
Molecular Hallmarks of Ischemia with Non-Obstructive Coronary Arteries: The “INOCA versus Obstructive CCS” Challenge

 , , , ,
, , , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Enrolment Criteria
- –
- Stable, chronic symptoms suggesting ischemic heart disease such as chest discomfort with both typical angina pectoris or atypical features in terms of location, quality, and in-citing factors.
- –
- Objective evidence of myocardial ischemia from the electrocardiogram (ECG) or a cardiac imaging study (echocardiography, nuclear imaging, magnetic resonance imaging, or spectroscopy) at rest or during stress (exercise or pharmacological), without the rise of myocardial injury biomarkers.
- –
- Absence of flow-limiting obstruction by coronary angiography as defined by any epicardial coronary artery diameter reduction ≥50% or fractional flow reserve <0.8.
- –
- Evidence of angina with a micro-vascular origin, identified during intracoronary infusion of acetylcholine with typical ischemic ST-segment changes without epicardial coronary constriction (<90% re-duction) in coronary artery diameter [13]. As described elsewhere, functional mechanisms responsible for CMD may be related to the presence of an impaired dilation (vasodilator abnormalities, most often detected as reduced coronary flow reserve -CFR-), an increased constriction of coronary micro vessels (microvascular spasm) or a combination of both mechanisms. Our population definitely belongs to the latter group [4].
- –
- Symptoms of stable effort angina lasting more than 12 months.
- –
- Obstructive CAD confirmed at the coronary angiography [10].
- –
- Age >85 years.
- –
- Evidence of infectious diseases, malignancies, immunologic or haematological disorders.
- –
- Allergic disorders.
- –
- Severe chronic HF (left ventricular ejection fraction -LVEF < 35%).
- –
- Treatment with anti-inflammatory drugs other than low-dose aspirin.
- –
- Chronic kidney disease stage 4 (glomerular filtration rate -GFR < 30 mL/min).
2.3. Ethical Clearance
2.4. Blood Sampling and PBMC Isolation
2.5. RNA Extraction and Retro-Transcription
2.6. Prime PCR Arrays
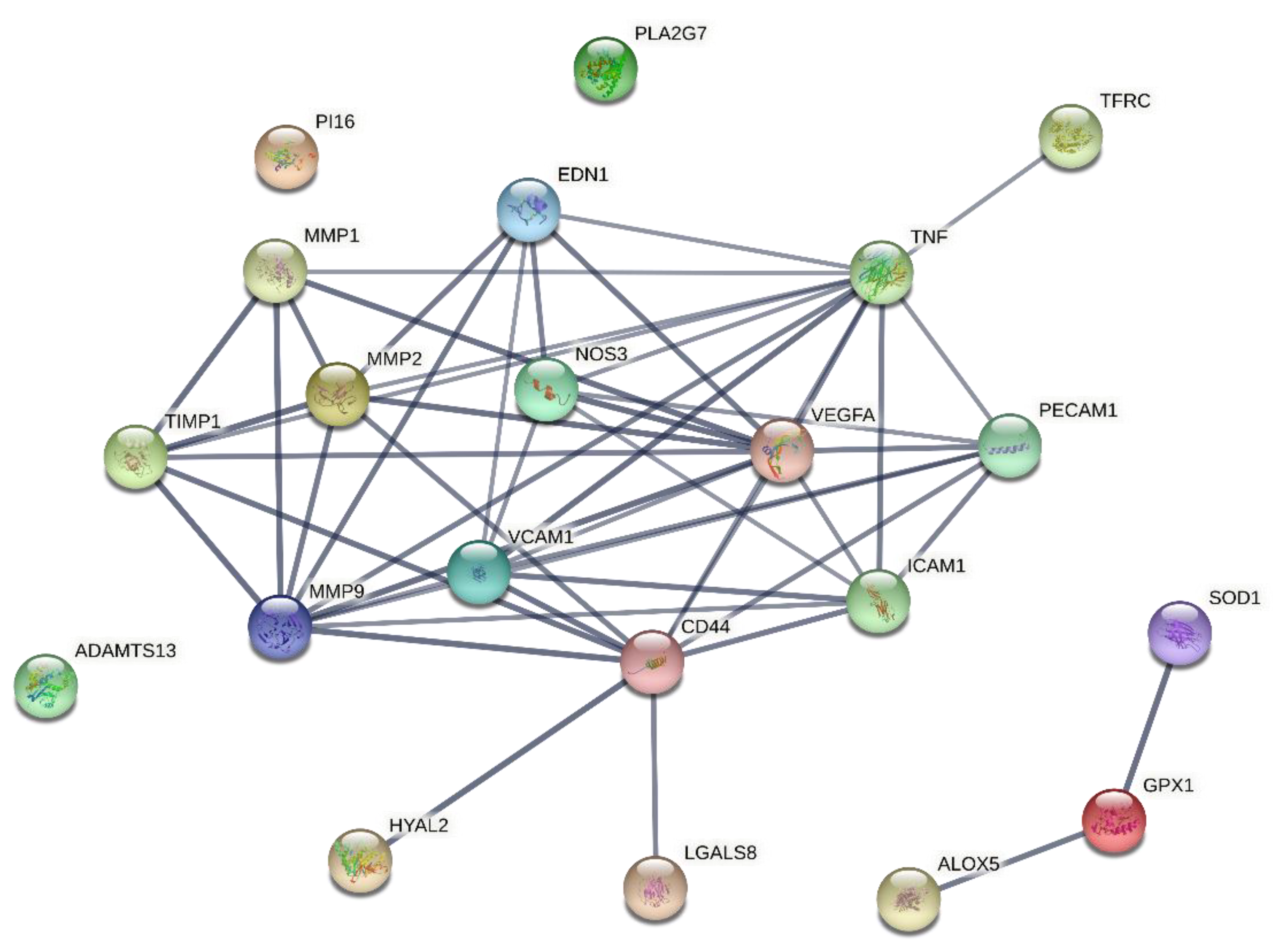
2.7. Networking Analysis
2.8. Gene Expression on Pooled cDNA
2.9. Validation of Gene Expression
2.10. Statistical Analysis
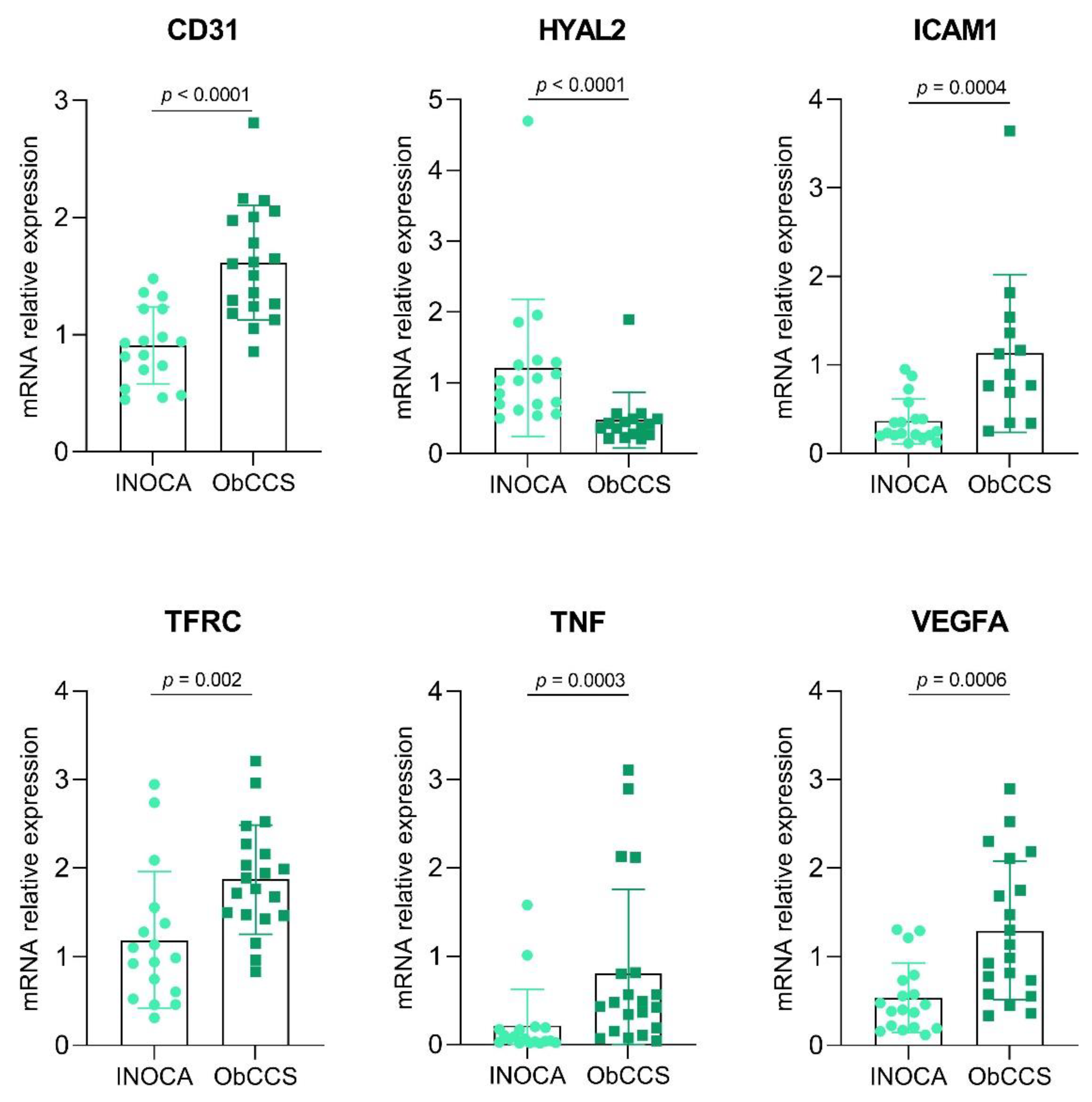
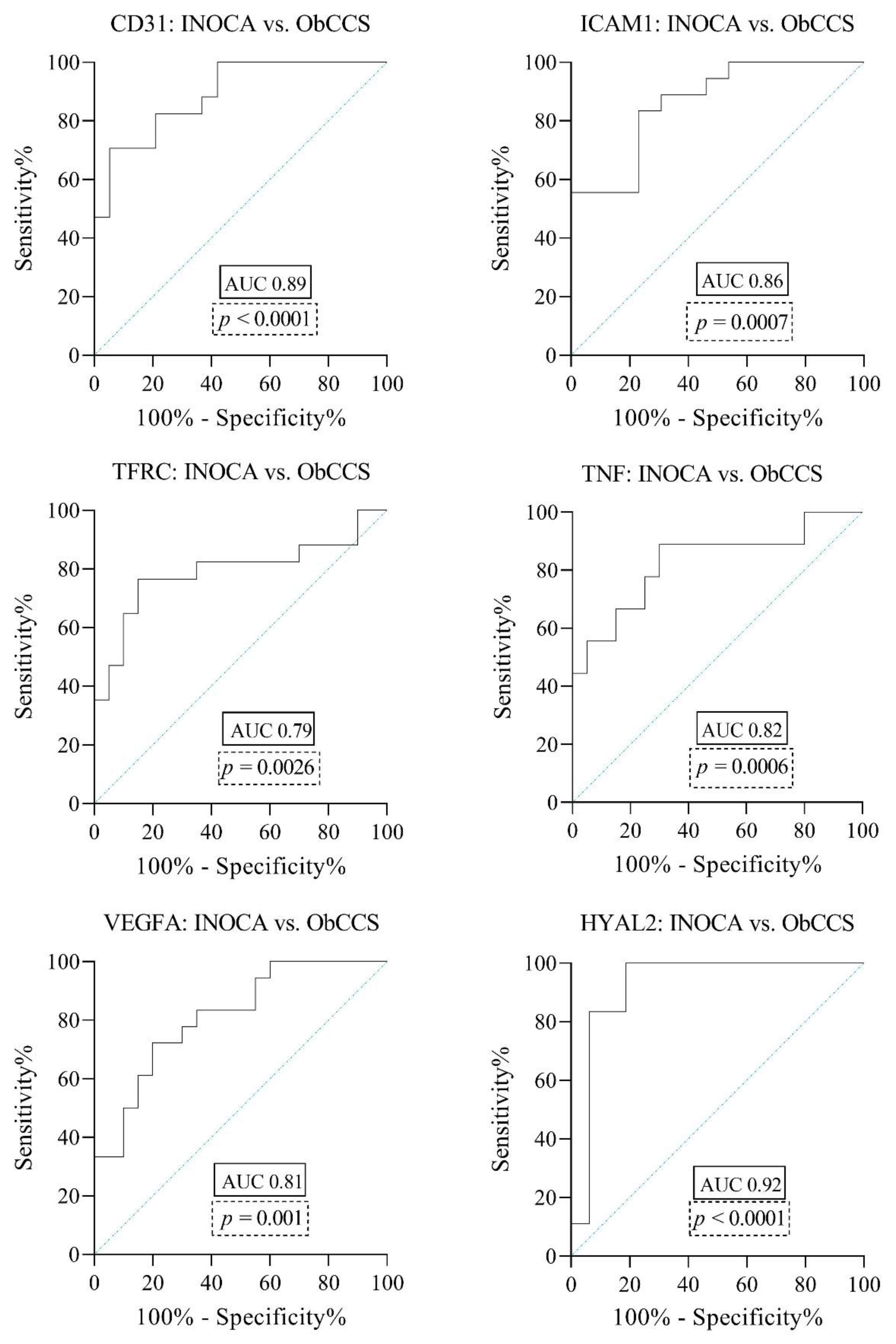
3. Results
4. Discussion
4.1. Study Limitations
4.2. Clinical Translation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bairey Merz, C.N.; Pepine, C.J.; Walsh, M.N.; Fleg, J.L. Ischemia and No Obstructive Coronary Artery Disease (INOCA): Developing Evidence-Based Therapies and Research Agenda for the Next Decade. Circulation 2017, 135, 1075–1092. [Google Scholar] [CrossRef] [PubMed]
- Parrinello, R.; Sestito, A.; Di Franco, A.; Russo, G.; Villano, A.; Figliozzi, S.; Nerla, R.; Tarzia, P.; Stazi, A.; Lanza, G.A.; et al. Peripheral arterial function and coronary microvascular function in patients with variant angina. Cardiology 2014, 129, 20–24. [Google Scholar] [CrossRef]
