
Ablation Index Predicts Successful Ablation of Focal Atrial Tachycardia: Results of a Multicenter Study

 ,
,  , , , , ,
, , , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Electrophysiology Study and Catheter Ablation
2.3. Ablation Index
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Electrophysiological and Procedural Findings
3.3. Outcomes
3.4. Ablation Index and Outcomes
4. Discussion
4.1. Main Findings
4.2. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, M.; Loveday, J.J.; Wynn, G.J.; Gomes, S.; Saeed, Y.; Bonnett, L.J.; Waktare, J.E.P.; Todd, D.M.; Hall, M.C.S.; Snowdon, R.L.; et al. Ablation index, a novel marker of ablation lesion quality: Prediction of pulmonary vein reconnection at repeat electrophysiology study and regional differences in target values. Europace 2017, 19, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.; Das, M.; Riva, S.; Morgan, M.; Ronayne, C.; Sahni, A.; Shaw, M.; Todd, D.; Hall, M.; Modi, S.; et al. Use of Ablation Index-Guided Ablation Results in High Rates of Durable Pulmonary Vein Isolation and Freedom from Arrhythmia in Persistent Atrial Fibrillation Patients: The PRAISE Study Results. Circ. Arrhythm. Electrophysiol. 2018, 11, e006576. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Dello Russo, A.; Riva, S.; Catto, V.; Negro, G.; Sicuso, R.; Cellucci, S.; Gasperetti, A.; Zucchetti, M.; Ribatti, V.; et al. An ablation index operator-independent approach to improve efficacy in atrial fibrillation ablation at 24-month follow-up: A single center experience. J. Interv. Card. Electrophysiol. 2020, 57, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, A.; Papageorgiou, N.; Lim, W.Y.; Wongwarawipat, T.; Hunter, R.J.; Dhillon, G.; Schilling, R.J.; Creta, A.; El Haddad, M.; Duytschaever, M.; et al. Efficacy and safety of ablation index-guided catheter ablation for atrial fibrillation: An updated meta-analysis. Europace 2020, 22, 1659–1671. [Google Scholar] [CrossRef] [PubMed]
- Viola, G.; Stabile, G.; Bandino, S.; Rossi, L.; Marrazzo, N.; Pecora, D.; Bottoni, N.; Solimene, F.; Schillaci, V.; Scaglione, M.; et al. Safety, efficacy, and reproducibility of cavotricuspid isthmus ablation guided by the ablation index: Acute results of the FLAI study. Europace 2021, 23, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Gasperetti, A.; Gianni, C.; Zucchelli, G.; Notarstefano, P.; Al-Ahmad, A.; Burkhardt, J.D.; Soldati, E.; Della Rocca, D.; Catto, V.; et al. Ablation Index as a predictor of long-term efficacy in premature ventricular complex ablation: A regional target value analysis. Heart. Rhythm 2019, 16, 888–895. [Google Scholar] [CrossRef] [PubMed]
