
Feasibility of 4D-Spatio Temporal Image Correlation (STIC) in the Comprehensive Assessment of the Fetal Heart Using FetalHQ®


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
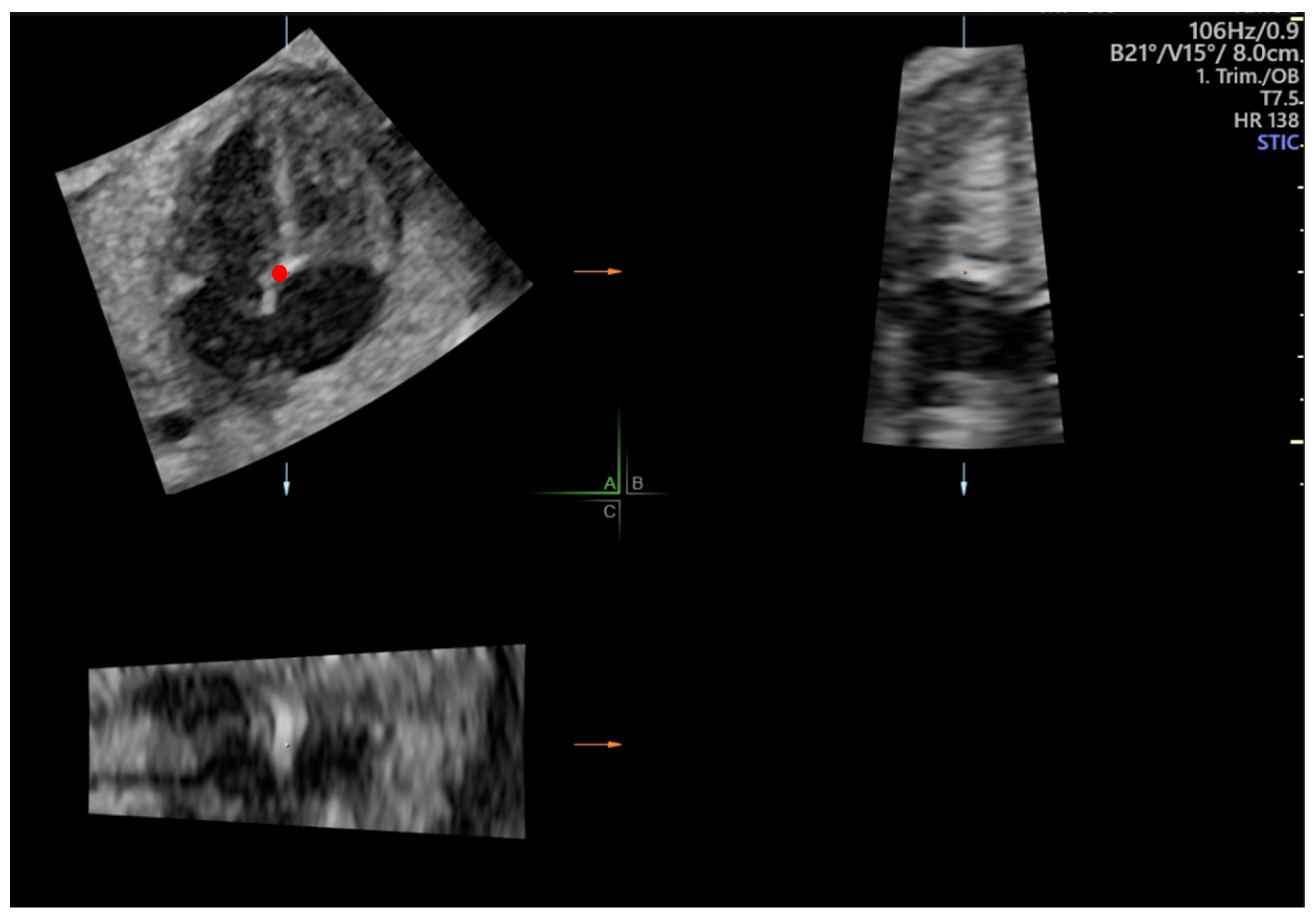
2.2. Fetal Echocardiography
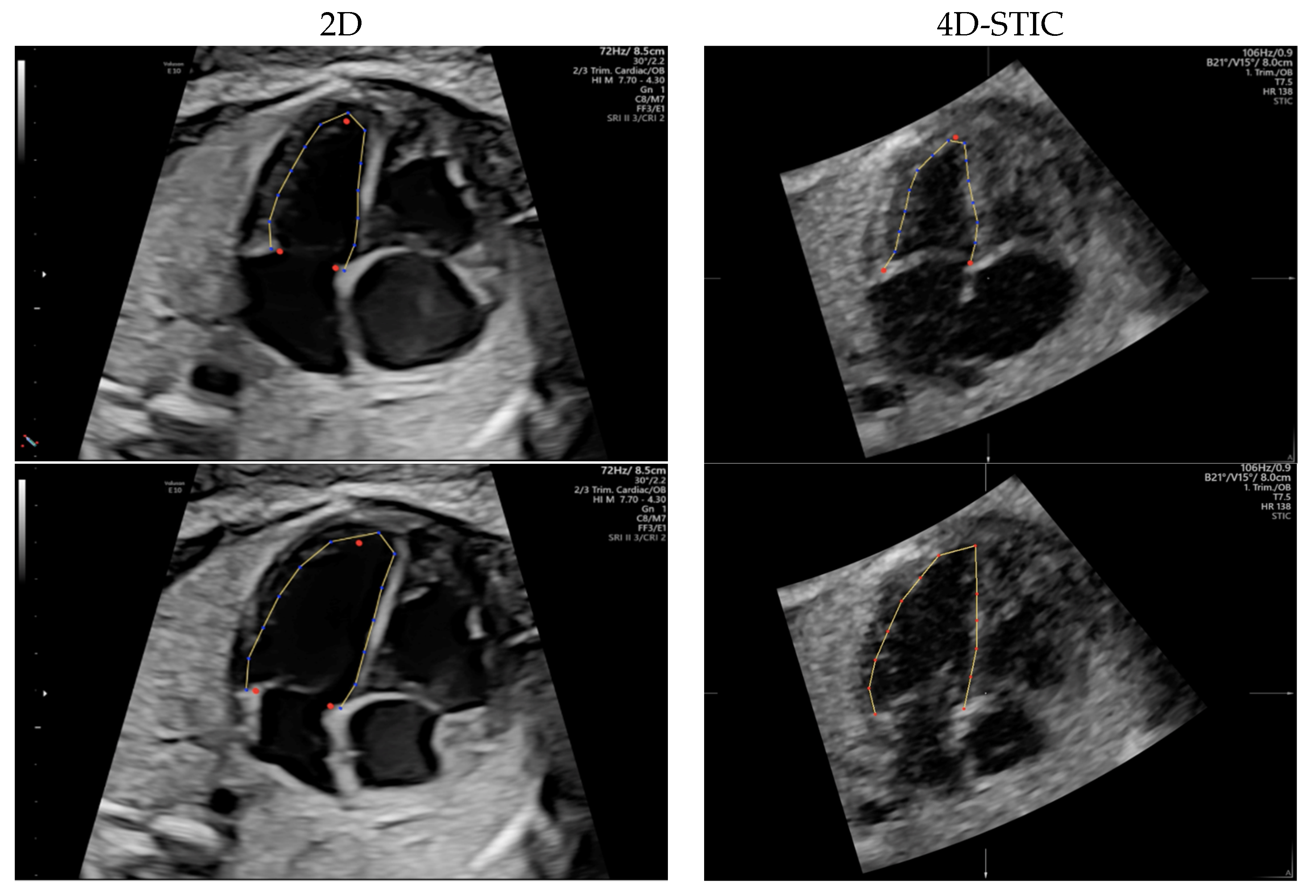
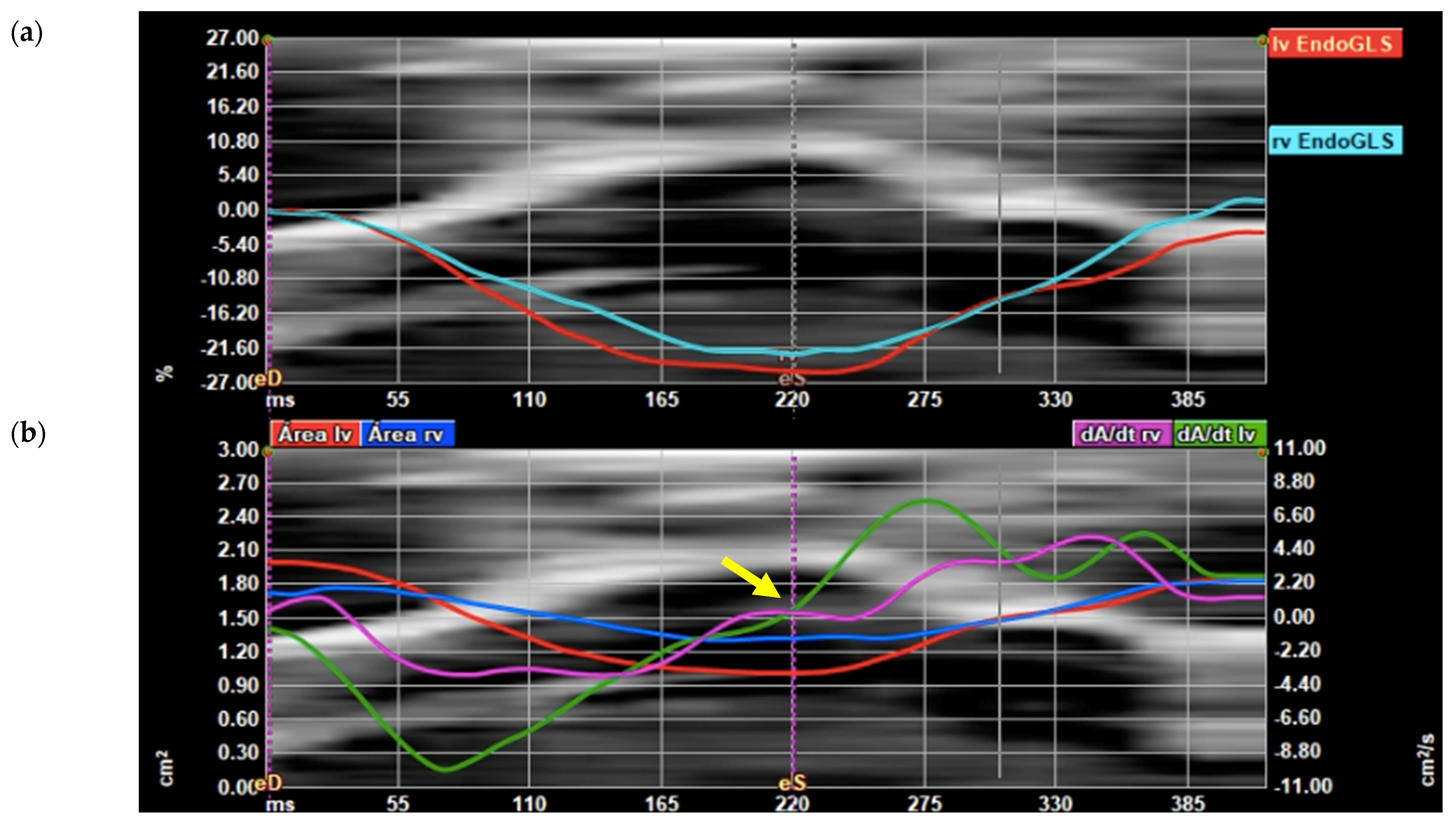
2.3. Speckle Tracking Analysis
2.4. Sample Size Calculation
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Feasibility
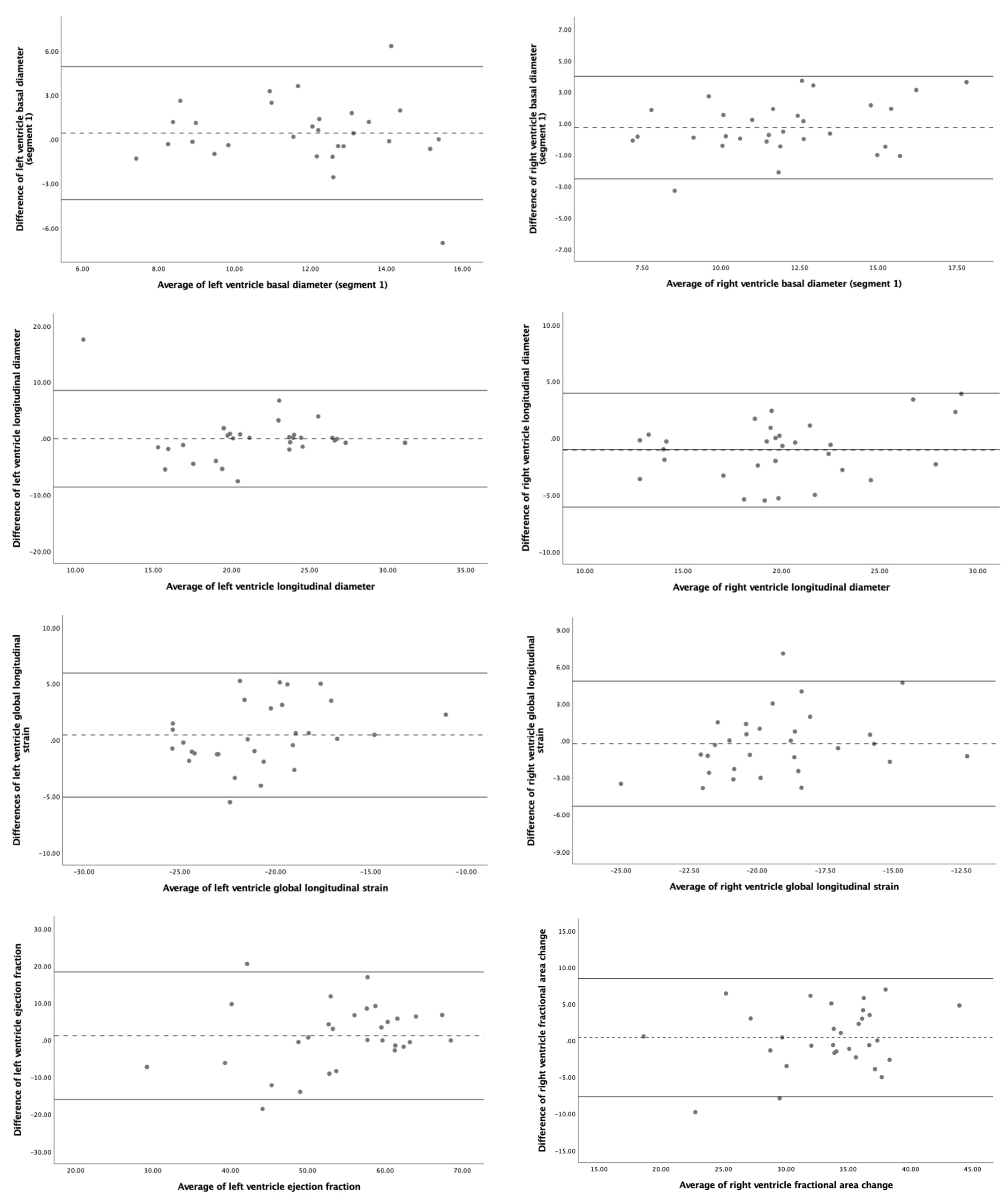
3.3. Reproducibility
3.4. Subanalysis Using Quiver Tool
4. Discussion
4.1. Speckle Tracking Echocardiography Using 2D- and 4D-STIC
4.2. Fetal Cardiac Morphometric and Functional Assessment Using 4D-STIC STE
4.3. Subanalysis Using Quiver Tool
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shapiro, I.; Degani, S.; Leibovitz, Z.; Ohel, G.; Tal, Y.; Abinader, E.G. Fetal Cardiac Measurements Derived by Transvaginal and Transabdominal Cross-Sectional Echocardiography from 14 Weeks of Gestation to Term. Ultrasound Obs. Gynecol 1998, 12, 404–418. [Google Scholar] [CrossRef]
- Firpo, C.; Silverman, N.H. Evaluation of Fetal Heart Dimensions from 12 Weeks to Term. Am. J. Cardiol. 2001, 87, 594–600. [Google Scholar] [CrossRef]
- Kleinman, S.; Lynch, C.; Hobbins, C.; Talner, S. Echocardiographic Studies of the Human Fetus: Prenatal Diagnosis of Congenital Heart Disease and Cardiac Dysrhythmias. Pediatrics 2021, 65, 1059–1067. [Google Scholar] [CrossRef]
- Allan, L.D.; Joseph, M.C.; Boyd, E.G.C.A.; Campbell, S.; Tynan, M. M-Mode Echocardiography in the Developing Human Fetus. Br Hear. J 1982, 47, 573–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comas, M.; Crispi, F. Assessment of Fetal Cardiac Function Using Tissue Doppler Techniques. Fetal Diagn. Ther. 2012, 32, 30–38. [Google Scholar] [CrossRef]
- Bennasar, M.; Mart, J.M.I.; Figueras, F.; Olivella, A.; Puerto, B. Intra- and Interobserver Repeatability of Fetal Cardiac Examination Using Four-Dimensional Spatiotemporal Image Correlation in Each Trimester of Pregnancy. Ultrasound Obstet. Gynecol. 2010, 35, 318–323. [Google Scholar] [CrossRef]
- DeVore, G.R.; Satou, G.; Sklansky, M. 4D Fetal Echocardiography—An Update. Echocardiography 2017, 34, 1788–1798. [Google Scholar] [CrossRef]
- Langeland, S.; Jan, D.; Wouters, P.F.; Leather, H.A.; Claus, P.; Bijnens, B.; Sutherland, G.R. Experimental Validation of a New Ultrasound Method for the Simultaneous Assessment of Radial and Longitudinal Myocardial Deformation Independent of Insonation Angle. Circulation 2005, 112, 2157–2162. [Google Scholar] [CrossRef] [Green Version]
- Kocabay, G.; Muraru, D.; Peluso, D.; Cucchini, U.; Mihaila, S.; Padayattil-jose, S.; Gentian, D.; Iliceto, S.; Vinereanu, D.; Badano, L.P. Normal Left Ventricular Mechanics by Two-Dimensional Speckle-Tracking Echocardiography. Reference Values in Healthy Adults. Rev. Esp. Cardiol. 2014, 67, 651–658. [Google Scholar] [CrossRef]