- Montone, R.A.; Niccoli, G.; Russo, M.; Giaccari, M.; Del Buono, M.G.; Meucci, M.C.; Gurguglione, F.; Vergallo, R.; D’Amario, D.; Buffon, A.; et al. Clinical, angiographic and echocardiographic correlates of epicardial and microvascular spasm in patients with myocardial ischaemia and non-obstructive coronary arteries. Clin. Res. Cardiol. 2020, 109, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Montone, R.A.; Meucci, M.C.; De Vita, A.; Lanza, G.A.; Niccoli, G. Coronary provocative tests in the catheterization laboratory: Pathophysiological bases, methodological considerations and clinical implications. Atherosclerosis 2021, 318, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Camici, P.G.; Bairey Merz, C.N. Coronary microvascular dysfunction: An update. Eur. Heart J. 2014, 35, 1101–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanza, G.A.; Spera, F.R.; Villano, A.; Russo, G.; Di Franco, A.; Lamendola, P.; Crea, F. Effect of smoking on endothelium-independent vasodilatation. Atherosclerosis 2015, 240, 330–332. [Google Scholar] [CrossRef]
- Wessel, T.R.; Arant, C.B.; McGorray, S.P.; Sharaf, B.L.; Reis, S.E.; Kerensky, R.A.; von Mering, G.O.; Smith, K.M.; Pauly, D.F.; Handberg, E.M.; et al. Coronary microvascular reactivity is only partially predicted by atherosclerosis risk factors or coronary artery disease in women evaluated for suspected ischemia: Results from the NHLBI Women’s Ischemia Syndrome Evaluation (WISE). Clin. Cardiol. 2007, 30, 69–74. [Google Scholar] [CrossRef]
- Wei, J.; Cheng, S.; Bairey Merz, C.N. Coronary Microvascular Dysfunction Causing Cardiac Ischemia in Women. JAMA 2019, 322, 2334–2335. [Google Scholar] [CrossRef] [PubMed]
- Ong, P.; Camici, P.G.; Beltrame, J.F.; Crea, F.; Shimokawa, H.; Sechtem, U.; Kaski, J.C.; Bairey Merz, C.N.; Coronary Vasomotion Disorders International Study Group (COVADIS). International standardization of diagnostic criteria for microvascular angina. Int. J. Cardiol. 2018, 250, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Biasucci, L.M.; La Rosa, G.; Pedicino, D.; D’Aiello, A.; Galli, M.; Liuzzo, G. Where Does Inflammation Fit? Curr. Cardiol. Rep. 2017, 19, 84. [Google Scholar] [CrossRef] [PubMed]
- Herscovici, R.; Sedlak, T.; Wei, J.; Pepine, C.J.; Handberg, E.; Bairey Merz, C.N. Ischemia and No Obstructive Coronary Artery Disease ( NOCA): What Is the Risk? J. Am. Heart Assoc. 2018, 7, e008868. [Google Scholar] [CrossRef]
- Ford, T.J.; Ong, P.; Sechtem, U.; Beltrame, J.; Camici, P.G.; Crea, F.; Kaski, J.C.; Bairey Merz, C.N.; Pepine, C.J.; Shimokawa, H.; et al. Assessment of Vascular Dysfunction in Patients Without Obstructive Coronary Artery Disease: Why, How, and When. JACC Cardiovasc. Interv. 2020, 13, 1847–1864. [Google Scholar] [CrossRef] [PubMed]
