
Early Treatment of Acute Myocardial Infarction with Melatonin: Effects on MMP-9 and Adverse Cardiac Events

 ,
,  , ,
, ,  , , and
, , and 
Abstract
:1. Introduction
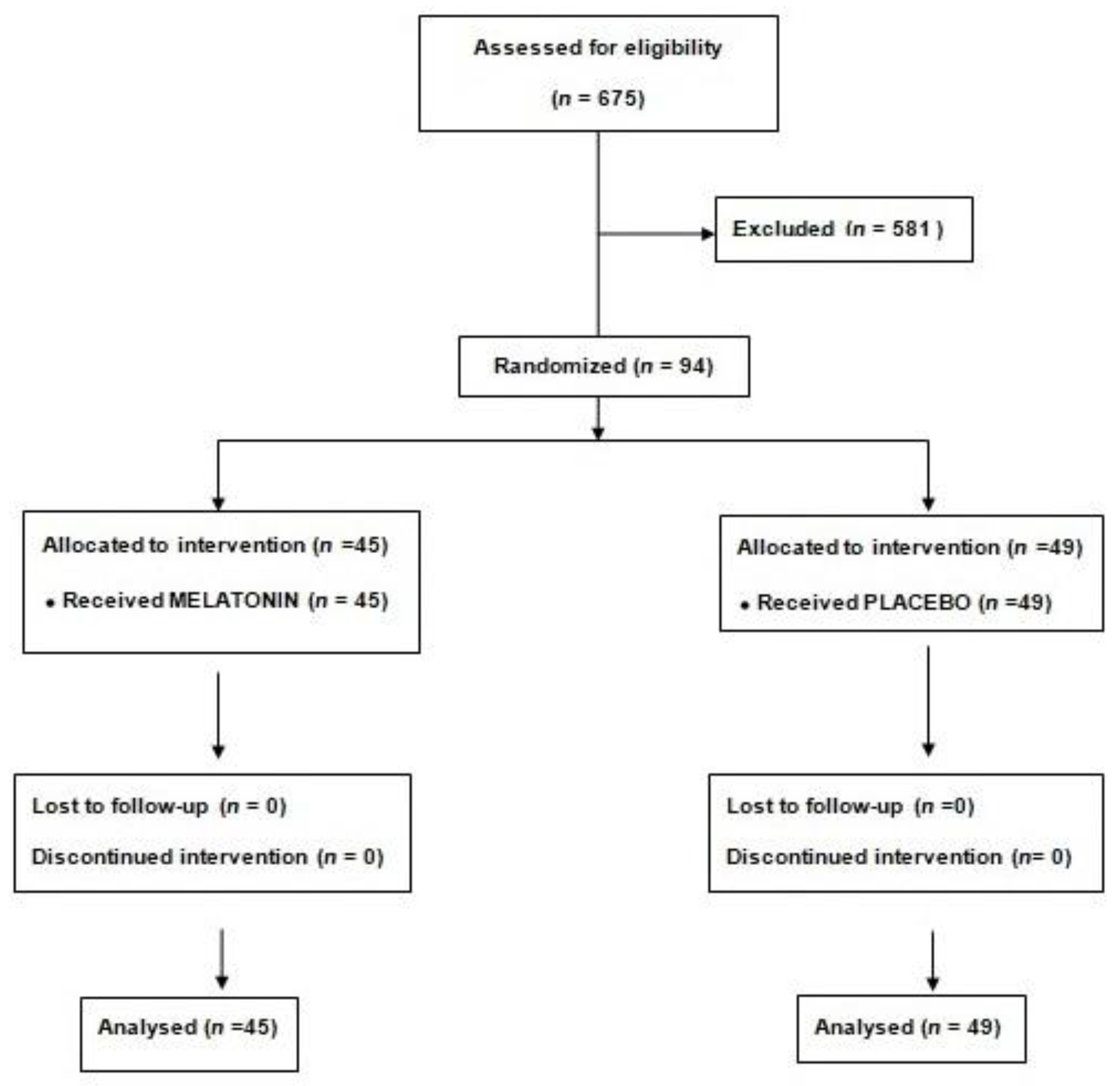
2. Methods
2.1. Study Population
2.2. Blood Sample Collection
2.3. End-Points
2.4. Statistical Analysis
3. Results
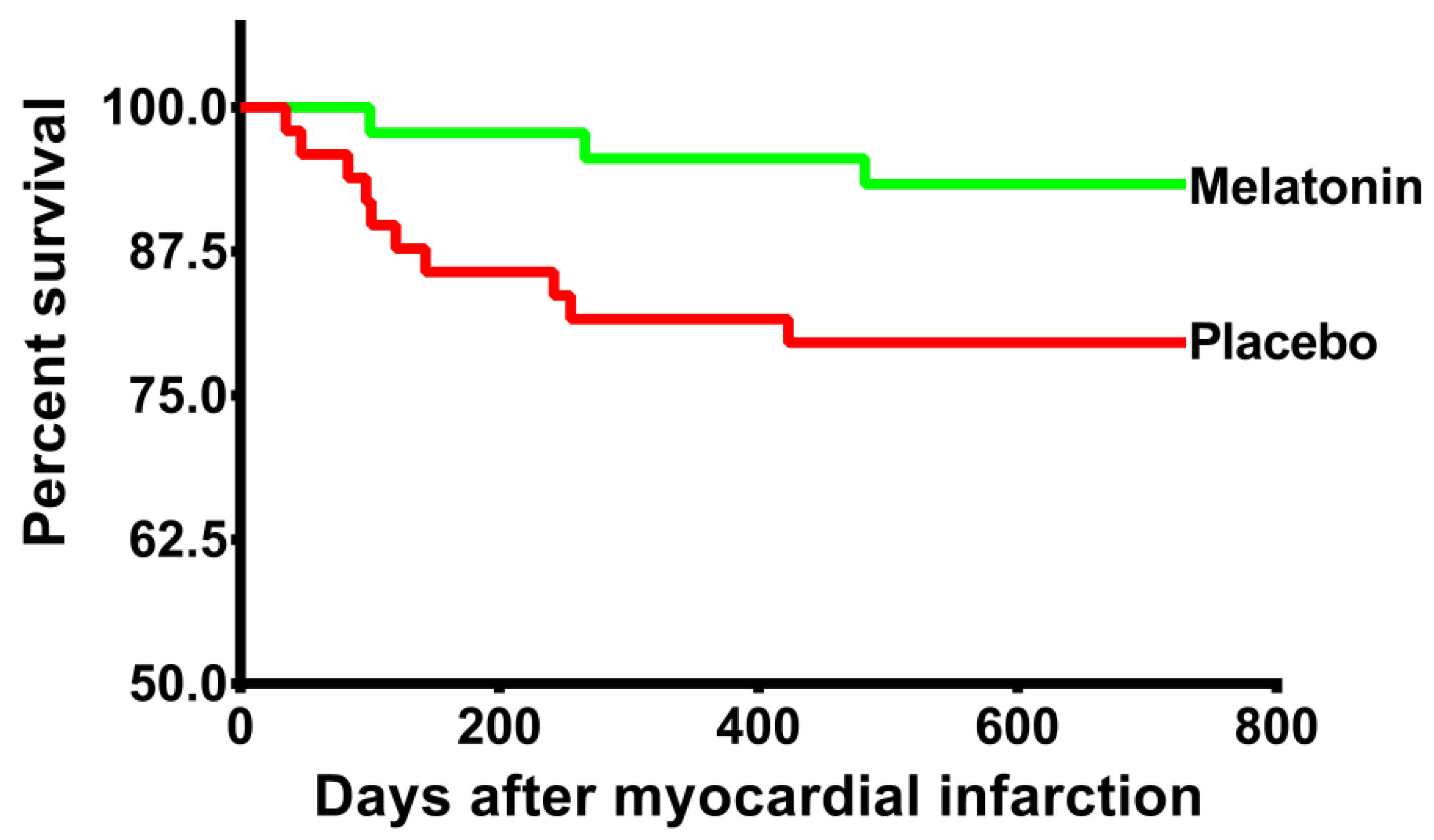
3.1. Primary End-Point
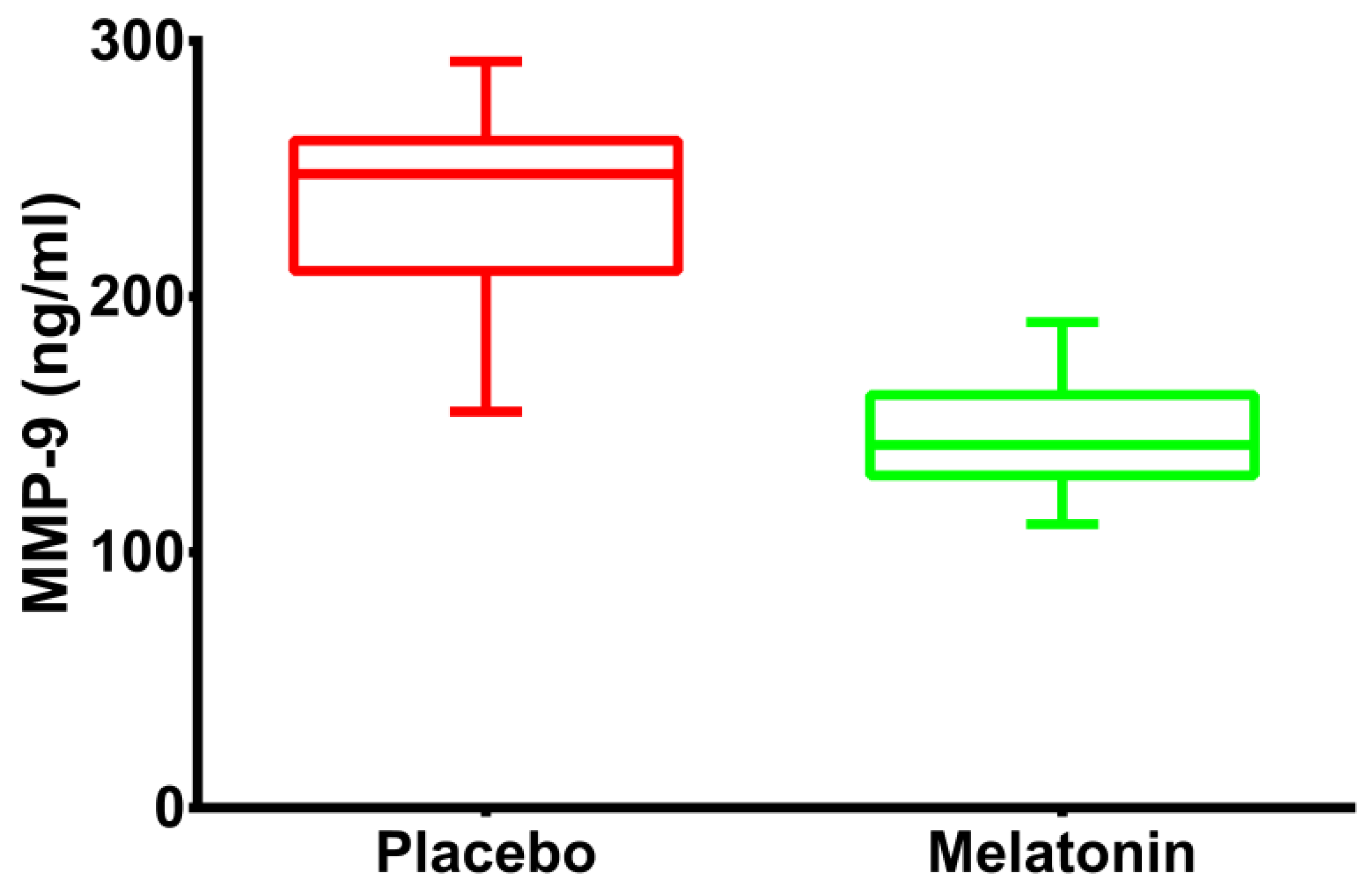
3.2. Secondary End-Point
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hausenloy, D.J.; Garcia-Dorado, D.; Bøtker, H.E.; Davidson, S.M.; Downey, J.; Engel, F.B.; Jennings, R.; Lecour, S.; Leor, J.; Madonna, R.; et al. Novel targets and future strategies for acute cardioprotection: Position Paper of the European Society of Cardiology Working Group on Cellular Biology of the Heart. Cardiovasc. Res. 2017, 113, 564–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausenloy, D.; Barrabés, J.A.; Bøtker, H.E.; Davidson, S.; Di Lisa, F.; Downey, J.; Engstrom, T.; Ferdinandy, P.; Carbrera-Fuentes, H.A.; Heusch, G.; et al. Ischaemic conditioning and targeting reperfusion injury: A 30 year voyage of discovery. Basic Res. Cardiol. 2016, 111, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob-Ferreira, A.L.; Schulz, R. Activation of intracellular matrix metalloproteinase-2 by reactive oxygen-nitrogen species: Consequences and therapeutic strategies in the heart. Arch. Biochem. Biophys. 2013, 540, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Rodriguez, A.; Abreu-Gonzalez, P.; Chen, Y.H. Cardioprotection and effects of melatonin administration on cardiac ischemia reperfusion: Insight from clinical studies. Melatonin Res. 2019, 2, 100–105. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; Abreu-Gonzalez, P.; Avanzas, P. The role of melatonin in acute myocardial infarction. Front. Biosci. 2012, 17, 2433–2441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dominguez-Rodriguez, A.; Abreu-Gonzalez, P.; Sanchez-Sanchez, J.J.; Kaski, J.C.; Reiter, R.J. Melatonin and circadian biology in human cardiovascular disease. J. Pineal Res. 2010, 49, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Mao, Z.J.; Lin, H.; Xiao, F.Y.; Huang, Z.Q.; Chen, Y.H. Melatonin against Myocardial Ischemia-Reperfusion Injury: A Meta-analysis and Mechanism Insight from Animal Studies. Oxid. Med. Cell. Longev. 2020, 2020, 1241065. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Rodriguez, A.; Abreu-Gonzalez, P.; de la Torre-Hernandez, J.M.; Consuegra-Sanchez, L.; Piccolo, R.; Gonzalez-Gonzalez, J.; Garcia-Camarero, T.; Del Mar Garcia-Saiz, M.; Aldea-Perona, A.; Reiter, R.J.; et al. Usefulness of Early Treatment With Melatonin to Reduce Infarct Size in Patients With ST-Segment Elevation Myocardial Infarction Receiving Percutaneous Coronary Intervention (From the Melatonin Adjunct in the Acute Myocardial Infarction Treated With Angioplasty Trial). Am. J. Cardiol. 2017, 120, 522–526. [Google Scholar] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [PubMed] [Green Version]
- Fujimoto, N.; Hosokawa, N.; Iwata, K.; Shinya, T.; Okada, Y.; Hayakawa, T. A one-step sandwich enzyme immunoassay for inactive precursor and complexed forms of human matrix metalloproteinase 9 (92 kDa gelatinase/type IV collagenase, gelatinase B) using monoclonal antibodies. Clin. Chim. Acta 1994, 231, 79–88. [Google Scholar] [CrossRef]
