
Intravascular Lithotripsy for the Treatment of Stent Underexpansion: The Multicenter IVL-DRAGON Registry

 ,
,  , , ,
, , ,  , ,
, ,  , , , , ,
, , , , ,  , , ,
, , ,  , , , ,
, , , ,  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Methods
2.1. Study Device
2.2. Patient Follow-Up and Study Endpoints
2.3. Procedure
2.4. QCA Measurements
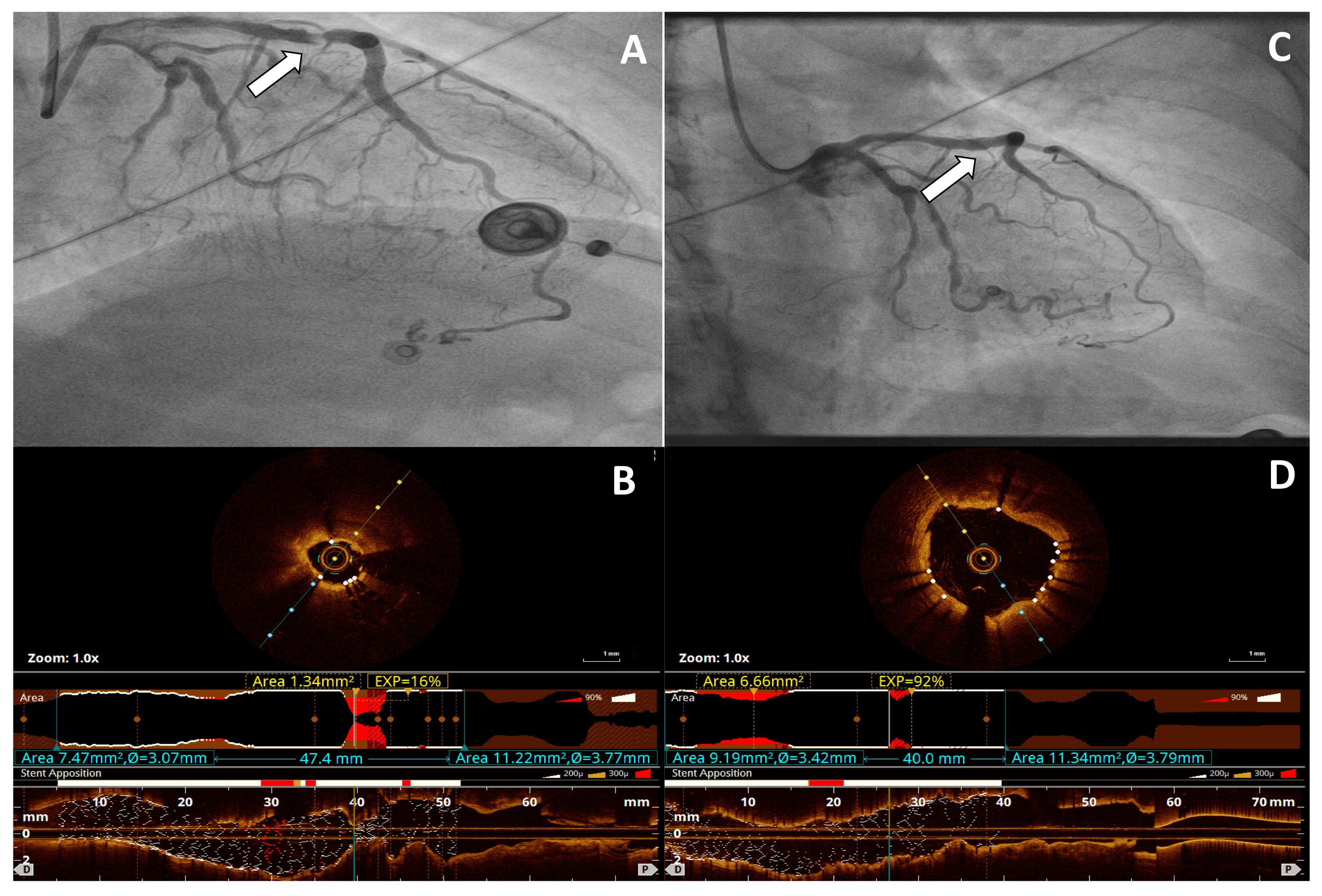
2.5. OCT Image Acquisition
2.6. IVUS Image Acquisition
2.7. Statistical Analysis
3. Results
3.1. Patients, Lesion Characteristics, and Procedural Data
3.2. Primary Efficacy Endpoint and Secondary Endpoint
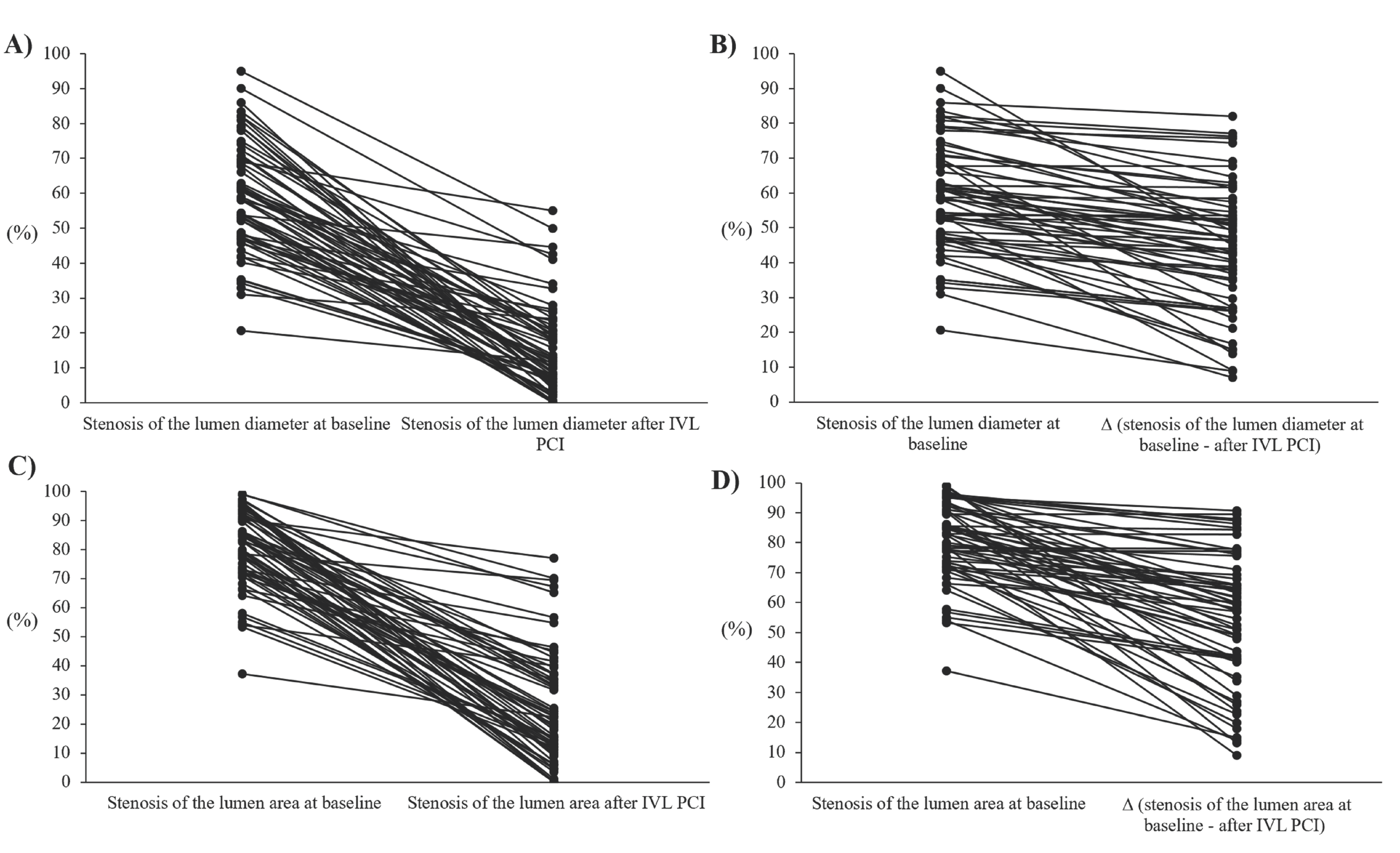
3.3. Quantitative Findings
3.4. OCT and IVUS Data
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| DOCE | device-oriented composite endpoint |
| ISR | in-stent restenosis |
| IVL | intravascular lithotripsy |
| IVUS | intravascular ultrasound |
| MI | myocardial infarction |
| OCT | optical coherence tomography |
| PCI | percutaneous coronary intervention |
| TLR | target lesion revascularization |
| TV-MI | target vessel myocardial infarction |
| QCA | quantitative coronary angiography |
References
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.J.; Mintz, G.S.; Park, D.W.; Lee, S.W.; Kim, Y.H.; Whan Lee, C.; Han, K.-H.; Kim, J.-J.; Park, S.-W.; Park, S.-J. Mechanisms of in-stent restenosis after drug-eluting stent implantation: Intravascular ultrasound analysis. Circ. Cardiovasc. Interv. 2011, 4, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Taniwaki, M.; Radu, M.D.; Zaugg, S.; Amabile, N.; Garcia-Garcia, H.M.; Yamaji, K.; Jørgensen, E.; Kelbæk, H.; Pilgrim, T.; Caussin, C.; et al. Mechanisms of Very Late Drug-Eluting Stent Thrombosis Assessed by Optical Coherence Tomography. Circulation 2016, 133, 650–660. [Google Scholar] [CrossRef] [PubMed]
- Wanha, W.; Januszek, R.; Kolodziejczak, M.; Kuzma, L.; Tajstra, M.; Figatowski, T.; Smolarek-Nicpoń, M.; Gruz-Kwapisz, M.; Tomasiewicz, B.; Bartuś, J.; et al. Procedural and 1-year outcomes following large vessel coronary artery perforation treated by covered stents implantation: Multicentre CRACK registry. PLoS ONE 2021, 16, e0249698. [Google Scholar] [CrossRef] [PubMed]