- Raman, K. Construction and analysis of protein–protein interaction networks. Autom. Exp. 2010, 2, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szklarczyk, D.; Gable, A.L.; Nastou, K.C.; Lyon, D.; Kirsch, R.; Pyysalo, S.; Doncheva, N.T.; Legeay, M.; Fang, T.; Bork, P.; et al. The STRING database in 2021: Customizable protein–protein networks, and functional characterization of user-uploaded gene/measurement sets. Nucleic Acids Res. 2021, 49, D605–D612. [Google Scholar] [CrossRef]
- Murdaca, G.; Spanò, F.; Cagnati, P.; Puppo, F. Free radicals and endothelial dysfunction: Potential positive effects of TNF-α inhibitors. Redox Rep. 2013, 18, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Goebel, S.; Huang, M.; Davis, W.C.; Jennings, M.; Siahaan, T.J.; Alexander, J.S.; Kevil, C.G. VEGF-A stimulation of leukocyte adhesion to colonic microvascular endothelium: Implications for inflammatory bowel disease. Am. J. Physiol. Gastrointest. Liver Physiol. 2006, 290, G648–G654. [Google Scholar] [CrossRef] [PubMed]
- Cursiefen, C.; Chen, L.; Borges, L.P.; Jackson, D.; Cao, J.; Radziejewski, C.; D’Amore, P.A.; Dana, M.R.; Wiegand, S.J.; Streilein, J.W. VEGF-A stimulates lymphangiogenesis and hemangiogenesis in inflammatory neovascularization via macrophage recruitment. J. Clin. Investig. 2004, 113, 1040–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imhof, B.A.; Dunon, D. Leukocyte migration and adhesion. Adv. Immunol. 1995, 58, 345–416. [Google Scholar] [CrossRef]
- Zehnder, J.L.; Shatsky, M.; Leung, L.L.; Butcher, E.C.; McGregor, J.L.; Levitt, L.J. Involvement of CD31 in lymphocyte-mediated immune responses: Importance of the membrane-proximal immunoglobulin domain and identification of an inhibiting CD31 peptide. Blood 1995, 85, 1282–1288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, D.P.; True, H.D.; Patel, J. Leukocyte Trafficking in Cardiovascular Disease: Insights from Experimental Models. Mediat. Inflamm. 2017, 2017, 9746169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Barrientos, T.; Mao, L.; Rockman, H.A.; Sauve, A.A.; Andrews, N.C. Lethal Cardiomyopathy in Mice Lacking Transferrin Receptor in the Heart. Cell Rep. 2015, 13, 533–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, J.W.; Qian, M. Molecular bases of cellular iron toxicity. Free Radic. Biol. Med. 2002, 32, 833–840. [Google Scholar] [CrossRef]
- Mittal, M.; Siddiqui, M.R.; Tran, K.; Reddy, S.P.; Malik, A.B. Reactive oxygen species in inflammation and tissue injury. Antioxid. Redox Signal. 2014, 20, 1126–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, X.; Chen, L.; Ye, P.; Wang, Z.; Zhang, J.; Ye, F.; Chen, S. The role of HYAL2 in LSS-induced glycocalyx impairment and the PKA-mediated decrease in eNOS-Ser-633 phosphorylation and nitric oxide production. Mol. Biol. Cell. 2016, 27, 3972–3979. [Google Scholar] [CrossRef]
- Yang, H.; Zhu, L.; Chao, Y.; Gu, Y.; Kong, X.; Chen, M.; Ye, P.; Luo, J.; Chen, S. Hyaluronidase2 (Hyal2) modulates low shear stress-induced glycocalyx impairment via the LKB1/AMPK/NADPH oxidase-dependent pathway. J. Cell Physiol. 2018, 233, 9701–9715. [Google Scholar] [CrossRef]