- Gasperetti, A.; Sicuso, R.; Dello Russo, A.; Zucchelli, G.; Saguner, A.M.; Notarstefano, P.; Soldati, E.; Bongiorni, M.G.; Della Rocca, D.G.; Mohanty, S.; et al. Prospective use of ablation index for the ablation of right ventricle outflow tract premature ventricular contractions: A proof of concept study. Europace 2021, 23, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Kistler, P.M.; Roberts-Thomson, K.C.; Haqqani, H.M.; Fynn, S.P.; Singarayar, S.; Vohra, J.K.; Morton, J.B.; Sparks, P.B.; Kalman, J.M. P-wave morphology in focal atrial tachycardia: Development of an algorithm to predict the anatomic site of origin. J. Am. Coll. Cardiol. 2006, 48, 1010–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saoudi, N.; Cosio, F.; Waldo, A.; Chen, S.A.; Iesaka, Y.; Lesh, M.; Saksena, S.; Salerno, J.; Schoels, W. Classification of atrial flutter and regular atrial tachycardia according to electrophysiologic mechanism and anatomic bases: A statement from a joint expert group from the Working Group of Arrhythmias of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. J. Cardiovasc. Electrophysiol. 2001, 12, 852–866. [Google Scholar] [CrossRef] [PubMed]
- Compagnucci, P.; Volpato, G.; Falanga, U.; Cipolletta, L.; Conti, M.; Grifoni, G.; Verticelli, L.; Schicchi, N.; Giovagnoni, A.; Casella, M.; et al. Recent advances in three-dimensional electroanatomical mapping guidance for the ablation of complex atrial and ventricular arrhythmias. J. Interv. Card. Electrophysiol. 2021, 61, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Manolis, A.S.; Lazaridis, K. Focal atrial tachycardia ablation: Highly successful with conventional mapping. J. Interv. Card. Electrophysiol. 2019, 55, 35–46. [Google Scholar] [CrossRef]
- De Martino, G.; Compagnucci, P.; Mancusi, C.; Vassallo, E.; Calvanese, C.; Della Ratta, G.; Librera, M.; Franciulli, M.; Marino, L.; Russo, A.D.; et al. Stepwise endo-/epicardial catheter ablation for atrial fibrillation: The Mediterranea approach. J. Cardiovasc. Electrophysiol. 2021, 32, 2107–2115. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, J.; Rajani, R.; Chubb, H.; Gabrawi, M.; Varela, M.; Wright, M.; Niederer, S.; O’Neill, M.D. The role of myocardial wall thickness in atrial arrhythmogenesis. Europace 2016, 18, 1758–1772. