
Prognostic Factors Associated with Recovery from Recurrent Idiopathic Sudden Sensorineural Hearing Loss: Retrospective Analysis and Systematic Review


Abstract
:1. Introduction
2. Subjects and Methods
2.1. Study Design
2.2. Statistical Analysis
2.3. Research on Recurrent ISSNHL
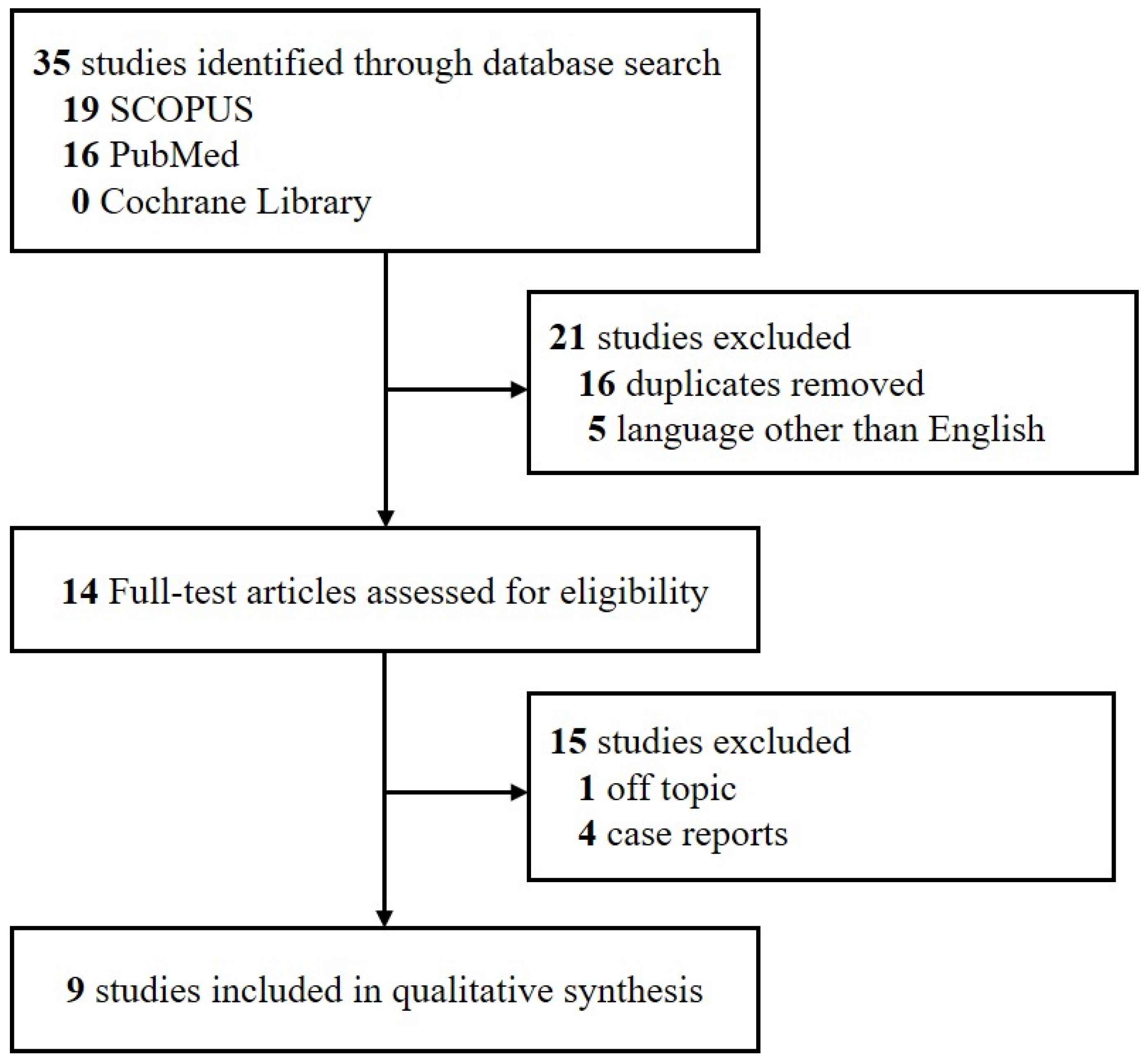
3. Results

{kind=link}
| Reference | Country | Study Design | Number of Patients with Recurrence | Recovery Rate from Recurrence | M:F | Conclusions |
|---|---|---|---|---|---|---|
| Seo et al. [9] | South Korea | Retrospective | First recurrence: 16 Second recurrence: 16 | First recurrence: 78.6% Second recurrence: 21.4% | 8:8 8:8 | NLR and PLR higher in patients with both recurrent and non-recurrent ISSNHL. |
| Park et al. [5] | South Korea | Retrospective | 11 | 72.7% | 6:5 | Hearing outcomes were poorer after a recurrent than after the first episode, with SSNHL almost always recurring in the same ear. |
| Ohashi et al. [6] | Japan | Retrospective | 23 | 69.5% | NA | Favorable prognostic factors in patients with recurrent ISSNHL included an enhanced SP/AP ratio of ECohG, a low initial AP threshold, a low initial hearing level, and an up-sloping type of audiogram. Initial vertigo was associated with unfavorable outcomes in patients with recurrent ISSNHL. |
| Kuo et al. [15] | Taiwan | Retrospective | Ipsilateral: 7 Contralateral: 9 | 50% (Ipsilateral type: 71.4% Contralateral type: 33.3%) | 3:4 5:4 | Normal VEMPs in the affected ear of patients with recurrent sudden deafness may indicate a good hearing outcome. |
| † Fushiki et al. [7] | Japan | Retrospective | 33 | * Recurrence rate 1 year: 29% 5 years: 47% (45% of recurrences occurred within 6 months of the first episode) | - | Recurrence rate higher in patients with elevated SP/AP and spontaneous nystagmus (78.6%) than in patients with normal SP/AP and absence of spontaneous nystagmus (31.8%) |
| Furuhashi et al. [3] | Japan | Retrospective | 14 | 78.5% | 9:5 | Recurrence of sudden deafness rare during long-term follow-up The degree of hearing deterioration on the first affected side was not significantly different from that on the non-affected side |
| † Wu et al. [8] | Taiwan | Retrospective | 2281 (Data from the Taiwan NHI) | * Recurrence rate 5 years: 4.99% | 1252:1029 | Factors associated with relapse included age 35–64 years, diabetes mellitus, and hypercholesterolemia |
| Pecorari et al. [16] | Italy | Retrospective | 73 | 63% * Recurrence rate 2 years: 5.6% 5 years: 10.34% | 30:43 | Recurrence correlated only with the presence of tinnitus during follow-up |
