
Thiol-Disulfide Homeostasis in Skin Diseases


 , and
, and 
Abstract
1. Introduction
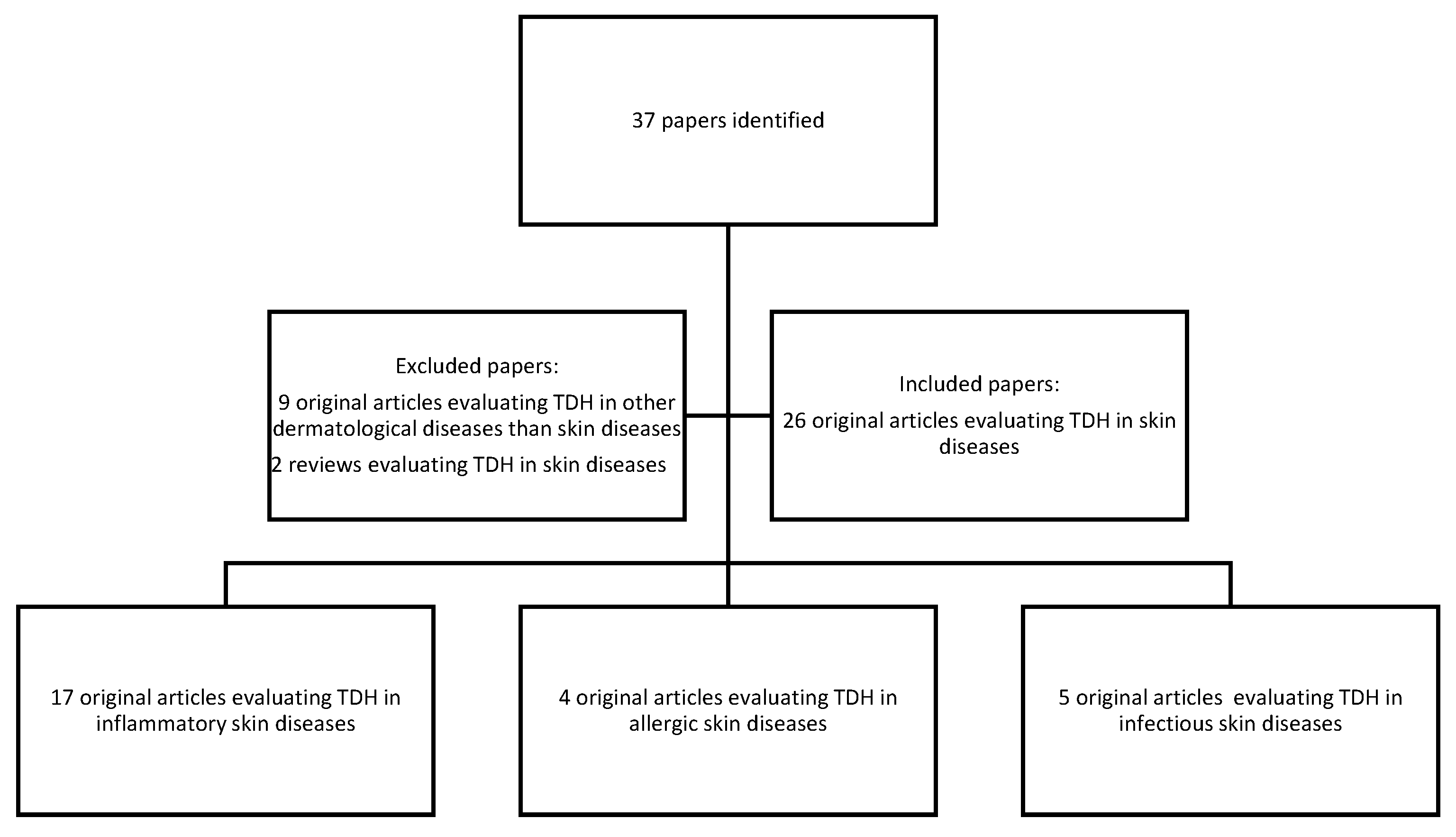
2. Materials and Methods
3. Results
4. Discussion
4.1. Inflammatory Skin Diseases
4.1.1. Psoriasis
4.1.2. Seborrheic Dermatitis
4.1.3. Atopic Dermatitis
4.1.4. Vitiligo
4.1.5. Cutaneous Lichen Planus
4.1.6. Acne Vulgaris
4.1.7. Rosacea
4.2. Allergic Skin Diseases
Urticaria
4.3. Infectious Skin Diseases
4.3.1. Warts
4.3.2. Pityriasis Rosea
4.3.3. Tinea Versicolor
5. Conclusions
Funding
Conflicts of Interest
References
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell. Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef] [PubMed]
- Poprac, P.; Jomova, K.; Simunkova, M.; Kollar, V.; Rhodes, C.J.; Valko, M. Targeting free radicals in oxidative stress-related human diseases. Trends Pharmacol. Sci. 2017, 38, 592–607. [Google Scholar] [CrossRef] [PubMed]
- Birben, E.; Sahiner, U.M.; Sackesen, C.; Erzurum, S.; Kalayci, O. Oxidative Stress and Antioxidant Defense. World Allergy Organ. J. 2012, 5, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Sies, H.; Jones, D.P. Reactive oxygen species (ROS) as pleiotropic physiological signalling agents. Nat. Rev. Mol. Cell Biol. 2020, 21, 363–383. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Rad, M.; Anil Kumar, N.V.; Zucca, P.; Varoni, E.M.; Dini, L.; Panzarini, E.; Rajkovic, J.; Tsouh Fokou, P.V.; Azzini, E.; Peluso, I.; et al. Lifestyle, Oxidative Stress, and Antioxidants: Back and Forth in the Pathophysiology of Chronic Diseases. Front. Physiol. 2020, 11, 694. [Google Scholar] [CrossRef]
- Ifeanyi, O.E. A Review on Free Radicals and Antioxidants. Int. J. Curr. Res. Med. Sci. 2018, 4, 123–133. [Google Scholar]
- Alkadi, H. A review on free radicals and antioxidants. Infect. Disord.-Drug Targets Former. Curr. Drug Targets-Infect. Disord. 2020, 20, 16–26. [Google Scholar] [CrossRef]
- He, L.; He, T.; Farrar, S.; Ji, L.; Liu, T.; Ma, X. Antioxidants Maintain Cellular Redox Homeostasis by Elimination of Reactive Oxygen Species. Cell. Physiol. Biochem. 2017, 44, 532–553. [Google Scholar] [CrossRef]
- Mates, J.M. Effects of antioxidant enzymes in the molecular control of reactive oxygen species toxicology. Toxicology 2000, 153, 83–104. [Google Scholar] [CrossRef]
- Pisoschi, A.M.; Pop, A. The role of antioxidants in the chemistry of oxidative stress: A review. Eur. J. Med. Chem. 2015, 97, 55–74. [Google Scholar] [CrossRef]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxid. Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, S.R.; Ene, C.D.; Tampa, M.; Matei, C.; Benea, V.; Nicolae, I. Oxidative Stress- related Markers and Alopecia Areata Through Latex Turbidimetric Immunoassay Method. Mater. Plast. 2016, 53, 522–526. [Google Scholar]
- Otal, Y.; Kahraman, F.A.; Haydar, F.G.; Erel, Ö. Dynamic thiol/disulfide homeostasis as oxidative stress marker in diabetic ketoacidosis. Turk. J. Med. Sci. 2021, 51, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Erel, Ö.; Erdoğan, S. Thiol-disulfide homeostasis: An integrated approach with biochemical and clinical aspects. Turk. J. Med. Sci. 2020, 50, 1728–1738. [Google Scholar] [CrossRef] [PubMed]
- Koca, A.O.; Dağdeviren, M.; Akkan, T.; Ateş, İ.; Neşelioğlu, S.; Erel, Ö.; Altay, M. Dynamic thiol/disulfide homeostasis and oxidant status in patients with hypoparathyroidism. J. Med. Biochem. 2020, 39, 231. [Google Scholar]
- Kükürt, A.; Gelen, V.; Başer, Ö.F.; Deveci, H.A.; Karapehlivan, M. Thiols: Role in oxidative stress-related disorders. In Lipid Peroxidation; IntechOpen: London, UK, 2021. [Google Scholar]
- Osik, N.A.; Zelentsova, E.A.; Tsentalovich, Y.P. Kinetic studies of antioxidant properties of ovothiol A. Antioxidants 2021, 10, 1470. [Google Scholar] [CrossRef] [PubMed]
- Nagy, P. Kinetics and Mechanisms of Thiol–Disulfide Exchange Covering Direct Substitution and Thiol Oxidation-Mediated Pathways. Antioxid. Redox Signal. 2013, 18, 1623–1641. [Google Scholar] [CrossRef]
- Yüksel, M.; Ülfer, G. Evaluation of thiol/disulfide homeostasis in patients with pityriasis rosea. Cutan. Ocul. Toxicol. 2019, 38, 338–343. [Google Scholar] [CrossRef]
- Erel, O.; Neselioglu, S. A novel and automated assay for thiol/disulphide homeostasis. Clin. Biochem. 2014, 47, 326–332. [Google Scholar] [CrossRef]
- Sezgin, B.; Pirinççi, F.; Camuzcuoğlu, A.; Şahin, E.A.; Erel, Ö.; Neşelioğlu, S.; Camuzcuoğlu, H. Evaluation of Dynamic Thiol-Disulfide Balance in Preinvasive Lesions of the Cervix. In Archives of Gynecology and Obstetrics; In Review; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar]
- Cakina, S.; Aydın, B.; Beyazit, F. Evaluation of thiol/disulfide homeostasis in patients with gestational diabetes mellitus. Gynecol. Endocrinol. 2020, 36, 1006–1009. [Google Scholar] [CrossRef]
- Akoglu, G.; Neselioglu, S.; Karaismailoglu, E.; Aktas, A.; Erel, O. Plasma thiol levels are associated with disease severity in nonsegmental vitiligo. Indian J. Dermatol. 2018, 63, 323. [Google Scholar] [CrossRef] [PubMed]