- Pirat, B.; Khoury, D.S.; Hartley, C.J.; Tiller, L.; Schulz, D.G.; Nagueh, S.F.; Zoghbi, W.A. A Novel Feature-Tracking Echocardiographic Method for the Quantitation of Regional Myocardial Function: Validation in an animal model of ischemia-reperfusion. J. Am. Coll. Cardiol. 2008, 51, 651–659. [Google Scholar] [CrossRef] [Green Version]
- Crispi, F.; Valenzuela-Alcaraz, B.; Gratacós, E. Ultrasound Assessment of Fetal Cardiac Function. AJUM 2013, 16, 158–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsey, J.; Friedberg, M.K.; Mertens, L. Speckle Tracking Echocardiography in Pediatric and Congenital Heart Disease. Echocardiography 2013, 30, 447–459. [Google Scholar] [CrossRef] [PubMed]
- Geyer, H.; Caracciolo, G.; Abe, H.; Wilansky, S.; Carerj, S. Assessment of Myocardial Mechanics Using Speckle Tracking Echocardiography: Fundamentals and Clinical Applications. J. Am. Soc. Echocardiogr. 2010, 23, 351–369. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.T.; Machefsky, A.; Sanchez, A.A.; Patel, M.D.; Rogal, S.; Singh, G.K. Reference Ranges of Left Ventricular Strain Measures by Two- Dimensional Speckle Tracking Echocardiography in Children: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 29, 209–225. [Google Scholar] [CrossRef] [Green Version]
- Di Salvo, G.; Russo, M.G.; Paladini, D.; Felicetti, M.; Castaldi, B.; Tartaglione, A.; Pietto, L.; Ricci, C.; Morelli, C.; Pacileo, G. Two-Dimensional Strain to Assess Regional Left and Right Ventricular Longitudinal Function in 100 Normal Foetuses. Eur. J. Echocardiogr. 2008, 9, 754–756. [Google Scholar] [CrossRef] [Green Version]
- Ta-shma, A.; Perles, Z.; Gavri, S.; Golender, J. Analysis of Segmental and Global Function of the Fetal Heart Using Novel Automatic Functional Imaging. Congenit. Heart Dis. 2008, 21, 146–150. [Google Scholar] [CrossRef]
- Willruth, A.M.; Geipel, A.K.; Fimmers, R.; Gembruch, U.G. Assessment of Right Ventricular Global and Regional Longitudinal Peak Systolic Strain, Strain Rate and Velocity in Healthy Fetuses and Impact of Gestational Age Using a Novel Speckle / Feature-Tracking Based Algorithm. Ultrasound Obs. Gynecol 2011, 37, 143–149. [Google Scholar] [CrossRef]
- Ishii, T.; McElhinney, D.B.; Harrild, D.M.; Marcus, E.N.; Sahn, D.J.; Truong, U.; Tworetzky, W.T. Circumferential and Longitudinal Ventricular Strain in the Normal Human Fetus. J. Am. Soc. Echocardiogr. 2012, 25, 105–111. [Google Scholar] [CrossRef]
- Germanakis, I. Assessment of Fetal Myocardial Deformation Using Speckle Tracking Techniques. Fetal Diagn. Ther. 2012, 32, 39–46. [Google Scholar] [CrossRef]
- Devore, G.R.; Polanco, B.; Satou, G.; Sklansky, M. Two-Dimensional Speckle Tracking of the Fetal Heart. J. Ultrasound Med. 2016, 35, 1765–1781. [Google Scholar] [CrossRef]
- Day, T.G.; Charakida, M.; Simpson, J.M. Using Speckle-Tracking Echocardiography to Assess Fetal Myocardial Deformation: Are We There Yet? Ultrasound Obstet. Gynecol. 2019, 54, 575–581. [Google Scholar] [CrossRef] [PubMed]
