
Addressing Chemotherapy-Induced Peripheral Neuropathy Using Multi-Frequency Vibrometry and Patient-Reported Outcomes

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurements
2.2. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
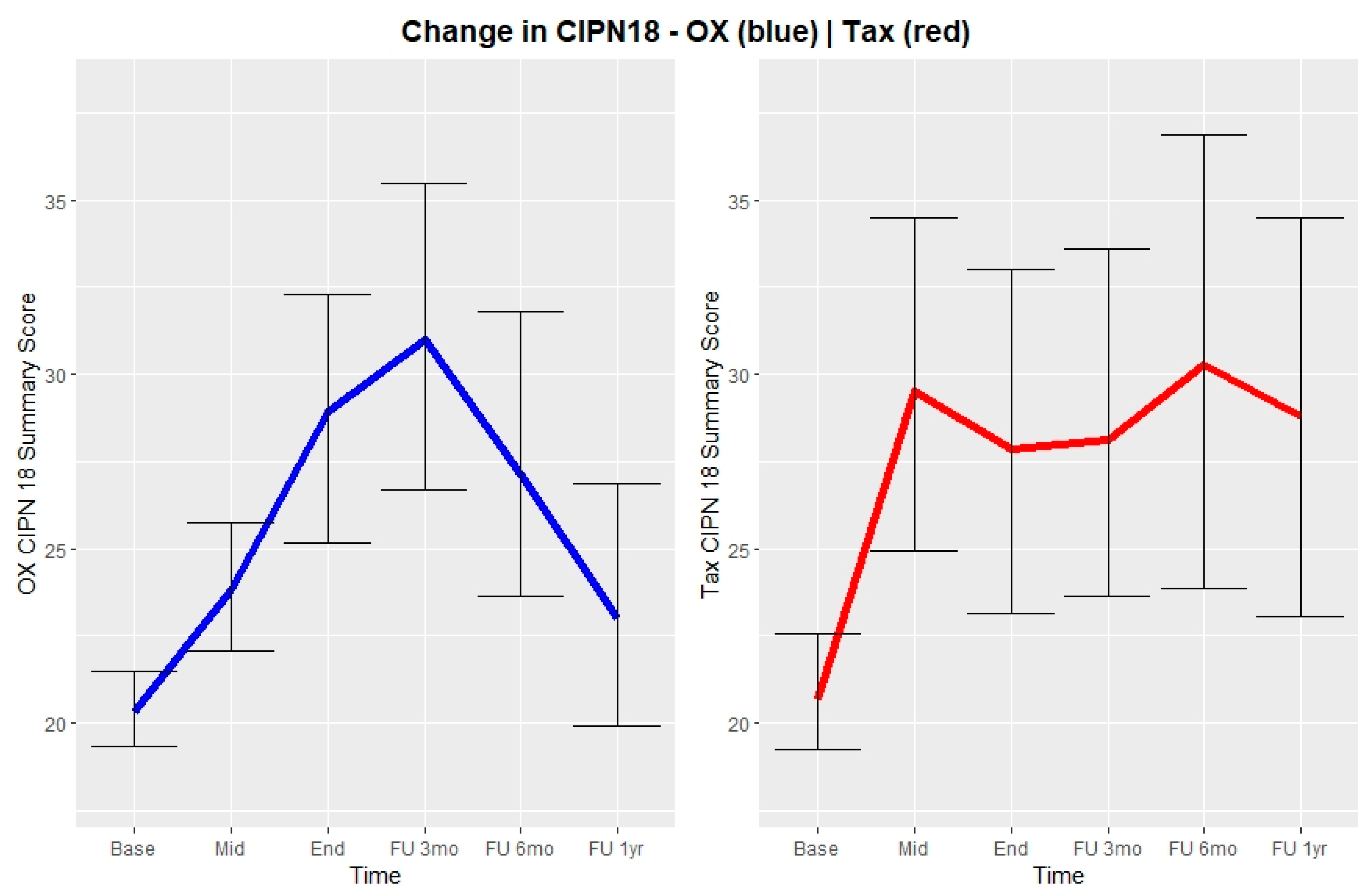
3.2. CIPN18
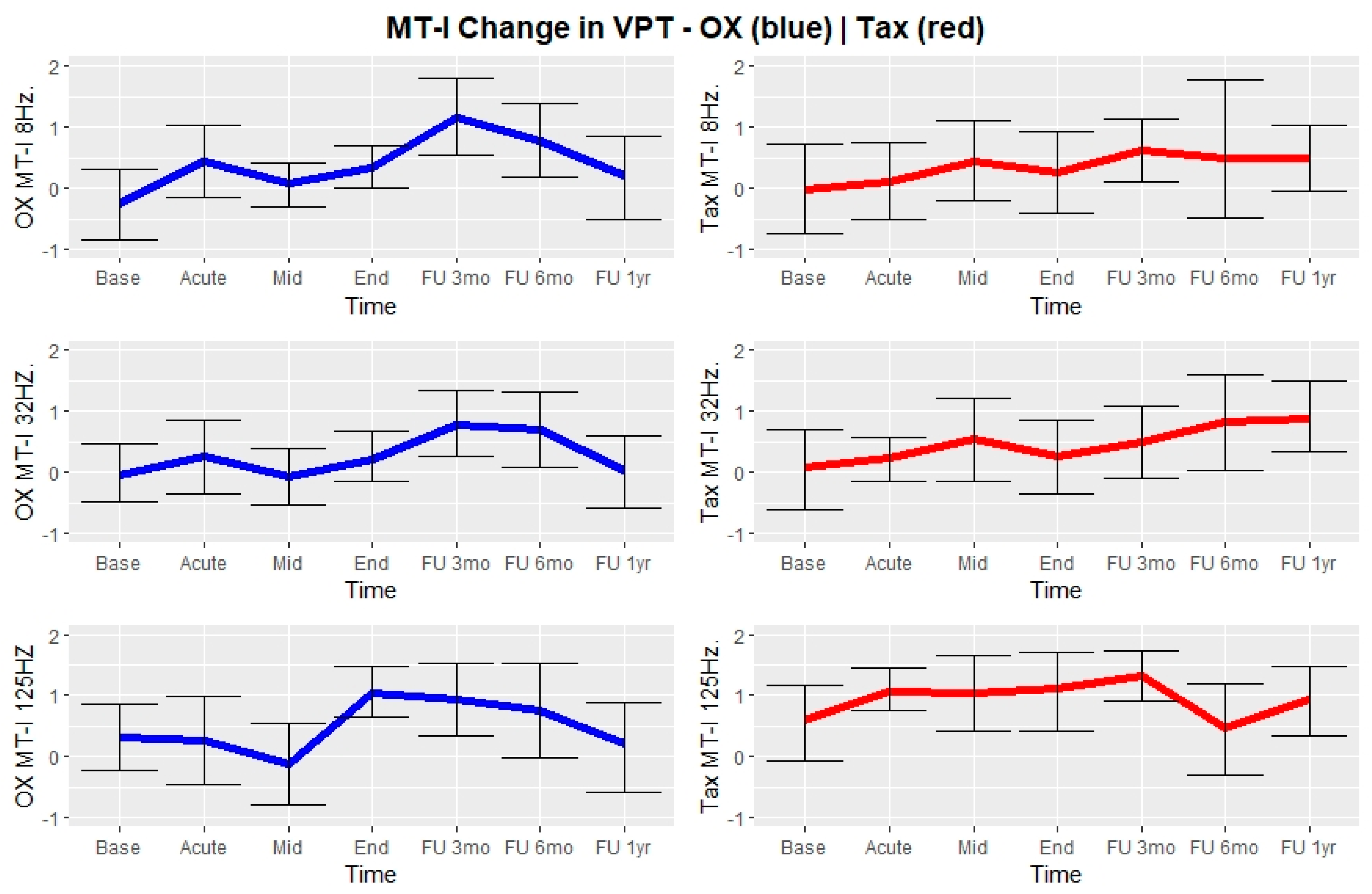
3.3. Vibrations Perceptions Thresholds
3.4. CIPN18 in Relation to VPTs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shapiro, C.L. Cancer Survivorship. N. Engl. J. Med. 2018, 379, 2438–2450. [Google Scholar] [CrossRef] [PubMed]
- Seretny, M.; Currie, G.L.; Sena, E.S.; Ramnarine, S.; Grant, R.; MacLeod, M.R.; Colvin, L.A.; Fallon, M. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: A systematic review and meta-analysis. Pain 2014, 155, 2461–2470. [Google Scholar] [CrossRef] [Green Version]
- Eckhoff, L.; Knoop, A.; Jensen, M.B.; Ewertz, M. Persistence of docetaxel-induced neuropathy and impact on quality of life among breast cancer survivors. Eur. J. Cancer 2015, 51, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.W.; Eckhoff, L.; Ruhlmann, C.H.B.; Herrstedt, J.; Dalton, S.O. The prevalence, distribution and impact of peripheral neuropathy among Danish patients with cancer–a population-based cross-sectional study. Acta Oncol. 2021, 61, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, S.W.; Herrstedt, J. Preventive Strategies for Chemotherapy-Induced Peripheral Neuropathy. In Diagnosis, Management and Emerging Strategies for Chemotherapy-Induced Neuropathy; Lustberg, M., Loprinzi, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 95–124. ISBN 978-3-030-78663-2. [Google Scholar]
- McCrary, J.M.; Goldstein, D.; Boyle, F.; Cox, K.; Grimison, P.; Kiernan, M.C.; Krishnan, A.V.; Lewis, C.R.; Webber, K.; Baron-Hay, S.; et al. Optimal clinical assessment strategies for chemotherapy-induced peripheral neuropathy (CIPN): A systematic review and Delphi survey. Support. Care Cancer 2017, 25, 3485–3493. [Google Scholar] [CrossRef] [PubMed]
- Colvin, L.A. Chemotherapy-induced peripheral neuropathy: Where are we now? Pain 2019, 160 (Suppl. S1), S1–S10. [Google Scholar] [CrossRef] [PubMed]
