choi, H.; et al. Substaging of Lymph Node Status in Resected Pancreatic Ductal Adenocarcinoma Has Strong Prognostic Correlations: Proposal for a Revised N Classification for TNM Staging. Ann. Surg. Oncol. 2015, 22, 1187–1195. [Google Scholar] [CrossRef]
- Ghaneh, P.; Kleeff, J.; Halloran, C.M.; Raraty, M.; Jackson, R.; Melling, J.; Jones, O.; Palmer, D.H.; Cox, T.F.; Smith, C.J.; et al. The Impact of Positive Resection Margins on Survival and Recurrence Following Resection and Adjuvant Chemotherapy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2019, 269, 520–529. [Google Scholar] [CrossRef]
- Schorn, S.; Demir, I.E.; Haller, B.; Scheufele, F.; Reyes, C.M.; Tieftrunk, E.; Sargut, M.; Goess, R.; Friess, H.; Ceyhan, G.O. The influence of neural invasion on survival and tumor recurrence in pancreatic ductal adenocarcinoma—A systematic review and meta-analysis. Surg. Oncol. 2017, 26, 105–115. [Google Scholar] [CrossRef]
- Yamada, M.; Sugiura, T.; Okamura, Y.; Ito, T.; Yamamoto, Y.; Ashida, R.; Sasaki, K.; Nagino, M.; Uesaka, K. Microscopic Venous Invasion in Pancreatic Cancer. Ann. Surg. Oncol. 2018, 25, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Panaro, F.; Kellil, T.; Vendrell, J.; Sega, V.; Souche, R.; Piardi, T.; Leon, P.; Cassinotto, C.; Assenat, E.; Rosso, E.; et al. Microvascular invasion is a major prognostic factor after pancreatico-duodenectomy for adenocarcinoma. J. Surg. Oncol. 2019, 120, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Bs, J.D.E.; Kozak, G.; Fong, Z.V.; He, J.; Javed, A.A.; Joneja, U.; Jiang, W.; Ferrone, C.R.; Lillemoe, K.D.; Cameron, J.L.; et al. Microscopic lymphovascular invasion is an independent predictor of survival in resected pancreatic ductal adenocarcinoma. J. Surg. Oncol. 2017, 116, 658–664. [Google Scholar] [CrossRef]
- Liebl, F.; Demir, I.E.; Mayer, K.; Schuster, T.; D’Haese, J.G.; Becker, K. The impact of neural invasion severity in gastrointestinal malignancies: A clinicopathological study. Ann. Surg. 2014, 260, 900–907. [Google Scholar] [CrossRef]
- Stopczynski, R.E.; Normolle, D.P.; Hartman, D.J.; Ying, H.; DeBerry, J.; Bielefeldt, K.; Rhim, A.D.; DePinho, R.; Albers, K.; Davis, B. Neuroplastic changes occur early in the development of pancreatic ductal adenocarcinoma. Cancer Res. 2014, 74, 1718–1727. [Google Scholar] [CrossRef]