- Sener, S.; Akbas, A.; Kilinc, F.; Baran, P.; Erel, O.; Aktas, A. Thiol/disulfide homeostasis as a marker of oxidative stress in rosacea: A controlled spectrophotometric study. Cutan. Ocul. Toxicol. 2019, 38, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Emre, S.; Demirseren, D.D.; Alisik, M.; Aktas, A.; Neselioglu, S.; Erel, O. Dynamic thiol/disulfide homeostasis and effects of smoking on homeostasis parameters in patients with psoriasis. Cutan. Ocul. Toxicol. 2017, 36, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Kilic, A.; Yorulmaz, A.; Erdogan, S.; Cakmak, S.K.; Guney, E.; Sen, O.; Erel, O. An evaluation of thiol/disulphide homeostasis in patients with psoriasis. Postepy Dermatol. Alergol. 2017, 34, 464–467. [Google Scholar] [CrossRef]
- Aksoy, M.; Kirmit, A. Thiol/disulphide balance in patients with psoriasis. Adv. Dermatol. Allergol. Dermatol. Alergol. 2020, 37, 52–55. [Google Scholar] [CrossRef]
- Demir Pektas, S.; Pektas, G.; Tosun, K.; Dogan, G.; Neselioglu, S.; Erel, O. Evaluation of Erythroid Disturbance and Thiol-Disulphide Homeostasis in Patients with Psoriasis. BioMed. Res. Int. 2018, 2018, 9548252. [Google Scholar] [CrossRef]
- Üstüner, P.; Balevi, A.; Özdemir, M.; Olmusçelik, O.; Ülfer, G.; Yiğitbaşı, T. The role of thiol/disulfide homeostasis in psoriasis: Can it be a new marker for inflammation? Turk. Arch. Dermatol. Venereol. 2018, 52, 120–125. [Google Scholar] [CrossRef]
- Emre, S.; Kalkan, G.; Erdoğan, S.; Aktaş, A.; Ergin, M. Dynamic Thiol/Disulfide Balance in Patients with Seborrheic Dermatitis: A Case-Control Study. Saudi J. Med. Med. Sci. 2020, 8, 12–16. [Google Scholar] [CrossRef]
- Uysal, P.; Avcil, S.; Neşelioğlu, S.; Biçer, C.; Çatal, F. Association of oxidative stress and dynamic thiol-disulphide homeostasis with atopic dermatitis severity and chronicity in children: A prospective study. Clin. Exp. Dermatol. 2018, 43, 124–130. [Google Scholar] [CrossRef]
- Karacan, G.; Ercan, N.; Bostanci, I.; Alisik, M.; Erel, O. A novel oxidative stress marker of atopic dermatitis in infants: Thiol–disulfide balance. Arch. Dermatol. Res. 2020, 312, 697–703. [Google Scholar] [CrossRef]
- Aksoy, M.; Çelik, H. Dynamic thiol/disulphide homeostasis in vitiligo patients. Adv. Dermatol. Allergol. Dermatol. Alergol. 2018, 35, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Pektaş, G.; Pektaş, S.D.; Öztekin, A.; Öztekin, C.; Neşelioğlu, S.; Erel, Ö.; Sadi, G. Dynamic thiol/disulfide homeostasis in serum of patients with generalized vitiligo. Arch. Biol. Sci. 2019, 71, 55–62. [Google Scholar] [CrossRef]
- Annan, D.S. Assessment of thiol level in cases of Non-segmental vitiligo. Int. J. Dermatol. Venereol. Lepr. Sci. 2019, 2, 10–12. [Google Scholar] [CrossRef]
- Kalkan, G.; Emre, S.; Alisik, M.; Aktaş, A.; Baran, P. Dynamic thiol/disulfide homeostasis in patients with lichen planus. J. Clin. Lab. Anal. 2019, 33, e22642. [Google Scholar] [CrossRef]
- Mitran, M.I.; Nicolae, I.; Tampa, M.; Mitran, C.I.; Caruntu, C.; Sarbu, M.I.; Ene, C.D.; Matei, C.; Georgescu, S.R.; Popa, M.I. Reactive Carbonyl Species as Potential Pro-Oxidant Factors Involved in Lichen Planus Pathogenesis. Metabolites 2019, 9, 213. [Google Scholar] [CrossRef]
- Gurel, G.; Karadol, M.; Bal, C.; Iptec, B.; Çölgeçen, E. Evaluation of thiol/disulfide homeostasis in patients with acne vulgaris. Ann. Clin. Anal. Med. 2019, 10, 166–169. [Google Scholar]
- Demir Pektas, S.; Cinar, N.; Pektas, G.; Akbaba, G.; Kara, A.; Hancer, H.S.; Demircioglu Duman, D.; Neselioglu, S.; Erel, O.; Yazgan Aksoy, D. Thiol/disulfide homeostasis and its relationship with insulin resistance in patients with rosacea. J. Cosmet. Dermatol. 2021, 11, 14477. [Google Scholar] [CrossRef]
- Akbas, A.; Kilinc, F.; Sener, S.; Aktaş, A.; Baran, P.; Ergin, M. Investigation of thiol-disulphide balance in patients with acute urticaria and chronic spontaneous urticaria. Cutan. Ocul. Toxicol. 2017, 36, 205–210. [Google Scholar] [CrossRef]
- Akdag, S.; Ozmen, S.; Ercan, N.; Bostanci, I.; Neselioglu, S. Assessment of thiol/disulphide homoeostasis and ischaemia-modified albumin and their relationship with disease severity in children with chronic urticaria. Cutan. Ocul. Toxicol. 2020, 39, 269–273. [Google Scholar] [CrossRef]
- Aydin, İ.E.; Savrun, Ş.T.; Savrun, A.; Önder, S.; NeşeliOğlu, S.; Erel, Ö.; Kaşko Arici, Y. Assessment of oxidative stress with thiol disulfide homeostasis and ischemia-modifıed albumin level in acute urticaria. Middle Black Sea J. Health Sci. 2021, 7, 115–121. [Google Scholar] [CrossRef]
- Matei, C.; Georgescu, S.R.; Nicolae, I.; Ene, C.D.; Mitran, C.I.; Mitran, M.I. Variations of Thiol–Disulfide Homeostasis Parameters after Treatment with H1-Antihistamines in Patients with Chronic Spontaneous Urticaria. J. Clin. Med. 2021, 10, 2980. [Google Scholar] [CrossRef] [PubMed]
- Erturan, I.; Kumbul Doğuç, D.; Korkmaz, S.; Büyükbayram, H.I.; Yıldırım, M.; Kocabey Uzun, S. Evaluation of oxidative stress in patients with recalcitrant warts. J. Eur. Acad. Dermatol. Venereol. JEADV 2019, 33, 1952–1957. [Google Scholar] [CrossRef] [PubMed]
- Mitran, C.I.; Mitran, M.I.; Popa, G.L. Molecular Targets and Oxidative Stress Biomarkers in HPV Infection. Rom. Arch. Microbiol. Immunol. 2021, 80, 164–172. [Google Scholar] [CrossRef]
- SCITECH—Research of Thiol-Disulphide Balance in Patients with Pityriasis Rosea—Dermatology Clinics and Research (ISSN:2380-5609). Available online: https://www.scitcentral.com/article/19/177/Research-of-Thiol-Disulphide-Balance-in-Patients-with-Pityriasis-Rosea (accessed on 18 May 2021).