- Kawata, M.; Kato, Y.; Takada, H.; Kamemura, K.; Matsuura, A.; Sakamoto, S. Successful rotational atherectomy for a repetitive restenosis lesion with underexpansion of double layer drug-eluting stents due to heavily calcified plaque. Cardiovasc. Interv. Ther. 2016, 31, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Edes, I.F.; Ruzsa, Z.; Szabo, G.; Lux, A.; Geller, L.; Molnar, L.; Nowotta, F.; Hajas, Á.; Szilveszter, B.; Becker, D.; et al. Rotational atherectomy of undilatable coronary stents: Stentablation, a clinical perspective and recommendation. EuroIntervention 2016, 12, e632–e635. [Google Scholar] [CrossRef] [PubMed]
- Latib, A.; Takagi, K.; Chizzola, G.; Tobis, J.; Ambrosini, V.; Niccoli, G.; Sardella, G.; DiSalvo, M.E.; Armigliato, P.; Valgimigli, M.; et al. Excimer Laser LEsion modification to expand non-dilatable stents: The ELLEMENT registry. Cardiovasc. Revasc. Med. 2014, 15, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Brinton, T.J.; Ali, Z.A.; Hill, J.M.; Meredith, I.T.; Maehara, A.; Illindala, U.; Lansky, A.; Götberg, M.; Van Mieghem, N.M.; Whitbourn, R.; et al. Feasibility of Shockwave Coronary Intravascular Lithotripsy for the Treatment of Calcified Coronary Stenoses. Circulation 2019, 139, 834–836. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.M.; Kereiakes, D.J.; Shlofmitz, R.A.; Klein, A.J.; Riley, R.F.; Price, M.J.; Herrmann, H.C.; Bachinsky, W.; Waksman, R.; Stone, G.W.; et al. Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 2635–2646. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Yamazaki, S.; Takahashi, A.; Namiki, A.; Kawasaki, T.; Otsuji, S.; Nakamura, S.; Shibata, Y.; Disrupt CAD IV Investigators. Intravascular Lithotripsy for Vessel Preparation in Severely Calcified Coronary Arteries Prior to Stent Placement—Primary Outcomes from the Japanese Disrupt CAD IV Study. Circ. J. 2021, 85, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; McEntegart, M.; Hill, J.M.; Spratt, J.C. Intravascular lithotripsy for treatment of stent underexpansion secondary to severe coronary calcification. Eur. Heart J. 2020, 41, 485–486. [Google Scholar] [CrossRef] [PubMed]