- Crippa, S.; Pergolini, I.; Javed, A.A.; Honselmann, K.C.; Weiss, M.J.; Di Salvo, F. Implications of Perineural Invasion on Disease Recurrence and Survival After Pancreatectomy for Pancreatic Head Ductal Adenocarcinoma. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- Göhrig, A.; Detjen, K.M.; Hilfenhaus, G.; Körner, J.L.; Welzel, M.; Arsenic, R.; Schmuck, R.; Bahra, M.; Wu, J.Y.; Wiedenmann, B.; et al. Axon Guidance Factor SLIT2 Inhibits Neural Invasion and Metastasis in Pancreatic Cancer. Cancer Res. 2014, 74, 1529–1540. [Google Scholar] [CrossRef]
- Cavel, O.; Shomron, O.; Shabtay, A.; Vital, J.; Trejo-Leider, L.; Weizman, N.; Krelin, Y.; Fong, Y.; Wong, R.J.; Amit, M.; et al. Endoneurial Macrophages Induce Perineural Invasion of Pancreatic Cancer Cells by Secretion of GDNF and Activation of RET Tyrosine Kinase Receptor. Cancer Res. 2012, 72, 5733–5743. [Google Scholar] [CrossRef]
- Abiatari, I.; DeOliveira, T.; Kerkadze, V.; Schwager, C.; Esposito, I.; Giese, N.A.; Huber, P.; Bergman, F.; Abdollahi, A.; Friess, H.; et al. Consensus transcriptome signature of perineural invasion in pancreatic carcinoma. Mol. Cancer Ther. 2009, 8, 1494–1504. [Google Scholar] [CrossRef]
- Gasparini, G.; Pellegatta, M.; Crippa, S.; Lena, M.S.; Belfiori, G.; Doglioni, C.; Taveggia, C.; Falconi, M. Nerves and Pancreatic Cancer: New Insights into a Dangerous Relationship. Cancers 2019, 11, 893. [Google Scholar] [CrossRef]
- Sobin, L.H.; Compton, C.C. TNM seventh edition: What’s new, what’s changed: Communication from the International Union Against Cancer and the American Joint Committee on Cancer. Cancer 2010, 116, 5336–5339. [Google Scholar] [CrossRef] [PubMed]
- Zins, M.; Matos, C.; Cassinotto, C. Pancreatic Adenocarcinoma Staging in the Era of Preoperative Chemotherapy and Radiation Therapy. Radiology 2018, 287, 374–390. [Google Scholar] [CrossRef] [PubMed]
- Kayahara, M.; Nakagawara, H.; Kitagawa, H.; Ohta, T. The Nature of Neural Invasion by Pancreatic Cancer. Pancreas 2007, 35, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.; Jin, G.; Hu, X.; Shi, M.; Zhang, Y.; Liu, R.; Zhou, Y.; Shao, C.; Zheng, J.; Zhu, M. Analysis of tumor-induced lymphangiogenesis and lymphatic vessel invasion of pancreatic carcinoma in the peripheral nerve plexus. Cancer Sci. 2012, 103, 1756–1763. [Google Scholar] [CrossRef]
- Tummers, W.S.; Groen, J.V.; Mulder, B.G.S.; Farina-Sarasqueta, A.; Morreau, J.; Putter, H.; Van De Velde, C.J.; Vahrmeijer, A.L.; Bonsing, B.A.; Mieog, J.S.; et al. Impact of resection margin status on recurrence and survival in pancreatic cancer surgery. Br. J. Surg. 2019, 106, 1055–1065. [Google Scholar] [CrossRef]
- Merz, V.; Cavaliere, A.; Messina, C.; Salati, M.; Zecchetto, C.; Casalino, S.; Milella, M.; Caffo, O.; Melisi, D. Multicenter Retrospective Analysis of Second-Line Therapy after Gemcitabine Plus Nab-Paclitaxel in Advanced Pancreatic Cancer Patients. Cancers 2020, 12, 1131. [Google Scholar] [CrossRef]
