
CXCL10/IP10 as a Biomarker Linking Multisystem Inflammatory Syndrome and Left Ventricular Dysfunction in Children with SARS-CoV-2

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Sample Collection
2.2. Statistical Analysis
3. Results
3.1. Demographic and Clinical Features, Laboratory Findings, and Management
3.2. Comparison of Patients According to Subgroups
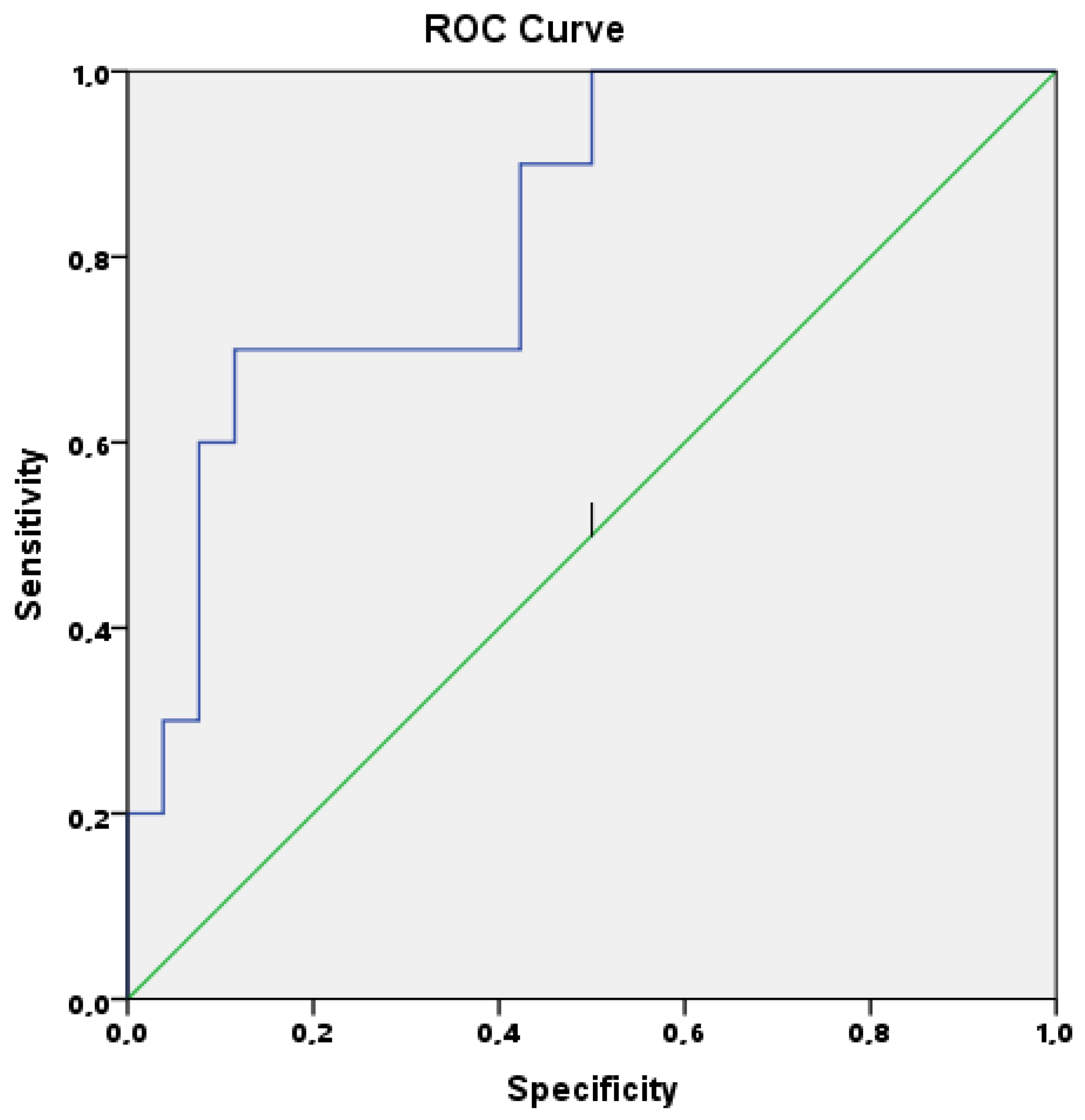
3.3. Potential Role of CXCL10/IP10 to Predict Disease Course
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://emergency.cdc.gov/han/2020/han00432.asp (accessed on 1 March 2022).