- Wang, G.; Tiemeier, G.L.; van den Berg, B.M.; Rabelink, T.J. Endothelial Glycocalyx Hyaluronan: Regulation and Role in Prevention of Diabetic Complications. Am. J. Pathol. 2020, 190, 781–790. [Google Scholar] [CrossRef]
- Pedicino, D.; Vinci, R.; Giglio, A.F.; Pisano, E.; Porto, I.; Vergallo, R.; Russo, G.; Ruggio, A.; D’Aiello, A.; Flego, D.; et al. Alterations of Hyaluronan Metabolism in Acute Coronary Syndrome: Implications for Plaque Erosion. J. Am. Coll. Cardiol. 2018, 72, 1490–1503. [Google Scholar] [CrossRef] [PubMed]
- Vinci, R.; Pedicino, D.; D’Aiello, A.; Ciampi, P.; Ponzo, M.; Bonanni, A.; Russo, G.; Montone, R.A.; Massetti, M.; Crea, F.; et al. Platelet hyaluronidase 2 enrichment in acute coronary syndromes: A conceivable role in monocyte-platelet aggregate formation. J. Enzyme. Inhib. Med. Chem. 2021, 36, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Godo, S.; Suda, A.; Takahashi, J.; Yasuda, S.; Shimokawa, H. Coronary Microvascular Dysfunction. Arterioscler Thromb Vasc Biol. 2021, 41, 1625–1637. [Google Scholar] [CrossRef] [PubMed]
- Kunadian, V.; Chieffo, A.; Camici, P.G.; Berry, C.; Escaned, J.; Maas, A.; Prescott, E.; Karam, N.; Appelman, Y.; Fraccaro, C.; et al. An EAPCI Expert Consensus Document on Ischaemia with Non-Obstructive Coronary Arteries in Collaboration with European Society of Cardiology Working Group on Coronary Pathophysiology & Microcirculation Endorsed by Coronary Vasomotor Disorders International Study Group. Eur. Heart J. 2020, 41, 3504–3520. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Lanza, G.A. Treatment of microvascular angina: The need for precision medicine. Eur. Heart J. 2016, 37, 1514–1516. [Google Scholar] [CrossRef] [Green Version]
- Del Buono, M.G.; Montone, R.A.; Camilli, M.; Carbone, S.; Narula, J.; Lavie, C.J.; Niccoli, G.; Crea, F. Coronary Microvascular Dysfunction Across the Spectrum of Cardiovascular Diseases: JACC State-of-the-Art Review. J. Am. Coll Cardiol. 2021, 78, 1352–1371. [Google Scholar] [CrossRef]
- Camici, P.G.; Crea, F. Coronary microvascular dysfunction. N. Engl. J. Med. 2007, 356, 830–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naya, M.; Aikawa, T.; Manabe, O.; Obara, M.; Koyanagawa, K.; Katoh, C.; Tamaki, N. Elevated serum endothelin-1 is an independent predictor of coronary microvascular dysfunction in non-obstructive territories in patients with coronary artery disease. Heart Vessels 2021, 36, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Pakhtusov, N.N.; Iusupova, A.O.; Privalova, E.V.; Khabarova, N.V.; Belenkov, Y.N. Endothelial dysfunction and inflammation in patients with non-obstructive coronary arteries. Kardiologiia 2021, 61, 52–58. [Google Scholar] [CrossRef]