- van Oostrum, N.H.; de Vet, C.M.; van der Woude, D.A.; Kemps, H.M.; Oei, S.G.; van Laar, J.O. Fetal Strain and Strain Rate during Pregnancy Measured with Speckle Tracking Echocardiography: A Systematic Review. Eur. J. Obstet. Gynecol. 2020, 250, 178–187. [Google Scholar] [CrossRef]
- Semmler, J.; Day, T.; Georgiopoulos, G.; Garcia-Gonzalez, C.; Aguilera, J.; Vigneswaran, T.; Zidere, V.; Miller, O.I.; Sharland, G.; Charakida, M.; et al. Fetal Speckle-Tracking: Impact of Angle of Insonation and Frame Rate on Global Longitudinal Strain. J. Am. Soc. Echocardiogr. 2020, 33, 1141–1146.e2. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.-U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J.-Cardiovasc. Imaging 2014, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Moen, C.A.; Salminen, P.-R.; Dahle, G.O.; Hjertaas, J.J.; Grong, K.; Matre, K. Is strain by Speckle Tracking Echocardiography dependent on user controlled spatial and temporal smoothing? An experimental porcine study. Cardiovasc. Ultrasound 2013, 11, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devore, G.R.; Klas, B.; Satou, G.; Sklansky, M. Twenty-Four Segment Transverse Ventricular Fractional Shortening: A new technique to evaluate fetal cardiac function. J. Ultrasound Med. 2018, 37, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Devore, G.R.; Klas, B.; Satou, G.; Sklansky, M. 24-Segment Sphericity Index: A New Technique to Evaluate Fetal Cardiac Diastolic Shape. Ultrasound Obstet. Gynecol. 2018, 51, 650–658. [Google Scholar] [CrossRef] [Green Version]
- Devore, G.R.; Klas, B.; Satou, G.; Sklansky, M. Evaluation of Fetal Left Ventricular Size and Function Using Speckle-Tracking and the Simpson Rule. J. Ultrasound Med. 2018, 38, 1209–1221. [Google Scholar] [CrossRef]
- Devore, G.R.; Klas, B.; Satou, G.; Sklansky, M. Speckle Tracking of the Basal Lateral and Septal Wall Annular Plane Systolic Excursion of the Right and Left Ventricles of the Fetal Heart. J. Ultrasound Med. 2019, 38, 1309–1318. [Google Scholar] [CrossRef]
- Devore, G.R.; Klas, B.; Satou, G.; Sklansky, M. Quantitative Evaluation of Fetal Right and Left Ventricular Fractional Area Change Using Speckle-Tracking Technology. Ultrasound Obs. Gynecol. 2019, 53, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Devore, G.R.; Klas, B.; Satou, G.; Sklansky, M. Longitudinal Annulae Systolic Displacement Compared to Global Strain in Normal Fetal Hearts and Those With Cardiac Abnormalities. J. Ultrasound Med. 2018, 37, 1156–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devore, G.R.; Cuneo, B.; Klas, B.; Satou, G.; Sklansky, M. Comprehensive Evaluation of Fetal Cardiac Ventricular Widths and Ratios Technique. J. Ultrasound Med. 2019, 38, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Devore, G.R.; Klas, B.; Satou, G.; Sklansky, M. Evaluation of the Right and Left Ventricles: An Integrated Approach Measuring the Area, Length and Width of the Chambers in Normal Fetuses. Prenat. Diagn. 2019, 37, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Devore, G.R.; Haxel, C.; Satou, G.; Sklansky, M. Improved Detection of Coarctation of the Aorta Using Speckle Tracking Analysis of the Fetal Heart Using the Last Examination Prior to Delivery. Ultrasound Obs. Gynecol. 2021, 57, 282–291. [Google Scholar] [CrossRef]