- Hertz, D.L.; Dockter, T.J.; Satele, D.V.; Loprinzi, C.L.; Le-Rademacher, J. Neuropathy severity at the time of oxaliplatin treatment alteration in patients with colon cancer (Alliance A151912). Support. Care Cancer 2021, 29, 7855–7863. [Google Scholar] [CrossRef] [PubMed]
- Timmins, H.C.; Li, T.; Trinh, T.; Kiernan, M.C.; Harrison, M.; Boyle, F.; Friedlander, M.; Goldstein, D.; Park, S.B. Weekly Paclitaxel-Induced Neurotoxicity in Breast Cancer: Outcomes and Dose Response. Oncologist 2021, 26, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Miura, Y.; Ando, M.; Yamazaki, K.; Hironaka, S.; Boku, N.; Muro, K.; Hyodo, I. Time-dependent discrepancies between physician-assessed and patient-reported oxaliplatin-induced peripheral neuropathy in patients with metastatic colorectal cancer who received mFOLFOX6 plus bevacizumab: A post hoc analysis (WJOG4407GSS2). Support. Care Cancer 2021, 29, 3715–3723. [Google Scholar] [CrossRef] [PubMed]
- Hertz, D.L.; Childs, D.S.; Park, S.B.; Faithfull, S.; Ke, Y.; Ali, N.T.; McGlown, S.M.; Chan, A.; Grech, L.B.; Loprinzi, C.L.; et al. Patient-centric decision framework for treatment alterations in patients with Chemotherapy-induced Peripheral Neuropathy (CIPN). Cancer Treat. Rev. 2021, 99, 102241. [Google Scholar] [CrossRef] [PubMed]
- Ekman, L.; Lindholm, E.; Brogren, E.; Dahlin, L.B. Normative values of the vibration perception thresholds at finger pulps and metatarsal heads in healthy adults. PLoS ONE 2021, 16, e0249461. [Google Scholar] [CrossRef] [PubMed]
- Ising, E.; Dahlin, L.B.; Elding Larsson, H. Impaired vibrotactile sense in children and adolescents with type 1 diabetes—Signs of peripheral neuropathy. PLoS ONE 2018, 13, e0196243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindholm, E.; Ndahl, M.L.; Fagher, K.; Apelqvist, J.; Dahlin, L.B. Strong association between vibration perception thresholds at low frequencies (4 and 8 Hz), neuropathic symptoms and diabetic foot ulcers. PLoS ONE 2019, 14, e0212921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, T.; Malayeri, R.; Doppelbauer, A.; Krajnik, G.; Huber, H.; Auff, E.; Pirker, R. Neurological monitoring of neurotoxicity induced by paclitaxel/cisplatin chemotherapy. Eur. J. Cancer 1997, 33, 1393–1399. [Google Scholar] [CrossRef]
