
Favorable Impact of a Multidisciplinary Team Approach on Heart Transplantation Outcomes in a Mid-Volume Center

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. MDT Approach
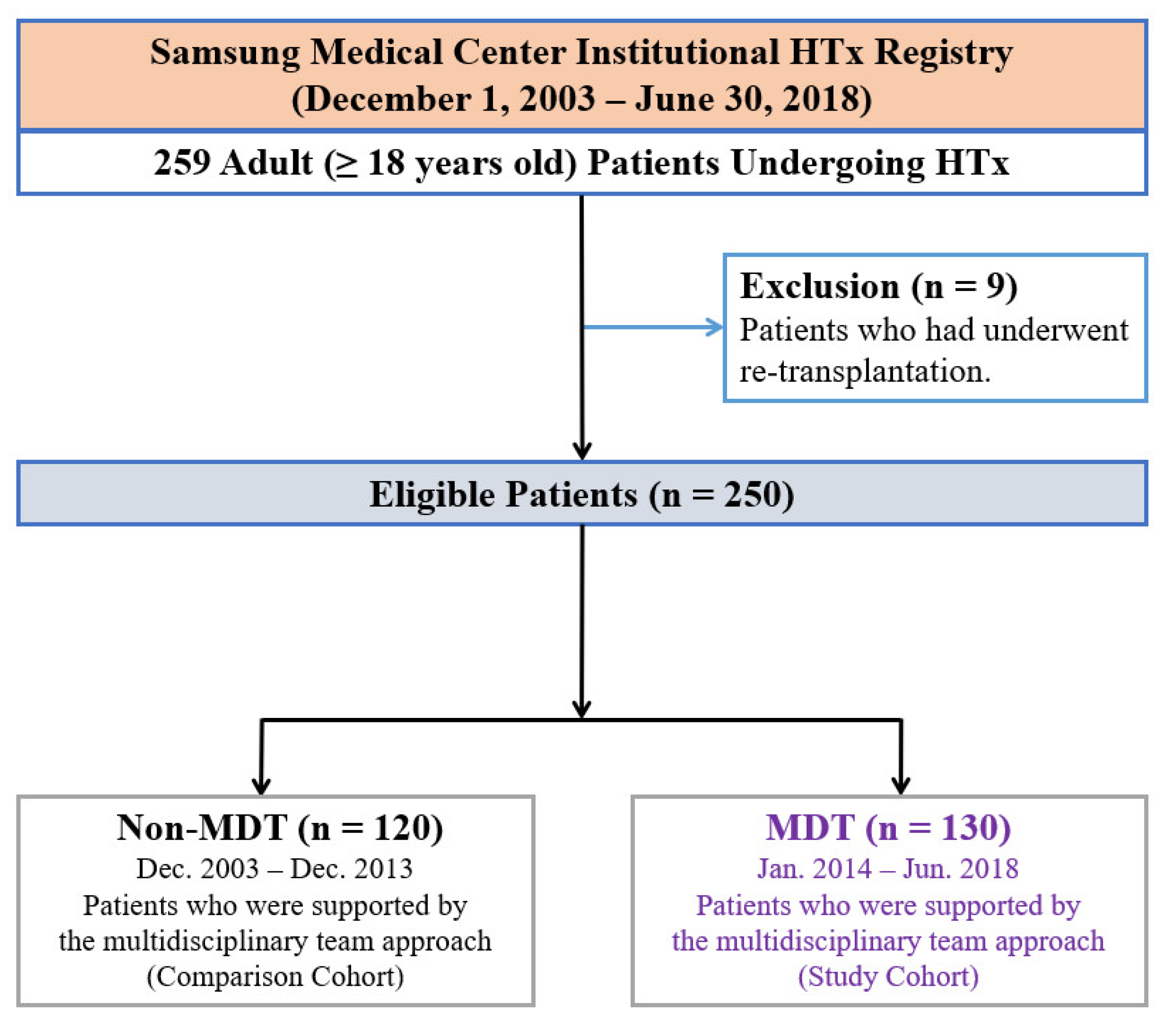
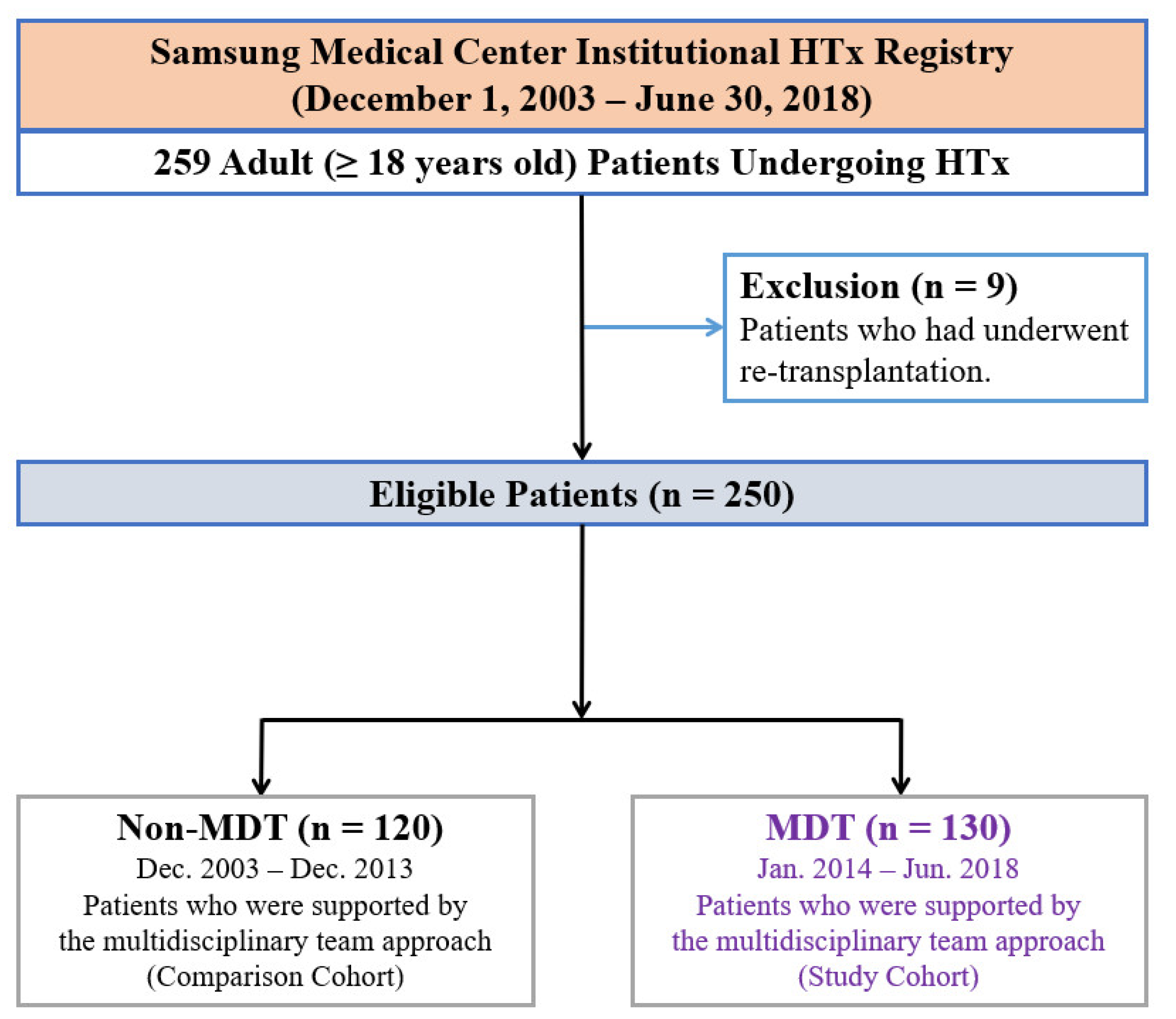
2.2. Study Population, Data Collection, and Endpoints
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Baseline Characteristics
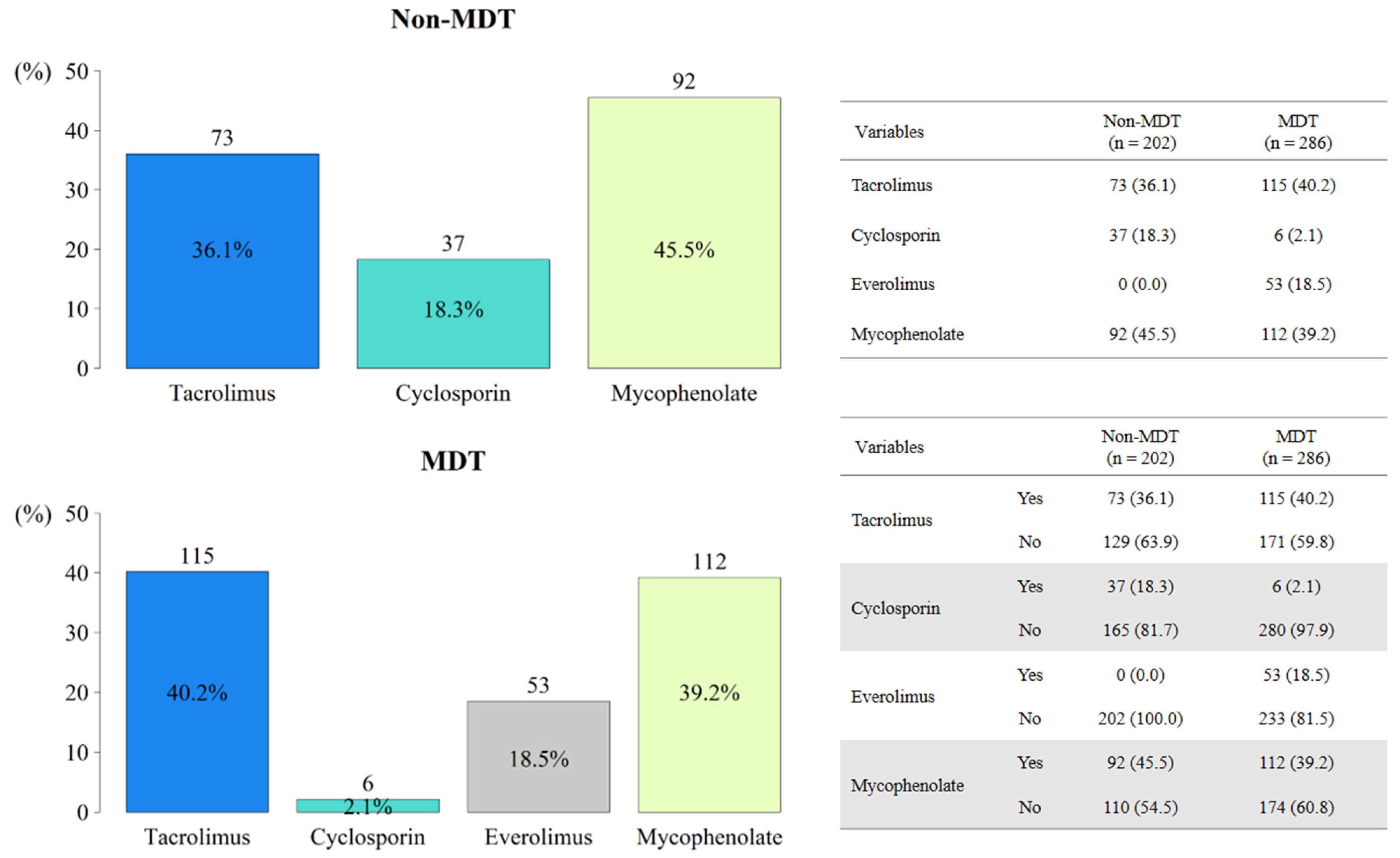
3.2. Operative and Postoperative Characteristics
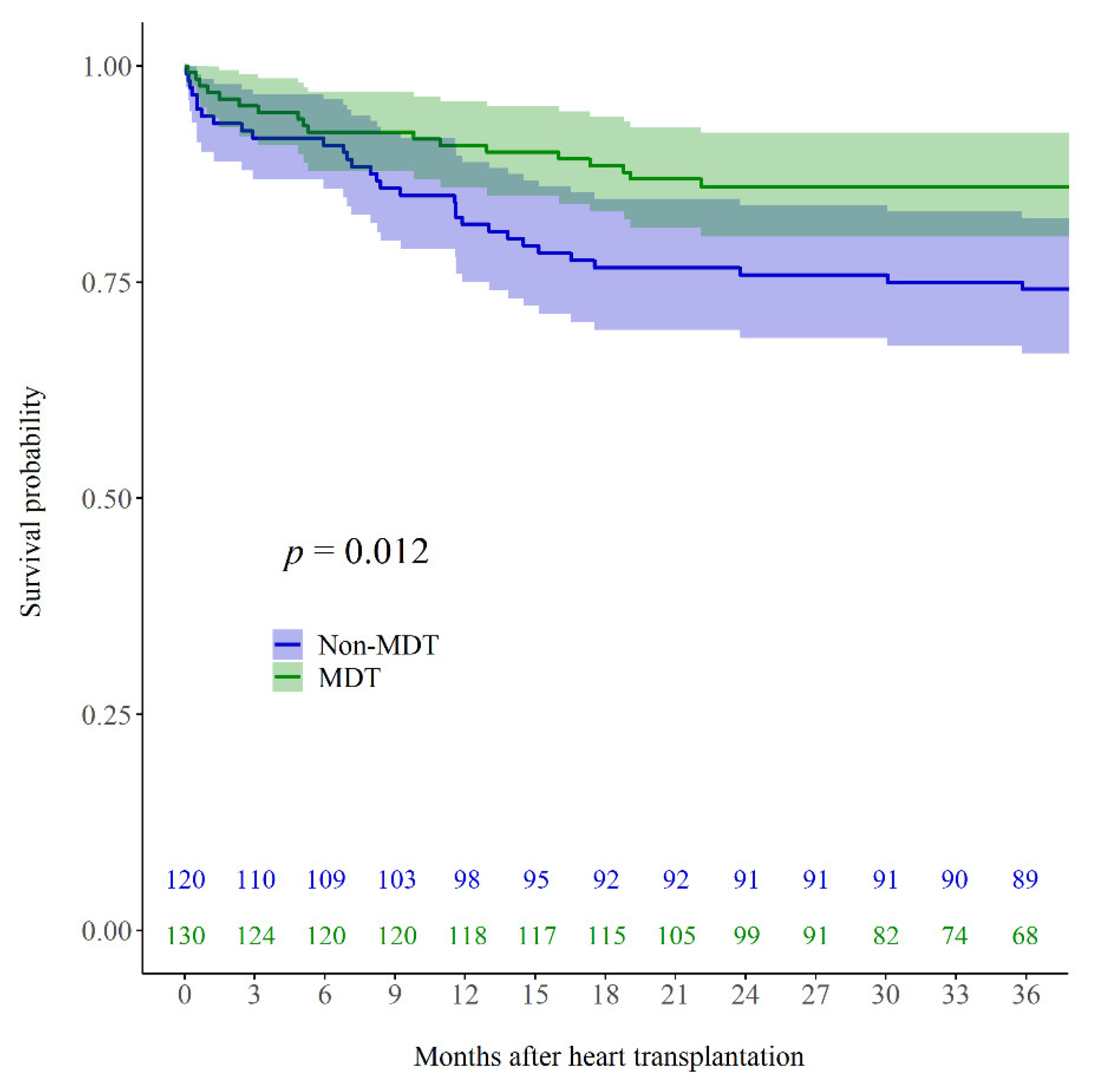
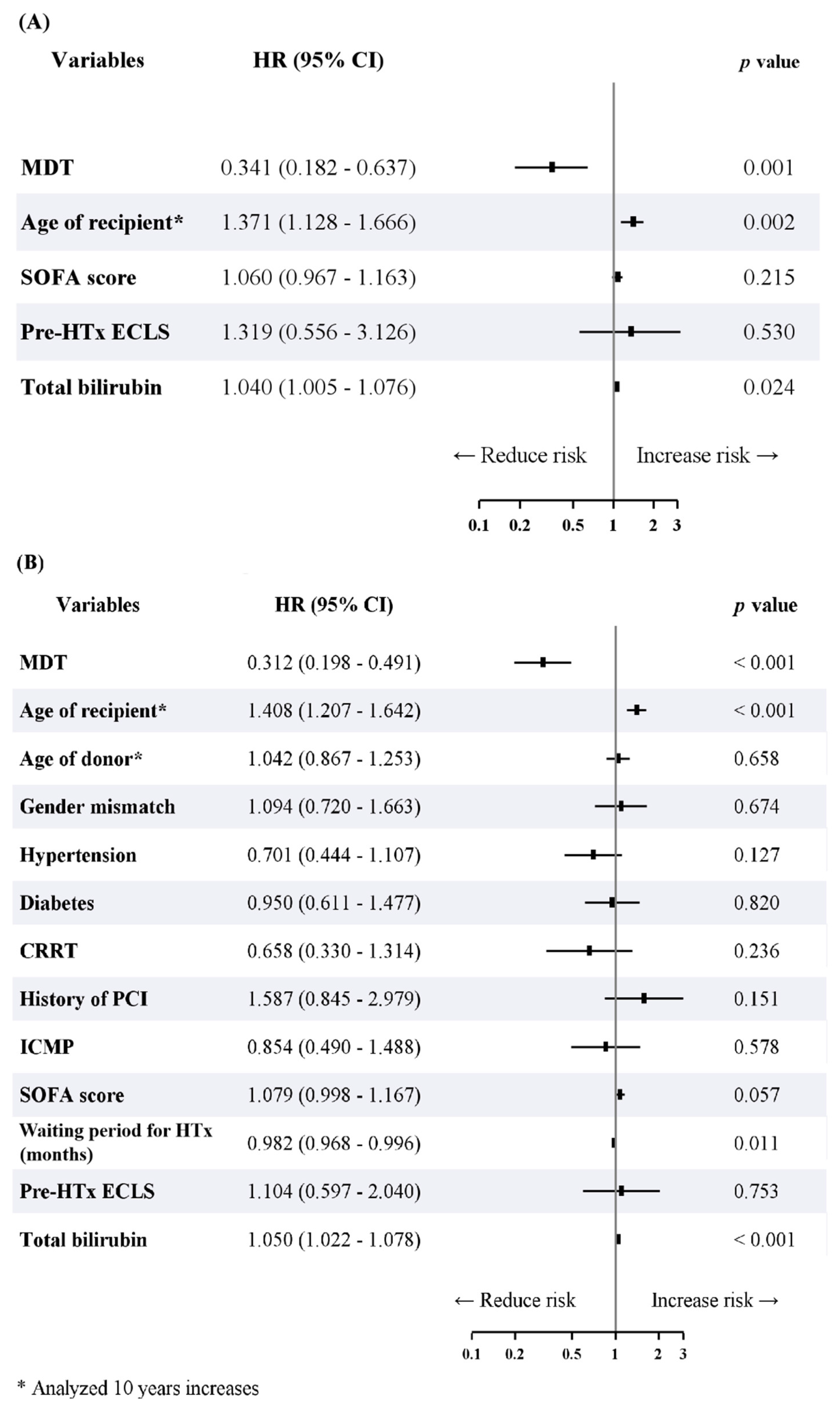
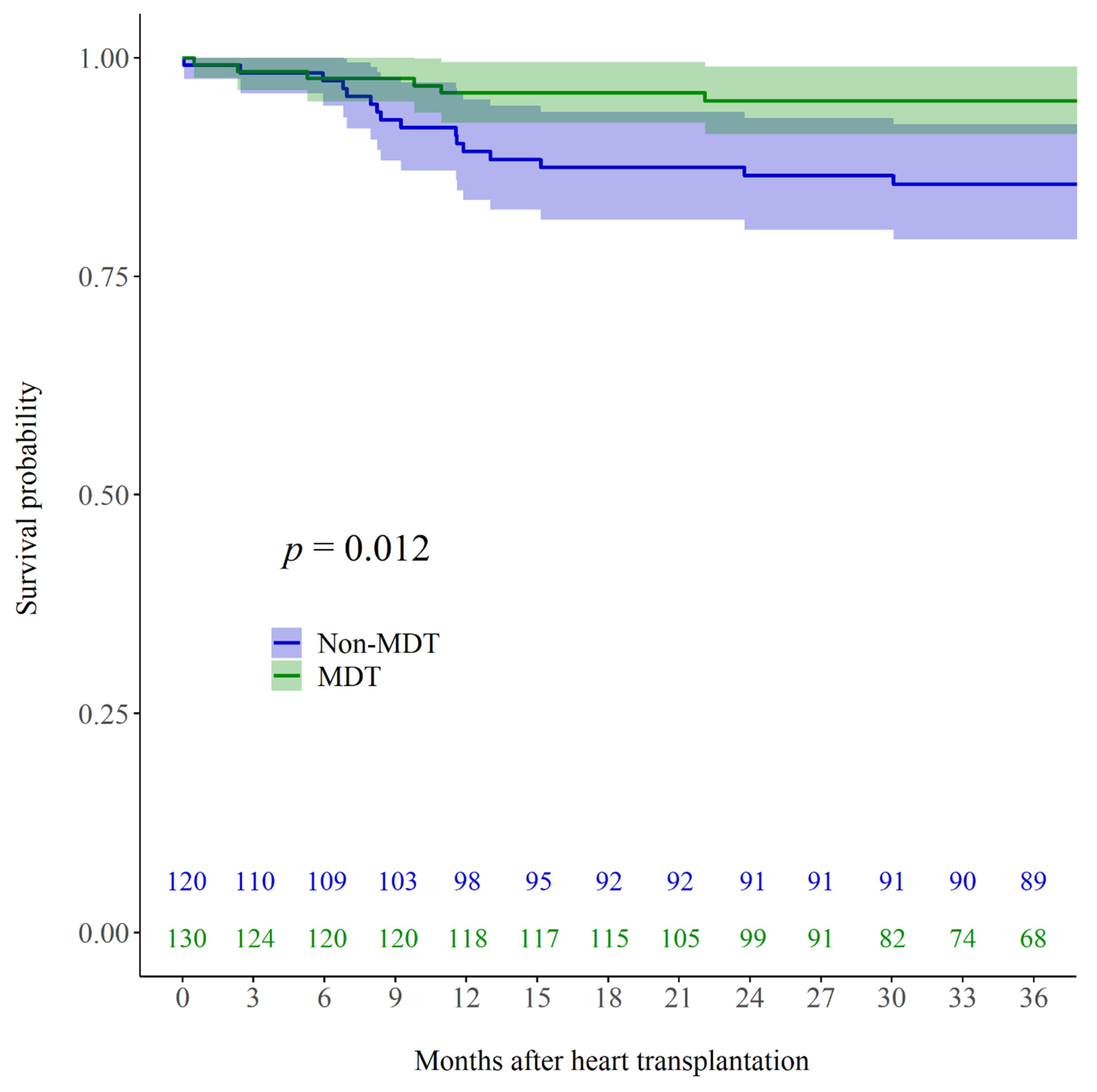
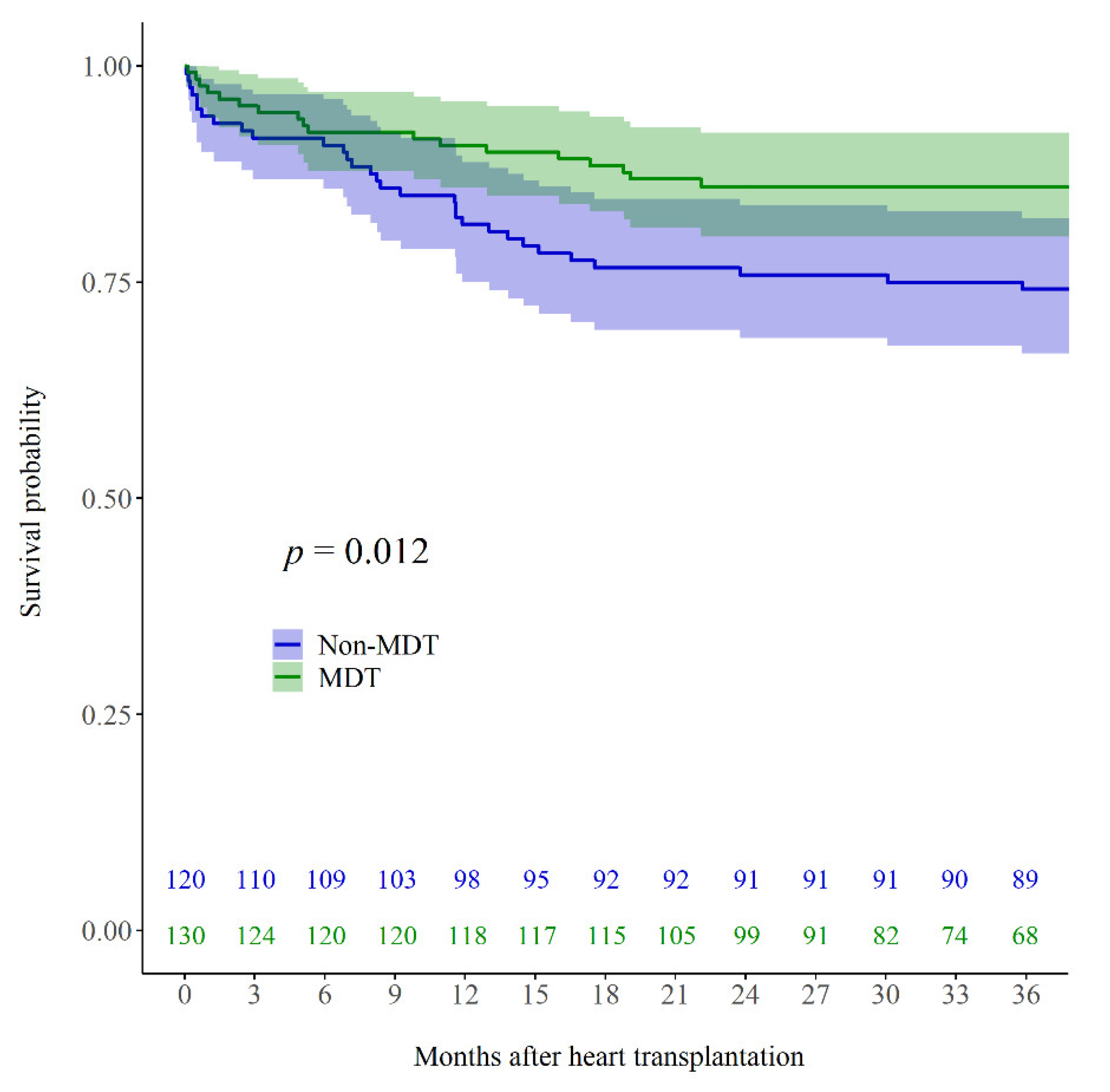
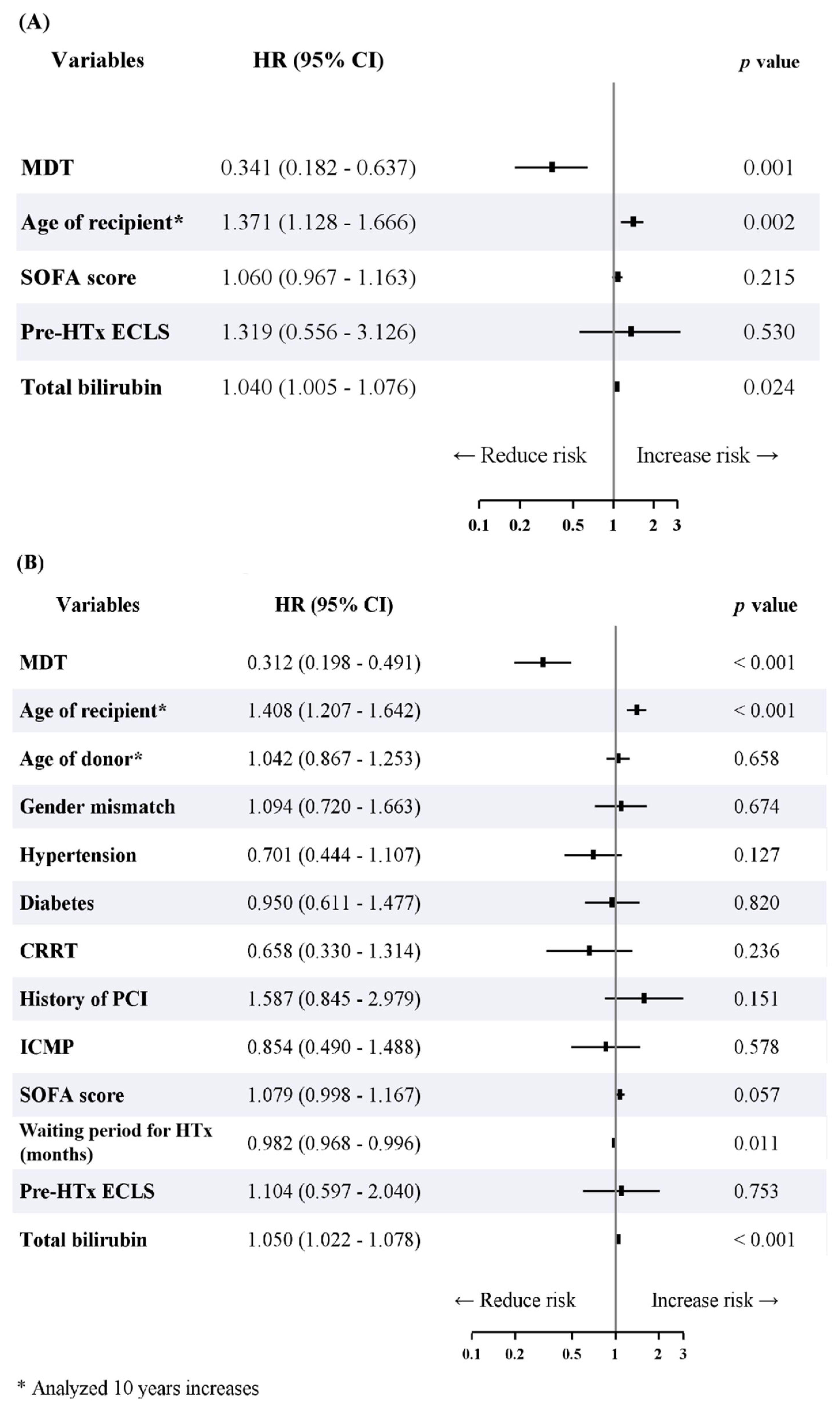
3.3. Impact of the MDT and Predictors of Overall Mortality
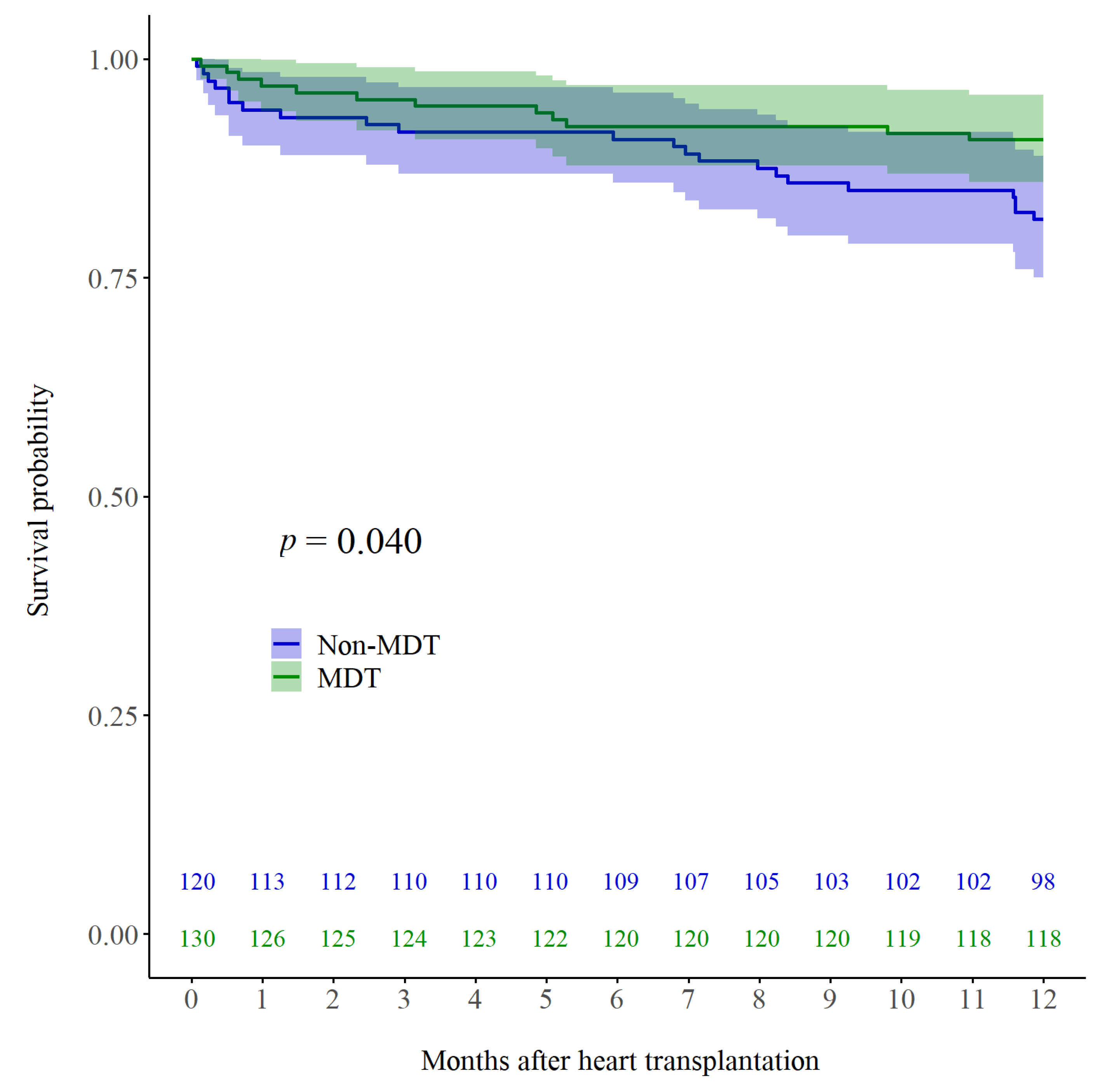
3.4. Early Clinical Outcomes
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-MDT | MDT | |
|---|---|---|
| Duration | Before 2014 | Since 2014 |
| Member | HF cardiologist Cardiac surgeon | HF cardiologist Cardiac surgeon Intensive care team ECLS team |
| Character of meeting | Weekly offline meeting | Weekly offline meeting Real-time online information sharing (24 h a day and seven days a week) |
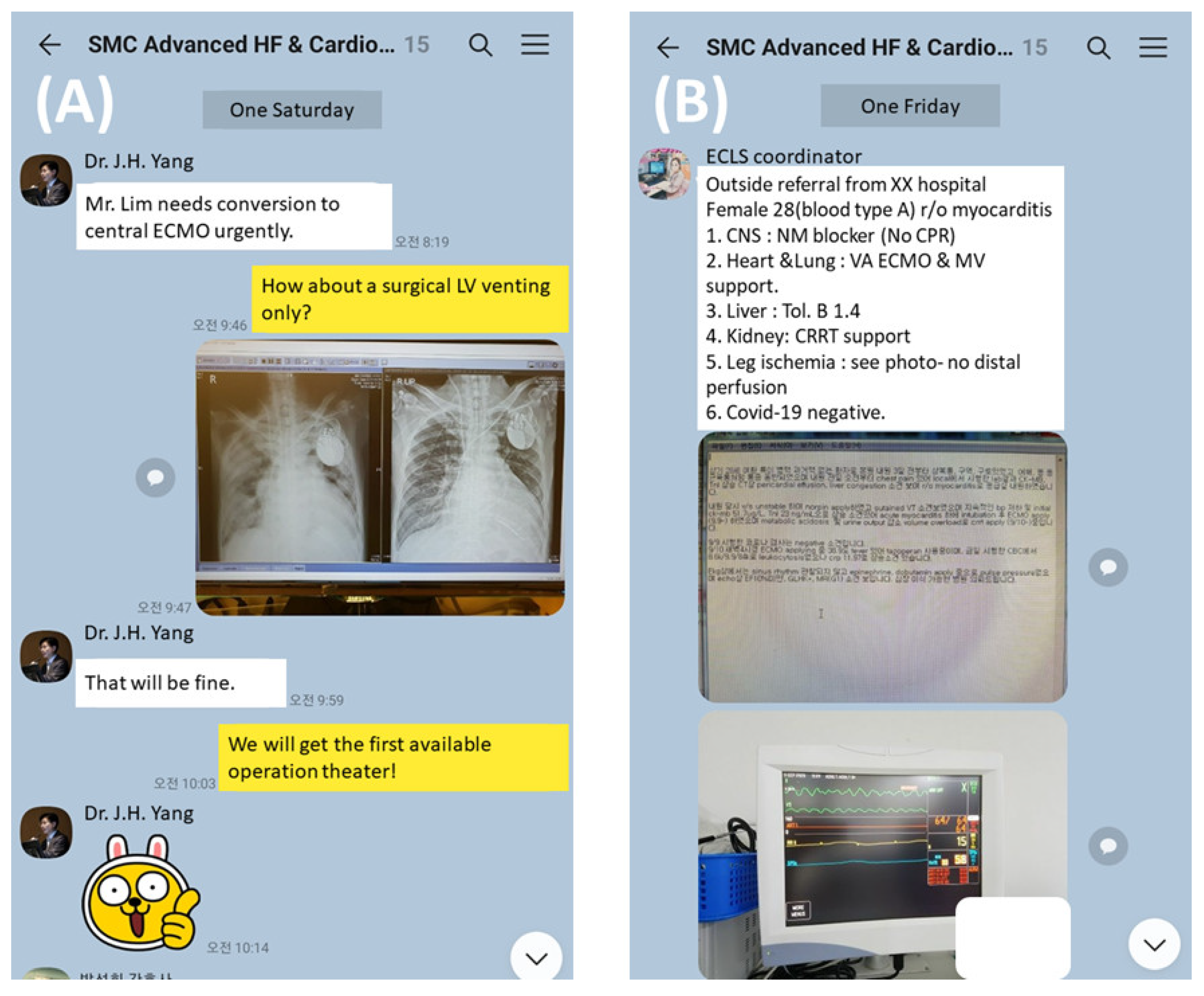
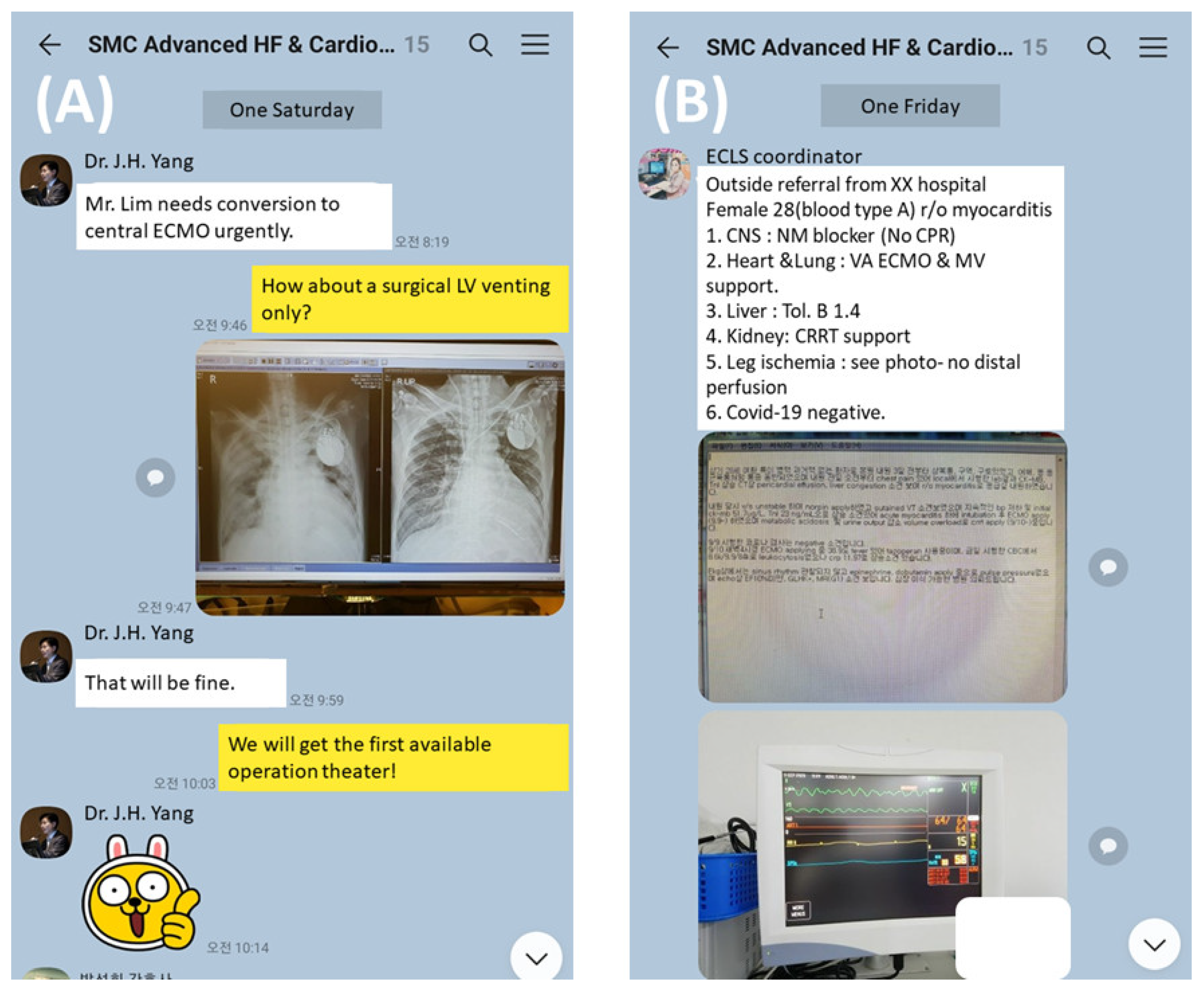
| Information sharing method | Traditional contact (face-to-face or telephone) | Combination of traditional method and a secure online group chat room provided by a social network service (KakaoTalk; Figure A1) |
Appendix C
| Variables |
|---|
| Age of recipient |
| Age of donor |
| Gender mismatch |
| Same ABO type matching |
| Hypertension |
| Diabetes |
| Stroke |
| Previous cardiac surgery |
| LVAD |
| Dialysis |
| CRRT |
| History of PCI |
| LVEF |
| HFpEF |
| ICMP |
| SOFA score |
| Waiting period for HTx (months) |
| Pre-HTx ECLS |
| Total bilirubin |
Appendix D