- Kilinc, F.; Akbas, A.; Sener, S.; Ergin, M.; Baran, P.; Metin, A. The effect of tinea versicolor on thiol/disulphide homeostasis. Postepy Dermatol. Alergol. 2018, 35, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Bickers, D.R.; Athar, M. Oxidative Stress in the Pathogenesis of Skin Disease. J. Investig. Dermatol. 2006, 126, 2565–2575. [Google Scholar] [CrossRef] [PubMed]
- Nicolae, I.; Ene, C.D.; Georgescu, S.R.; Tampa, M.; Matei, C.; Ceausu, E. Effects of UV Radiation and Oxidative DNA Adduct 8-hydroxy-2’-deoxiguanosine on the Skin Diseases. REV CHIM 2014, 65, 1036–1041. [Google Scholar]
- Emre, S.; Akoglu, G.; Metin, A.; Demirseren, D.D.; Isikoglu, S.; Oztekin, A.; Erel, O. The oxidant and antioxidant status in pityriasis rosea. Indian J. Dermatol. 2016, 61, 118. [Google Scholar] [CrossRef] [PubMed]
- Demir Pektaş, S.; Alataş, E.T.; Doğan, G.; Neşelioğlu, S.; Erel, Ö. A Marker for Evaluation of Oxidative Stress in Patients with Alopecia Areta: Thiol-Disulphide Homeostasis. Meandros Med. Dent. J. 2018, 19, 205–210. [Google Scholar] [CrossRef]
- Rendon, A.; Schäkel, K. Psoriasis pathogenesis and treatment. Int. J. Mol. Sci. 2019, 20, 1475. [Google Scholar] [CrossRef]
- Schleicher, S.M. Psoriasis. Clin. Podiatr. Med. Surg. 2016, 33, 355–366. [Google Scholar] [CrossRef]
- Hawkes, J.E.; Chan, T.C.; Krueger, J.G. Psoriasis pathogenesis and the development of novel targeted immune therapies. J. Allergy Clin. Immunol. 2017, 140, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.-H.; Brembilla, N.C. Unmet Needs in the Field of Psoriasis: Pathogenesis and Treatment. Clin. Rev. Allergy Immunol. 2018, 55, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Huang, T. Oxidative stress in psoriasis and potential therapeutic use of antioxidants. Free Radic. Res. 2016, 50, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Pleńkowska, J.; Gabig-Cimińska, M.; Mozolewski, P. Oxidative Stress as an Important Contributor to the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2020, 21, 6206. [Google Scholar] [CrossRef] [PubMed]
- Simeoni, L.; Bogeski, I. Redox regulation of T-cell receptor signaling. Biol. Chem. 2015, 396, 555–568. [Google Scholar] [CrossRef]
- Barygina, V.; Becatti, M.; Soldi, G.; Prignano, F.; Lotti, T.; Nassi, P.; Wright, D.; Taddei, N.; Fiorillo, C. Altered redox status in the blood of psoriatic patients: Involvement of NADPH oxidase and role of anti-TNF-α therapy. Redox Rep. 2013, 18, 100–106. [Google Scholar] [CrossRef]
- Drewa, G.; Krzyżyńska-Malinowska, E.; Woźniak, A.; Protas-Drozd, F.; Mila-Kierzenkowska, C.; Rozwodowska, M.; Kowaliszyn, B.; Czajkowski, R. Activity of superoxide dismutase and catalase and the level of lipid peroxidation products reactive with TBA in patients with psoriasis. Med. Sci. Monit. 2002, 8, BR338–BR343. [Google Scholar]
- Tampa, M.; Nicolae, I.; Ene, C.D.; Sarbu, I.; Matei, C.; Georgescu, S.R. Vitamin C and Thiobarbituric Acid Reactive Substances (TBARS) in Psoriasis Vulgaris Related to Psoriasis Area Severity Index (PASI). Rev. Chim. 2017, 68, 43–47. [Google Scholar] [CrossRef]
- Kadam, D.P.; Suryakar, A.N.; Ankush, R.D.; Kadam, C.Y.; Deshpande, K.H. Role of oxidative stress in various stages of psoriasis. Indian J. Clin. Biochem. 2010, 25, 388–392. [Google Scholar] [CrossRef]
- Kute, P.; Muddeshwar, M.; Sonare, A. Pro-Oxidants and Anti-Oxidant Status in Patients of Psoriasis with Relation to Smoking and Alcoholism. J. Evol. Med. Dent. Sci. 2019, 8, 2677–2681. [Google Scholar]
- Peluso, I.; Cavaliere, A.; Palmery, M. Plasma total antioxidant capacity and peroxidation biomarkers in psoriasis. J. Biomed. Sci. 2016, 23, 52. [Google Scholar] [CrossRef] [PubMed]
- Magnus, I.A. Observations on the thiol content of abnormal stratum corneum in psoriasis and other conditions. Br. J. Dermatol. 1956, 68, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.T.; Watson, W.H.; Kirlin, W.G.; Ziegler, T.R.; Jones, D.P. Oxidation of the glutathione/glutathione disulfide redox state is induced by cysteine deficiency in human colon carcinoma HT29 cells. J. Nutr. 2002, 132, 2303–2306. [Google Scholar] [CrossRef] [PubMed]
- Laborde, E. Glutathione transferases as mediators of signaling pathways involved in cell proliferation and cell death. Cell Death Differ. 2010, 17, 1373–1380. [Google Scholar] [CrossRef]
- Relhan, V.; Gupta, S.K.; Dayal, S.; Pandey, R.; Lal, H. Blood Thiols and Malondialdehyde Levels in Psoriasis. J. Dermatol. 2002, 29, 399–403. [Google Scholar] [CrossRef]
- Bakardzhiev, I. New Insights into the Etiopathogenesis of Seborrheic Dermatitis. J. Clin. Res. Dermatol. 2017, 4, 1–5. [Google Scholar] [CrossRef]
- Adalsteinsson, J.A.; Kaushik, S.; Muzumdar, S.; Guttman-Yassky, E.; Ungar, J. An update on the microbiology, immunology and genetics of seborrheic dermatitis. Exp. Dermatol. 2020, 29, 481–489. [Google Scholar] [CrossRef]
- Wikramanayake, T.C.; Borda, L.J.; Miteva, M.; Paus, R. Seborrheic dermatitis—Looking beyond Malassezia. Exp. Dermatol. 2019, 28, 991–1001. [Google Scholar] [CrossRef]
- Dessinioti, C.; Katsambas, A. Seborrheic dermatitis: Etiology, risk factors, and treatments: Facts and controversies. Clin. Dermatol. 2013, 31, 343–351. [Google Scholar] [CrossRef]
- Emre, S.; Metin, A.; Demirseren, D.D.; Akoglu, G.; Oztekin, A.; Neselioglu, S.; Erel, O. The association of oxidative stress and disease activity in seborrheic dermatitis. Arch. Dermatol. Res. 2012, 304, 683–687. [Google Scholar] [CrossRef]
- Jahan, I.; Islam, M.R.; Islam, M.R.; Ali, R.; Rahman, S.M.M.; Nahar, Z.; Hasnat, A.; Islam, M.S. Altered serum elements, antioxidants, MDA, and immunoglobulins are associated with an increased risk of seborrheic dermatitis. Heliyon 2021, 7, e06621. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, P.; Arican, O.; Belge Kurutas, E.; Karakas, T.; Kabakci, B. Oxidative stress in patients with scalp seborrheic dermatitis. Acta Dermatovenerol. Croat. ADC 2013, 21, 80–85. [Google Scholar] [PubMed]
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef]