- Griffith, K.A.; Couture, D.J.; Zhu, S.; Pandya, N.; Johantgen, M.E.; Cavaletti, G.; Davenport, J.M.; Tanguay, L.J.; Choflet, A.; Milliron, T.; et al. Evaluation of chemotherapy-induced peripheral neuropathy using current perception threshold and clinical evaluations. Support. Care Cancer 2014, 22, 1161–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attal, N.; Bouhassira, D.; Gautron, M.; Vaillant, J.N.; Mitry, E.; Lepère, C.; Rougier, P.; Guirimand, F. Thermal hyperalgesia as a marker of oxaliplatin neurotoxicity: A prospective quantified sensory assessment study. Pain 2009, 144, 245–252. [Google Scholar] [CrossRef]
- Forsyth, P.A.; Balmaceda, C.; Peterson, K.; Seidman, A.D.; Brasher, P.; DeAngelis, L.M. Prospective study of paclitaxel-induced peripheral neuropathy with quantitative sensory testing. J. Neurooncol. 1997, 35, 47–53. [Google Scholar] [CrossRef]
- Curry, Z.A.; Wilkerson, J.L.; Bagdas, D.; Kyte, S.L.; Patel, N.; Donvito, G.; Mustafa, M.A.; Poklis, J.L.; Niphakis, M.J.; Hsu, K.-L.; et al. Association between patient reported outcomes and quantitative sensory tests for measuring long-term neurotoxicity in breast cancer survivors treated with adjuvant paclitaxel chemotherapy. Breast Cancer Res. Treat. 2018, 125, 767–774. [Google Scholar] [CrossRef] [Green Version]
- du Bois, A.; Schlaich, M.; Lück, H.J.; Mollenkopf, A.; Wechsel, U.; Rauchholz, M.; Bauknecht, T.; Meerpohl, H.G. Evaluation of neurotoxicity induced by paclitaxel second-line chemotherapy. Support. Care Cancer 1999, 7, 354–361. [Google Scholar] [CrossRef]
- Krøigård, T.; Svendsen, T.K.; Wirenfeldt, M.; Schrøder, H.D.; Qvortrup, C.; Pfeiffer, P.; Gaist, D.; Sindrup, S.H. Oxaliplatin Neuropathy: Predictive Values of Skin Biopsy, QST and Berve Conduction. J. Neuromuscul. Dis. 2021, 8, 679–688. [Google Scholar] [CrossRef]
- Pietra, B.A.; Kantor, P.F.; Bartlett, H.L.; Chin, C.; Canter, C.E.; Larsen, R.L.; Edens, R.E.; Colan, S.D.; Towbin, J.A.; Lipshultz, S.E.; et al. Neuroscience, Mechanoreceptors Specialized to Receive Tactile Information. Circulation 2012, 126, 1079–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velasco, R.; Bruna, J. Taxane-Induced Peripheral Neurotoxicity. Toxics 2015, 3, 152–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paré, M.; Elde, R.; Mazurkiewicz, J.E.; Smith, A.M.; Rice, F.L. The Meissner corpuscle revised: A multiafferented mechanoreceptor with nociceptor immunochemical properties. J. Neurosci. 