Appendix E
| Before Adjustment (IPTW) | After Adjustment (IPTW) | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | |||||
| p Value | Unadjusted HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | Adjusted HR (95% CI) | |
| MDT | 0.014 | 0.486 (0.274–0.863) | 0.001 | 0.341 (0.182–0.637) | 0.002 | 0.506 (0.327–0.783) | <0.001 | 0.312 (0.198–0.491) |
| Age of recipient * | 0.010 | 1.301 (1.064–1.592) | 0.002 | 1.371 (1.128–1.666) | < 0.001 | 1.460 (1.233–1.728) | <0.001 | 1.408 (1.207–1.642) |
| Age of donor * | 0.840 | 1.022 (0.824–1.269) | 0.002 | 1.285 (1.093–1.511) | 0.658 | 1.042 (0.867–1.253) | ||
| Gender mismatch | 0.222 | 1.371 (0.826–2.277) | 0.011 | 1.625 (1.117–2.364) | 0.674 | 1.094 (0.720–1.663) | ||
| Same ABO type matching | 0.652 | 0.875 (0.489–1.565) | 0.548 | 0.864 (0.535–1.393) | ||||
| Hypertension | 0.926 | 0.976 (0.582–1.635) | 0.002 | 0.540 (0.368–0.794) | 0.127 | 0.701 (0.444–1.107) | ||
| Diabetes | 0.430 | 1.257 (0.713–2.218) | 0.012 | 1.663 (1.116–2.478) | 0.820 | 0.950 (0.611–1.477) | ||
| Stroke | 0.543 | 0.731 (0.265–2.010) | 0.508 | 0.765 (0.347–1.689) | ||||
| Previous cardiac surgery | 0.690 | 1.128 (0.623–2.042) | 0.847 | 1.046 (0.662–1.653) | ||||
| LVAD | 0.806 | 1.135 (0.412–3.125) | 0.832 | 1.092 (0.484–2.462) | ||||
| Dialysis | 0.419 | 1.308 (0.683–2.505) | 0.254 | 1.338 (0.812–2.204) | ||||
| CRRT | 0.516 | 1.280 (0.608–2.696) | 0.048 | 1.742 (1.006–3.015) | 0.236 | 0.658 (0.330–1.314) | ||
| History of PCI | 0.641 | 0.845 (0.417–1.712) | 0.013 | 1.749 (1.126–2.715) | 0.151 | 1.587 (0.845–2.979) | ||
| LVEF (%) | 0.414 | 1.008 (0.989–1.028) | 0.635 | 0.996 (0.980–1.012) | ||||
| HFpEF | 0.314 | 1.437 (0.710–2.908) | 0.985 | 1.005 (0.572–1.768) | ||||
| ICMP | 0.583 | 1.177 (0.658–2.105) | 0.006 | 1.756 (1.173–2.627) | 0.578 | 0.854 (0.490–1.488) | ||