- WHO. Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19: Scientific Brief; World Health Organization: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/handle/10665/332095 (accessed on 15 May 2020).
- Godfred-Cato, S.; Bryant, B.; Leung, J.; Oster, M.E.; Conklin, L.; Abrams, J.; Roguski, K.; Wallace, B.; Prezzato, E.; Koumans, E.H.; et al. COVID-19-associated multisystem inflammatory syndrome in children—United States, March–July 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Liu, Z.; Lim, T.; Zhang, H.; He, J.; Walker, E.; Shier, C.; Wang, Y.; Su, Y.; Sall, A.; et al. CXCL10 inhibits viral replication through recruitment of natural killer cells in coxsackievirus B3-induced myocarditis. Circ. Res. 2009, 104, 628–638. [Google Scholar] [CrossRef]
- Omura, S.; Kawai, E.; Sato, F.; Martinez, N.E.; Chaitanya, G.V.; Rollyson, P.A.; Cvek, U.; Trutschl, M.; Alexander, J.S.; Tsunoda, I. Bioinformatics multivariate analysis determined a set of phase-specific biomarker candidates in a novel mouse model for viral myocarditis. Circ. Cardiovasc. Genet. 2014, 7, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Hardison, J.L.; Wrightsman, R.A.; Carpenter, P.M.; Lane, T.E.; Manning, J.E. The chemokines CXCL9 and CXCL10 promote a protective immune response but do not contribute to cardiac inflammation following infection with Trypanosoma cruzi. Infect. Immun. 2006, 74, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Lorè, N.I.; De Lorenzo, R.; Rancoita, P.M.V.; Cugnata, F.; Agresti, A.; Benedetti, F.; Bianchi, M.E.; Bonini, C.; Capobianco, A.; Conte, C.; et al. CXCL10 levels at hospital admission predict COVID-19 outcome: Hierarchical assessment of 53 putative inflammatory biomarkers in an observational study. Mol. Med. 2021, 27, 129. [Google Scholar] [CrossRef]
- Vono, M.; Huttner, A.; Lemeille, S.; Martinez-Murillo, P.; Meyer, B.; Baggio, S.; Sharma, S.; Thiriard, A.; Marchant, A.; Godeke, G.J.; et al. Robust innate responses to SARS-CoV-2 in children resolve faster than in adults without compromising adaptive immunity. Cell Rep. 2021, 37, 109773. [Google Scholar] [CrossRef]
- Caldarale, F.; Giacomelli, M.; Garrafa, E.; Tamassia, N.; Morreale, A.; Poli, P.; Timpano, S.; Baresi, G.; Zunica, F.; Cattalini, M.; et al. Plasmacytoid dendritic cells depletion and elevation of IFN-γ dependent chemokines CXCL9 and CXCL10 in children with multisystem inflammatory syndrome. Front. Immunol. 2021, 12, 654587. [Google Scholar] [CrossRef]
- Başar, E.Z.; Sönmez, H.E.; Öncel, S.; Yetimakman, A.F.; Babaoğlu, K. Multisystemic inflammatory syndrome in children associated with COVID-19: A single center experience in Turkey. Turk. Arch. Pediatr. 2021, 56, 192–199. [Google Scholar] [CrossRef]