2001, 21, 7236–7246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le-Rademacher, J.; Kanwar, R.; Seisler, D.; Pachman, D.R.; Qin, R.; Abyzov, A.; Ruddy, K.J.; Banck, M.S.; Lavoie Smith, E.M.; Dorsey, S.G.; et al. Patient-reported (EORTC QLQ-CIPN20) versus physician-reported (CTCAE) quantification of oxaliplatin- and paclitaxel/carboplatin-induced peripheral neuropathy in NCCTG/Alliance clinical trials. Support. Care Cancer 2017, 25, 3537–3544. [Google Scholar] [CrossRef]
- Kieffer, J.M.; Postma, T.J.; van de Poll-Franse, L.; Mols, F.; Heimans, J.J.; Cavaletti, G.; Aaronson, N.K. Evaluation of the psychometric properties of the EORTC chemotherapy-induced peripheral neuropathy questionnaire (QLQ-CIPN20). Qual. Life Res. 2017, 26, 2999–3010. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, C.L.; Reeves, B.N.; Dakhil, S.R.; Sloan, J.A.; Wolf, S.L.; Burger, K.N.; Kamal, A.; Le-Lindqwister, N.A.; Soori, G.S.; Jaslowski, A.J.; et al. Natural history of paclitaxel-associated acute pain syndrome: Prospective cohort study NCCTG N08C1. J. Clin. Oncol. 2011, 29, 1472–1478. [Google Scholar] [CrossRef]
- Pachman, D.R.; Qin, R.; Seisler, D.; Smith, E.M.L.; Kaggal, S.; Novotny, P.; Ruddy, K.J.; Lafky, J.M.; Ta, L.E.; Beutler, A.S.; et al. Comparison of oxaliplatin and paclitaxel-induced neuropathy (Alliance A151505). Support. Care Cancer 2016, 24, 5059–5068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bæksted, C.; Nissen, A.; Pappot, H.; Bidstrup, P.E.; Mitchell, S.A.; Basch, E.; Dalton, S.O.; Johansen, C. Danish Translation and Linguistic Validation of the U.S. National Cancer Institute’s Patient-Reported Outcomes version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). J. Pain Symptom Manag. 2016, 52, 292–297. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Keller, S.D.; Gandek, B.; Brazier, J.E.; Sullivan, M. Evaluating Translations of Health Status Questionnaires: Methods from the IQOLA Project. Int. J. Technol. Assess. Health Care 1995, 11, 525–551. [Google Scholar] [CrossRef]
