
Positive Effect of a New Combination of Antioxidants and Natural Hormone Stimulants for the Treatment of Oligoasthenoteratozoospermia


 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients Recruitment
2.2. Semen Analysis
2.3. Assisted Reproduction Techniques
2.4. Statistical Analysis
3. Results
3.1. Effect on Hormone and Metabolic Profile
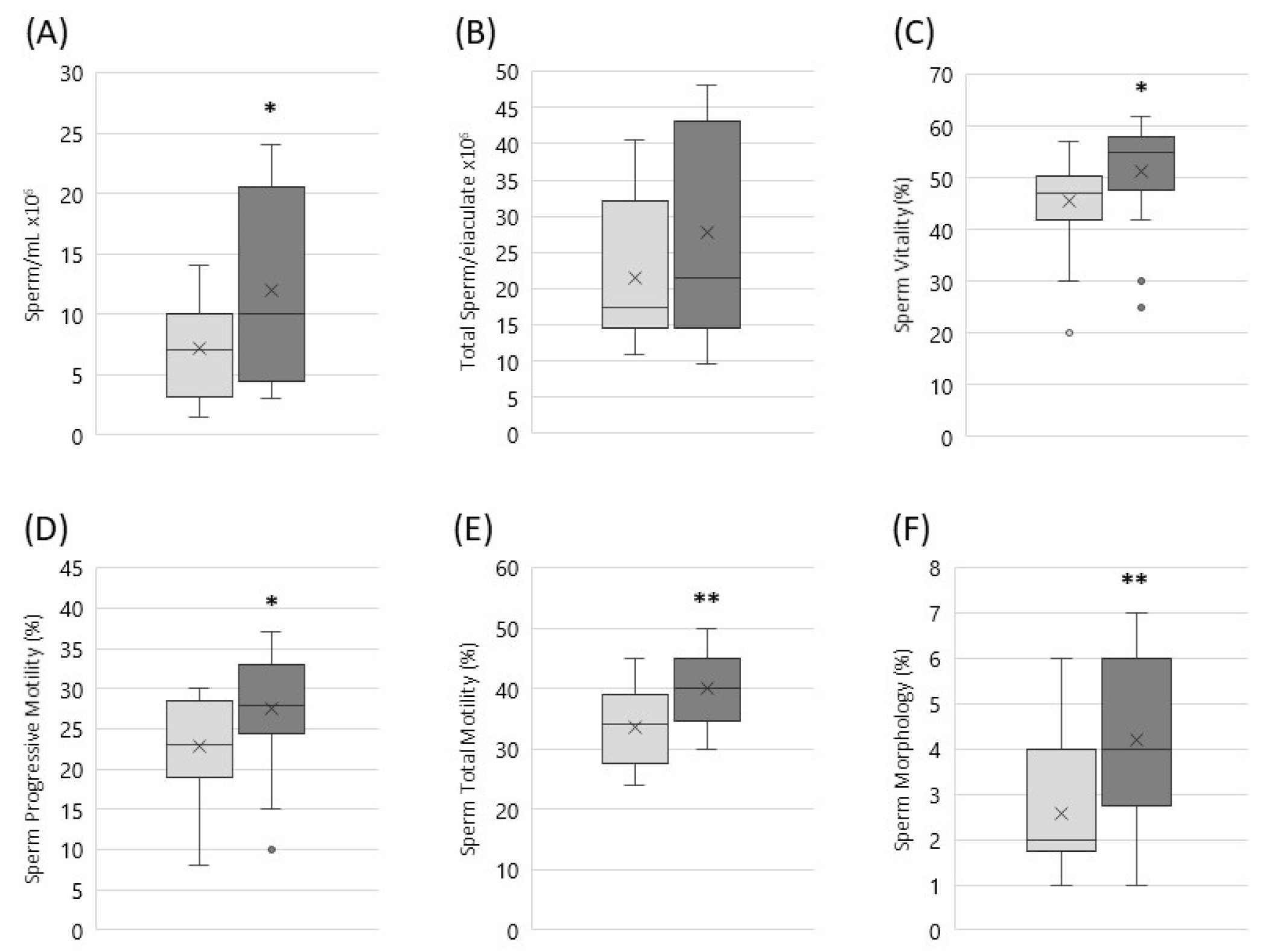
3.2. Effect on Sperm Parameters
3.3. Reproductive Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hamada, A.; Esteves, S.C.; Agarwal, A. Unexplained Male Infertility: Potential Causes and Management. Hum. Androl. 2011, 1, 2–16. [Google Scholar] [CrossRef] [Green Version]
- Rouchou, B. Consequences of Infertility in Developing Countries. Perspect. Public Health 2013, 133, 174–179. [Google Scholar] [CrossRef]
- Vine, M.F. Smoking and Male Reproduction: A Review. Int. J. Androl. 1996, 19, 323–337. [Google Scholar] [CrossRef]
- Auger, J.; Eustache, F.; Andersen, A.G.; Irvine, D.S.; Jørgensen, N.; Skakkebaek, N.E.; Suominen, J.; Toppari, J.; Vierula, M.; Jouannet, P. Sperm Morphological Defects Related to Environment, Lifestyle and Medical History of 1001 Male Partners of Pregnant Women from Four European Cities. Hum. Reprod. 2001, 16, 2710–2717. [Google Scholar] [CrossRef] [Green Version]
- Silva, T.; Jesus, M.; Cagigal, C.; Silva, C. Food with Influence in the Sexual and Reproductive Health. Curr. Pharm. Biotechnol. 2019, 20, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Majzoub, A. Role of Antioxidants in Assisted Reproductive Techniques. World J. Men’s Health 2017, 35, 77–93. [Google Scholar] [CrossRef]
- Baker, H.W.; Brindle, J.; Irvine, D.S.; Aitken, R.J. Protective Effect of Antioxidants on the Impairment of Sperm Motility by Activated Polymorphonuclear Leukocytes. Fertil. Steril. 1996, 65, 411–419. [Google Scholar] [CrossRef]
- Sabeti, P.; Pourmasumi, S.; Rahiminia, T.; Akyash, F.; Talebi, A.R. Etiologies of Sperm Oxidative Stress. Int. J. Reprod. Biomed. 2016, 14, 231–240. [Google Scholar] [CrossRef]
- Henkel, R.R. Leukocytes and Oxidative Stress: Dilemma for Sperm Function and Male Fertility. Asian J. Androl. 2011, 13, 43–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eskenazi, B.; Kidd, S.A.; Marks, A.R.; Sloter, E.; Block, G.; Wyrobek, A.J. Antioxidant Intake Is Associated with Semen Quality in Healthy Men. Hum. Reprod. 2005, 20, 1006–1012. [Google Scholar] [CrossRef] [Green Version]
- Garolla, A.; Petre, G.C.; Francini-Pesenti, F.; De Toni, L.; Vitagliano, A.; Di Nisio, A.; Foresta, C. Dietary Supplements for Male Infertility: A Critical Evaluation of Their Composition. Nutrients 2020, 12, 1472. [Google Scholar] [CrossRef]