| SOFA score | <0.001 | 1.102 (1.045–1.162) | 0.215 | 1.060 (0.967–1.163) | <0.001 | 1.138 (1.096–1.181) | 0.057 | 1.079 (0.998–1.167) |
| Waiting period for HTx (months) | 0.358 | 0.985 (0.954–1.017) | <0.001 | 0.968 (0.953–0.983) | 0.011 | 0.982 (0.968–0.996) | ||
| Pre-HTx ECLS | 0.060 | 1.622 (0.981–2.682) | 0.530 | 1.319 (0.556–3.126) | <0.001 | 2.448 (1.704–3.518) | 0.753 | 1.104 (0.597–2.040) |
| Total bilirubin (mg/dL) | 0.000 | 1.047 (1.021–1.074) | 0.024 | 1.040 (1.005–1.076) | <0.001 | 1.064 (1.045–1.083) | <0.001 | 1.050 (1.022–1.078) |
Appendix F
Appendix G
References
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA Guideline for the management of heart failure. Circulation 2013, 128, e240–e327. [Google Scholar] [PubMed]
- Costanzo, M.R.; Dipchand, A.; Starling, R.; Anderson, A.; Chan, M.; Desai, S.; Fedson, S.; Fisher, P.; Gonzales-Stawinski, G.; Martinelli, L.; et al. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2010, 29, 914–956. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC): Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- Morton, G.; Masters, J.; Cowburn, P.J. Multidisciplinary team approach to heart failure management. Heart 2018, 104, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Jaarsma, T. Inter-professional team approach to patients with heart failure. Heart 2005, 91, 832–838. [Google Scholar] [CrossRef] [Green Version]
- McAlister, F.A.; Stewart, S.; Ferrua, S.; McMurray, J.J.J.V. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: A systematic review of randomized trials. J. Am. Coll. Cardiol. 2004, 44, 810–819. [Google Scholar]
- Gattis, W.A.; Hasselblad, V.; Whellan, D.J.; O’Connor, C.M. Reduction in heart failure events by the addition of a clinical pharmacist to the heart failure management team: Results of the Pharmacist in Heart Failure Assessment Recommendation and Monitoring (PHARM) Study. Arch. Intern. Med. 1999, 159, 1939–1945. [Google Scholar] [CrossRef] [Green Version]