- Dahlin, L.B.; Güner, N.; Elding Larsson, H.; Speidel, T. Vibrotactile Perception in Finger Pulps and in the Sole of the Foot in Healthy Subjects among Children or Adolescents. PLoS ONE 2015, 10, e0119753. [Google Scholar] [CrossRef]
- Timmins, H.C.; Li, T.; Kiernan, M.C.; Baron-Hay, S.; Marx, G.; Boyle, F.; Goldstein, D.; Park, S.B. Taxane-induced peripheral neuropathy: Differences in patient report and objective assessment. Support. Care Cancer 2020, 28, 4459–4466. [Google Scholar] [CrossRef]
- Fieuws, S.; Verbeke, G.; Molenberghs, G. Random-effects models for multivariate repeated measures. Stat. Methods Med. Res. 2007, 16, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Bakdash, J.Z.; Marusich, L.R. Repeated Measures Correlation. Front. Psychol. 2017, 8, 456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Lancaster, G.A.; Dodd, S.; Williamson, P.R. Design and analysis of pilot studies: Recommendations for good practice. J. Eval. Clin. Pract. 2004, 10, 307–312. [Google Scholar] [CrossRef]
- Drechsel, T.J.; Monteiro, R.L.; Zippenfennig, C.; Ferreira, J.S.S.P.; Milani, T.L.; Sacco, I.C.N. Low and High Frequency Vibration Perception Thresholds Can Improve the Diagnosis of Diabetic Neuropathy. J. Clin. Med. 2021, 10, 3073. [Google Scholar] [CrossRef] [PubMed]
- Nelander, J.; Speidel, T.; Björkman, A.; Dahlin, L.B. Vibration thresholds are increased at low frequencies in the sole of the foot in diabetes-a novel multi-frequency approach. Diabet. Med. 2012, 29, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Hertz, D.L.; Tofthagen, C.; Faithfull, S. Predisposing Factors for the Development of Chemotherapy-Induced Peripheral Neuropathy (CIPN). In Diagnosis, Management and Emerging Strategies for Chemotherapy-Induced Neuropathy: A MASCC Book; Lustberg, M., Loprinzi, C., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 19–51. ISBN 978-3-030-78663-2. [Google Scholar]
- Chan, A.; Hertz, D.L.; Morales, M.; Adams, E.J.; Gordon, S.; Tan, C.J.; Staff, N.P.; Kamath, J.; Oh, J.; Shinde, S.; et al. Biological predictors of chemotherapy-induced peripheral neuropathy (CIPN): MASCC neurological complications working group overview. Support. Care Cancer 2019, 27, 3729–3737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizrahi, D.; Park, S.B.; Li, T.; Timmins, H.C.; Trinh, T.; Au, K.; Battaglini, E.; Wyld, D.; Henderson, R.D.; Grimison, P.; et al. Hemoglobin, Body Mass Index, and Age as Risk Factors for Paclitaxel- and Oxaliplatin-Induced Peripheral Neuropathy. JAMA Netw. Open 2021, 4, e2036695. [Google Scholar] [CrossRef]