- Dominguez-Rodriguez, A.; Abreu-Gonzalez, P.; Garcia-Gonzalez, M.J.; Kaski, J.C. High serum matrix metalloproteinase-9 level predict increased risk of in-hospital cardiac events in patients with type 2 diabetes and ST segment elevation myocardial infarction. Atherosclerosis 2008, 196, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Uno, H.; Wei, L.J. Restricted Mean Survival Time as a Measure to Interpret Clinical Trial Results. JAMA Cardiol. 2017, 2, 1179–1180. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; Parmar, M.K. Restricted mean survival time: An alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med. Res. Methodol. 2013, 13, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalu, M.M.; Pasini, E.; Schulze, C.J.; Ferrari-Vivaldi, M.; Ferrari-Vivaldi, G.; Bachetti, T.; Schulz, R. Ischaemia-reperfusion injury activates matrix metalloproteinases in the human heart. Eur. Heart J. 2004, 26, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Lan, H.; Su, Y.; Liu, Y.; Deng, C.; Wang, J.; Chen, T.; Jules, K.E.D.; Masau, J.F.; Li, H.; Wei, X. Melatonin protects circulatory death heart from ischemia/reperfusion injury via the JAK2/STAT3 signalling pathway. Life Sci. 2019, 228, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Chitimus, D.M.; Popescu, M.R.; Voiculescu, S.E.; Panaitescu, A.M.; Pavel, B.; Zagrean, L.; Zagrean, A.-M. Melatonin’s Impact on Antioxidative and Anti-Inflammatory Reprogramming in Homeostasis and Disease. Biomolecules 2020, 10, 1211. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Rodríguez, A.; Abreu-González, P.; Báez-Ferrer, N.; Reiter, R.J.; Avanzas, P.; Hernández-Vaquero, D. Melatonin and Cardioprotection in Humans: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Cardiovasc. Med. 2021, 8, 635083. [Google Scholar] [CrossRef]