- Shi, Q.; Wang, Z.; Liu, J.; Wang, X.; Zhou, Q.; Li, Q.; Yu, Y.; Luo, Z.; Liu, E.; Chen, Y. Risk factors for poor prognosis in children and adolescents with COVID-19: A systematic review and meta-analysis. EClinicalMedicine 2021, 41, 101155. [Google Scholar] [CrossRef]
- Ramcharan, T.; Nolan, O.; Lai, C.Y.; Prabhu, N.; Krishnamurthy, R.; Richter, A.G.; Jyothish, D.; Kanthimathinathan, H.K.; Welch, S.B.; Hackett, S.; et al. Paediatric inflammatory multisystem syndrome: Temporally associated with SARS-CoV-2 (PIMS-TS): Cardiac features, management and short-term outcomes at a UK Tertiary paediatric hospital. Pediatr. Cardiol. 2020, 41, 1391–1401. [Google Scholar] [CrossRef]
- Davies, P.; Evans, C.; Kanthimathinathan, H.K.; Lillie, J.; Brierley, J.; Waters, G.; Johnson, M.; Griffiths, B.; Du Pré, P.; Mohammad, Z.; et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: A multicentre observational study. Lancet Child Adolesc. Health 2020, 4, 669–677. [Google Scholar] [CrossRef]
- Zhao, Y.; Yin, L.; Patel, J.; Tang, L.; Huang, Y. The inflammatory markers of multisystem inflammatory syndrome in children (MIS-C) and adolescents associated with COVID-19: A meta-analysis. J. Med. Virol. 2021, 93, 4358–4369. [Google Scholar] [CrossRef] [PubMed]
- Reisner, A.; Blackwell, L.S.; Sayeed, I.; Myers, H.E.; Wali, B.; Heilman, S.; Figueroa, J.; Lu, A.; Hussaini, L.; Anderson, E.J.; et al. Osteopontin as a biomarker for COVID-19 severity and multisystem inflammatory syndrome in children: A pilot study. Exp. Biol. Med. 2021, 247, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Sarmiento, J.; Flórez, S.; Alarcón-Forero, L.C.; Salazar-Peláez, L.M.; Garcia-Casallas, J.; Mulett, H.; Acevedo, L.; Salamanca, C. Case Report: Endothelial glycocalyx damage in critically ill patients with SARS-CoV-2-Related multisystem inflammatory syndrome (MIS-C). Front. Pediatr. 2021, 9, 726949. [Google Scholar] [CrossRef]
- Kavurt, A.V.; Bağrul, D.; Gül, A.E.K.; Özdemiroğlu, N.; Ece, İ.; Çetin, İ.İ.; Özcan, S.; Uyar, E.; Emeksiz, S.; Çelikel, E.; et al. Echocardiographic findings and correlation with laboratory values in multisystem inflammatory syndrome in children (MIS-C) associated with COVID-19. Pediatr. Cardiol. 2022, 43, 413–425. [Google Scholar] [CrossRef]
- Chang, J.C.; Matsubara, D.; Morgan, R.W.; Diorio, C.; Nadaraj, S.; Teachey, D.T.; Bassiri, H.; Behrens, E.M.; Banerjee, A. Skewed cytokine responses rather than the magnitude of the cytokine storm may drive cardiac dysfunction in multisystem inflammatory syndrome in children. J. Am. Heart Assoc. 2021, 10, e021428. [Google Scholar] [CrossRef]
- Mach, F.; Sauty, A.; Iarossi, A.S.; Sukhova, G.K.; Neote, K.; Libby, P.; Luster, A.D. Differential expression of three T lymphocyte-activating CXC chemokines by human atheroma-associated cells. J. Clin. Investig. 1999, 104, 1041–1050. [Google Scholar] [CrossRef]