- Vernuccio, F.; Messina, C.; Merz, V.; Cannella, R.; Midiri, M. Resectable and Borderline Resectable Pancreatic Ductal Adenocarcinoma: Role of the Radiologist and Oncologist in the Era of Precision Medicine. Diagnostics 2021, 11, 2166. [Google Scholar] [CrossRef]
- Timmermann, L.; Rosumeck, N.; Klein, F.; Pratschke, J.; Pelzer, U.; Bahra, M.; Malinka, T. Neoadjuvant Chemotherapy Enhances Local Postoperative Histopathological Tumour Stage in Borderline Resectable Pancreatic Cancer—A Matched-Pair Analysis. Anticancer Res. 2019, 39, 5781–5787. [Google Scholar] [CrossRef]
- Chatterjee, D.; Katz, M.H.; Rashid, A.; Wang, H.; Iuga, A.C.; Varadhachary, G.R.; Wolff, R.A.; Lee, J.E.; Pisters, P.W.; Crane, C.H.; et al. Perineural and Intraneural Invasion in Posttherapy Pancreaticoduodenectomy Specimens Predicts Poor Prognosis in Patients with Pancreatic Ductal Adenocarcinoma. Am. J. Surg. Pathol. 2012, 36, 409–417. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Marchegiani, G.; Hong, T.S.; Ryan, D.P.; Deshpande, V.; McDonnell, E.I.; Sabbatino, F.; Santos, D.D.; Allen, J.N.; Blaszkowsky, L.S.; et al. Radiological and Surgical Implications of Neoadjuvant Treatment with FOLFIRINOX for Locally Advanced and Borderline Resectable Pancreatic Cancer. Ann. Surg. 2015, 261, 12–17. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | % | Pn0 | % | Pn1 | % | Statistics * | |
|---|---|---|---|---|---|---|---|
| Cases | 571 | 40 | 531 | ||||
| Age (years) | 65.6 (+/−11.1) | 64.7 (+/−10.5) | 65.6 (+/−10.8) | p = 0.58 | |||
| Sex | female 264 | 46.2 | female 22 | 55 | female 242 | 45.6 | p = 0.26 |
| male 307 | 53.8 | male 18 | 45 | male 289 | 54.4 | ||
| Body mass index (BMI) (in kg/m2) | 25.1 (+/−4.3) | 23.6 (+/−4.0) | 25.2 (+/−4.3) | p = 0.05 | |||
| Diabetes mellitus (DM) | |||||||
| DM I | 19 | 3.3 | 0 | 0 | 19 | 3.6 | p = 0.39 |
| DM II | 116 | 20.3 | 7 | 17.5 | 109 | 20.5 | p = 0.84 |
| Beta blocker | p = 0.22 | ||||||
| ß1 selective | 168 | 29.4 | 9 | 22.5 | 159 | 29.9 | |
| Non-selective | 12 | 2.1 | 0 | 0 | 12 | 2.3 | |
| Carbohydrate-antigen 19-9 (in U/mL) | 846.3 (+/−3014) | 453.6 (+/−1303) | 888.5 (+/−3142) | p = 0.49 | |||
| Carcinoembryonic antigen (in µg/L) | 18.8 (+/−67.9) | 4.5 (+/−3.2) | 20.0 (+/−72.9) | p = 0.28 | |||
| Tumor entity | p = 0.77 | ||||||
| Head | 427 | 74.8 | 28 | 70 | 399 | 75.1 | |
| Tail | 70 | 12.3 | 7 | 17.5 | 63 | 11.9 | |
| Body | 46 | 8.1 | 3 | 7.5 | 43 | 8.1 | |
| Uncinate | 28 | 4.9 | 2 | 5 | 26 | 4.9 | |
| Surgical procedure | p = 0.05 | ||||||