- DeVore, G.R.; Satou, G.M.; Afshar, Y.; Harake, D.; Sklansky, M. Evaluation of Fetal Cardiac Size and Shape: A New Screening Tool to Identify Fetuses at Risk for Tetralogy of Fallot. J. Ultrasound Med. 2021, 40, 2537–2548. [Google Scholar] [CrossRef]
- DeVore, G.R.; Gumina, D.L.; Hobbins, J.C. Assessment of ventricular contractility in fetuses with an estimated fetal weight less than the tenth centile. Am. J. Obstet. Gynecol. 2019, 221, 498.e1–498.e22. [Google Scholar] [CrossRef]
- Georgiopoulos, G.; Nicolaides, K.H.; Charakida, M.; Sciences, I. Impact of Gestational Diabetes Mellitus on Fetal Cardiac Morphology and Function: Cohort Comparison of Second- and Third-Trimester Fetuses. Ultrasound Obstet. Gynecol. 2021, 57, 607–613. [Google Scholar] [CrossRef]
- Harbison, A.L.; Chmait, R.H.; Pruetz, J.D.; Ma, S.; Sklansky, M.S.; Devore, G.R. Evaluation of Cardiac Function in the Recipient Twin in Successfully Treated Twin-to-Twin Transfusion Syndrome Using a Novel Fetal Speckle-Tracking Analysis. Prenat. Diagn. 2021, 41, 136–144. [Google Scholar] [CrossRef]
- Bennasar, M.; Martínez, J.M.; Gómez, O.; Bartrons, J.; Olivella, A.; Puerto, B.; Gratacós, E. Accuracy of Four-Dimensional Spatiotemporal Image Correlation Echocardiography in the Prenatal Diagnosis of Congenital Heart Defects. Ultrasound Obstet. Gynecol. 2010, 36, 458–464. [Google Scholar] [CrossRef]
- Figueras, F.; Meler, E.; Iraola, A.; Eixarch, E.; Coll, O.; Figueras, J. Customized Birthweight Standards for a Spanish Population. Eur. J. Obs. Gynecol. Reprod. Biol. 2008, 136, 20–24. [Google Scholar] [CrossRef]
- Carvalho, J.S.; Allan, L.D.; Chaoui, R.; Copel, J.A.; DeVore, G.R.; Hecher, K.; Lee, W.; Munoz, H.; Paladini, D.; Tutschek, B.; et al. ISUOG Practice Guidelines (Updated): Sonographic Screening Examination of the Fetal Heart. Ultrasound Obstet. Gynecol. 2013, 41, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Salomon, L.J.; Alfirevic, Z.; Berghella, V.; Bilardo, C.; Hernandez-Andrade, E.; Johnsen, S.L.; Kalache, K.; Leung, K.-Y.; Malinger, G.; Munoz, H.; et al. Practice Guidelines for Performance of the Routine Mid-Trimester Fetal Ultrasound Scan. Ultrasound Obstet. Gynecol. 2011, 37, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Hadlock, F.P.; Harrist, R.B.; Shah, Y.P.; King, D.E.; Park, S.K.; Sharman, R.S. Estimating Fetal Age Using Multiple Parameters: A Prospective Evaluation in a Racially Mixed Population. Am. J. Obstet. Gynecol. 1987, 156, 955–957. [Google Scholar] [CrossRef]