- Buhling, K.J.; Laakmann, E. The Effect of Micronutrient Supplements on Male Fertility. Curr. Opin. Obstet. Gynecol. 2014, 26, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, S. Male Infertility: Nutritional and Environmental Considerations. Altern. Med. Rev. 2000, 5, 28–38. [Google Scholar]
- Dinicola, S.; Unfer, V.; Facchinetti, F.; Soulage, C.O.; Greene, N.D.; Bizzarri, M.; Laganà, A.S.; Chan, S.-Y.; Bevilacqua, A.; Pkhaladze, L.; et al. Inositols: From Established Knowledge to Novel Approaches. Int. J. Mol. Sci. 2021, 22, 10575. [Google Scholar] [CrossRef]
- Governini, L.; Ponchia, R.; Artini, P.G.; Casarosa, E.; Marzi, I.; Capaldo, A.; Luddi, A.; Piomboni, P. Respiratory Mitochondrial Efficiency and DNA Oxidation in Human Sperm after In Vitro Myo-Inositol Treatment. J. Clin. Med. 2020, 9, 1638. [Google Scholar] [CrossRef]
- Ponchia, R.; Bruno, A.; Renzi, A.; Landi, C.; Shaba, E.; Luongo, F.P.; Haxhiu, A.; Artini, P.G.; Luddi, A.; Governini, L.; et al. Oxidative Stress Measurement in Frozen/Thawed Human Sperm: The Protective Role of an In Vitro Treatment with Myo-Inositol. Antioxidants 2021, 11, 10. [Google Scholar] [CrossRef]
- Appleton, J. Arginine: Clinical Potential of a Semi-Essential Amino Acid. Altern. Med. Rev. 2002, 7, 512–522. [Google Scholar]
- Rolf, C.; Cooper, T.G.; Yeung, C.H.; Nieschlag, E. Antioxidant Treatment of Patients with Asthenozoospermia or Moderate Oligoasthenozoospermia with High-Dose Vitamin C and Vitamin E: A Randomized, Placebo-Controlled, Double-Blind Study. Hum. Reprod. 1999, 14, 1028–1033. [Google Scholar] [CrossRef] [Green Version]
- Sabetian, S.; Jahromi, B.N.; Vakili, S.; Forouhari, S.; Alipour, S. The Effect of Oral Vitamin E on Semen Parameters and IVF Outcome: A Double-Blinded Randomized Placebo-Controlled Clinical Trial. BioMed Res. Int. 2021, 2021, 5588275. [Google Scholar] [CrossRef]
- Mortazavi, M.; Salehi, I.; Alizadeh, Z.; Vahabian, M.; Roushandeh, A.M. Protective Effects of Antioxidants on Sperm Parameters and Seminiferous Tubules Epithelium in High Fat-Fed Rats. J. Reprod. Infertil. 2014, 15, 22–28. [Google Scholar]
- Fraga, C.G.; Motchnik, P.A.; Shigenaga, M.K.; Helbock, H.J.; Jacob, R.A.; Ames, B.N. Ascorbic Acid Protects against Endogenous Oxidative DNA Damage in Human Sperm. Proc. Natl. Acad. Sci. USA 1991, 88, 11003–11006. [Google Scholar] [CrossRef] [Green Version]
- Jacob, R.A.; Pianalto, F.S.; Agee, R.E. Cellular Ascorbate Depletion in Healthy Men. J. Nutr. 1992, 122, 1111–1118. [Google Scholar] [CrossRef]
- Ahmadi, S.; Bashiri, R.; Ghadiri-Anari, A.; Nadjarzadeh, A. Antioxidant Supplements and Semen Parameters: An Evidence Based Review. Int. J. Reprod. Biomed. 2016, 14, 729–736. [Google Scholar] [CrossRef]