- Cheng, C.; Tempel, D.; van Haperen, R.; de Boer, H.C.; Segers, D.; Huisman, M.; van Zonneveld, A.J.; Leenen, P.J.; van der Steen, A.; Serruys, P.W.; et al. Shear stress induced changes in atherosclerotic plaque composition are modulated by chemokines. J. Clin. Investig. 2007, 117, 616–626. [Google Scholar] [CrossRef]
- Niki, T.; Soeki, T.; Yamaguchi, K.; Taketani, Y.; Yagi, S.; Iwase, T.; Yamada, H.; Wakatsuki, T.; Shimabukuro, M.; Sata, M. Elevated concentration of interferon-inducible protein of 10 kD (IP-10) is associated with coronary atherosclerosis. Int. Heart J. 2015, 56, 269–272. [Google Scholar] [CrossRef][Green Version]
- Safa, A.; Rashidinejad, H.R.; Khalili, M.; Dabiri, S.; Nemati, M.; Mohammadi, M.M.; Jafarzadeh, A. Higher circulating levels of chemokines CXCL10, CCL20 and CCL22 in patients with ischemic heart disease. Cytokine 2016, 83, 147–157. [Google Scholar] [CrossRef]
- Ko, T.M.; Kuo, H.C.; Chang, J.S.; Chen, S.P.; Liu, Y.M.; Chen, H.W.; Tsai, F.J.; Lee, Y.C.; Chen, C.H.; Wu, J.Y.; et al. CXCL10/IP-10 is a biomarker and mediator for Kawasaki disease. Circ. Res. 2015, 116, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Hsu, Y.W.; Lu, H.F.; Chou, W.H.; Kuo, H.C.; Chang, W.C. Functional correlations between CXCL10/IP10 gene polymorphisms and risk of Kawasaki disease. Pediatr. Allergy Immunol. 2021, 32, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Bracaglia, C.; De Graaf, K.; Marafon, D.P.; Guilhot, F.; Ferlin, W.; Prencipe, G.; Caiello, I.; Davì, S.; Schulert, G.; Ravelli, A.; et al. Elevated circulating levels of interferon-γ and interferon-γ-induced chemokines characterise patients with macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. Ann. Rheum. Dis. 2016, 76, 166–172. [Google Scholar] [CrossRef] [PubMed]
- De Benedetti, F.; Brogan, P.; Bracaglia, C.; Pardeo, M.; Marucci, G.; Sacco, E.; Eleftheriou, D.; Papadopoulou, C.; Grom, A.; Quartier, P.; et al. OP0290 Emapalumab (anti-interferon-gamma monoclonal antibody) in patients with macrophage activation syndrome (mas) complicating systemic juvenile idiopathic arthritis (sjia). Ann. Rheum Dis. 2020, 79, 180. [Google Scholar] [CrossRef]
- Kesmez Can, F.; Özkurt, Z.; Öztürk, N.; Sezen, S. Effect of IL-6, IL-8/CXCL8, IP-10/CXCL 10 levels on the severity in COVID 19 infection. Int. J. Clin. Pract. 2021, 9, 14970. [Google Scholar] [CrossRef]
- Altara, R.; Manca, M.; Hessel, M.H.; Gu, Y.; van Vark, L.C.; Akkerhuis, K.M.; Staessen, J.A.; Struijker-Boudier, H.A.; Booz, G.W.; Blankesteijn, W.M. CXCL10 is a circulating inflammatory marker in patients with advanced heart failure: A pilot study. J. Cardiovasc. Transl. Res. 2016, 9, 302–314. [Google Scholar] [CrossRef]