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Dello Russo, A.; Pelargonio, G.; Del Greco, M.; Zingarini, G.; Piacenti, M.; Di Cori, A.; Casula, V.; Marini, M.; Pizzamiglio, F.; et al. Near zerO fluoroscopic exPosure during catheter ablAtion of supRavenTricular arrhYthmias: The NO-PARTY multicentre randomized trial. Europace 2016, 18, 1565–1572. [Google Scholar] [CrossRef]
- Bergonti, M.; Dello Russo, A.; Sicuso, R.; Ribatti, V.; Compagnucci, P.; Catto, V.; Gasperetti, A.; Zucchetti, M.; Cellucci, S.; Vettor, G.; et al. Long-Term Outcomes of Near-Zero Radiation Ablation of Paroxysmal Supraventricular Tachycardia: A Comparison with Fluoroscopy-Guided Approach. JACC Clin. Electrophysiol. 2021, 7, 1108–1117. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.; Jeevanantham, V.; Simon, R.; Filippone, J.; Vorobiof, G.; Daubert, J. Variation in left atrial transmural wall thickness at sites commonly targeted for ablation of atrial fibrillation. J. Interv. Card. Electrophysiol. 2006, 17, 127–132. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 45) | |
| Age—years (SD) | 49 (17) |
| Male sex—no. (%) | 27 (60) |
| CHA2DS2-VASc score—median (1st–3rd quartile) | 1 (1–2) |
| HASBLED score—median (1st–3rd quartile) | 0 (0–1) |
| EHRA score at baseline—median (1st–3rd quartile) | 1 (0–2) |
| Structural heart disease—no. (%) | 11 (24) |
| Congenital heart disease s/p surgical procedure—no. (%) | 4 (9) |
| Valvular heart disease s/p surgical procedure—no. (%) | 2 (4) |
| Mitral valve disease s/p mitral valve repair plus coronary artery disease—no. (%) | 1 (2) |
| Myocarditis—no. (%) | 1 (2) |
| Dilated cardiomyopathy—no. (%) | 1 (2) |
| Restrictive cardiomyopathy plus coronary artery disease—no. (%) | 1 (2) |
| Hypertensive heart disease—no. (%) | 1 (2) |
| Echocardiography: Left ventricular ejection fraction—% (1st–3rd quartile) Indexed left atrial volume—ml/m2 (1st–3rd quartile) Right atrial area—cm2 (SD) | 60 (58–65) 32 (24–50) 20 (7) |
| History of atrial fibrillation—no. (%) | 13 (29) |
| History of atrial flutter—no. (%) | 10 (22) |
| Frequent PACs—no. (%) | 13 (29) |
| Frequent PACs burden—no./24 h (SD) | 11471 (7412) |
| Prior catheter ablation: | 13 (29) |
| Prior pulmonary vein isolation—no. (%) | 6 (13) |
| Prior focal AT ablation—no. (%) | 3 (7) |
| Prior cavotricuspid isthmus ablation—no. (%) | 3 (7) |