- Verma, P.; Devaraj, J.; Skiles, J.L.; Sajdyk, T.; Ho, R.H.; Hutchinson, R.; Wells, E.; Li, L.; Renbarger, J.; Cooper, B.; et al. A Metabolomics Approach for Early Prediction of Vincristine-Induced Peripheral Neuropathy. Sci. Rep. 2020, 10, 9659. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.Y.; Lee, B.; Yoo, W.S.; Park, J.W.; Hyun, J.K. Prediction of Diabetic Sensorimotor Polyneuropathy Using Machine Learning Techniques. J. Clin. Med. 2021, 10, 4576. [Google Scholar] [CrossRef] [PubMed]
- Handler, A.; Ginty, D.D. The mechanosensory neurons of touch and their mechanisms of activation. Nat. Rev. Neurosci. 2021, 22, 521–537. [Google Scholar] [CrossRef] [PubMed]
- Boyette-Davis, J.A.; Cata, J.P.; Driver, L.C.; Novy, D.M.; Bruel, B.M.; Mooring, D.L.; Wendelschafer-Crabb, G.; Kennedy, W.R.; Dougherty, P.M. Persistent chemoneuropathy in patients receiving the plant alkaloids paclitaxel and vincristine. Cancer Chemother. Pharmacol. 2013, 71, 619–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyette-Davis, J.A.; Cata, J.P.; Zhang, H.; Driver, L.C.; Wendelschafer-Crabb, G.; Kennedy, W.R.; Dougherty, P.M. Follow-up psychophysical studies in bortezomib-related chemoneuropathy patients. J. Pain 2011, 12, 1017–1024. [Google Scholar] [CrossRef] [Green Version]
- Molassiotis, A.; Cheng, H.L.; Lopez, V.; Au, J.S.K.; Chan, A.; Bandla, A.; Leung, K.T.; Li, Y.C.; Wong, K.H.; Suen, L.K.P.; et al. Are we mis-estimating chemotherapy-induced peripheral neuropathy? Analysis of assessment methodologies from a prospective, multinational, longitudinal cohort study of patients receiving neurotoxic chemotherapy. BMC Cancer 2019, 19, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Overall | Oxaliplatin | Paclitaxel | ||
|---|---|---|---|---|
| N (%) | Mean | Mean (Range) | Mean (Range) | |
| Age and Gender | ||||
| Overall | 31 | 58 | ||
| Women | 26 (84) | 59 | 58 (46–72) | 60 (47–77) |
| Men | 5 (16) | 51 | 51 (42–59) | n/a |
| BMI | ||||