- Bertino, L.; Guarneri, F.; Cannavò, S.P.; Casciaro, M.; Pioggia, G.; Gangemi, S. Oxidative Stress and Atopic Dermatitis. Antioxidants 2020, 9, 196. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, O.; Bacchetti, T.; Ferretti, G.; Molinelli, E.; Rizzetto, G.; Bellachioma, L.; Offidani, A. Oxidative Stress and Alterations of Paraoxonases in Atopic Dermatitis. Antioxidants 2021, 10, 697. [Google Scholar] [CrossRef]
- Amin, M.N.; Liza, K.F.; Sarwar, M.S.; Ahmed, J.; Adnan, M.T.; Chowdhury, M.I.; Hossain, M.Z.; Islam, M.S. Effect of lipid peroxidation, antioxidants, macro minerals and trace elements on eczema. Arch. Dermatol. Res. 2015, 307, 617–623. [Google Scholar] [CrossRef]
- Pecorelli, A.; Woodby, B.; Prieux, R.; Valacchi, G. Involvement of 4-hydroxy-2-nonenal in pollution-induced skin damage. BioFactors 2019, 45, 536–547. [Google Scholar] [CrossRef]
- Tsukahara, H.; Shibata, R.; Ohshima, Y.; Todoroki, Y.; Sato, S.; Ohta, N.; Hiraoka, M.; Yoshida, A.; Nishima, S.; Mayumi, M. Oxidative stress and altered antioxidant defenses in children with acute exacerbation of atopic dermatitis. Life Sci. 2003, 72, 2509–2516. [Google Scholar] [CrossRef]
- Chen, P.-Y.; Chen, C.-W.; Su, Y.-J.; Chang, W.-H.; Kao, W.-F.; Yang, C.-C.; Wang, I.-J. Associations between Levels of Urinary Oxidative Stress of 8-OHdG and Risk of Atopic Diseases in Children. Int. J. Environ. Res. Public. Health 2020, 17, 8207. [Google Scholar] [CrossRef]
- Peroni, D.G.; Bodini, A.; Corradi, M.; Coghi, A.; Boner, A.L.; Piacentini, G.L. Markers of oxidative stress are increased in exhaled breath condensates of children with atopic dermatitis: Exhaled breath condensates in atopic dermatitis. Br. J. Dermatol. 2012, 166, 839–843. [Google Scholar] [CrossRef]
- Niwa, Y.; Sumi, H.; Kawahira, K.; Terashima, T.; Nakamura, T.; Akamatsu, H. Protein oxidative damage in the stratum corneum: Evidence for a link between environmental oxidants and the changing prevalence and nature of atopic dermatitis in Japan. Br. J. Dermatol. 2003, 149, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Sivaranjani, N. Role of Reactive Oxygen Species and Antioxidants in Atopic Dermatitis. J. Clin. Diagn. Res. 2013, 7, 2683. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.-Y.; Chung, J.; Kim, M.-K.; Kwon, S.O.; Cho, B.-H. Antioxidant nutrient intakes and corresponding biomarkers associated with the risk of atopic dermatitis in young children. Eur. J. Clin. Nutr. 2010, 64, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Uysal, P.; Avcil, S.; Abas, B.İ.; Yenisey, Ç. Evaluation of Oxidant–Antioxidant Balance in Children with Atopic Dermatitis: A Case–Control Study. Am. J. Clin. Dermatol. 2016, 17, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Devadasan, S.; Sarkar, R.; Barman, K.D.; Kaushik, S. Role of Serum Melatonin and Oxidative Stress in Childhood Atopic Dermatitis: A Prospective Study. Indian Dermatol. Online J. 2020, 11, 925–929. [Google Scholar] [PubMed]
- Frisoli, M.L.; Essien, K.; Harris, J.E. Vitiligo: Mechanisms of Pathogenesis and Treatment. Annu. Rev. Immunol. 2020, 38, 621–648. [Google Scholar] [CrossRef] [PubMed]
- Rashighi, M.; Harris, J.E. Vitiligo Pathogenesis and Emerging Treatments. Dermatol. Clin. 2017, 35, 257–265. [Google Scholar] [CrossRef]
- Speeckaert, R.; Dugardin, J.; Lambert, J.; Lapeere, H.; Verhaeghe, E.; Speeckaert, M.M.; van Geel, N. Critical appraisal of the oxidative stress pathway in vitiligo: A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1089–1098. [Google Scholar] [CrossRef]
- Speeckaert, R.; Speeckaert, M.; De Schepper, S.; van Geel, N. Biomarkers of disease activity in vitiligo: A systematic review. Autoimmun. Rev. 2017, 16, 937–945. [Google Scholar] [CrossRef]
- Jain, A.; Mal, J.; Mehndiratta, V.; Chander, R.; Patra, S.K. Study of Oxidative Stress in Vitiligo. Indian J. Clin. Biochem. 2011, 26, 78–81. [Google Scholar] [CrossRef][Green Version]
- Cui, T.; Zhang, W.; Li, S.; Chen, X.; Chang, Y.; Yi, X.; Kang, P.; Yang, Y.; Chen, J.; Liu, L.; et al. Oxidative Stress–Induced HMGB1 Release from Melanocytes: A Paracrine Mechanism Underlying the Cutaneous Inflammation in Vitiligo. J. Investig. Dermatol. 2019, 139, 2174–2184.e4. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, S.; Li, C. Perspectives of New Advances in the Pathogenesis of Vitiligo: From Oxidative Stress to Autoimmunity. Med. Sci. Monit. 2019, 25, 1017–1023. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhu, G.; Yang, Y.; Jian, Z.; Guo, S.; Dai, W.; Shi, Q.; Ge, R.; Ma, J.; Liu, L.; et al. Oxidative stress drives CD8 + T-cell skin trafficking in patients with vitiligo through CXCL16 upregulation by activating the unfolded protein response in keratinocytes. J. Allergy Clin. Immunol. 2017, 140, 177–189.e9. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Lundbäck, P.; Ottosson, L.; Erlandsson-Harris, H.; Venereau, E.; Bianchi, M.E.; Al-Abed, Y.; Andersson, U.; Tracey, K.J. Redox modifications of cysteine residues regulate the cytokine activity of HMGB1. Mol. Med. 2021, 27, 58. [Google Scholar] [CrossRef]
- Laddha, N.C.; Dwivedi, M.; Mansuri, M.S.; Gani, A.R.; Ansarullah, M.; Ramachandran, A.V.; Dalai, S.; Begum, R. Vitiligo: Interplay between oxidative stress and immune system. Exp. Dermatol. 2013, 22, 245–250. [Google Scholar] [CrossRef]
- Yang, Y.; Li, S.; Zhu, G.; Zhang, Q.; Wang, G.; Gao, T.; Li, C.; Wang, L.; Jian, Z. A similar local immune and oxidative stress phenotype in vitiligo and halo nevus. J. Dermatol. Sci. 2017, 87, 50–59. [Google Scholar] [CrossRef]
- Denat, L.; Kadekaro, A.L.; Marrot, L.; Leachman, S.A.; Abdel-Malek, Z.A. Melanocytes as Instigators and Victims of Oxidative Stress. J. Invest. Dermatol. 2014, 134, 1512–1518. [Google Scholar] [CrossRef]
- Kishida, R.; Kasai, H.; Aspera, S.M.; Arevalo, R.L.; Nakanishi, H. Branching Reaction in Melanogenesis: The Effect of Intramolecular Cyclization on Thiol Binding. J. Electron. Mater. 2017, 46, 3784–3788. [Google Scholar] [CrossRef]
- Mathachan, S.R.; Khurana, A.; Gautam, R.K.; Kulhari, A.; Sharma, L.; Sardana, K. Does oxidative stress correlate with disease activity and severity in vitiligo? An analytical study. J. Cosmet. Dermatol. 2021, 20, 352–359. [Google Scholar] [CrossRef]