| Wu et al. [17] | Taiwan | Retrospective | 30 | 43.44% (First episode: 53.55%) | 16:14 | Hearing recovery after a recurrent episode correlated significantly with hearing outcome after the initial episode. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stachler, R.J.; Chandrasekhar, S.S.; Archer, S.M.; Rosenfeld, R.M.; Schwartz, S.R.; Barrs, D.M.; Robertson, P.J. Clinical practice guideline: Sudden hearing loss. Otolaryngol. Head Neck Surg. 2012, 146, S1–S35. [Google Scholar] [CrossRef] [Green Version]
- Byl, F.M., Jr. Sudden hearing loss: Eight years’ experience and suggested prognostic table. Laryngoscope 1984, 94, 647–661. [Google Scholar] [CrossRef] [PubMed]
- Furuhashi, A.; Matsuda, K.; Asahi, K.; Nakashima, T. Sudden deafness: Long-term follow-up and recurrence. Clin. Otolaryngol. 2002, 27, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Psifidis, A.D.; Psillas, G.K.; Daniilidis, J.C. Sudden sensorineural hearing loss: Long-term follow-up results. Otolaryngol. Head Neck Surg. 2006, 134, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Park, I.S.; Kim, Y.B.; Choi, S.H.; Hon, S.M. Clinical analysis of recurrent sudden sensorineural hearing loss. ORL 2013, 75, 245–249. [Google Scholar] [CrossRef]
- Ohashi, T.; Nishino, H.; Arai, Y.; Nishimoto, Y.; Kakutani, T.; Koizuka, I. Electrocochleographic findings in recurrent idiopathic sudden sensorineural hearing loss. Acta Otolaryngol. 2012, 132, 1022–1027. [Google Scholar] [CrossRef]
- Fushiki, H.; Junicho, M.; Aso, S.; Watanabe, Y. Recurrence rate of idiopathic sudden low-tone sensorineural hearing loss without vertigo: A long-term follow-up study. Otol. Neurotol. 2009, 30, 295–298. [Google Scholar] [CrossRef]
- Wu, C.M.; Lee, K.J.; Chang, S.L.; Weng, S.F.; Lin, Y.S. Recurrence of idiopathic sudden sensorineural hearing loss: A retrospective cohort study. Otol. Neurotol. 2014, 35, 1736–1741. [Google Scholar] [CrossRef]
- Seo, Y.J.; Park, Y.A.; Bong, J.P.; Park, D.J.; Park, S.Y. Predictive value of neutrophil to lymphocyte ratio in first-time and recurrent idiopathic sudden sensorineural hearing loss. Auris Nasus Larynx. 2015, 42, 438–442. [Google Scholar] [CrossRef]
- Hughes, F.B.; Freedman, M.A.; Haberkamp, T.J.; Guay, M.E. Sudden sensorineural hearing loss. Otolryngol. Clin. N. Am. 1996, 29, 393–405. [Google Scholar] [CrossRef]
- Cvorovic, L.; Deric, D.; Probst, R.; Hegemann, S. Prognostic model for predicting hearing recovery in idiopathic sudden sensorineural hearing loss. Otol. Neurotol. 2008, 29, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Mattox, D.E.; Lyles, C.A. Idiopathic sudden sensorineural hearing loss. Am. J. Otol. 1989, 10, 242–247. [Google Scholar] [PubMed]