- Altara, R.; Manca, M.; Brandao, R.D.; Zeidan, A.; Booz, G.W.; Zouein, F.A. Emerging importance of chemokine receptor CXCR3 and its ligands in cardiovascular diseases. Clin. Sci. 2016, 130, 463–478. [Google Scholar] [CrossRef]
- Philippe, A.; Chocron, R.; Gendron, N.; Bory, O.; Beauvais, A.; Peron, N.; Khider, L.; Guerin, C.L.; Goudot, G.; Levasseur, F.; et al. Circulating Von Willebrand factor and high molecular weight multimers as markers of endothelial injury predict COVID-19 in-hospital mortality. Angiogenesis 2021, 24, 505–517. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Ouldali, N.; Toubiana, J.; Antona, D.; Javouhey, E.; Madhi, F.; Lorrot, M.; Léger, P.L.; Galeotti, C.; Claude, C.; Wiedemann, A.; et al. Association of intravenous immunoglobulins plus methylprednisolone vs immunoglobulins alone with course of fever in multisystem inflammatory syndrome in children. JAMA 2021, 325, 855–864. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients (n = 36) | |
|---|---|
| Fever, n | 36 |
| Mucocutaneous findings | |
| Polymorphous rash, n | 22 |
| Conjunctivitis, n | 19 |
| Oral changes, n | 12 |
| Extremity changes, n | 8 |
| Cervical lymphadenopathy, n | 1 |
| Musculoskeletal findings | |
| Myalgia, n | 4 |
| Gastrointestinal findings | |
| Abdominal pain, n | 21 |
| Diarrhea, n | 13 |
| Appendicitis or bowel edema, n | 5 |
| Cardiovascular findings | |
| LV dysfunction or myocarditis, n | 10 |
| Pericarditis, n | 6 |
| Coronary artery dilatation, n | 1 |
| Coronary artery brightness, n | 2 |
| Mild mitral valve insufficiency, n | 13 |
| Moderate-severe mitral valve insufficiency, n | 4 |
| Mild tricuspid valve insufficiency, n | 1 |
| Renal involvement, n | 3 |
| Neurologic involvement, n | 2 |
| Group I (n = 11) | Group II (n = 9) | Group III (n = 16) | p | |
|---|---|---|---|---|
| Gender (Female/Male) | 5/6 | 4/5 | 7/9 | 0.996 |
| Fever, n | 11 | 9 | 16 | - |
| Polymorphous rash, n | 10 | 6 | 6 | 0.009 |
| Conjunctivitis, n | 8 | 4 | 7 | 0.187 |
| Oral changes, n | 7 | 2 | 3 | 0.02 |
| Extremity changes, n | 4 | 3 | 1 | 0.113 |
| Cervical lymphadenopathy, n | 1 | 0 | 0 | 0.521 |
| Myalgia, n | 1 | 2 | 1 | 0.813 |
| Abdominal pain, n | 4 | 6 | 11 | 0.206 |
| Diarrhea, n | 1 | 2 | 10 | 0.01 |
| Appendicitis or bowel edema, n | 0 | 0 | 5 | 0.02 |
| LV * dysfunction or myocarditis, n | 1 | 9 | 0 | <0.001 |
| Renal involvement, n | 1 | 2 | 0 | 0.356 |
| Neurologic involvement, n | 0 | 2 | 0 | 0.139 |
| Intensive care unit, n | 1 | 6 | 0 | <0.001 |
| IVIG *, n | 11 | 9 | 16 | - |
| Second dose of IVIG | 0 | 1 | 0 | 0.253 |
| Pulse steroid, n | 2 | 6 | 1 | 0.02 |
| Methylprednisolone (2 mg/kg), n | 3 | 2 | 7 | 0.02 |
| Anakinra, n | 1 | 5 | 0 | 0.002 |