- De Silva, K.; Roy, J.; Webb, I.; Dworakowski, R.; Melikian, N.; Byrne, J.; MacCarthy, P.; Hill, J. A Calcific, Undilatable Stenosis: Lithoplasty, a New Tool in the Box? JACC Cardiovasc. Interv. 2017, 10, 304–306. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Alfonso, F.; Bastante, T.; Antuna, P.; de la Cuerda, F.; Cuesta, J.; Garcia-Guimaraes, M.; Rivero, F. Coronary Lithoplasty for the Treatment of Undilatable Calcified De Novo and In-Stent Restenosis Lesions. JACC Cardiovasc. Interv. 2019, 12, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Watkins, S.; Good, R.; Hill, J.; Brinton, T.J.; Oldroyd, K.G. Intravascular lithotripsy to treat a severely underexpanded coronary stent. EuroIntervention 2019, 15, 124–125. [Google Scholar] [CrossRef] [PubMed]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.A.; Steg, P.G.; Morel, M.; Mauri, L.; Vranckx, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef] [PubMed]
- Raber, L.; Mintz, G.S.; Koskinas, K.C.; Johnson, T.W.; Holm, N.R.; Onuma, Y.; Radu, M.D.; Joner, M.; Yu, B.; Jia, H.; et al. Clinical use of intracoronary imaging. Part 1: Guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. EuroIntervention 2018, 14, 656–677. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.A.; Nef, H.; Escaned, J.; Werner, N.; Banning, A.P.; Hill, J.M.; de Bruyne, B.; Montorfano, M.; Lefevre, T.; Stone, G.W.; et al. Safety and Effectiveness of Coronary Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Stenoses: The Disrupt CAD II Study. Circ. Cardiovasc. Interv. 2019, 12, e008434. [Google Scholar] [CrossRef] [PubMed]