- Guirado, L.; Crispi, F.; Soveral, I.; Valenzuela-alcaraz, B.; Rodriguez-López, M.; García-Otero, L.; Torres, X.; Sepúlveda-Martínez, Á.; Escobar-Diaz, M.C.; Martinez, J.M.; et al. Nomograms of Fetal Right Ventricular Fractional Area Change by 2D Echocardiography. Fetal Diagn. Ther. 2020, 47, 399–410. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J.-Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Devore, G.R.; Satou, G.; Sklansky, M. Using Speckle-Tracking Echocardiography to Assess Fetal Myocardial Deformation: Are We There yet? Yes We Are! Ultrasound Obs. Gynecol. 2019, 54, 703–704. [Google Scholar] [CrossRef]
- Devore, G.R.; Satou, G.; Sklansky, M. Comparing the Non-Quiver and Quiver Techniques for Identi Fi Cation of the Endocardial Borders Used for Speckle-Tracking Analysis of the Ventricles of the Fetal Heart. J. Ultrasound Med. 2020, 40, 1955–1961. [Google Scholar] [CrossRef]
- Watson, P.F.; Petrie, A. Method Agreement Analysis: A Review of Correct Methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef] [Green Version]
- Crispi, F.; Sepulveda-swatson, E.; Cruz-lemini, M. Original Paper: Techniques Feasibility and Reproducibility of a Standard Protocol for 2D Speckle Tracking and Tissue Doppler-Based Strain and Strain Rate Analysis of the Fetal Heart. Fetal Diagn. Ther. 2012, 32, 96–108. [Google Scholar] [CrossRef]
- Enzensberger, C.; Achterberg, F.; Degenhardt, J.; Wolter, A.; Graupner, O.; Herrmann, J.; Axt-fliedner, R. Feasibility and Reproducibility of Two-Dimensional Wall Motion Tracking ( WMT ) in Fetal Echocardiography Study Population. Ultrasound Int. Open 2017, 3, 26–33. [Google Scholar]
- Younoszai, A.K.; Saudek, D.E.; Emery, S.P.; Thomas, J.D. Evaluation of Myocardial Mechanics in the Fetus by Velocity Vector Imaging. J. Am. Soc. Echocardiogr. 2008, 21, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Belghiti, H.; Brette, S.; Lafitte, S.; Reant, P.; Picard, F.; Serri, K.; Lafitte, M.; Courregelongue, M.; Dos Santos, P.; Douard, H.; et al. Automated Function Imaging: A New Operator-Independent Strain Method for Assessing Left Ventricular Function Imagerie Paramétrique Fonctionnelle Automatique. Arch. Cardiovasc. Dis. 2008, 101, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Barker, P.C.A.; Houle, H.; Li, J.S.; Miller, S.; Herlong, J.R.; Camitta, M.G.W. Global Longitudinal Cardiac Strain and Strain Rate for Assessment of Fetal Cardiac Function: Novel Experience with Velocity Vector Imaging. Echocardiography 2009, 26, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Maskatia, S.A.; Pignatelli, R.H.; Ayres, N.A.; Altman, C.A.; Sangi-haghpeykar, H.; Lee, W. Longitudinal Changes and Interobserver Variability of Systolic Myocardial Deformation Values in a Prospective Cohort of Healthy Fetuses across Gestation and after Delivery. J. Am. Soc. Echocardiogr. 2016, 29, 341–349. [Google Scholar] [CrossRef]
- Huntley, E.S.; Hernandez-Andrade, E.; Soto, E.; Devore, G.; Sibai, B.M. Novel Speckle Tracking Analysis Showed Excellent Reproducibility for Size and Shape of the Fetal Heart and Good Reproducibility for Strain and Fractional Shortening. Fetal Diagn. Ther. 2021, 48, 541–550. [Google Scholar] [CrossRef]