- Davidson, P.M.; Newton, P.J.; Tankumpuan, T.; Paull, G.; Dennison-Himmelfarb, C. Multidisciplinary management of chronic heart failure: Principles and future trends. Clin. Ther. 2015, 37, 2225–2233. [Google Scholar] [CrossRef] [PubMed]
- Chava, R.; Karki, N.; Ketlogetswe, K.; Ayala, T. Multidisciplinary rounds in prevention of 30-day readmissions and decreasing length of stay in heart failure patients: A community hospital based retrospective study. Medicine 2019, 98, e16233. [Google Scholar] [CrossRef] [PubMed]
- Fanari, Z.; Barekatain, A.; Kerzner, R.; Hammami, S.; Weintraub, W.S.; Maheshwari, V. Impact of a multidisciplinary team approach including an intensivist on the outcomes of critically ill patients in the cardiac care unit. Mayo Clin. Proc. 2016, 91, 1727–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused update of the 2013 ACCF/AHA Guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [PubMed]
- Moonsamy, P.; Axtell, A.L.; Ibrahim, N.E.; Funamoto, M.; Tolis, G.; Lewis, G.D.; D’Alessandro, D.A.; Villavicencio, M.A. Survival after heart transplantation in patients bridged with mechanical circulatory support. J. Am. Coll. Cardiol. 2020, 75, 2892–2905. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, S.; Takeda, K.; Kurlansky, P.A.; Naka, Y.; Takayama, H. Extracorporeal membrane oxygenation as a direct bridge to heart transplantation in adults. J. Thorac. Cardiovasc. Surg. 2018, 155, 1607–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutance, G.; Jacob, N.; Demondion, P.; Nguyen, L.S.; Bouglé, A.; Bréchot, N.; Varnous, S.; Leprince, P.; Combes, A.; Lebreton, G. Favorable outcomes of a direct heart transplantation strategy in selected patients on extracorporeal membrane oxygenation support. Crit. Care Med. 2020, 48, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Rousse, N.; Juthier, F.; Pinçon, C.; Hysi, I.; Banfi, C.; Robin, E.; Fayad, G.; Jegou, B.; Prat, A.; Vincentelli, A. ECMO as a bridge to decision: Recovery, VAD, or heart transplantation? Int. J. Cardiol. 