| Group I (n = 11) | Group II (n = 9) | Group III (n = 16) | p | |
|---|---|---|---|---|
| Complete Blood Count ** | ||||
| WBC *, mm3 (at diagnosis) | 8611 (4328–19,000) | 11,666 (1388–18,930) | 8341 (3090–23,000) | 0.389 |
| WBC *, mm3 (at day 3) | 13,045 (4471–17,800) | 19,200 (1749–28,200) | 5713 (3448–9706) | 0.015 |
| WBC *, mm3 (at day 7) | 15,854 (5040–30,220) | 11,805 (5061–20,020) | 10,641 (4370–20,656) | 0.876 |
| Lymphocyte, mm3 (at diagnosis) | 1801 (604–5190) | 451 (248–1080) | 1085 (710–3283) | 0.002 |
| Lymphocyte, mm3 (at day 3) | 2993 (1191–7410) | 880 (562–1303) | 1540 (766–3623) | 0.006 |
| Lymphocyte, mm3 (at day 7) | 3370 (1440–14,420) | 2092 (942–3160) | 3412 (1640–7061) | 0.011 |
| Hemoglobin, g/dL (at diagnosis) | 10.9 (8.2–12.5) | 10.9 (10.5–10.4) | 11.4 (7.7–13.7) | 0.641 |
| Hemoglobin, g/dL (at day 3) | 10.6 (8.7–12.5) | 10 (8.7–14.1) | 10.6 (8.8–12.8) | 0.897 |
| Hemoglobin, g/dL (at day 7) | 11.8 (7.30–13.4) | 12 (11–14.3) | 11.6 (9.1–13.6) | 0.377 |
| Platelet, mm3 (at diagnosis) | 176,250 (110,000–462,000) | 120,500 (55,400–209,000) | 195,000 (67,000–384,000) | 0.090 |
| Platelet, mm3 (at day 3) | 341,000 (198,000–665,400) | 173,500 (73,600–284,000) | 195,500 (180,000–767,000) | 0.013 |
| Platelet, mm3 (at day 7) | 535,000 (412,000–804,000) | 340,000 (175,000–410,000) | 334,500 (278,000–718,000) | 0.250 |
| Inflammatory Markers ** | ||||
| CXCL10/IP10 *, pg/mL (at diagnosis) | 2280 (0–4174) | 3938 (1571–4558) | 763 (0–346) | 0.004 |
| CXCL10/IP10 *, pg/mL (at day 3) | 933 (0–2545) | 3467 (123–4319) | 37 (0–4132) | 0.019 |
| CXCL10/IP10 *, pg/mL (at day 7) | 116 (0–3161) | 2264 (0–4121) | 0 (0–577) | 0.021 |
| IL-6 *, pg/mL (at diagnosis) | 36.4 (3.1–136) | 324 (9.1–2330) | 18 (0–346) | 0.066 |
| IL-6 *, pg/mL (at day 3) | 2.6 (0–58) | 4.6 (3.3–147) | 5.5 (0–22) | 0.979 |
| IL-6 *, pg/mL (at day 7) | 1.1 (0–24) | 0 (0–6) | 0 (0–4.5) | 0.235 |
| CRP *, mg/L (at diagnosis) | 145 (24–333) | 187.5 (29–278) | 138.5 (1.98–233) | 0.388 |
| CRP *, mg/L (at day 3) | 33 (8–98) | 122.5 (8.9–219) | 47 (5.2–109) | 0.074 |
| CRP *, mg/L (at day 7) | 10.8 (0.94–20.6) | 14.8 (2.29–35) | 4.7 (2–98) | 0.550 |
| ESR *, mm/hr (at diagnosis) | 50 (10–115) | 42 (4–69) | 46 (8–114) | 0.421 |
| ESR *, mm/hr (at day 3) | 79 (8–140) | 24 (13–45) | 58 (38–137) | 0.027 |
| ESR *, mm/hr (at day 7) | 43 (5–140) | 13.5 (4–40) | 38 (14–63) | 0.003 |
| Procalcitonin, ng/mL (at diagnosis) | 3.5 (0.48–42) | 18.5 (0.61–100) | 1.9 (0.24–25.2) | 0.070 |
| Procalcitonin, ng/mL (at day 3) | 0.25 (0.08–6.2) | 1.5 (0.12–88) | 0.64 (0.07–16) | 0.095 |
| Procalcitonin, ng/mL (at day 7) | 0.24 (0.04–1.36) | 0.5 (0.04–15) | 0.06 (0.02–9.2) | 0.545 |
| Ferritin, ug/L (at diagnosis) | 337 (142–8632) | 616 (127–1746) | 141 (12–2275) | 0.064 |