- Hata, T.; Koyanagi, A.; Yamanishi, T.; Bouno, S.; Takayoshi, R. A 24-Segment Fractional Shortening of the Fetal Heart Using Fetal HQ. J. Perinat. Med. 2021, 49, 371–376. [Google Scholar] [CrossRef]
- Hata, T.; Koyanagi, A.; Yamanishi, T.; Bouno, S.; Ahmed, M.; Aboellail, M.; Miyake, T. Evaluation of 24-Segment Sphericity Index of Fetal Heart Using Fetal HQ. J. Matern. Neonatal Med. 2020, 1–7. [Google Scholar] [CrossRef]
- Luo, Y.; Xiao, F.; Long, C.; Kuang, H.; Jiang, M. Evaluation of the Sphericity Index of the Fetal Heart during Middle and Late Pregnancy Using FetalHQ. J. Matern. Neonatal Med. 2021, 1–6. [Google Scholar] [CrossRef]
- Dodaro, M.G.; Montaguti, E.; Balducci, A.; Perolo, A.; Angeli, E.; Lenzi, J.; Lombardo, L.; Donti, A.; Pilu, G.; Gaia, M.; et al. Fetal Speckle-Tracking Echocardiography: A Comparison between Two-Dimensional and Electronic Spatio-Temporal Image Correlation ( e- STIC ) Technique Two-Dimensional and Electronic Spatio-Temporal Image Correlation. J. Matern. Neonatal Med. 2021, 1–7. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Result |
|---|---|
| MATERNAL BASELINE CHARACTERISTICS | |
| Maternal age, years | 33.3 ± 6.16 |
| Body mass index, kg/m2 | 22.1 ± 2.5 |
| Chronic diseases (hypothyroidism, ulcerative colitis) | 2 (6.4%) |
| Race | |
| White | 28 (80%) |
| Latin American | 2 (5.7%) |
| Asian | 1 (2.9%) |
| Smoking habit | 1 (3.2%) |
| Nulliparity | 18 (58.1%) |
| Use of artificial reproductive technologies | 2 (6.5 %) |
| PERINATAL RESULTS | |
| Gestational age at birth, weeks | 39.5 ± 1.1 |
| Cesarean section | 3 (9.7%) |
| Birthweight, g | 3513 ± 417 |
| Birthweight centile | 53.7 ± 28 |
| Five minutes APGAR score below 7 | 0 (0%) |
| Data expressed as mean ± standard deviation, median (range) or n (%) | |
| Variable | ICC | 95% Confidence Interval | p-Value | ICC | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|---|
| FETAL CARDIAC MORPHOMETRY | ||||||
| Left Ventricle | Right Ventricle | |||||
| Ventricular Area | 0.976 | 0.950 to 0.988 | <0.001 | 0.970 | 0.936 to 0.986 | <0.001 |
| Longitudinal diameter | 0.933 | 0.862 to 0.968 | <0.001 | 0.970 | 0.938 to 0.9585 | <0.001 |
| Basal diameter (segment 1) | 0.853 | 0.696 to 0.929 | <0.001 | 0.855 | 0.702 to 0.930 | <0.001 |
| Mid-ventricular diameter (segment 9) | 0.924 | 0.841 to 0.964 | <0.001 | 0.936 | 0.867 to 0.969 | <0.001 |
| Apical diameter (segment 17) | 0.912 | 0.818 to 0.958 | <0.001 | 0.943 | 0.881 to 0.972 | <0.001 |
| Basal sphericity index (segment 1) | 0.440 | −0.201 to 0.736 | 0.067 | 0.526 | −0.042 to 0.872 | 0.061 |
| Mid-ventricular sphericity index (segment 9) | 0.702 | 0.392 to 0.855 | <0.001 | 0.665 | 0.298 to 0.840 | 0.002 |
| Apical sphericity index (segment 17) | 0.787 | 0.561 to 0.897 | <0.001 | 0.609 | 0.129 to 0.812 | 0.006 |
| FETAL CARDIAC FUNCTION | ||||||
| Left Ventricle | Right Ventricle | |||||