- Siegel, L.G. The treatment of idiopathic sudden sensorineural hearing loss. Otolaryngol. Clin. N. Am. 1975, 8, 467–473. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Kuo, Y.L.; Young, Y.H. Hearing outcome of recurrent sudden deafness: Ipsilateral versus contralateral types. Acta Otolaryngol. 2012, 132, 247–254. [Google Scholar] [CrossRef]
- Pecorari, G.; Riva, G.; Bruno, G.; Naqe, N.; Nardo, M.; Albera, A.; Albera, R. Recurrences in Sudden Sensorineural Hearing Loss: A Long-Term Observational Study. Am. J. Audiol. 2020, 29, 18–22. [Google Scholar] [CrossRef]
- Wu, P.H.; Lee, C.Y.; Chen, H.C.; Lee, J.C.; Chu, Y.H.; Cheng, L.H.; Shih, C.P. Clinical characteristics and correlation between hearing outcomes after different episodes of recurrent idiopathic sudden sensorineural hearing loss. Auris Nasus Larynx. 2021, 48, 870–877. [Google Scholar] [CrossRef]
- Rauch, S.D. Clinical practice. Idiopathic sudden sensorineural hearing loss. N. Engl. J. Med. 2008, 359, 833–840. [Google Scholar] [CrossRef]
- Fujita, T.; Saito, K.; Kashiwagi, N.; Sato, M.; Seo, T.; Doi, K. The prevalence of vestibular schwannoma among patients treated as sudden sensorineural hearing loss. Auris Nasus Larynx. 2019, 26, 78–82. [Google Scholar] [CrossRef]
- Edizer, D.T.; Çelebi, Ö.; Hamit, B.; Baki, A.; Yiğit, Ö. Recovery of idiopathic sudden sensorineural hearing loss. J. Int. Adv. Otol. 2015, 11, 122–126. [Google Scholar] [CrossRef]
- Sakata, T.; Esaki, Y.; Yamano, T.; Sueta, N.; Nakagawa, T. A comparison between the feeling of ear fullness and tinnitus in acute sensorineural hearing loss. Int. J. Audiol. 2008, 47, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Gorga, M.P.; Kaminski, J.R.; Beauchaine, K.L. Effects of stimulus phase on the latency of the auditory brainstem response. J. Am. Acad. Audiol. 1991, 2, 1–6. [Google Scholar] [PubMed]
- Tonndorf, J.; Tabor, J.R. Closure of th cochlear windows: Its effect upon air- and bone-conduction. Ann. Otol. Rhinol. Laryngol. 1962, 71, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Sakata, T.; Kato, T. Feeling of ear fullness in acute sensorineural hearing loss. Acta Oto-Laryngol. 2006, 126, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.L.; Hsieh, C.C.; Tseng, K.S.; Weng, S.F.; Lin, Y.S. Hypercholesterolemia is correlated with an increased risk of idiopathic sudden sensorineural hearing loss: A historical prospective cohort study. Ear Hear. 2014, 35, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Lin, S.W.; Lin, Y.S.; Weng, S.F.; Lee, T.M. Sudden sensorineural hearing loss is correlated with an increased risk of acute myocardial infarction: A population-based cohort study. Laryngoscope 2013, 123, 2254–2258. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.W.; Lin, Y.S.; Weng, S.F.; Chou, C.W. Risk of developing sudden sensorineural hearing loss in diabetic patients: A population-based cohort study. Otol. Neurotol. 2012, 33, 1482–1488. [Google Scholar] [CrossRef]
- Lin, C.; Hsu, H.T.; Lin, Y.S.; Weng, S.F. Increased risk of getting sudden sensorineural hearing loss in patients with chronic kidney disease: A population-based cohort study. Laryngoscope 2013, 123, 767–773. [Google Scholar] [CrossRef]
- Lin, H.C.; Chao, P.Z.; Lee, H.C. Sudden sensorineural hearing loss increases the risk of stroke: A 5-year follow-up study. Stroke 2008, 39, 2744–2748. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, Y.; Platz, E.A.; Niparko, J.K. Prevalence of hearing loss and differences by demographic characteristics among US adults: Data from the National Health and Nutrition Examination Survey, 1999–2004. Arch Intern. Med. 2008, 168, 1522–1530. [Google Scholar] [CrossRef] [Green Version]
- Siegelaub, A.B.; Friedman, G.D.; Adour, K.; Seltzer, C.C. Hearing loss in adults: Relation to age, sex, exposure to loud noise, and cigarette smoking. Arch Environ. Occup. Health 1974, 29, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Lionello, M.; Staffieri, C.; Breda, S.; Turato, C.; Giacomelli, L.; Magnavita, P.; Marioni, G. Uni-and multivariate models for investigating potential prognostic factors in idiopathic sudden sensorineural hearing loss. Eur. Arch. Otorhinol. 2015, 272, 1899–1906. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.J.; Krall, R.; Westerberg, B.D.; Chadha, N.K.; Chau, J.K. Systematic review and meta-analysis of the risk factors for sudden sensorineural hearing loss in adults. Laryngoscope 2012, 122, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Sasso, F.C.; Salvatore, T.; Tranchino, G.; Cozzolino, D.; Caruso, A.A.; Persico, M.; Torella, R. Cochlear Dysfunction in Type 2 Diabetes: A complication Independent of Neuropathy and Acute Hyperglycemia. Metabolism 1999, 48, 1346–1350. [Google Scholar] [CrossRef]
| Variables | First Episode | Recurrent Episode | |||||
|---|---|---|---|---|---|---|---|
| Recovery (n = 30) | No Recovery (n = 8) | p-Value | Recovery (n = 24) | No Recovery (n = 14) | p-Value | ||
| n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | ||||
| Age (year) mean ± SD | 48.90 ± 16.40 | 48.75 ± 18.11 | 0.7489 | 53.63 ± 14.13 | 51.00 ± 19.52 | 0.9880 | |