- Kunugi, S.; Shimizu, A.; Kuwahara, N.; Du, X.; Takahashi, M.; Terasaki, Y.; Fujita, E.; Mii, A.; Nagasaka, S.; Akimoto, T.; et al. Inhibition of matrix metalloproteinases reduces ischemia-reperfusion acute kidney injury. Lab. Investig. 2010, 91, 170–180. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Placebo (n = 49) | Melatonin (n = 45) | p-Value |
|---|---|---|---|
| Age (years) | 60.5 (54.9–69.7) | 60.4 (57–77.3) | 0.11 |
| Women; n (%) | 26 (53.1%) | 17 (37.8%) | 0.15 |
| Diabetes; n (%) | 7 (14.3%) | 4 (8.9%) | 0.53 |
| Hypertension; n (%) | 28 (57.1%) | 23 (51.1%) | 0.68 |
| Dyslipidemia; n (%) | 29 (59.2%) | 23 (51.1%) | 0.53 |
| Weight (kg) | 61.7 ± 8.9 | 67 ± 10 | 0.01 |
| Height (m) | 1.7 ± 0.1 | 1.7 ± 0.1 | 0.31 |
| Smoking habit; n (%) | 28 (57.1%) | 23 (51.1%) | 0.68 |
| Total cholesterol (mg/dL) | 174 (153–213) | 177 (153–208) | 0.87 |
| LDL cholesterol (mg/dL) | 104 (82–138) | 108 (86–136) | 0.94 |
| Hemoglobin (g/dL) | 13.5 (12–14.8) | 14.4 (13.1–15.2) | 0.049 |
| Cardiac characteristics | |||
| Infarction location | 0.7 | ||
| Anterior; n (%) | 23 (46.9%) | 18 (40%) | |
| Inferior; n (%) | 23 (46.9%) | 25 (55.6%) | |
| Lateral; n (%) | 3 (6.1%) | 2 (4.4%) | |
| Pain-to-reperfusion time (minutes) | 137.4 ± 18.4 | 134.6 ± 19.0 | 0.46 |
| Left ventricular ejection fraction (%) | 56.1 (50–60) | 57.5 (53.3–63.8) | 0.24 |
| Troponin I peak (pg/mL) | 204 (176–239) | 219 (188–277) | 0.23 |
| Number of diseased vessels | 0.03 | ||
| 1 vessel disease; n (%) | 30 (61.2%) | 36 (80%) | |
| 2 vessel disease; n (%) | 17 (34.7%) | 9 (20%) | |
| 3 vessel disease; n (%) | 2 (4.1%) | 0 (0%) | |
| Treatment at discharge | |||
| Antiplatelet drugs; n (%) | 49 (100%) | 45 (100%) | 1 |