- Kereiakes, D.J.; Virmani, R.; Hokama, J.Y.; Illindala, U.; Mena-Hurtado, C.; Holden, A.; Hill, J.M.; Lyden, S.P.; Ali, Z.A. Principles of Intravascular Lithotripsy for Calcific Plaque Modification. JACC Cardiovasc. Interv. 2021, 14, 1275–1292. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.; Shammas, N.; Mangalmurti, S.; Bernardo, N.L.; Miller, W.E.; Soukas, P.A.; Parikh, S.A.; Armstrong, E.J.; Tepe, G.; Lansky, A.; et al. Intravascular Lithotripsy for Treatment of Calcified Lower Extremity Arterial Stenosis: Initial Analysis of the Disrupt PAD III Study. J. Endovasc. Ther. 2020, 27, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Shlofmitz, R.A.; Song, L.; Tsiamtsiouris, T.; Pappas, T.; Madrid, A.; Jeremias, A.; Haag, E.S.; Ali, Z.A.; Moses, J.W.; et al. The effectiveness of excimer laser angioplasty to treat coronary in-stent restenosis with peri-stent calcium as assessed by optical coherence tomography. EuroIntervention 2019, 15, e279–e288. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| PCI with IVL | |
|---|---|
| Age, y | 69 ± 7.1 |
| Male sex | 41 (66.1) |
| Body mass index, kg/m2 | 30 ± 4.2 |
| Discharge diagnosis | |
| Chronic coronary syndrome, n (%) | 30 (48.4) |
| Unstable angina, n (%) | 10 (16.1) |
| Non–ST-segment elevation myocardial infarction | 20 (32.3) |
| ST-segment elevation myocardial infarction | 2 (3.2) |
| Previous myocardial infarction | 43 (69.4) |
| Previous CABG | 10 (16.1) |
| Diabetes mellitus | 28 (45.2) |
| On insulin | 9 (14.5) |
| Hypertension | 58 (93.5) |
| Hyperlipidemia | 58 (93.5) |
| Chronic kidney disease * | 10 (16.1) |
| Dialysis | 1 (1.6) |
| Atrial fibrillation | 15 (24.2) |
| Prior smoker | 14 (22.6) |
| Current smoker | 11 (17.7) |
| Pulmonary disease | 10 (16.1) |
| Peripheral artery disease | 16 (25.8) |
| Time since last PCI of target lesion, months | 12.0 (4.0–54.0) |
| Recurrent in-stent restenosis | 28 (45.2) |
| Number of in-stent restenosis events | 1.8 ± 1.4 |
| Left ventricular ejection fraction, % | 48 ± 11.5 |
| PCI with IVL (n = 62) | |
|---|---|
| Number of diseased vessels | |
| 1 | 30 (48.4) |
| 2 | 15 (24.2) |
| 3 | 17 (27.4) |
| Treated artery | |
| LM | 6 (9.7) |
| LAD | 16 (25.8) |
| LCx | 9 (14.5) |
| RCA | 31 (50.0) |
| Underexpansion in drug-eluting stent | 61 (98.4) |
| Underexpansion in bare-metal stents | 1 (1.6) |