| Ferritin, ug/L (at day 3) | 384 (135–4103) | 723 (279–1889) | 195 (48–423) | 0.004 |
| Ferritin, ug/L (at day 7) | 200 (110–2000) | 400 (127–1021) | 97 (39–742) | 0.018 |
| Cardiac Markers ** | ||||
| NT-pro-BNP *, ng/L (at diagnosis) | 2201 (70–14,900) | 2885 (282–24,000) | 426 (70–14,100) | 0.032 |
| NT-pro-BNP *, ng/L (at day 3) | 1083 (106–3960) | 2870 (428–35,000) | 601 (70–1230) | 0.004 |
| NT-pro-BNP *, ng/L (at day 7) | 190 (70–894) | 181 (123–4150) | 70 (70–380) | 0.088 |
| Troponin-I, ng/L (at diagnosis) | 0 (0–65) | 17.5 (0–140) | 0 (0–0) | 0.006 |
| Troponin-I, ng/L (at day 3) | 0 (0–21) | 44.5 (0–390) | 0 (0–18) | 0.097 |
| Troponin-I, ng/L (at day 7) | 0 (0–0) | 0 (0–39) | 0 (0–0) | 0.051 |
| Coagulation Parameters ** | ||||
| D-dimer, µg/mL (at diagnosis) | 2.1 (0.6–7.45) | 12.8 (1.1–21.8) | 1.7 (0.19–12.5) | 0.030 |
| D-dimer, µg/mL (at day 3) | 1.4 (0.62–2.82) | 4.2 (0.85–6.24) | 1.07 (0.36–6.5) | 0.184 |
| D-dimer, µg/mL (at day 7) | 1.22 (0.58–9.87) | 2.05 (0.73–384) | 0.91 (0.20–11.1) | 0.556 |
| Fibrinogen, g/L (at diagnosis) | 5.2 (2.6–8.6) | 5.1 (2.4–7.9) | 4.7 (2.9–6.6) | 0.480 |
| Fibrinogen, g/L (at day 3) | 4.1 (1.9–8.6) | 4.05 (3.23–6.34) | 4.3 (2.9–5.73) | 0.824 |
| Fibrinogen, g/L (at day 7) | 3.5 (0–5.9) | 2.3 (1.05–3.91) | 3.1 (0.94–4.6) | 0.180 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Başar, E.Z.; Sönmez, H.E.; Uzuner, H.; Karadenizli, A.; Güngör, H.S.; Akgün, G.; Yetimakman, A.F.; Öncel, S.; Babaoğlu, K. CXCL10/IP10 as a Biomarker Linking Multisystem Inflammatory Syndrome and Left Ventricular Dysfunction in Children with SARS-CoV-2. J. Clin. Med. 2022, 11, 1416. https://doi.org/10.3390/jcm11051416
Başar EZ, Sönmez HE, Uzuner H, Karadenizli A, Güngör HS, Akgün G, Yetimakman AF, Öncel S, Babaoğlu K. CXCL10/IP10 as a Biomarker Linking Multisystem Inflammatory Syndrome and Left Ventricular Dysfunction in Children with SARS-CoV-2. Journal of Clinical Medicine. 2022; 11(5):1416. https://doi.org/10.3390/jcm11051416
Chicago/Turabian StyleBaşar, Eviç Zeynep, Hafize Emine Sönmez, Hüseyin Uzuner, Aynur Karadenizli, Hüseyin Salih Güngör, Gökmen Akgün, Ayşe Filiz Yetimakman, Selim Öncel, and Kadir Babaoğlu. 2022. "CXCL10/IP10 as a Biomarker Linking Multisystem Inflammatory Syndrome and Left Ventricular Dysfunction in Children with SARS-CoV-2" Journal of Clinical Medicine 11, no. 5: 1416. https://doi.org/10.3390/jcm11051416
APA StyleBaşar, E. Z., Sönmez, H. E., Uzuner, H., Karadenizli, A., Güngör, H. S., Akgün, G., Yetimakman, A. F., Öncel, S., & Babaoğlu, K. (2022). CXCL10/IP10 as a Biomarker Linking Multisystem Inflammatory Syndrome and Left Ventricular Dysfunction in Children with SARS-CoV-2. Journal of Clinical Medicine, 11(5), 1416. https://doi.org/10.3390/jcm11051416