| Angiotensin converting enzyme inhibitors; n (%) | 40 (81.6%) | 30 (66.7%) | 0.11 |
| Beta blockers; n (%) | 47 (95.9%) | 42 (93.3%) | 0.67 |
| Statins; n (%) | 49 (100%) | 45 (100%) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domínguez-Rodríguez, A.; Hernández-Vaquero, D.; Abreu-González, P.; Báez-Ferrer, N.; Díaz, R.; Avanzas, P.; Simko, F.; Domínguez-González, V.; Sharma, R.; Reiter, R.J. Early Treatment of Acute Myocardial Infarction with Melatonin: Effects on MMP-9 and Adverse Cardiac Events. J. Clin. Med. 2022, 11, 1909. https://doi.org/10.3390/jcm11071909
Domínguez-Rodríguez A, Hernández-Vaquero D, Abreu-González P, Báez-Ferrer N, Díaz R, Avanzas P, Simko F, Domínguez-González V, Sharma R, Reiter RJ. Early Treatment of Acute Myocardial Infarction with Melatonin: Effects on MMP-9 and Adverse Cardiac Events. Journal of Clinical Medicine. 2022; 11(7):1909. https://doi.org/10.3390/jcm11071909
Chicago/Turabian StyleDomínguez-Rodríguez, Alberto, Daniel Hernández-Vaquero, Pedro Abreu-González, Néstor Báez-Ferrer, Rocío Díaz, Pablo Avanzas, Fedor Simko, Virginia Domínguez-González, Ramaswamy Sharma, and Russel J. Reiter. 2022. "Early Treatment of Acute Myocardial Infarction with Melatonin: Effects on MMP-9 and Adverse Cardiac Events" Journal of Clinical Medicine 11, no. 7: 1909. https://doi.org/10.3390/jcm11071909
APA StyleDomínguez-Rodríguez, A., Hernández-Vaquero, D., Abreu-González, P., Báez-Ferrer, N., Díaz, R., Avanzas, P., Simko, F., Domínguez-González, V., Sharma, R., & Reiter, R. J. (2022). Early Treatment of Acute Myocardial Infarction with Melatonin: Effects on MMP-9 and Adverse Cardiac Events. Journal of Clinical Medicine, 11(7), 1909. https://doi.org/10.3390/jcm11071909