2015, 187, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Robins, J.M.; Hernán, M.Á.; Brumback, B. Marginal structural models and causal inference in epidemiology. Epidemiology 2000, 11, 550–560. [Google Scholar] [CrossRef]
- Roussel, M.G.; Gorham, N.; Wilson, L.; Mangi, A.A. Improving recovery time following heart transplantation: The role of the multidisciplinary health care team. J. Multidiscip. Healthc. 2013, 6, 293–302. [Google Scholar] [PubMed] [Green Version]
- Na, S.J.; Chung, C.R.; Jeon, K.; Park, C.M.; Suh, G.Y.; Ahn, J.H.; Carriere, K.C.; Song, Y.B.; Choi, J.O.; Hahn, J.Y.; et al. Association between presence of a cardiac intensivist and mortality in an adult cardiac care unit. J. Am. Coll. Cardiol. 2016, 68, 2637–2648. [Google Scholar] [CrossRef]
- Hong, D.; Choi, K.H.; Cho, Y.H.; Cho, S.H.; Park, S.J.; Kim, D.; Park, T.K.; Lee, J.M.; Song, Y.B.; Choi, J.O.; et al. Multidisciplinary team approach in acute myocardial infarction patients undergoing veno-arterial extracorporeal membrane oxygenation. Ann. Intensive Care 2020, 10, 83. [Google Scholar] [CrossRef] [PubMed]
- Na, S.J.; Chung, C.R.; Choi, H.J.; Cho, Y.H.; Sung, K.; Yang, J.H.; Suh, G.Y.; Jeon, K. The effect of multidisciplinary extracorporeal membrane oxygenation team on clinical outcomes in patients with severe acute respiratory failure. Ann. Intensive Care 2018, 8, 31. [Google Scholar] [CrossRef] [PubMed]
| Overall Cohort | IPTW | ||||||
|---|---|---|---|---|---|---|---|
| Total (n = 250) | Non-MDT (n = 120) | MDT (n = 130) | p Value | Standardized Difference | p Value | Standardized Difference | |