| Prior AVNRT ablation—no. (%) | 1 (2) |
| Antiarrhythmic drugs at baseline: | |
| None | 14 (31) |
| Class I | 21 (47) |
| Class III | 3 (7) |
| Class II | 16 (36) |
| Class IV | 3 (7) |
| No Recurrence Group (n = 36) | Recurrence Group (n = 9) | p | |
|---|---|---|---|
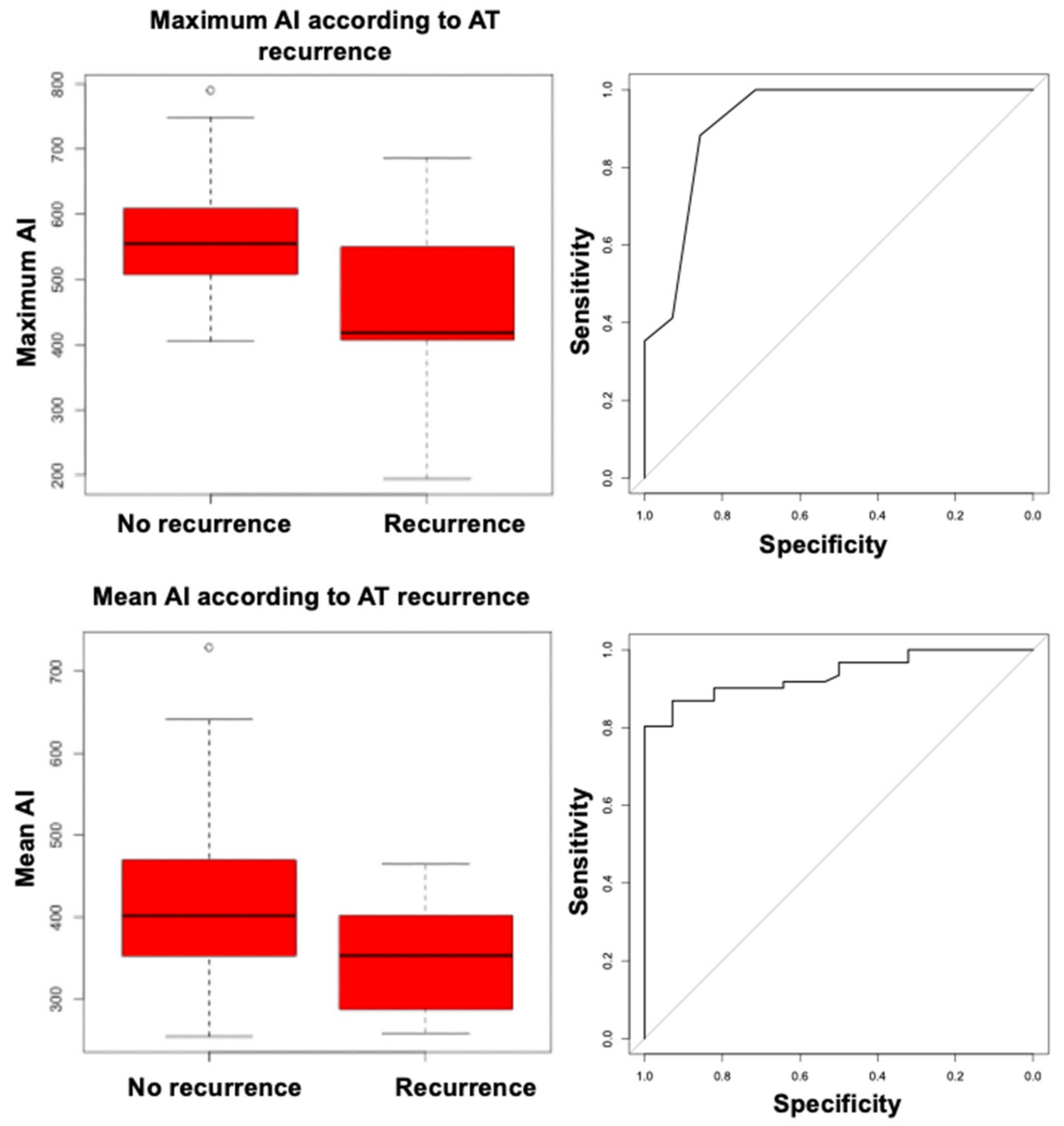
| Maximum AI—mean (SD) | 568 (91) | 447(142) | 0.036 |
| Mean AI—mean (SD) | 426 (105) | 352 (76) | 0.0284 |
| Minimum AI—median (1st–3rd quartile) | 243 (196–338) | 244 (161–320) | 0.60 |
| Procedural duration—min (1st–3rd quartile) | 120 (90–150) | 130 (120–150) | 0.45 |
| RF time—min (1st–3rd quartile) | 5 (2–8) | 3 (2–4) | 0.50 |
| Number of RF pulses—median (1st–3rd quartile) | 10 (3–18) | 6 (6–7) | 0.30 |
| VISITAG no.—median (1st–3rd quartile) | 12 (4–21) | 8 (7–17) | 0.80 |
| Fluoroscopy time—min (1st–3rd quartile) | 13 (6–21) | 10 (4–11) | 0.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Compagnucci, P.; Dello Russo, A.; Bergonti, M.; Anselmino, M.; Zucchelli, G.; Gasperetti, A.; Cipolletta, L.; Volpato, G.; Ascione, C.; Ferraris, F.; et al. Ablation Index Predicts Successful Ablation of Focal Atrial Tachycardia: Results of a Multicenter Study. J. Clin. Med. 2022, 11, 1802. https://doi.org/10.3390/jcm11071802
Compagnucci P, Dello Russo A, Bergonti M, Anselmino M, Zucchelli G, Gasperetti A, Cipolletta L, Volpato G, Ascione C, Ferraris F, et al. Ablation Index Predicts Successful Ablation of Focal Atrial Tachycardia: Results of a Multicenter Study. Journal of Clinical Medicine. 2022; 11(7):1802. https://doi.org/10.3390/jcm11071802
Chicago/Turabian StyleCompagnucci, Paolo, Antonio Dello Russo, Marco Bergonti, Matteo Anselmino, Giulio Zucchelli, Alessio Gasperetti, Laura Cipolletta, Giovanni Volpato, Ciro Ascione, Federico Ferraris, and et al. 2022. "Ablation Index Predicts Successful Ablation of Focal Atrial Tachycardia: Results of a Multicenter Study" Journal of Clinical Medicine 11, no. 7: 1802. https://doi.org/10.3390/jcm11071802
APA StyleCompagnucci, P., Dello Russo, A., Bergonti, M., Anselmino, M., Zucchelli, G., Gasperetti, A., Cipolletta, L., Volpato, G., Ascione, C., Ferraris, F., Valeri, Y., Bongiorni, M. G., Natale, A., Tondo, C., De Ferrari, G. M., & Casella, M. (2022). Ablation Index Predicts Successful Ablation of Focal Atrial Tachycardia: Results of a Multicenter Study. Journal of Clinical Medicine, 11(7), 1802. https://doi.org/10.3390/jcm11071802