- Schroder, J.; Mygind, N.D.; Frestad, D.; Michelsen, M.; Suhrs, H.E.; Bove, K.B.; Gustafsson, I.; Kastrup, J.; Prescott, E. Pro-inflammatory biomarkers in women with non-obstructive angina pectoris and coronary microvascular dysfunction. Int. J. Cardiol. Heart Vasc. 2019, 24, 100370. [Google Scholar] [CrossRef] [PubMed]
- Tona, F.; Serra, R.; Di Ascenzo, L.; Osto, E.; Scarda, A.; Fabris, R.; Montisci, R.; Famoso, G.; Tellatin, S.; Foletto, M.; et al. Systemic inflammation is related to coronary microvascular dysfunction in obese patients without obstructive coronary disease. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 447–453. [Google Scholar] [CrossRef] [PubMed]
- AlBadri, A.; Lai, K.; Wei, J.; Landes, S.; Mehta, P.K.; Li, Q.; Johnson, D.; Reis, S.E.; Kelsey, S.F.; Bittner, V.; et al. Inflammatory biomarkers as predictors of heart failure in women without obstructive coronary artery disease: A report from the NHLBI-sponsored Women’s Ischemia Syndrome Evaluation (WISE). PLoS ONE 2017, 12, e0177684. [Google Scholar] [CrossRef] [PubMed]
- Vancheri, F.; Longo, G.; Vancheri, S.; Henein, M. Coronary Microvascular Dysfunction. J. Clin. Med. 2020, 9, 2880. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.J.; Liu, C.A.; Huang, B.; Tseng, A.H.; Wang, D.L. Shear-induced endothelial mechanotransduction: The interplay betweenreactive oxygen species (ROS) and nitric oxide (NO) and the pathophysiological implications. J. Biomed. Sci. 2014, 21, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepine, C.J.; Anderson, R.D.; Sharaf, B.L.; Reis, S.E.; Smith, K.M.; Handberg, E.M.; Johnson, B.D.; Sopko, G.; Bairey Merz, C.N. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the National Heart, Lung and Blood Institute WISE (Women’s Ischemia Syndrome Evaluation) study. J. Am. Coll. Cardiol. 2010, 55, 2825–2832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.K.; Lim, H.S.; Fearon, W.F.; Yong, A.S.; Yamada, R.; Tanaka, S.; Lee, D.P.; Yeung, A.C.; Tremmel, J.A. Invasive evaluation of patients with angina in the absence of obstructive coronary artery disease. Circulation 2015, 131, 1054–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khuddus, M.A.; Pepine, C.J.; Handberg, E.M.; Bairey Merz, C.N.; Sopko, G.; Bavry, A.A.; Denardo, S.J.; McGorray, S.P.; Smith, K.M.; Sharaf, B.L.; et al. An intravascular ultrasound analysis in women experiencing chest pain in the absence of obstructive coronary artery disease: A substudy from the National Heart, Lung and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation (WISE). J. Interv. Cardiol. 2010, 23, 511–519. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Nomenclature | Gene Name | Principal Function |
|---|---|---|
| ADAMTS13 | ADAM Metallopeptidase with Thrombospondin Type 1 Motif 13 | von Willebrand factor cleavage |
| ALOX5 | Arachidonate 5-Lipoxygenase | Leukotriene biosynthesis |
| CD31 | Platelet And Endothelial Cell Adhesion Molecule 1 | Ig-like adhesion molecule Leukocyte migration, angiogenesis, integrin activation, immunomodulation, mechanotrasduction |
| CD44 | Hyaluronan receptor | Cell–cell interactions, cell adhesion and migration |