| Overall | 31 | 26.5 | 25.3 (20.5–33.7) | 27.1 (16.1–41.1) |
| Comorbidities | ||||
| None | 18 (56) | 10 | 8 | |
| Diabetes | 3 (9) | 1 | 2 | |
| Hypertension | 2 (6) | 1 | 1 | |
| COPD | 2 (6) | 0 | 2 | |
| Arthritis | 3 (9) | 0 | 3 | |
| Alcohol overconsumption (≥14 units/week) | 1 (3) | 1 | 0 | |
| Other | 6 (19) | 2 | 4 | |
| With polymorbidity (≥2) | 3 (9) | 0 | 3 | |
| With polypharmacy (≥5) | 4 (12) | 1 | 3 | |
| Smoking | ||||
| Yes | 9 (29) | 3 | 6 | |
| No (+former) | 22 (71) | 12 | 10 | |
| Alcohol Status | ||||
| No (abstains) | 4 (13) | 0 | 4 | |
| Yes | 27 (89) | 15 | 12 | |
| Cancer Diagnoses | ||||
| Rectal | 4 (13) | 4 | ||
| Colon | 10 (31) | 10 | ||
| Appendix | 1 (3) | 1 | ||
| Endometrial | 2 (6) | 2 | ||
| Ovarian and Fallopian tube | 14 (44) | 14 | ||
| Stage—Colorectal cancers | ||||
| III | 12 (39) | 12 | ||
| IV | 4 (13) | 4 | ||
| Stage—Gynecological cancers | ||||
| I | 2 (6) | 2 | ||
| II | 2 (6) | 2 | ||
| III | 9 (29) | 9 | ||
| IV | 3 (9) | 3 | ||
| Performance status (ECOG) | ||||
| 0 | 24 (77) | 12 | 12 | |
| 1 | 7 (23) | 3 | 4 |
| Oxaliplatin | Paclitaxel | |||
|---|---|---|---|---|
| 3 Months after Treatment (n = 13) | 12 Months after Treatment (n = 14) | 3 Months after Treatment (n = 14) | 12 Months after Treatment (n = 15) | |
| Beta-Coefficient | Beta-Coefficient | Beta-Coefficient | Beta-Coefficient | |
| Age | 0.43 | 0.12 | −0.06 | 0.18 |
| Gender (Ref.: Male) | 0.62 | −1.21 | N/a | N/a |
| BMI | 0.42 | −0.12 | 0.18 | −0.13 |
| Smoking (Active) | 4.83 | −3.27 | 1.62 | −1.86 |
| Alcohol weekly | 0.03 | −0.22 | −0.36 | 0.09 |
| No. medications (0–9) | −2.08 | −1.43 | 1.63 | 1.75 |
| Cumulative dose (/100 mg) | 0.20 | 0.03 | −0.10 | 0.02 |
| Baseline z-scores compared to follow-up CIPN18 score | ||||
| Dig-II-32 Hz | −1.00 | −3.47 | −4.56 | −3.03 |
| Dig-II-125 Hz | 4.23 | 3.76 * | 5.02 | 0.31 |
| Dig-II-250 Hz | 4.86 * | 3.13 * | 8.37 | 10.52 |
| Dig-V-32 Hz | 0.39 | 0.72 | 0.39 | 0.64 |
| Dig-V-125 Hz | 2.04 | 2.74 | 2.02 | −1.74 |
| Dig-V-250 Hz | 2.99 | 2.18 | −0.02 | −2.61 |
| MT-I-8 Hz | 3.26 | 1.30 | −0.92 | 2.78 |
| MT-I-32 Hz | 2.48 | 1.11 | 0.83 | 2.91 |
| MT-I-125 Hz | 2.20 | 0.66 | 2.80 | 3.61 |
| MT-V-8 Hz | 0.87 | −1.46 | −1.10 | 1.14 |
| MT-V-32 HZ | 3.21 | 0.84 | 0.32 | 1.82 |