| Sex | Male | 12 (40.00%) | 2 (25.00%) | 0.6836 | 8 (3.33%) | 6 (42.86%) | 0.7293 |
| Female | 18 (60.00%) | 6 (75.00%) | 16 (66.67%) | 8 (57.14%) | |||
| BMI (kg/m2), mean ± SD | 22.89 ± 2.57 | 22.42 ± 2.78 | 0.6605 | 22.78 ± 2.75 | 22.80 ± 2.37 | 0.8373 | |
| Alcohol | 4 (13.33%) | 3 (37.50%) | 0.1461 | 5 (20.83%) | 2 (14.29%) | 1.0000 | |
| Smoking | 8 (26.67%) | 2 (25.00%) | 1.0000 | 5 (20.83%) | 5 (35.71%) | 0.4485 | |
| HTN | 5 (16.67%) | 2 (25.00%) | 0.6236 | 3 (12.50%) | 4 (28.57%) | 0.3870 | |
| DM | 7 (23.33%) | 1 (12.50%) | 0.6600 | 6 (25.00%) | 2 (14.29%) | 0.6836 | |
| Tinnitus | 19 (63.33%) | 6 (75.00%) | 0.6893 | 16 (66.67%) | 12 (85.71%) | 0.2685 | |
| Ear fullness | 20 (66.67%) | 8 (100.00%) | 0.0821 | 22 (91.67%) | 4 (28.57%) | 0.0001 * | |
| Treatment onset (days), mean ± SD | 7.17 ± 16.07 | 5.50 ± 5.01 | 0.5193 | 5.58 ± 11.99 | 16.71 ± 20.73 | 0.0361 * | |
| Recovery time (months), mean ± SD | 0.95 ± 1.04 | 4.57 ± 10.29 | 0.2630 | 1.31 ± 2.04 | 3.01 ± 5.07 | 0.0303 * | |
| Hearing level of the affected ear before treatment (dB), mean ± SD | 48.44 ± 25.45 | 47.60 ± 16.27 | 0.8588 | 44.58 ± 21.94 | 49.17 ± 11.92 | 0.5686 | |
| Hearing level of the affected ear after treatment (dB), mean ± SD | 21.00 ± 14.87 | 41.56 ± 15.88 | 0.0023 * | 23.13 ± 13.60 | 53.39 ± 15.35 | <0.0001 * | |
| Time to recurrence (days), mean ± SD | - | - | - | 43.22 ± 54.31 | 44.86 ± 37.84 | 0.3697 | |
| Recurrent Episode | ||||||
|---|---|---|---|---|---|---|
| Recovery Type | Complete | Partial | Slight | No | Total | |
| First episode | Complete | 15 | 0 | 1 | 5 | 21 |
| Partial | 1 | 2 | 2 | 3 | 8 | |
| Slight | 0 | 0 | 0 | 1 | 1 | |
| No | 2 | 1 | 0 | 5 | 8 | |
| Total | 18 | 3 | 3 | 14 | 38 | |
| Variables | No Worse than after the First Episode (n = 18) | Worse than after the First Episode (n = 12) | p-Value | |
|---|---|---|---|---|
| n (%) or Mean ± SD | n (%) or Mean ± SD | |||
| Age (year), mean ± SD | 52.33 ± 13.81 | 53.00 ± 20.78 | 0.5855 | |
| Sex | Male | 7 (38.89%) | 5 (41.67%) | 1.0000 |
| Female | 11 (61.11%) | 7 (58.33%) | ||
| BMI (kg/m2), mean ± SD | 22.70 ± 2.71 | 23.18 ± 2.42 | 0.3645 | |
| Alcohol | 3 (16.67%) | 1(8.33%) | 0.6315 | |
| Smoking | 5 (27.78%) | 3 (25.00%) | 1.0000 | |
| HTN | 1 (5.65%) | 4 (33.33%) | 0.1282 | |
| DM | 4 (22.22%) | 3 (25.00%) | 1.0000 | |
| Tinnitus | 12 (66.67%) | 10 (83.33%) | 0.4192 | |
| Ear fullness | 16 (88.89%) | 6 (50.00%) | 0.0342 * | |
| Treatment onset (days), mean ± SD | 5.67 ± 13.69 | 8.33 ± 10.74 | 0.1721 | |
| Recovery time (months), mean ± SD | 1.26 ± 2.25 | 1.47 ± 1.29 | 0.0992 | |