- Zheleva, A.; Nikolova, G.; Karamalakova, Y.; Hristakieva, E.; Lavcheva, R.; Gadjeva, V. Comparative study on some oxidative stress parameters in blood of vitiligo patients before and after combined therapy. Regul. Toxicol. Pharmacol. 2018, 94, 234–239. [Google Scholar] [CrossRef]
- Xiao, B.; Shi, M.; Chen, H.; Cui, S.; Wu, Y.; Gao, X.-H.; Chen, H.-D. Glutathione Peroxidase Level in Patients with Vitiligo: A Meta-Analysis. BioMed. Res. Int. 2016, 2016, 3029810. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Satyam, A.; Gupta, S.; Sharma, V.K.; Sharma, A. Circulatory levels of antioxidants and lipid peroxidation in Indian patients with generalized and localized vitiligo. Arch. Dermatol. Res. 2009, 301, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.W.; Nam, K.M.; Choi, H.R.; Huh, S.Y.; Kim, S.W.; Youn, S.W.; Huh, C.H.; Park, K.C. Erythrocyte Malondialdehyde and Glutathione Levels in Vitiligo Patients. Ann. Dermatol. 2010, 22, 279. [Google Scholar] [CrossRef] [PubMed]
- Dammak, I.; Boudaya, S.; Ben Abdallah, F.; Turki, H.; Attia, H.; Hentati, B. Antioxidant enzymes and lipid peroxidation at the tissue level in patients with stable and active vitiligo. Int. J. Dermatol. 2009, 48, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Sravani, P.V.; Babu, N.K.; Gopal, K.V.T.; Rao, G.; Rao, A.R.; Moorthy, B.; Rao, T.R. Determination of oxidative stress in vitiligo by measuring superoxide dismutase and catalase levels in vitiliginous and non-vitiliginous skin. Indian J. Dermatol. Venereol. Leprol. 2009, 75, 268–271. [Google Scholar]
- Tziotzios, C.; Lee, J.Y.W.; Brier, T.; Saito, R.; Hsu, C.-K.; Bhargava, K.; Stefanato, C.M.; Fenton, D.A.; McGrath, J.A. Lichen planus and lichenoid dermatoses. J. Am. Acad. Dermatol. 2018, 79, 789–804. [Google Scholar] [CrossRef]
- Georgescu, S.; Tampa, M.; Mitran, M.; Mitran, C.; Sarbu, M.; Nicolae, I.; Matei, C.; Caruntu, C.; Neagu, M.; Popa, M. Potential pathogenic mechanisms involved in the association between lichen planus and hepatitis C virus infection (Review). Exp. Ther. Med. 2019, 17, 1045–1051. [Google Scholar] [CrossRef]
- Pietschke, K.; Holstein, J.; Meier, K.; Schäfer, I.; Müller-Hermelink, E.; Gonzalez-Menendez, I.; Quintanilla-Martinez, L.; Ghoreschi, F.C.; Solimani, F.; Ghoreschi, K. The inflammation in cutaneous lichen planus is dominated by IFN-ϒ and IL-21—A basis for therapeutic JAK1 inhibition. Exp. Dermatol. 2021, 30, 262–270. [Google Scholar] [CrossRef]
- Sezer, E.; Ozugurlu, F.; Ozyurt, H.; Sahin, S.; Etikan, I. Lipid peroxidation and antioxidant status in lichen planus. Clin. Exp. Dermatol. Clin. Dermatol. 2007, 32, 430–434. [Google Scholar] [CrossRef]
- Sander, C.; Cooper, S.; Ali, I.; Dean, D.; Thiele, J.; Wojnarowska, F. Decreased antioxidant enzyme expression and increased oxidative damage in erosive lichen planus of the vulva. BJOG Int. J. Obstet. Gynaecol. 2005, 112, 1572–1575. [Google Scholar] [CrossRef]
- Matei, C.; Tampa, M.; Ion, R.M.; Neagu, M.; Constantin, C. Photodynamic properties of aluminium sulphonated phthalocyanines in human displazic oral keratinocytes experimental model. Dig. J. Nanomater. Biostructures 2012, 7, 1535–1547. [Google Scholar]
- Scrobotă, I.; Mocan, T.; Cătoi, C.; Bolfă, P.; Mureşan, A.; Băciuţ, G. Histopathological aspects and local implications of oxidative stress in patients with oral lichen planus. Rom. J. Morphol. Embryol. 2011, 52, 1305–1309. [Google Scholar] [PubMed]
- Shakibaei, M.; Schulze-Tanzil, G.; Takada, Y.; Aggarwal, B.B. Redox regulation of apoptosis by members of the TNF superfamily. Antioxid. Redox Signal. 2005, 7, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Karim, M.; Ahmed, N.; Abdel-Mawgoud, A. Oxidative Stress in Classic Type Lichen Planus. Bull. Egypt. Soc. Physiol. Sci. 2012, 32, 125–134. [Google Scholar] [CrossRef]
- Hassan, I.; Keen, A.; Majid, S.; Hassan, T. Evaluation of the antioxidant status in patients of lichen planus in Kashmir valley—A hospital based study. J. Saudi Soc. Dermatol. Dermatol. Surg. 2013, 17, 13–16. [Google Scholar] [CrossRef]
- Chakraborti, G.; Biswas, R.; Chakraborti, S.; Sen, P.K. Altered Serum Uric Acid Level in Lichen Planus Patients. Indian J. Derm. 2014, 59, 558–561. [Google Scholar] [CrossRef]
- Barikbin, B.; Yousefi, M.; Rahimi, H.; Hedayati, M.; Razavi, S.M.; Lotfi, S. Antioxidant status in patients with lichen planus. Clin. Exp. Dermatol. 2011, 36, 851–854. [Google Scholar] [CrossRef]
- Gollnick, H.P.M. From new findings in acne pathogenesis to new approaches in treatment. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1–7. [Google Scholar] [CrossRef]
- Tan, J.K.; Gold, L.S.; Alexis, A.F.; Harper, J.C. Current Concepts in Acne Pathogenesis: Pathways to Inflammation. Sem. Cutan. Med. Surg. 2018, 37, S60–S62. [Google Scholar] [CrossRef]
- Kircik, L.H. Advances in the Understanding of the Pathogenesis of Inflammatory Acne. J. Drugs Dermatol. JDD 2016, 15, s7–s10. [Google Scholar]
- Kardeh, S.; Moein, S.; Namazi, M.R.; Kardeh, B. Evidence for the Important ¬Role of Oxidative Stress in the Pathogenesis of Acne. Galen Med. J. 2019, 8, 1291. [Google Scholar] [CrossRef]
- Al-Shobaili, H.A.; Alzolibani, A.A.; Al Robaee, A.A.; Meki, A.-R.M.A.; Rasheed, Z. Biochemical Markers of Oxidative and Nitrosative Stress in Acne Vulgaris: Correlation With Disease Activity: Oxidative and Nitrosative Stress in Acne Vulgaris. J. Clin. Lab. Anal. 2013, 27, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Mikhael, N.W.; Rezk, S.M.; Abdel Khalik, H.A.; Mowafy, M.A. Serum total thiol level in Acne Vulgaris Patients and its relation to oxidative stress. Benha J. Appl. Sci. 2021, 6, 191–197. [Google Scholar] [CrossRef]
- Ahn, C.S.; Huang, W.W. Rosacea Pathogenesis. Dermatol. Clin. 2018, 36, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Buddenkotte, J.; Steinhoff, M. Recent advances in understanding and managing rosacea. F1000Research 2018, 7, 1885. [Google Scholar] [CrossRef]
- Falay Gur, T.; Erdemir, A.V.; Gurel, M.S.; Kocyigit, A.; Guler, E.M.; Erdil, D. The investigation of the relationships of demodex density with inflammatory response and oxidative stress in rosacea. Arch. Dermatol. Res. 2018, 310, 759–767. [Google Scholar] [CrossRef]