| MT-V-125 Hz | 8.44 * | 2.88 | 0.95 | 1.09 |
| NCCTG Acute Neuropathy Scores compared to follow-up CIPN18 score | ||||
| TAPS Sum Score | 1.94 | 1.63 | ||
| Acute CIPN Sum Score | −1.16 | −0.36 | ||
| CIPN18 Score | ||||
|---|---|---|---|---|
| Coefficient ± S.E. | r | CI-95 | p | |
| Dig-II-32 Hz | 0.019 ± 0.007 | 0.25 | (0.08, 0.45) | 0.003 |
| Dig-II-125 Hz | 0.045 ± 0.008 | 0.43 | (0.28, 0.57) | <0.0001 |
| Dig-II-250 Hz | 0.042 ± 0.009 | 0.35 | (0.18, 0.49) | <0.0001 |
| Dig-V-32 Hz | 0.034 ± 0.008 | 0.35 | (0.18, 0.49) | <0.0001 |
| Dig-V-125 Hz | 0.041 ± 0.007 | 0.40 | (0.24, 0.54) | <0.0001 |
| Dig-V-250 Hz | 0.051 ± 0.010 | 0.37 | (0.20, 0.50) | <0.0001 |
| MT-I-8 Hz | 0.058 ± 0.009 | 0.45 | (0.29, 0.58) | <0.0001 |
| MT-I-32 Hz | 0.059 ± 0.009 | 0.48 | (0.32, 0.60) | <0.0001 |
| MT-I-125 Hz | 0.046 ± 0.011 | 0.32 | (0.14, 0.47) | 0.003 |
| MT-V-8 Hz | 0.051 ± 0.009 | 0.38 | (0.22, 0.52) | <0.0001 |
| MT-V-32 Hz | 0.045 ± 0.009 | 0.36 | (0.19, 0.50) | <0.0001 |
| MT-V-125 Hz | 0.051 ± 0.008 | 0.45 | (0.29, 0.58) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nielsen, S.W.; Lindberg, S.; Ruhlmann, C.H.B.; Eckhoff, L.; Herrstedt, J. Addressing Chemotherapy-Induced Peripheral Neuropathy Using Multi-Frequency Vibrometry and Patient-Reported Outcomes. J. Clin. Med. 2022, 11, 1862. https://doi.org/10.3390/jcm11071862
Nielsen SW, Lindberg S, Ruhlmann CHB, Eckhoff L, Herrstedt J. Addressing Chemotherapy-Induced Peripheral Neuropathy Using Multi-Frequency Vibrometry and Patient-Reported Outcomes. Journal of Clinical Medicine. 2022; 11(7):1862. https://doi.org/10.3390/jcm11071862
Chicago/Turabian StyleNielsen, Sebastian W., Sanne Lindberg, Christina Halgaard Bruvik Ruhlmann, Lise Eckhoff, and Jørn Herrstedt. 2022. "Addressing Chemotherapy-Induced Peripheral Neuropathy Using Multi-Frequency Vibrometry and Patient-Reported Outcomes" Journal of Clinical Medicine 11, no. 7: 1862. https://doi.org/10.3390/jcm11071862
APA StyleNielsen, S. W., Lindberg, S., Ruhlmann, C. H. B., Eckhoff, L., & Herrstedt, J. (2022). Addressing Chemotherapy-Induced Peripheral Neuropathy Using Multi-Frequency Vibrometry and Patient-Reported Outcomes. Journal of Clinical Medicine, 11(7), 1862. https://doi.org/10.3390/jcm11071862