| Hearing level of the affected ear before treatment (dB), mean ± SD | 40.05 ± 20.17 | 57.22 ± 12.92 | 0.0357 * | |
| Hearing level of the affected ear after treatment (dB), mean ± SD | 18.29 ± 8.47 | 52.36 ± 12.08 | <0.0001 * | |
| Time to recurrence (days), mean ± SD | 34.65 ± 37.54 | 53.35 ± 37.46 | 0.1139 | |
| Variables | Simple Logistic Model | Multiple Logistic Model * | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (year) | 1.00 | 0.96–1.05 | 0.9128 | adj. | ||
| Female (ref. Male) | 0.89 | 0.20–3.95 | 0.8791 | adj. | ||
| BMI | 1.08 | 0.80–1.45 | 0.6213 | 1.01 | 0.69–1.47 | 0.9703 |
| Alcohol | 0.46 | 0.04–4.98 | 0.5185 | 0.44 | 0.04–4.89 | 0.4997 |
| Smoking | 0.87 | 0.16–4.58 | 0.8662 | 0.69 | 0.09–5.67 | 0.7323 |
| HTN † | 6.18 | 0.69–55.18 | 0.1032 | 10.03 | 0.82–123.31 | 0.0717 |
| DM | 1.17 | 0.21–6.48 | 0.8602 | 1.17 | 0.17–8.2 | 0.8761 |
| Tinnitus | 2.50 | 0.41–15.23 | 0.3203 | 2.58 | 0.42–16.04 | 0.3092 |
| Ear fullness | 0.13 | 0.02–0.80 | 0.0280 | 0.10 | 0.01–0.76 | 0.0262 ** |
| Treatment onset (days) | 1.02 | 0.96–1.09 | 0.5032 | 1.03 | 0.96–1.11 | 0.4077 |
| Recovery time (months) | 1.06 | 0.72–1.56 | 0.7698 | 1.06 | 0.72–1.57 | 0.7546 |
| Hearing level of the affected ear before treatment (dB) | 1.06 | 1.01–1.11 | 0.0263 | 1.06 | 1.01–1.12 | 0.0210 ** |
| Time to recurrence (days) | 1.02 | 1.00–1.03 | 0.0442 | 1.02 | 0.99–1.04 | 0.1569 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, S.Y.; Kang, D.W.; Kim, S.H.; Byun, J.Y.; Yeo, S.G. Prognostic Factors Associated with Recovery from Recurrent Idiopathic Sudden Sensorineural Hearing Loss: Retrospective Analysis and Systematic Review. J. Clin. Med. 2022, 11, 1453. https://doi.org/10.3390/jcm11051453
Jeon SY, Kang DW, Kim SH, Byun JY, Yeo SG. Prognostic Factors Associated with Recovery from Recurrent Idiopathic Sudden Sensorineural Hearing Loss: Retrospective Analysis and Systematic Review. Journal of Clinical Medicine. 2022; 11(5):1453. https://doi.org/10.3390/jcm11051453
Chicago/Turabian StyleJeon, So Young, Dae Woong Kang, Sang Hoon Kim, Jae Yong Byun, and Seung Geun Yeo. 2022. "Prognostic Factors Associated with Recovery from Recurrent Idiopathic Sudden Sensorineural Hearing Loss: Retrospective Analysis and Systematic Review" Journal of Clinical Medicine 11, no. 5: 1453. https://doi.org/10.3390/jcm11051453
APA StyleJeon, S. Y., Kang, D. W., Kim, S. H., Byun, J. Y., & Yeo, S. G. (2022). Prognostic Factors Associated with Recovery from Recurrent Idiopathic Sudden Sensorineural Hearing Loss: Retrospective Analysis and Systematic Review. Journal of Clinical Medicine, 11(5), 1453. https://doi.org/10.3390/jcm11051453