| PPPD ** | 363 | 63.6 | 20 | 50 | 343 | 64.6 | |
| Whipple | 29 | 5.1 | 5 | 12.5 | 24 | 4.5 | |
| Total | 94 | 16.5 | 6 | 15 | 88 | 16.5 | |
| Distal | 85 | 14.9 | 9 | 22.5 | 76 | 14.3 | |
| Chemotherapy | |||||||
| Pre-operative | 64 | 11.2 | 8 | 20 | 56 | 10.5 | p = 0.11 |
| Post-operative | 353 | 61.8 | 28 | 70 | 325 | 61.2 | p = 0.31 |
| Clinical Outcome | |||||||
| Follow-up (months) | 17.2 | 24.2 | 16.6 | p = 0.04 | |||
| 30-day mortality | 28 | 5.2 | 0 | 0 | 28 | 5.6 | p = 0.25 |
| Death | 383 | 78.8 | 15 | 41.7 | 368 | 81.8 | p < 0.001 |
| Alive | 103 | 18.0 | 21 | 52.5 | 82 | 15.4 | p < 0.001 |
| Lost to follow-up | 85 | 14.9 | 4 | 10 | 81 | 15.3 | p = 0.49 |
| LTS *** (>5 years) | 19 | 3.3 | 4 | 10 | 15 | 2.8 | p = 0.04 |
| Recurrence | |||||||
| Yes | 167 | 29.2 | 11 | 27.5 | 156 | 29.4 | p = 0.86 |
| No | 404 | 70.8 | 29 | 72.5 | 375 | 70.6 |
| Total | % | Pn0 | % | Pn1 | % | Statistics * | |
|---|---|---|---|---|---|---|---|
| Cases | 571 | 40 | 531 | ||||
| Tumor stage | p = 0.007 | ||||||
| pT1 (<2 cm) | 68 | 11.9 | 12 | 30 | 56 | 10.5 | |
| pT2 (2–4 cm) | 323 | 56.6 | 20 | 50 | 299 | 57.1 | |
| pT3 (>4 cm) | 176 | 27.3 | 8 | 20 | 148 | 27.9 | |
| pT4 (vessel infiltration) | 24 | 4.2 | 0 | 0 | 24 | 4.5 | |
| Lymph node metastasis | p < 0.001 | ||||||
| N− | 154 | 27 | 24 | 60 | 130 | 24.5 | |
| N+ | 417 | 73 | 16 | 40 | 401 | 75.5 | |
| Distant metastasis | p = 0.3 | ||||||
| M0 | 510 | 89.3 | 38 | 95 | 472 | 88.9 | |
| M1 | 61 | 10.7 | 2 | 5 | 59 | 11.1 | |
| Histologic grade | p = 0.03 | ||||||
| G1 | 20 | 3.5 | 4 | 10 | 16 | 3 | |
| G2 | 348 | 60.9 | 27 | 67.5 | 321 | 60.5 | |
| G3 | 203 | 35.6 | 9 | 22.5 | 194 | 36.5 | |
| Resection margin | p = 0.06 | ||||||
| R0 | 359 | 62.9 | 31 | 77.5 | 328 | 61.8 | |
| R1 | 212 | 37.1 | 9 | 22.5 | 203 | 38.2 | |
| Vascular invasion | p = 0.09 | ||||||
| V0 | 467 | 81.8 | 37 | 92.5 | 430 | 81 | |
| V1 | 104 | 18.2 | 3 | 7.5 | 101 | 19 | |
| Lymphatic invasion | p < 0.001 | ||||||
| L0 | 330 | 57.8 | 33 | 82.5 | 297 | 55.9 | |
| L1 | 241 | 42.2 | 7 | 17.5 | 234 | 44.1 |
| Variable | Odds Ratio | Standard Error | Estimate | p-Value |
|---|---|---|---|---|
| Age | 1.155 | 0.323 | 0.444 | 0.657 |
| Sex | 0.615 | 0.684 | −0.710 | 0.478 |
| Tumor size (<4 cm vs. >4 cm) | 0.747 | 0.736 | −0.395 | 0.693 |
| G1-2 vs. G3 | 1.921 | 0.755 | 0.864 | 0.388 |
| R0 vs. R1 | 3.166 | 0.892 | 1.292 | 0.196 |
| pN+ vs. pN- | 6.080 | 0.679 | 2.659 | 0.008 |
| neoadjuvant Chemo | 0.830 | 0.705 | −0.264 | 0.792 |
| BMI | 1.517 | 0.315 | 1.325 | 0.185 |
| DM II | 0.480 | 0.813 | −0.905 | 0.366 |
| CEA | 5.105 | 2.140 | 0.762 | 0.446 |