| EDN1 | Endothelin 1 | Vasoconstrictor |
| GPX1 | Glutathione peroxidase 1 | Redox-balancer |
| HYAL2 | Hyaluronidase 2 | Hyaluronan degradation |
| ICAM1 | Intercellular Adhesion Molecule 1 | Cell proliferation, differentiation, motility, trafficking, apoptosis and tissue architecture |
| LGALS8 | Galectin 8 | Cell–cell adhesion, cell–matrix interaction, growth regulation, apoptosis, and RNA splicing |
| MMP1 | Matrix metalloproteinase 1 | ECM and molecule degradation |
| MMP2 | Matrix metalloproteinase 2 | ECM and molecule degradation; remodeling of the vasculature, angiogenesis, tissue repair, inflammation, and atherosclerotic plaque rupture |
| MMP9 | Matrix metalloproteinase 9 | ECM and molecule degradation; leukocyte migration |
| NOS3 | Endothelial nitric oxide synthase | Implication in vascular smooth muscle relaxation |
| PI16 | Peptidase Inhibitor 16 | Cardiomyocyte growth inhibition |
| PLA2G7 | Phospholipase A2 Group VII | Platelet-activating factor (PAF) activity modulation |
| SOD1 | Superoxide dismutase 1 | Superoxide anion radical destruction |
| TFRC | Transferrin Receptor | Cell surface receptor for cellular iron uptake |
| TIMP1 | TIMP Metallopeptidase Inhibitor 1 | Cell proliferation and potential an anti-apoptotic function |
| TNF | Tumor Necrosis Factor | Cell apoptosis, proliferation, differentiation, lipid metabolism, and coagulation. Multifunctional proinflammatory cytokine |
| VCAM1 | Vascular cell adhesion molecule 1 | Cell–cell recognition, mediates leukocyte-endothelial cell adhesion |
| VEGFA | Vascular endothelial growth factor A | Vascular endothelial cell proliferation and migration. Angiogenesis |
| Gene Name | Sequence (5′→3′) | Length | Reference |
|---|---|---|---|
| ADAMTS13 | ATGTCGTGGCTGGGAAGATG | 20 | NM_139026.6 |
| GCCATACCGCCTGTAAACCT | 20 | ||
| ALOX5 | GAGAAGCACCTGCTGGACAA | 20 | NM_000698.5 |
| CGTCCACAGTCACGTCGTAT | 20 | ||
| B2M | AGGACTGGTCTTTCTATCTCTTGT | 24 | NM_004048.4 |
| ACCTCCATGATGCTGCTTACA | 21 | ||
| CD31 | GTGCAGTACACGGAAGTTCAAG | 22 | NM_000442.5 |
| TTTCCACGGCATCAGGGACA | 20 | ||
| CD44 | CAGCAAACAACACAGGGGTG AGGTGGAGCTGAAGCATTGA | 20 20 | NM_001202555.2 |
| EDN1 | AACCAGGTCGGAGACCATGA TCACCAATGTGCTCGGTTGT | 20 20 | NM_001168319.2 |
| GPX1 | ACCCGGCACTTTATTAGTGGG TACGAGGGAGGAACACCTGAT | 21 21 | NM_001329503.2 |
| HYAL2 | CCAGTCTACGTCTTCACA GCACTCTCGCCAATGGTA | 18 18 | NM_033158.4 |
| ICAM1 | CAGTCAGATACAACAGCATTTGGG ACTACAGATCAGATGCGTGGC | 24 21 | NM_000201.3 |
| LGALS8 | CTCCAATCGACAAGAAGCTGG GAATGGTGCCAACAAACGGG | 21 20 | NM_201544.4 |
| MMP1 | GAAGCTGCTTACGAATTTGCC AACAGCCCAGTACTTATTCCCT | 21 22 | NM_002421.4 |
| MMP2 | TGCTGAAGGACACACTAAAGAAGA TCCGCATGGTCTCGATGGTA | 24 20 | NM_004530.6 |
| MMP9 | CTGCAACGTGAACATCTT CTCAGAGAATCGCCAGTA | 18 18 | NM_004994.3 |
| NOS3 | ATGAGCACTGAGATCGGCAC GTCTTTCCACAGGGACGAGG | 20 20 | NM_000603.5 |
| PI16 | TGCACATGAGATGGGACGAG AGGTTGTAGTGCTCACGCTC | 20 20 | NM 153370.3 |