- Akmal, M.; Qadri, J.Q.; Al-Waili, N.S.; Thangal, S.; Haq, A.; Saloom, K.Y. Improvement in Human Semen Quality after Oral Supplementation of Vitamin C. J. Med. Food 2006, 9, 440–442. [Google Scholar] [CrossRef] [PubMed]
- Blomberg Jensen, M. Vitamin D and Male Reproduction. Nat. Rev. Endocrinol. 2014, 10, 175–186. [Google Scholar] [CrossRef]
- Alahmar, A.T.; Singh, R. Comparison of the Effects of Coenzyme Q10 and Centrum Multivitamins on Semen Parameters, Oxidative Stress Markers, and Sperm DNA Fragmentation in Infertile Men with Idiopathic Oligoasthenospermia. Clin. Exp. Reprod. Med. 2022, 49, 49–56. [Google Scholar] [CrossRef]
- Sharma, A.P.; Sharma, G.; Kumar, R. Systematic Review and Meta-Analysis on Effect of Carnitine, Coenzyme Q10 and Selenium on Pregnancy and Semen Parameters in Couples with Idiopathic Male Infertility. Urology 2021, 161, 4–11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (Ed.) WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; World Health Organization: Geneva, Switzerland, 2010; ISBN 978-92-4-154778-9. [Google Scholar]
- Calogero, A.E.; Aversa, A.; La Vignera, S.; Corona, G.; Ferlin, A. The Use of Nutraceuticals in Male Sexual and Reproductive Disturbances: Position Statement from the Italian Society of Andrology and Sexual Medicine (SIAMS). J. Endocrinol. Investig. 2017, 40, 1389–1397. [Google Scholar] [CrossRef]
- Duca, Y.; Calogero, A.E.; Cannarella, R.; Condorelli, R.A.; La Vignera, S. Current and Emerging Medical Therapeutic Agents for Idiopathic Male Infertility. Expert Opin. Pharmacother. 2019, 20, 55–67. [Google Scholar] [CrossRef]
- Smits, R.M.; Mackenzie-Proctor, R.; Yazdani, A.; Stankiewicz, M.T.; Jordan, V.; Showell, M.G. Antioxidants for Male Subfertility. Cochrane Database Syst. Rev. 2019, CD007411. [Google Scholar] [CrossRef] [PubMed]
- Amorini, A.M.; Listorti, I.; Bilotta, G.; Pallisco, R.; Saab, M.W.; Mangione, R.; Manca, B.; Lazzarino, G.; Tavazzi, B.; Lazzarino, G.; et al. Antioxidant-Based Therapies in Male Infertility: Do We Have Sufficient Evidence Supporting Their Effectiveness? Antioxidants 2021, 10, 220. [Google Scholar] [CrossRef]
- Agarwal, A.; Sekhon, L.H. The Role of Antioxidant Therapy in the Treatment of Male Infertility. Hum. Fertil. 2010, 13, 217–225. [Google Scholar] [CrossRef]
- Majzoub, A.; Agarwal, A. Antioxidant Therapy in Idiopathic Oligoasthenoteratozoospermia. Indian J. Urol. 2017, 33, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Helli, B.; Kavianpour, M.; Ghaedi, E.; Dadfar, M.; Haghighian, H.K. Probiotic Effects on Sperm Parameters, Oxidative Stress Index, Inflammatory Factors and Sex Hormones in Infertile Men. Hum. Fertil. 2020, 1–9. [Google Scholar] [CrossRef]