| Global longitudinal strain | 0.906 | 0.807 to 0.955 | <0.001 | 0.732 | 0.437 to 0.873 | <0.001 |
| Fractional area change | 0.845 | 0.665 to 0.926 | <0.001 | 0.746 | 0.482 to 0.877 | <0.001 |
| Basal shortening fraction (segment 1) | 0.302 | −0.561 to 0.684 | 0.188 | 0.775 | 0.526 to 0.895 | <0.001 |
| Mid-ventricular shortening fraction (Segment 9) | 0.748 | 0.472 to 0.879 | <0.001 | 0.801 | 0.579 to 0.906 | <0.001 |
| Apical shortening fraction (segment 17) | 0.805 | 0.599 to 0.906 | <0.001 | 0.619 | 0.188 to 0.820 | 0.007 |
| End-diastolic volume | 0.968 | 0.933 to 0.985 | <0.001 | |||
| End-systolic volume | 0.936 | 0.866 to 0.969 | <0.001 | |||
| Ejection fraction | 0.760 | 0.501 to 0.885 | <0.001 | |||
| Cardiac Output | 0.782 | 0.500 to 0.904 | <0.001 | |||
| Variable | ICC | 95% Confidence Interval | p-Value | ICC | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|---|
| FETAL CARDIAC MORPHOMETRY | ||||||
| Left Ventricle | Right Ventricle | |||||
| Ventricular area | 0.931 | 0.857 to 0.967 | <0.001 | 0.966 | 0.930 to 0.984 | <0.001 |
| Longitudinal diameter | 0.756 | 0.483 to 0.885 | <0.001 | 0.909 | 0.797 to 0.958 | <0.001 |
| Basal diameter (segment 1) | 0.746 | 0.464 to 0.881 | <0.001 | 0.891 | 0.751 to 0.950 | <0.001 |
| Mid-ventricular diameter (segment 9) | 0.841 | 0.666 to 0.924 | <0.001 | 0.921 | 0.835 to 0.962 | <0.001 |
| Apical diameter (segment 17) | 0.884 | 0.675 to 0.925 | <0.001 | 0.882 | 0.745 to 0.994 | <0.001 |
| Basal sphericity index (segment 1) | 0.390 | −0.161 to 0.694 | 0.064 | 0.333 | −0.227 to 0.659 | 0.095 |
| Mid-ventricular sphericity index (segment 9) | 0.495 | −0.11 to 0.754 | 0.027 | 0.683 | 0.329 to 0.850 | 0.001 |
| Apical sphericity index (segment 17) | 0.445 | −0.101 to 0.728 | 0.047 | 0.628 | 0.212 to 0.823 | 0.005 |
| FETAL CARDIAC FUNCTION | ||||||
| Left Ventricle | Right Ventricle | |||||
| Global longitudinal strain | 0.825 | 0.634 to 0.916 | <0.001 | 0.767 | 0.508 to 0.889 | <0.001 |
| Fractional area change | 0.831 | 0.646 to 0.920 | <0.001 | 0.843 | 0.671 to 0.925 | <0.001 |
| Basal shortening fraction (segment 1) | 0.116 | −0.951 to 0.595 | 0.378 | 0.506 | −0.055 to 0.772 | 0.036 |
| Mid-ventricular shortening fraction (Segment 9) | 0.742 | 0.466 to 0.875 | <0.001 | 0.666 | 0.303 to 0.839 | 0.002 |
| Apical shortening fraction (segment 17) | 0.782 | 0.554 to 0.894 | <0.001 | 0.745 | 0.476 to 0.876 | <0.001 |
| End-diastolic volume | 0.872 | 0.718 to 0.942 | <0.001 | |||
| End-systolic volume | 0.773 | 0.497 to 0.898 | <0.001 | |||
| Ejection fraction | 0.769 | 0.516 to 0.890 | <0.001 | |||
| Cardiac Output | 0.602 | 0.082 to 0.828 | 0.016 | |||
| Variable | ICC | 95% Confidence Interval | p-Value | ICC | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|---|
| CARDIAC MORPHOMETRY | ||||||
| Left Ventricle | Right Ventricle | |||||
| Ventricular area | 0.930 | 0.817 to 0.970 | <0.001 | 0.949 | 0.895 to 0.975 | <0.001 |