- Takci, Z.; Bilgili, S.G.; Karadag, A.S.; Kucukoglu, M.E.; Selek, S.; Aslan, M. Decreased serum paraoxonase and arylesterase activities in patients with rosacea. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 367–370. [Google Scholar] [CrossRef]
- Tisma, V.S.; Basta-Juzbasic, A.; Jaganjac, M.; Brcic, L.; Dobric, I.; Lipozencic, J.; Tatzber, F.; Zarkovic, N.; Poljak-Blazi, M. Oxidative stress and ferritin expression in the skin of patients with rosacea. J. Am. Acad. Dermatol. 2009, 60, 270–276. [Google Scholar] [CrossRef]
- Khvoryk, D.; Yarmolik, A. Lipid peroxidation and antioxidant protection in patients with papulo-pustular rosacea. Prog. Health Sci. 2015, 5, 54–60. [Google Scholar]
- Erdogan, H.K.; Bulur, I.; Kocaturk, E.; Saracoglu, Z.N.; Alatas, O.; Bilgin, M. Advanced oxidation protein products and serum total oxidant/antioxidant status levels in rosacea. Adv. Dermatol. Allergol. 2018, 35, 304–308. [Google Scholar] [CrossRef]
- Turkmen, D. Serum bilirubin and uric acid antioxidant levels in rosacea patients. J. Cosmet. Dermatol. 2020, 19, 2717–2720. [Google Scholar] [CrossRef] [PubMed]
- Radonjic-Hoesli, S.; Hofmeier, K.S.; Micaletto, S.; Schmid-Grendelmeier, P.; Bircher, A.; Simon, D. Urticaria and Angioedema: An Update on Classification and Pathogenesis. Clin. Rev. Allergy Immunol. 2018, 54, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Asero, R.; Tedeschi, A.; Marzano, A.V.; Cugno, M. Chronic urticaria: A focus on pathogenesis. F1000Research 2017, 6, 1095. [Google Scholar] [CrossRef] [PubMed]
- Dinu, L.; Ene, C.D.; Nicolae, I.; Tampa, M.; Matei, C.; Georgescu, S.R. Serum Levels of 8-hydroxy-deoxyguanosine under the Chemicals Influence. Rev. Chim. 2014, 65, 1319–1326. [Google Scholar]
- Kudryavtseva, A.V.; Neskorodova, K.A.; Staubach, P. Urticaria in children and adolescents: An updated review of the pathogenesis and management. Pediatr. Allergy Immunol. 2019, 30, 17–24. [Google Scholar] [CrossRef]
- Kasperska-Zajac, A.; Brzoza, Z.; Polaniak, R.; Rogala, B.; Birkner, E. Markers of antioxidant defence system and lipid peroxidation in peripheral blood of female patients with chronic idiopathic urticaria. Arch. Dermatol. Res. 2007, 298, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Dilek, F.; Ozceker, D.; Ozkaya, E.; Guler, N.; Tamay, Z.; Kesgin, S.; Yazici, M.; Kocyigit, A. Oxidative Stress in Children with Chronic Spontaneous Urticaria. Oxid. Med. Cell. Longev. 2016, 2016, 3831071. [Google Scholar] [CrossRef]
- Chelombitko, M.A.; Fedorov, A.V.; Ilyinskaya, O.P.; Zinovkin, R.A.; Chernyak, B.V. Role of reactive oxygen species in mast cell degranulation. Biochem. Mosc. 2016, 81, 1564–1577. [Google Scholar] [CrossRef]
- Sagdic, A.; Sener, O.; Bulucu, F.; Karadurmus, N.; Yamanel, L.; Tasci, C.; Naharci, I.; Ocal, R.; Aydin, A. Oxidative stress status in patients with chronic idiopathic urticaria. Allergol. Immunopathol. Madr. 2011, 39, 150–153. [Google Scholar] [CrossRef]
- Kalkan, G.; Seçkin, H.Y.; Duygu, F.; Akbaş, A.; Ozyurt, H.; Sahin, M. Oxidative stress status in patients with acute urticaria. Cutan. Ocul. Toxicol. 2014, 33, 109–114. [Google Scholar] [CrossRef]
- Nettis, E.; Distaso, M.; Saitta, S.; Casciaro, M.; Cristani, M.; Saija, A.; Vacca, A.; Gangemi, S.; Minciullo, P.L. Involvement of new oxidative stress markers in chronic spontaneous urticaria. Postepy Dermatol. Alergol. 2017, 34, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Tampa, M.; Mitran, C.I.; Mitran, M.I.; Nicolae, I.; Dumitru, A.; Matei, C.; Manolescu, L.; Popa, G.L.; Caruntu, C.; Georgescu, S.R. The Role of Beta HPV Types and HPV-Associated Inflammatory Processes in Cutaneous Squamous Cell Carcinoma. J. Immunol. Res. 2020, 2020, 5701639. [Google Scholar] [CrossRef] [PubMed]
- Nada, H.A.; El-Shabrawy, M.M.; Ibrahim, S.H.; Azab, M. Measurement of serum glutathione peroxidase, catalase and superoxide dismutase concentration in patients with external anogenital warts before and after treatment with intralesional tuberculin purified protein derivative. Andrologia 2020, 52, e13661. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Gregorio, A.; Aranda-Rivera, A.K.; Ortega-Lozano, A.J.; Pedraza-Chaverri, J.; Mendoza-Hoffmann, F. Lipid metabolism and oxidative stress in HPV-related cancers. Free Radic. Biol. Med. 2021, 172, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, S.; Soltani, A.; Hashemy, S.I. Oxidative stress in cervical cancer pathogenesis and resistance to therapy. J. Cell. Biochem. 2019, 120, 6868–6877. [Google Scholar] [CrossRef]
- Nicolae, I.; Tampa, M.; Mitran, C.; Ene, C.D.; Mitran, L.; Matei, C.; Mu, A.; Pi, S.; Pop, C.S.; Georgescu, S.-R. Gamma-glutamyl transpeptidase alteration as a biomarker of oxidative stress in patients with human papillomavirus lesions following topical treatment with sinecatechins. Farmacia 2017, 65, 7. [Google Scholar]
- Cruz-Gregorio, A.; Manzo-Merino, J.; Gonzaléz-García, M.C.; Pedraza-Chaverri, J.; Medina-Campos, O.N.; Valverde, M.; Rojas, E.; Rodríguez-Sastre, M.A.; García-Cuellar, C.M.; Lizano, M. Human Papillomavirus Types 16 and 18 Early-expressed Proteins Differentially Modulate the Cellular Redox State and DNA Damage. Int. J. Biol. Sci. 2018, 14, 21–35. [Google Scholar] [CrossRef]
- Ku, J.W.K.; Gan, Y.-H. New roles for glutathione: Modulators of bacterial virulence and pathogenesis. Redox Biol. 2021, 44, 102012. [Google Scholar] [CrossRef]
- Sezgin, B.; Kinci, M.F.; Pirinççi, F.; Camuzcuoğlu, A.; Erel, Ö.; Neşelioğlu, S.; Camuzcuoğlu, H. Thiol-disulfide status of patients with cervical cancer. J. Obstet. Gynaecol. Res. 2020, 46, 2423–2429. [Google Scholar] [CrossRef]
- Cokluk, E.; Sekeroglu, M.R.; Aslan, M.; Balahoroglu, R.; Bilgili, S.G.; Huyut, Z. Determining oxidant and antioxidant status in patients with genital warts. Redox Rep. 2015, 20, 210–214. [Google Scholar] [CrossRef]
- Bali Medical Journal Published by DiscoverSys Inc. Available online: https://www.balimedicaljournal.org/index.php/bmj/article/view/1441 (accessed on 12 December 2021).