- Lanzafame, F.M.; La Vignera, S.; Vicari, E.; Calogero, A.E. Oxidative Stress and Medical Antioxidant Treatment in Male Infertility. Reprod. Biomed. Online 2009, 19, 638–659. [Google Scholar] [CrossRef] [Green Version]
- Aitken, R.J.; Drevet, J.R.; Moazamian, A.; Gharagozloo, P. Male Infertility and Oxidative Stress: A Focus on the Underlying Mechanisms. Antioxidants 2022, 11, 306. [Google Scholar] [CrossRef] [PubMed]
- Symeonidis, E.N.; Evgeni, E.; Palapelas, V.; Koumasi, D.; Pyrgidis, N.; Sokolakis, I.; Hatzichristodoulou, G.; Tsiampali, C.; Mykoniatis, I.; Zachariou, A.; et al. Redox Balance in Male Infertility: Excellence through Moderation-“Μέτρον ἄριστον”. Antioxidants 2021, 10, 1534. [Google Scholar] [CrossRef]
- Blomberg Jensen, M.; Lawaetz, J.G.; Petersen, J.H.; Juul, A.; Jørgensen, N. Effects of Vitamin D Supplementation on Semen Quality, Reproductive Hormones, and Live Birth Rate: A Randomized Clinical Trial. J. Clin. Endocrinol. Metab. 2018, 103, 870–881. [Google Scholar] [CrossRef] [PubMed]
- Maghsoumi-Norouzabad, L.; Zare Javid, A.; Mansoori, A.; Dadfar, M.; Serajian, A. The Effects of Vitamin D3 Supplementation on Spermatogram and Endocrine Factors in Asthenozoospermia Infertile Men: A Randomized, Triple Blind, Placebo-Controlled Clinical Trial. Reprod. Biol. Endocrinol. 2021, 19, 102. [Google Scholar] [CrossRef]
- Mongioi, L.; Calogero, A.E.; Vicari, E.; Condorelli, R.A.; Russo, G.I.; Privitera, S.; Morgia, G.; La Vignera, S. The Role of Carnitine in Male Infertility. Andrology 2016, 4, 800–807. [Google Scholar] [CrossRef]
- Condorelli, R.A.; Barbagallo, F.; Calogero, A.E.; Cannarella, R.; Crafa, A.; La Vignera, S. D-Chiro-Inositol Improves Sperm Mitochondrial Membrane Potential: In Vitro Evidence. J. Clin. Med. 2020, 9, 1373. [Google Scholar] [CrossRef]


{kind=link}
| Nutraceutical Composition | Per 1 Packet | NRV |
|---|---|---|
| Inositol | 1000 mg | - |
| L-Carnitine | 250 mg | - |
| Acetyl L-Carnitine Hydrochloride | 250 mg | - |
| Vitamin E | 60 mg | 500% |
| Vitamin C | 100 mg | 125% |
| Vitamin D3 | 5 mcg | 100% |
| Coenzyme Q10 | 20 mg | - |
| Selenium | 50 mcg | 90.90% |
| Required Examination | T-1 | T0 Basal | T1 Post Treatment |
|---|---|---|---|
| Spermiogram | X | X | X |
| Hormonal panel | X | X | |
| Hemato-Metabolic panel | X | X |
| Test Parameters | T0 Basal | T1 Post Treatment | Reference Values |
|---|---|---|---|
| Testosterone (ng/mL) | 4.5 ± 1.6 | 5.2 ± 1.8 | 2.8–8.0 |
| FSH (mUI/mL) | 5.2 ± 1.3 | 4.8 ± 0.9 | 0.7–11.0 |
| LH (mUI/mL) | 6.1 ± 1.7 | 5.5 ± 0.6 | 0.8–8.0 |
| SHBG (nmol/mL) | 48.0 ± 12.0 | 55 ± 16 | 10.0–57.0 |
| Prolactin (ng/mL) | 11.2 ± 3.0 | 10.6 ± 2.0 | 2.0–13.0 |
| Estradiol (pg/mL) | 32.0 ± 6.0 | 25.0 ± 4.0 | <32.0 |