| Number of stent layers | 1.4 ± 0.8 |
| Bifurcation lesion | 9 (14.5) |
| Severe calcification on angiography | 37 (59.7) |
| IVL data | |
| Total procedure time, min | 86.3 ± 58.4 |
| Fluoroscopy time, min | 21.7 ± 13.2 |
| Number of IVL catheters | 1.0 ± 0.1 |
| Number of pulses | 66.3 ± 25.7 |
| IVL balloon size, mm | 3.3 ± 0.4 |
| IVL balloon pressure, atm | 8.0 ± 3.3 |
| PCI with drug-eluting stent | 24 (38.7) |
| PCI with drug-coated balloon | 20 (32.3) |
| Plain old balloon angioplasty | 18 (29.0) |
| Predilation | |
| Semi-compliant balloon | 2 (3.2) |
| Non- compliant balloon | 57 (91.9) |
| Very high-pressure balloon | 3 (4.9) |
| Predilation balloon nominal diameter, mm | 3.3 ± 0.5 |
| Maximum predilation inflation pressure, atm | 21.4 ± 5.2 |
| Postdilation | |
| Semi-compliant balloon | 4 (6.5) |
| Non-compliant balloon | 49 (79.0) |
| Very high-pressure balloon | - |
| Postdilation balloon nominal diameter, mm | 3.8 ± 0.5 |
| Maximum postdilation inflation pressure, atm | 19.6 ± 5.1 |
| Complications | |
| Perforation | 1 (1.6) |
| Dissection | 1 (1.6) |
| No reflow | - |
| Procedural use of intracoronary imaging | |
| 1-IVUS | 14 (22.6) |
| 2-OCT | 15 (24.2) |
| Before IVL | Post IVL | p | |
|---|---|---|---|
| Quantitative findings, n = 62 (100) | |||
| Diameter stenosis at MLD, (%) | 58.5 (47.5–69.7) | 11.4 (5.8–20.7) | <0.001 |
| Area stenosis at MLD, (%) | 82.6 (72.4–90.8) | 21.5 (11.1–37.2) | <0.001 |
| MLD, (mm) | 1.1(0.7–1.4) | 2.6 (2.3–3.1) | <0.001 |
| Lesion length, mm | 21.2 ± 11.2 | - | |
| OCT, n = 15 (24.2) | |||
| Stent expansion at MSA, % | 37.5 (16.0–66.0) | 86.0 (69.2–90.7) | <0.001 |
| MLA, mm2 | 1.9 (1.7–2.9) | 5.8 (5.5–8.0) | <0.001 |
| MSA, mm2 | 2.8 (1.8–4.0) | 6.4 (5.5–8.1) | <0.001 |
| Maximal calcium angle behind stent, ° | 277 (235–313) | 207 (175–240) | 0.004 |
| Maximum calcium thickness, mm | 0.7 (0.6–0.8) | 0.6 (0.5–0.7) | 0.003 |
| Calcium length behind stent, mm | 12.3 (11.1–17.3) | - | - |
| Malapposition, | 4 (28.6) | 1 (7.1) | 0.146 |
| Thrombus, n (%) | - | - | |