| Age of recipient (years) | 54.0 (43.8–61.0) | 52.5 (40.3–61.0) | 55.0 (45.0–61.0) | 0.121 | 0.217 | 0.312 | 0.060 |
| Female recipients | 77 (30.8) | 41 (34.2) | 36 (27.7) | 0.268 | −0.140 | <0.001 | −0.559 |
| Age of donor (years) | 43.0 (34.0–50.0) | 41.0 (34.0–48.0) | 44.5 (33.8–51.3) | 0.012 | 0.271 | 0.146 | 0.235 |
| Female donors | 64 (25.6) | 31 (25.8) | 33 (25.4) | 0.935 | −0.010 | <0.001 | −0.449 |
| Gender mismatch | 81 (32.4) | 38 (31.7) | 43 (33.1) | 0.812 | 0.030 | 0.204 | 0.109 |
| Same ABO type matching | 191 (78.3) | 90 (78.9) | 101 (77.7) | 0.812 | −0.031 | 0.242 | −0.100 |
| Hypertension | 88 (35.2) | 43 (35.8) | 45 (34.6) | 0.840 | −0.026 | <0.001 | −0.399 |
| Diabetes | 56 (22.4) | 20 (16.7) | 36 (27.7) | 0.037 | 0.268 | 0.160 | 0.120 |
| Stroke | 21 (8.4) | 11 (9.2) | 10 (7.7) | 0.675 | −0.053 | 0.618 | 0.043 |
| Previous cardiac surgery | 52 (20.8) | 23 (19.2) | 29 (22.3) | 0.541 | 0.078 | <0.001 | 0.331 |
| LVAD | 14 (5.6) | 4 (3.3) | 10 (7.7) | 0.134 | 0.192 | 0.179 | 0.114 |
| Dialysis | 38 (15.3) | 16 (13.3) | 22 (17.2) | 0.400 | 0.107 | 0.006 | 0.235 |
| CRRT | 30 (12.1) | 9 (7.5) | 21 (16.4) | 0.032 | 0.277 | 0.091 | 0.144 |
| History of PCI | 43 (17.2) | 14 (11.7) | 29 (22.3) | 0.026 | 0.286 | 0.238 | 0.101 |
| LVEF (%) | 21.0 (17.0–27.0) | 21.5 (17.0–27.8) | 21.0 (17.0–27.0) | 0.613 | −0.122 | 0.953 | 0.088 |
| HFpEF | 28 (11.2) | 16 (13.3) | 12 (9.2) | 0.304 | −0.130 | 0.007 | 0.230 |
| ICMP | 56 (22.4) | 21 (17.5) | 35 (26.9) | 0.074 | 0.228 | 0.032 | 0.183 |
| SOFA score | 7.0 (4.0–11.0) | 6.0 (4.0–10.0) | 8.0 (5.0–12.0) | 0.052 | 0.244 | 0.087 | 0.258 |
| Waiting period for HTx (days) | 49.0 (18.0–124.5) | 36.0 (14.3–80.8) | 72.5 (22.0–167.0) | 0.002 | 0.300 | 0.683 | −0.449 |
| Pre-HTx ECLS | 92 (36.8) | 28 (23.3) | 64 (49.2) | <0.001 | 0.559 | 0.006 | 0.234 |