| Longitudinal diameter | 0.745 | 0.480 to 0.876 | <0.001 | 0.907 | 0.806 to 0.955 | <0.001 |
| Basal diameter (segment 1) | 0.833 | 0.529 to 0.930 | <0.001 | 0.912 | 0.803 to 0.959 | <0.001 |
| Mid-ventricular diameter (segment 9) | 0.858 | 0.461 to 0.947 | <0.001 | 0.825 | 0.638 to 0.915 | <0.001 |
| Apical diameter (segment 17) | 0.871 | 0.661 to 0.944 | <0.001 | 0.871 | 0.753 to 0.938 | <0.001 |
| Basal sphericity index (segment 1) | 0.222 | −0.401 to 0.601 | 0.211 | 0.637 | 0.226 to 0.823 | 0.003 |
| Mid-ventricular sphericity index (segment 9) | 0.463 | −0.062 to 0.737 | 0.018 | 0.738 | 0.457 to 0.873 | <0.001 |
| Apical sphericity index (segment 17) | 0.589 | 0.172 to 0.799 | 0.005 | 0.698 | 0.370 to 0.855 | 0.001 |
| CARDIAC FUNCTION | ||||||
| Left Ventricle | Right Ventricle | |||||
| Global longitudinal strain | 0.898 | 0.779 to 0.952 | <0.001 | 0.878 | 0.746 to 0.941 | <0.001 |
| Fractional area change | 0.682 | 0.350 to 0.846 | 0.001 | 0.667 | 0.307 to 0.842 | 0.002 |
| Basal shortening fraction (segment 1) | 0.643 | 0.227 to 0.838 | 0.003 | 0.339 | −0.521 to 0.710 | 0.163 |
| Mid-ventricular shortening fraction (Segment 9) | 0.387 | −0.196 to 0,695 | 0.078 | −0.05 | −1.1 to 0.493 | 0.553 |
| Apical shortening fraction (segment 17) | 0.501 | −0.021 to 0.758 | 0.030 | 0.480 | −0.091 to 0.752 | 0.043 |
| End-diastolic volume | 0.936 | 0.669 to 0.978 | <0.001 | |||
| End-systolic volume | 0.896 | 0.774 to 0.952 | <0.001 | |||
| Ejection fraction | 0.628 | 0.243 to 0.819 | 0.004 | |||
| Cardiac Output | 0.562 | −0.149 to 0.826 | 0.001 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogué, L.; Gómez, O.; Izquierdo, N.; Mula, C.; Masoller, N.; Martínez, J.M.; Gratacós, E.; Devore, G.; Crispi, F.; Bennasar, M. Feasibility of 4D-Spatio Temporal Image Correlation (STIC) in the Comprehensive Assessment of the Fetal Heart Using FetalHQ®. J. Clin. Med. 2022, 11, 1414. https://doi.org/10.3390/jcm11051414
Nogué L, Gómez O, Izquierdo N, Mula C, Masoller N, Martínez JM, Gratacós E, Devore G, Crispi F, Bennasar M. Feasibility of 4D-Spatio Temporal Image Correlation (STIC) in the Comprehensive Assessment of the Fetal Heart Using FetalHQ®. Journal of Clinical Medicine. 2022; 11(5):1414. https://doi.org/10.3390/jcm11051414
Chicago/Turabian StyleNogué, Laura, Olga Gómez, Nora Izquierdo, Cristina Mula, Narcís Masoller, Josep M. Martínez, Eduard Gratacós, Greggory Devore, Fàtima Crispi, and Mar Bennasar. 2022. "Feasibility of 4D-Spatio Temporal Image Correlation (STIC) in the Comprehensive Assessment of the Fetal Heart Using FetalHQ®" Journal of Clinical Medicine 11, no. 5: 1414. https://doi.org/10.3390/jcm11051414
APA StyleNogué, L., Gómez, O., Izquierdo, N., Mula, C., Masoller, N., Martínez, J. M., Gratacós, E., Devore, G., Crispi, F., & Bennasar, M. (2022). Feasibility of 4D-Spatio Temporal Image Correlation (STIC) in the Comprehensive Assessment of the Fetal Heart Using FetalHQ®. Journal of Clinical Medicine, 11(5), 1414. https://doi.org/10.3390/jcm11051414