| PLA2G7 | CTTGGAACACACTGGCTTATGG TGCAGGAGTTGTCATTGAACC | 22 21 | NM_005084.4 |
| SOD1 | TGCAGGTCCTCACTTTAATCCTC AGTCACATTGCCCAAGTCTCC | 23 21 | NM_000454.5 |
| TFRC | AGCATTCCCGAAATCTGTTGT GGCCTGAGTTTACAGTGGCT | 21 20 | NM_003234.4 |
| TIMP1 | TTCTGCAATTCCGACCTCGT GCTGGTATAAGGTGGTCTGGT | 20 21 | NM_003254.3 |
| TNF | CCGACTATCTCGACTTTGCC GATGTTCGTCCTCCTCACAG | 20 20 | NM_000594.4 |
| VCAM1 | CAGGCTGGAAGAAGCAGAAAG TGTCTCCTTCTTTGACACTCTCAG | 21 24 | NM_001078.4 |
| VEGFA | ATCCAATCGAGACCCTGGTG AGGATGGCTTGAAGATGTACTCG | 20 23 | NM_001025366.3 |
| INOCA (n = 18) | ObCCS (n = 20) | p-Value | |
|---|---|---|---|
| Demographic characteristics | |||
| Age, yrs | 61 ± 9 | 69 ± 9 | 0.01 * |
| Sex, male/female | 14/4 | 15/5 | 0.57 |
| BMI (kg/m2) | 27 ± 3 | 27 ± 2 | 0.67 |
| Cardiovascular risk factors | |||
| Hypertension (%) | 17 (94) | 17 (85) | 0.61 |
| Dyslipidemia (%) | 12 (67) | 16 (80) | 0.47 |
| Smoke (%) | 12 (67) | 13 (65) | 0.59 |
| Family history of IHD (%) | 8 (44) | 11 (55) | 0.75 |
| Obesity (%) | 3 (17) | 2 (10) | 0.65 |
| Diabetes (%) | 5 (28) | 3 (15) | 0.44 |
| History | |||
| Previous ACS (%) | 2 (11) | 4 (20) | 0.56 |
| Previous PCI (%) | 0 (0) | 12 (60) | <0.001 * |
| Previous CABG (%) | 0 (0) | 1 (5) | 0.53 |
| Medications (at the time of blood sampling) | |||
| Aspirin (%) | 13 (72) | 19 (95) | 0.08 |
| P2Y12 receptor inhibitors (%) | 3 (18) | 12 (63) | 0.01 * |
| ACE inhibitors (%) | 6 (33) | 7 (35) | 1 |
| ARBs (%) | 5 (28) | 7 (35) | 0.73 |
| Calcium-channel blockers (%) | 2 (18) | 2 (10) | 0.68 |
| Statins (%) | 10 (56) | 19 (95) | 0.01 * |
| β-Blockers (%) | 9 (50) | 16 (80) | 0.09 |
| Diuretic agents (%) | 5 (28) | 2 (10) | 0.22 |
| Oral antidiabetic drugs (%) | 4 (22) | 2 (10) | 0.40 |
| Anticoagulant drugs (%) | 0 (0) | 1 (5) | 1 |
| Insulin (%) | 1 (6) | 1 (5) | 1 |
| Laboratory assay | |||
| cTnI > 0.004 ng/mL | 0 (0) | 0 (0) | NA |
| Haemoglobin, g/dL | 13.3 ± 3.5 | 14.1 ± 1.5 | 0.73 |
| Lymphocyte count, 109/l | 2.1 ± 0.8 | 2.3 ± 0.8 | 0.70 |
| Platelets, 103/mL | 230 ± 66 | 212 ± 33 | 0.30 |
| Glycemia, mg/dL | 92 ± 13 | 92 ± 18 | 0.29 |
| Total cholesterol, mg/dL | 160 ± 27 | 150 ± 31 | 0.31 |
| LDL, mg/dL | 90 ± 24 | 88 ± 24 | 0.86 |
| HDL, mg/dL | 49 ± 8 | 44 ± 11 | 0.18 |
| Triglycerides, mg/dL | 104 ± 33 | 128 ± 60 | 0.17 |
| Creatinine, mg/dL | 0.89 ± 0.16 | 0.95 ± 0.18 | 0.27 |
| hs-CRP, mg/L | 3 ± 3 | 7.2 ± 1.8 | 0.72 |
| In-hospital management | |||
| Multivessel disease (%) | 0 (0) | 16 (80) | <0.001 * |
| LVEF ≥ 50% (%) | 18 (100) | 19 (95) | 1 |
| PCI for index event | 0 (0) | 15 (75) | <0.001 * |
| CABG for index event | 0 (0) | 3 (15) | 0.23 |
| OMT for index event | 18 (100) | 2 (10) | <0.001 * |
| Cut-Point | Sensitivity | Specificity | Correctly Classified | LR+ | LR− |
|---|---|---|---|---|---|
| ≥0.1807 | 100.00% | 0.00% | 42.86% | 1.0000 | |
| ≥0.1898 | 100.00% | 6.25% | 46.43% | 1.0667 | 0.0000 |
| ≥0.1954 | 100.00% | 12.50% | 50.00% | 1.1429 | 0.0000 |