- Sasmaz, S.; Arican, O.; Kurutas, E.B. Oxidative stress in patients with nongenital warts. Mediat. Inflamm. 2005, 2005, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Arican, O.; Ozturk, P.; Kurutas, E.B.; Unsal, V. Status of oxidative stress on lesional skin surface of plantar warts: Cutaneous oxidative stress in plantar warts. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Mitran, C.I.; Nicolae, I.; Tampa, M.; Mitran, M.I.; Caruntu, C.; Sarbu, M.I.; Ene, C.D.; Matei, C.; Ionescu, A.C.; Georgescu, S.R.; et al. The Relationship between the Soluble Receptor for Advanced Glycation End Products and Oxidative Stress in Patients with Palmoplantar Warts. Med. Mex. 2019, 55, 706. [Google Scholar] [CrossRef] [PubMed]
- Villalon-Gomez, J.M. Pityriasis Rosea: Diagnosis and Treatment. Am. Fam. Physician 2018, 97, 38–44. [Google Scholar]
- Schadt, C. Pityriasis rosea. JAMA Dermatol. 2018, 154, 1496. [Google Scholar] [CrossRef]
- Drago, F.; Ciccarese, G.; Broccolo, F.; Ghio, M.; Contini, P.; Thanasi, H.; Parodi, A. The Role of Cytokines, Chemokines, and Growth Factors in the Pathogenesis of Pityriasis Rosea. Mediat. Inflamm. 2015, 2015, 438963. [Google Scholar] [CrossRef]
- Gupta, A.K.; Lyons, D.C. Pityriasis versicolor: An update on pharmacological treatment options. Expert Opin. Pharmacother. 2014, 15, 1707–1713. [Google Scholar] [CrossRef]
- Später, S.; Hipler, U.C.; Haustein, U.F.; Nenoff, P. Generation of reactive oxygen species in vitro by Malassezia yeasts. Hautarzt Z. Dermatol. Venerol. Verwandte Geb. 2009, 60, 122–127. [Google Scholar] [CrossRef]
- Kurutas, E.B.; Ozturk, P. The evaluation of local oxidative/nitrosative stress in patients with pityriasis versicolor: A preliminary study. Mycoses 2016, 59, 720–725. [Google Scholar] [CrossRef]
- Kilic, M.; Oguztuzun, S.; Karadag, A.S.; Cakir, E.; Aydin, M.; Ozturk, L. Expression of GSTM4 and GSTT1 in patients with Tinea versicolor, Tinea inguinalis and Tinea pedis infections: A preliminary study: GSTM4 and GSTT1 in dermatophytes and T. versicolor. Clin. Exp. Dermatol. 2011, 36, 590–594. [Google Scholar] [CrossRef]


{kind=link}
| Disease | Patients/ Controls | Results | Conclusion | Ref. |
|---|---|---|---|---|
| Psoriasis | 90/76 | NT-higher levels * | Thiol-disulfide balance shifted toward thiols in psoriasis patients. Elevated thiol levels may be involved in keratinocyte proliferation. | Emre et al. (2017) [25] |
| TT-higher levels * | ||||
| DS NS | ||||
| DS/NT, DS/TT and NT/TT-no data available | ||||
| Psoriasis | 92/71 | NT NS | TDH may represent a useful tool in the management of psoriasis patients. | Kilic et al. (2017) [26] |
| TT NS | ||||
| DS-lower levels ** | ||||
| DS/NT NS | ||||
| DS/TT-lower ** | ||||
| NT/TT-higher ** | ||||
| Psoriasis | 80/80 | NT-lower levels ** | The results support the involvement of oxidative stress in the pathogenesis of psoriasis. Thiol/disulfide balance shifted toward disulfides in patients with psoriasis. | Aksoy et al. (2020) [27] |
| TT-lower levels ** | ||||
| DS NS | ||||
| DS/NT-higher ** | ||||
| DS/TT-higher ** | ||||
| NT/TT-lower ** | ||||
| Psoriasis | 87/76 | NT-lower levels ** | The inflammatory process and oxidative stress encountered in psoriasis lead to the generation of pro-oxidant compounds that are neutralized by thiols, which explains the low levels of thiols. | Demir Pektas et al. (2018) [28] |
| TT NS | ||||
| DS-higher levels ** | ||||
| DS/NT-higher ** | ||||
| DS/TT-higher ** | ||||
| NT/TT-lower ** | ||||
| Psoriasis | 29/30 | NT NS | Thiol-disulfide balance shifted toward disulfides in psoriasis patients resulting in an increase in the total oxidant status that may promote chronic inflammation. | Ustuner et al. (2018) [29] |
| TT NS | ||||
| DS-higher levels * | ||||
| DS/NT NS | ||||
| DS/TT NS | ||||
| NT/TT-no data available | ||||
| Seborrheic dermatitis | 70/61 | NT-higher levels ** | High levels of total thiol may be the result of oxidative stress. Thiols may be involved in the increased cell proliferation that characterizes the disease. | Emre et al. (2020) [30] |
| TT-higher levels ** | ||||
| DS NS | ||||
| DS/NT NS | ||||
| DS/TT NS | ||||
| NT/TT NS | ||||
| Atopic dermatitis | 60/60 | NT NS | In atopic dermatitis, the balance between oxidants and antioxidants is altered. Antioxidants may be helpful in slowing the progression of the disease. | Uysal et al. (2018) [31] |
| TT NS | ||||
| DS-higher levels * | ||||
| DS/NT-lower ** | ||||
| DS/TT-lower ** | ||||
| NT/TT NS | ||||
| Atopic dermatitis | 31/30 | NT-lower levels * | In infants with atopic dermatitis, there is an increased level of oxidative stress and a deficient antioxidant defense. | Karacan et al. (2020) [32] |
| TT-lower levels * | ||||
| DS-higher levels * | ||||
| DS/NT-higher ** | ||||
| DS/TT-higher ** | ||||
| NT/TT-lower ** | ||||
| Vitiligo | 32/35 | NT NS | TDH is not altered in vitiligo. Therefore, oxidative damage is not very advanced in patients with vitiligo. | Aksoy et al. (2018) [33] |
| TT NS | ||||
| DS NS | ||||
| DS/NT NS | ||||
| DS/TT NS | ||||
| NT/TT NS | ||||
| Vitiligo | 73/69 | NT-higher levels ** | Elevated thiol levels may be involved in the pathogenesis of vitiligo and are associated with increased pheomelanogenesis. | Akoglu et al. (2018) [23] |
| TT-higher levels ** | ||||
| DS NS | ||||
| DS/NT, DS/TT and NT/TT-no data available | ||||
| Vitiligo | 76/67 | NT-lower levels ** | TDH shifted toward disulfide formation. TDH could be involved in vitiligo pathogenesis by modulating melanin release or impairing melanocyte function. | Pektas et al. (2019) [34] |
| TT-lower levels ** | ||||
| DS NS | ||||
| DS/NT-higher * | ||||
| DS/TT-higher * | ||||
| NT/TT-lower * | ||||
| Vitiligo | 185/185 | NT-higher levels * | Elevated thiol levels may be associated with increased pheomelanin production. | Annan et al. (2019) [35] |