| Pre-HTx ECLS duration (days) | 10.0 (6.0–17.0) | 8.0 (2.0–14.5) | 11.0 (7.0–18.8) | 0.050 | 0.394 | 0.101 | 0.270 |
| Hemoglobin (g/dL) | 10.8 (9.6–12.5) | 11.3 (9.7–12.9) | 10.5 (9.4–12.1) | 0.019 | −0.308 | 0.044 | −0.324 |
| Platelet count(×103/mm3) | 149.0 (100.0–214.0) | 158.0 (111.0–216.3) | 143.0 (93.3–214.0) | 0.157 | −0.203 | 0.265 | −0.166 |
| Creatinine (mg/dL) | 1.1 (0.9–1.5) | 1.2 (0.9–1.5) | 1.1 (0.9–1.5) | 0.381 | 0.093 | 0.504 | 0.205 |
| Total bilirubin (mg/dL) | 1.7 (0.9–2.9) | 1.6 (0.9–3.0) | 1.7 (0.8–2.8) | 0.879 | 0.120 | 0.185 | 0.106 |
| Albumin (g/dL) | 3.6 (3.1–4.1) | 3.6 (3.0–4.2) | 3.6 (3.1–4.1) | 0.836 | 0.007 | 0.349 | −0.181 |
| NT-proBNP (pg/mL) | 8058.0 (3799.5–18,433.5) | 7792.0 (3813.0–21,543.0) | 8105.0 (3742.8–16,024.8) | 0.640 | −0.149 | 0.105 | −0.137 |
| Total (n = 250) | Non-MDT (n = 120) | MDT (n = 130) | p Value | |
|---|---|---|---|---|
| CPB time (minutes) | 147.0 (126.0–177.0) | 159.0 (135.0–190.5) | 139.0 (121.0–161.0) | <0.001 |
| ACC time (minutes) | 86.0 (68.0–105.0) | 97.0 (86.0–112.0) | 70.0 (60.0–87.0) | <0.001 |
| Total ischemic time (minutes) | 181.0 (147.0–235.0) | 173.0 (143.0–237.0) | 187.0 (150.0–235.0) | 0.383 |
| Cold ischemic time (minutes) | 116.0 (82.0–169.0) | 100.0 (70.0–163.0) | 120.0 (96.0–174.0) | 0.003 |
| Warm ischemic time (minutes) | 65.0 (54.0–76.0) | 70.0 (63.0–82.0) | 56.0 (47.0–68.0) | <0.001 |
| Post-HTx ECLS | 30 (12.0) | 12 (10.0) | 18 (13.8) | 0.350 |
| Post-HTx new ECLS | 8 (5.1) | 2 (2.2) | 6 (9.1) | 0.069 |
| Post-HTx ICU stay (days) | 10.0 (6.0–16.0) | 7.0 (5.0–14.0) | 12.0 (8.0–20.0) | <0.001 |
| Total ICU stay (days) | 14.0 (7.0–28.3) | 10.5 (5.3–21.8) | 17.0 (9.0–35.0) | <0.001 |
| Post-HTx hospital stay (days) | 30.0 (23.0–50.0) | 30.5 (24.0–41.0) | 30.0 (22.0–59.3) | 0.993 |
| Outcomes | p Value | Hazard Ratio | 95% Confidence Interval | |
|---|---|---|---|---|
| Lower 0.95 | Upper 0.95 | |||