| CA 19-9 | 0.924 | 0.285 | −0.278 | 0.781 |
| Variable | Hazard Ratio | Standard Error | Estimate | p-Value |
|---|---|---|---|---|
| Overall survival (OS) | ||||
| Age | 1.021 | 0.005 | 3.902 | <0.001 |
| Sex | 0.827 | 0.109 | −1.739 | 0.082 |
| Pn0 vs. Pn1 | 2.013 | 0.270 | 2.596 | 0.009 |
| Tumor size (<4 cm vs. >4 cm) | 1.203 | 0.116 | 1.591 | 0.112 |
| pN+ vs. pN- | 1.190 | 0.130 | 1.340 | 0.180 |
| R0 vs. R1 | 1.708 | 0.115 | 4.637 | <0.001 |
| G1-2 vs. G3 | 1.211 | 0.112 | 1.706 | 0.088 |
| adjuvant Chemo | 0.721 | 0.121 | −2.696 | 0.007 |
| neoadjuvant Chemo | 0.601 | 0.240 | −2.121 | 0.034 |
| Disease-free survival (DFS) | ||||
| Age | 1.014 | 0.005 | 2.712 | 0.007 |
| Sex | 0.872 | 0.109 | −1.261 | 0.207 |
| Pn0 vs. Pn1 | 1.963 | 0.271 | 2.490 | 0.013 |
| Tumor size (<4 cm vs. >4 cm) | 1.204 | 0.117 | 1.592 | 0.111 |
| pN+ vs. pN- | 1.308 | 0.130 | 2.058 | 0.040 |
| R0 vs. R1 | 1.568 | 0.116 | 3.885 | <0.001 |
| G1-2 vs. G3 | 1.269 | 0.113 | 2.112 | 0.035 |
| adjuvant Chemo | 0.936 | 0.123 | −0.538 | 0.590 |
| neoadjuvant Chemo | 0.658 | 0.241 | −1.737 | 0.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Felsenstein, M.; Lindhammer, F.; Feist, M.; Hillebrandt, K.H.; Timmermann, L.; Benzing, C.; Globke, B.; Zocholl, D.; Hu, M.; Fehrenbach, U.; et al. Perineural Invasion in Pancreatic Ductal Adenocarcinoma (PDAC): A Saboteur of Curative Intended Therapies? J. Clin. Med. 2022, 11, 2367. https://doi.org/10.3390/jcm11092367
Felsenstein M, Lindhammer F, Feist M, Hillebrandt KH, Timmermann L, Benzing C, Globke B, Zocholl D, Hu M, Fehrenbach U, et al. Perineural Invasion in Pancreatic Ductal Adenocarcinoma (PDAC): A Saboteur of Curative Intended Therapies? Journal of Clinical Medicine. 2022; 11(9):2367. https://doi.org/10.3390/jcm11092367
Chicago/Turabian StyleFelsenstein, Matthäus, Flora Lindhammer, Mathilde Feist, Karl Herbert Hillebrandt, Lea Timmermann, Christian Benzing, Brigitta Globke, Dario Zocholl, Mengwen Hu, Uli Fehrenbach, and et al. 2022. "Perineural Invasion in Pancreatic Ductal Adenocarcinoma (PDAC): A Saboteur of Curative Intended Therapies?" Journal of Clinical Medicine 11, no. 9: 2367. https://doi.org/10.3390/jcm11092367
APA StyleFelsenstein, M., Lindhammer, F., Feist, M., Hillebrandt, K. H., Timmermann, L., Benzing, C., Globke, B., Zocholl, D., Hu, M., Fehrenbach, U., Sinn, B. V., Pelzer, U., Sauer, I. M., Pratschke, J., & Malinka, T. (2022). Perineural Invasion in Pancreatic Ductal Adenocarcinoma (PDAC): A Saboteur of Curative Intended Therapies? Journal of Clinical Medicine, 11(9), 2367. https://doi.org/10.3390/jcm11092367