| TT-higher levels * | ||||
| DS NS | ||||
| DS/NT, DS/TT and NT/TT-no data available | ||||
| Cutaneous lichen planus | 81/80 | NT-higher levels * | Elevated thiol levels may be involved in cell proliferation and the progression of LP lesions. | Kalkan et al. (2019) [36] |
| TT-higher levels * | ||||
| DS NS | ||||
| DS/NT NS | ||||
| DS/TT NS | ||||
| NT/TT NS | ||||
| Cutaneous lichen planus | 31/26 | NT-lower levels * | The low levels of thiols failed to remove the lipid peroxides and failed to defend cells against the harmful effects of reactive carbonyl species in LP patients. | Mitran et al. (2019) [37] |
| TT-lower levels * | ||||
| DS-higher lower * | ||||
| DS/NT-higher * | ||||
| DS/TT-higher * | ||||
| NT/TT-lower * | ||||
| Acne vulgaris | 74/60 | NT NS | The oxidative stress present in acne vulgaris occurs through a mechanism that is not related to the level of disulfides. | Gurel et al. (2019) [38] |
| TT-lower levels * | ||||
| DS NS | ||||
| DS/NT NS | ||||
| DS/TT-lower * | ||||
| NT/TT NS | ||||
| Rosacea | 50/42 | NT NS | In rosacea, the thiol-disulfide balance shifted toward disulfides. Thiol-based treatments may be helpful in patients with rosacea. | Sener et al. (2019) [24] |
| TT NS | ||||
| DS-higher levels ** | ||||
| DS/NT-higher ** | ||||
| DS/TT-higher ** | ||||
| NT/TT-lower * | ||||
| Rosacea | 42/50 | NT-lower levels * | Rosacea is a complex condition that combines increased oxidative stress and metabolic changes. | Demir Pektas et al. (2021) [39] |
| TT-lower levels * | ||||
| DS-higher levels * | ||||
| DS/NT-higher * | ||||
| DS/TT-higher * | ||||
| NT/TT-lower * |
| Disease | Patients/ Controls | Results | Conclusion | Ref. |
|---|---|---|---|---|
| Acute urticaria | 53/47 | NT NS TT NS DS NS DS/NT NS DS/TT NS NT/TT NS | TDH is not altered in acute urticaria. | Akbas et al. (2017) [40] |
| Chronic urticaria | 57/57 | NT NS TT NS DS NS DS/NT NS DS/TT-higher ** NT/TT NS | Instead, in chronic urticaria, TDH shifted toward disulfides. | |
| Chronic urticaria (children) | 30/20 | NT-lower levels ** | Oxidative stress may be involved in the pathogenesis of urticaria. Oxidative stress was higher in children who had autoimmune diseases in the family. Therefore, there may be a link between oxidative stress and autoimmunity in chronic urticaria. | Akdag et al. (2020) [41] |
| TT-lower levels ** | ||||
| DS NS | ||||
| DS/NT-higher ** | ||||
| DS/TT-higher ** | ||||
| NT/TT-lower ** | ||||
| Acute urticaria | 35/33 | NT-lower levels * | Low levels of NT and TT can be markers of oxidative stress in acute urticaria. | Aydin et al. (2021) [42] |
| TT-lower levels ** | ||||
| DS NS | ||||
| DS/NT NS | ||||
| DS/TT NS | ||||
| NT/TT NS | ||||
| Chronic urticaria | 30/- before and after therapy with H1-antihistamines | NT-lower levels ** | Treatment with H1-antihistamines leads to an increase in thiol levels and a decrease in disulfide levels. The TDH parameters could be useful for monitoring the therapy with H1-antihistamines, in urticaria. | Matei et al. (2021) [43] |
| TT-lower levels ** | ||||
| DS-higher levels ** | ||||
| DS/NT-higher ** | ||||
| DS/TT-higher ** | ||||
| NT/TT-lower ** |
| Disease | Patients/ Controls | Results | Conclusion | Ref. |
|---|---|---|---|---|
| Warts | 80 e/40 | NT-higher levels ** | Alteration of thiol disulfide balance is associated with cell damage caused by oxidative stress. Thiol-based treatment may be useful in warts. | Erturan et al. (2019) [44] |
| TT-higher levels ** | ||||
| DS-higher levels ** (warts < 2 years) DS NS (recalcitrant warts) | ||||
| DS/NT-lower ** | ||||
| DS/TT-lower ** | ||||
| NT/TT-higher ** | ||||
| Warts | 26/28 | NT NS | These findings indicate the exceeded capacity of thiols as antioxidant molecules; therefore thiols could be a useful adjuvant therapy in patients with warts. | Mitran et al. (2021) [45] |
| TT-higher levels * | ||||
| DS NS | ||||
| DS/NT-higher * | ||||
| DS/TT-higher * | ||||
| NT/TT-lower * | ||||
| Pityriasis rosea | 52/47 | NT NS | In pityriasis rosea, the thiol-disulfide balance is not altered. | Akbas et al. (2018) [46] |
| TT NS | ||||
| DS NS | ||||
| DS/NT NS | ||||
| DS/TT NS | ||||
| NT/TT NS | ||||
| Pityriasis rosea | 34/30 | NT NS | In patients with pityriasis rosea the thiol-disulfide balance shifted toward disulfides, suggesting that oxidative stress is involved in the pathogenesis of the disease. | Yuksel et al. (2019) [19] |
| TT NS | ||||
| DS-higher levels ** | ||||
| DS/NT-higher ** | ||||
| DS/TT-higher ** | ||||
| NT/TT-no data available | ||||
| Tinea versicolor | 42/36 | NT NS | Oxidative stress does not seem to play an important role in the pathogenesis of tinea versicolor. | Kilinc et al. (2018) [47] |
| TT NS | ||||
| DS NS | ||||
| DS/NT NS | ||||
| DS/TT NS | ||||
| NT/TT NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgescu, S.R.; Mitran, C.I.; Mitran, M.I.; Matei, C.; Popa, G.L.; Erel, O.; Tampa, M. Thiol-Disulfide Homeostasis in Skin Diseases. J. Clin. Med. 2022, 11, 1507. https://doi.org/10.3390/jcm11061507
Georgescu SR, Mitran CI, Mitran MI, Matei C, Popa GL, Erel O, Tampa M. Thiol-Disulfide Homeostasis in Skin Diseases. Journal of Clinical Medicine. 2022; 11(6):1507. https://doi.org/10.3390/jcm11061507
Chicago/Turabian StyleGeorgescu, Simona Roxana, Cristina Iulia Mitran, Madalina Irina Mitran, Clara Matei, Gabriela Loredana Popa, Ozcan Erel, and Mircea Tampa. 2022. "Thiol-Disulfide Homeostasis in Skin Diseases" Journal of Clinical Medicine 11, no. 6: 1507. https://doi.org/10.3390/jcm11061507
APA StyleGeorgescu, S. R., Mitran, C. I., Mitran, M. I., Matei, C., Popa, G. L., Erel, O., & Tampa, M. (2022). Thiol-Disulfide Homeostasis in Skin Diseases. Journal of Clinical Medicine, 11(6), 1507. https://doi.org/10.3390/jcm11061507