| Test Parameters | T0 Basal | T1 Post Treatment | Reference Values |
|---|---|---|---|
| Glucose (mg/dL) | 98 ± 7 | 91 ± 3 | 60–110 |
| Insulin (microU/mL) | 12.7 ± 4.2 | 9.3 ± 2.6 | 2.6–24.9 |
| Creatinine (mg/dL) | 0.88 ± 0.2 | 0.80 ± 0.3 | 0.55–1.40 |
| Total Cholesterol (mg/dL) | 218 ± 9 | 202 ± 5 | 140–220 |
| Triglycerides (mg/dL) | 160 ± 8 | 154 ± 7 | <200 |
| Oxaloacetic Transaminase(AST)(GOT) (U/L) | 24 ± 5 | 22 ± 6 | <30 |
| Pyruvic Transaminase(ALT)(GPT) (U/L) | 19 ± 3 | 18 ± 4 | <41 |
| C Reactive Protein (CRP) (mg/L) | 0.8 ± 0.3 | 0.7 ± 0.4 | 0.0–5.0 |
| Semen Parameters | T0 Basal | T1 Post Treatment | p Value |
|---|---|---|---|
| Concentration (×106/mL) | 7.13 ± 4.24 | 12.24 ± 7.83 | * |
| Total sperm count (×106/ejaculate) | 21.54 ± 10.15 | 27.70 ± 14.87 | ns |
| Vitality (%) | 45.4 ± 8.2 | 51.2 ± 9.5 | * |
| Progressive Motility (%) | 22.8 ± 5.9 | 27.5 ± 6.4 | * |
| Total motility (%) | 33.6 ± 5.5 | 40.2 ± 5.8 | ** |
| Morphology (%) | 2.6 ± 1.4 | 4.2 ± 1.9 | ** |
| Reproductive Outcomes | Group A | Group B | p Value |
|---|---|---|---|
| Male patient’s age (years) | 34.4 ± 6.8 | 35.2 ± 6.3 | ns |
| Female patient’age at pick-up (years) | 33.7 ± 2.5 | 34.1 ± 3.2 | ns |
| Number retrieved oocytes | 9.8 ± 3.5 | 9.2 ± 3.3 | ns |
| Number MII oocytes | 7.9 ± 2.7 | 7.5 ± 2.4 | ns |
| Fertilization rate (%) | 87.3 ± 15.7 | 74.3 ± 22.6 | * |
| Pregnancy rate (%) | 19.6 ± 3.7 | 17.2 ± 2.9 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Leo, V.; Tosti, C.; Morgante, G.; Ponchia, R.; Luddi, A.; Governini, L.; Piomboni, P. Positive Effect of a New Combination of Antioxidants and Natural Hormone Stimulants for the Treatment of Oligoasthenoteratozoospermia. J. Clin. Med. 2022, 11, 1991. https://doi.org/10.3390/jcm11071991
De Leo V, Tosti C, Morgante G, Ponchia R, Luddi A, Governini L, Piomboni P. Positive Effect of a New Combination of Antioxidants and Natural Hormone Stimulants for the Treatment of Oligoasthenoteratozoospermia. Journal of Clinical Medicine. 2022; 11(7):1991. https://doi.org/10.3390/jcm11071991
Chicago/Turabian StyleDe Leo, Vincenzo, Claudia Tosti, Giuseppe Morgante, Rosetta Ponchia, Alice Luddi, Laura Governini, and Paola Piomboni. 2022. "Positive Effect of a New Combination of Antioxidants and Natural Hormone Stimulants for the Treatment of Oligoasthenoteratozoospermia" Journal of Clinical Medicine 11, no. 7: 1991. https://doi.org/10.3390/jcm11071991
APA StyleDe Leo, V., Tosti, C., Morgante, G., Ponchia, R., Luddi, A., Governini, L., & Piomboni, P. (2022). Positive Effect of a New Combination of Antioxidants and Natural Hormone Stimulants for the Treatment of Oligoasthenoteratozoospermia. Journal of Clinical Medicine, 11(7), 1991. https://doi.org/10.3390/jcm11071991