| Overall Mortality | ||||
| Crude | 0.014 | 0.486 | 0.274 | 0.863 |
| IPTW | 0.002 | 0.506 | 0.327 | 0.783 |
| IPTW + multivariable * | <0.001 | 0.396 | 0.253 | 0.621 |
| 1-year mortality | ||||
| Crude | 0.044 | 0.485 | 0.240 | 0.981 |
| IPTW | 0.007 | 0.487 | 0.290 | 0.817 |
| IPTW + multivariable * | 0.001 | 0.403 | 0.237 | 0.687 |
| 3-year mortality | ||||
| Crude | 0.024 | 0.513 | 0.287 | 0.918 |
| IPTW | 0.007 | 0.542 | 0.348 | 0.843 |
| IPTW + multivariable * | 0.001 | 0.457 | 0.290 | 0.721 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.H.; Kim, J.Y.; Park, I.; Sung, K.; Kim, W.S.; Kim, D.; Yang, J.H.; Jeon, E.-S.; Choi, J.-O.; Choi, N.; et al. Favorable Impact of a Multidisciplinary Team Approach on Heart Transplantation Outcomes in a Mid-Volume Center. J. Clin. Med. 2022, 11, 2296. https://doi.org/10.3390/jcm11092296
Lee JH, Kim JY, Park I, Sung K, Kim WS, Kim D, Yang JH, Jeon E-S, Choi J-O, Choi N, et al. Favorable Impact of a Multidisciplinary Team Approach on Heart Transplantation Outcomes in a Mid-Volume Center. Journal of Clinical Medicine. 2022; 11(9):2296. https://doi.org/10.3390/jcm11092296
Chicago/Turabian StyleLee, Jun Ho, Joo Yeon Kim, Ilkun Park, Kiick Sung, Wook Sung Kim, Darae Kim, Jeong Hoon Yang, Eun-Seok Jeon, Jin-Oh Choi, Nayeon Choi, and et al. 2022. "Favorable Impact of a Multidisciplinary Team Approach on Heart Transplantation Outcomes in a Mid-Volume Center" Journal of Clinical Medicine 11, no. 9: 2296. https://doi.org/10.3390/jcm11092296
APA StyleLee, J. H., Kim, J. Y., Park, I., Sung, K., Kim, W. S., Kim, D., Yang, J. H., Jeon, E.-S., Choi, J.-O., Choi, N., Hong, H., & Cho, Y. H. (2022). Favorable Impact of a Multidisciplinary Team Approach on Heart Transplantation Outcomes in a Mid-Volume Center. Journal of Clinical Medicine, 11(9), 2296. https://doi.org/10.3390/jcm11092296