| Stent fracture, n (%) | - | - | |
| Tissue protrusion, n (%) | - | - | |
| Dissection/intramural hematoma, n (%) | - | - | |
| IVUS, n = 14 (22.6) | |||
| Stent expansion at MSA, % | 57.0 (31.5–77.2) | 89.0 (85.0–92.0) | 0.002 |
| MLA, mm2 | 2.5 (1.8–2.9) | 5.1 (3.8–8.3) | <0.001 |
| MSA, mm2 | 4.1 (2.7–5.0) | 8.3 (6.7–8.5) | <0.001 |
| Plaque burden behind stent at MLA, % | 71.0 (55.0–82.4) | 40.0 (32.2–64.7) | 0.051 |
| Remodeling index | 0.9 (0.8–0.9) | 1.2 (1.0–1.4) | 0.051 |
| Dissection/intramural hematoma, n (%) | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wańha, W.; Tomaniak, M.; Wańczura, P.; Bil, J.; Januszek, R.; Wolny, R.; Opolski, M.P.; Kuźma, Ł.; Janas, A.; Figatowski, T.; et al. Intravascular Lithotripsy for the Treatment of Stent Underexpansion: The Multicenter IVL-DRAGON Registry. J. Clin. Med. 2022, 11, 1779. https://doi.org/10.3390/jcm11071779
Wańha W, Tomaniak M, Wańczura P, Bil J, Januszek R, Wolny R, Opolski MP, Kuźma Ł, Janas A, Figatowski T, et al. Intravascular Lithotripsy for the Treatment of Stent Underexpansion: The Multicenter IVL-DRAGON Registry. Journal of Clinical Medicine. 2022; 11(7):1779. https://doi.org/10.3390/jcm11071779
Chicago/Turabian StyleWańha, Wojciech, Mariusz Tomaniak, Piotr Wańczura, Jacek Bil, Rafał Januszek, Rafał Wolny, Maksymilian P. Opolski, Łukasz Kuźma, Adam Janas, Tomasz Figatowski, and et al. 2022. "Intravascular Lithotripsy for the Treatment of Stent Underexpansion: The Multicenter IVL-DRAGON Registry" Journal of Clinical Medicine 11, no. 7: 1779. https://doi.org/10.3390/jcm11071779
APA StyleWańha, W., Tomaniak, M., Wańczura, P., Bil, J., Januszek, R., Wolny, R., Opolski, M. P., Kuźma, Ł., Janas, A., Figatowski, T., Gąsior, P., Milewski, M., Roleder-Dylewska, M., Lewicki, Ł., Kulczycki, J., Włodarczak, A., Tomasiewicz, B., Iwańczyk, S., Sacha, J., ... Wojakowski, W. (2022). Intravascular Lithotripsy for the Treatment of Stent Underexpansion: The Multicenter IVL-DRAGON Registry. Journal of Clinical Medicine, 11(7), 1779. https://doi.org/10.3390/jcm11071779