| ≥0.2261 | 100.00% | 18.75% | 53.57% | 1.2308 | 0.0000 |
| ≥0.2717 | 100.00% | 25.00% | 57.14% | 1.3333 | 0.0000 |
| ≥0.2732 | 100.00% | 31.25% | 60.71% | 1.4545 | 0.0000 |
| ≥0.3037 | 100.00% | 37.50% | 64.29% | 1.6000 | 0.0000 |
| ≥0.3062 | 100.00% | 43.75% | 67.86% | 1.7778 | 0.0000 |
| ≥0.3530 | 100.00% | 50.00% | 71.43% | 2.0000 | 0.0000 |
| ≥0.3617 | 100.00% | 56.25% | 75.00% | 2.2857 | 0.0000 |
| ≥0.4059 | 100.00% | 62.50% | 78.57% | 2.6667 | 0.0000 |
| ≥0.4277 | 100.00% | 68.75% | 82.14% | 3.2000 | 0.0000 |
| ≥0.4572 | 100.00% | 75.00% | 85.71% | 4.0000 | 0.0000 |
| ≥0.4675 | 100.00% | 81.25% | 89.29% | 5.3333 | 0.0000 |
| ≥0.4715 | 100.00% | 87.50% | 92.86% | 8.0000 | 0.0000 |
| ≥0.5896 | 100.00% | 93.75% | 96.43% | 16.0000 | 0.0000 |
| ≥0.6289 | 91.67% | 93.75% | 92.86% | 14.6667 | 0.0889 |
| ≥0.681622 | 83.33% | 93.75% | 89.29% | 13.3333 | 0.1778 |
| ≥0.7401 | 75.00% | 93.75% | 85.71% | 12.0000 | 0.2667 |
| ≥0.8326 | 66.67% | 93.75% | 82.14% | 10.6667 | 0.3556 |
| ≥0.9196 | 58.33% | 93.75% | 78.57% | 9.3333 | 0.4444 |
| ≥1.209 | 50.00% | 93.75% | 75.00% | 8.0000 | 0.5333 |
| ≥2.020 | 41.67% | 93.75% | 71.43% | 6.6667 | 0.6222 |
| ≥2.179 | 41.67% | 100.00% | 75.00% | 0.5833 | |
| ≥2.62764 | 33.33% | 100.00% | 71.43% | 0.6667 | |
| ≥2.69799 | 25.00% | 100.00% | 67.86% | 0.7500 | |
| ≥3.249 | 16.67% | 100.00% | 64.29% | 0.8333 | |
| ≥4.971 | 8.33% | 100.00% | 60.71% | 0.9167 | |
| >4.971 | 0.00% | 100.00% | 57.14% | 1.0000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonanni, A.; d’Aiello, A.; Pedicino, D.; Di Sario, M.; Vinci, R.; Ponzo, M.; Ciampi, P.; Lo Curto, D.; Conte, C.; Cribari, F.; et al. Molecular Hallmarks of Ischemia with Non-Obstructive Coronary Arteries: The “INOCA versus Obstructive CCS” Challenge. J. Clin. Med. 2022, 11, 1711. https://doi.org/10.3390/jcm11061711
Bonanni A, d’Aiello A, Pedicino D, Di Sario M, Vinci R, Ponzo M, Ciampi P, Lo Curto D, Conte C, Cribari F, et al. Molecular Hallmarks of Ischemia with Non-Obstructive Coronary Arteries: The “INOCA versus Obstructive CCS” Challenge. Journal of Clinical Medicine. 2022; 11(6):1711. https://doi.org/10.3390/jcm11061711
Chicago/Turabian StyleBonanni, Alice, Alessia d’Aiello, Daniela Pedicino, Marianna Di Sario, Ramona Vinci, Myriana Ponzo, Pellegrino Ciampi, Denise Lo Curto, Cristina Conte, Francesco Cribari, and et al. 2022. "Molecular Hallmarks of Ischemia with Non-Obstructive Coronary Arteries: The “INOCA versus Obstructive CCS” Challenge" Journal of Clinical Medicine 11, no. 6: 1711. https://doi.org/10.3390/jcm11061711
APA StyleBonanni, A., d’Aiello, A., Pedicino, D., Di Sario, M., Vinci, R., Ponzo, M., Ciampi, P., Lo Curto, D., Conte, C., Cribari, F., Canonico, F., Russo, G., Montone, R. A., Trani, C., Severino, A., Crea, F., & Liuzzo, G. (2022). Molecular Hallmarks of Ischemia with Non-Obstructive Coronary Arteries: The “INOCA versus Obstructive CCS” Challenge. Journal of Clinical Medicine, 11(6), 1711. https://doi.org/10.3390/jcm11061711