
Better Control of Body Temperature Is Not Associated with Improved Hemodynamic and Respiratory Parameters in Mechanically Ventilated Patients with Sepsis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
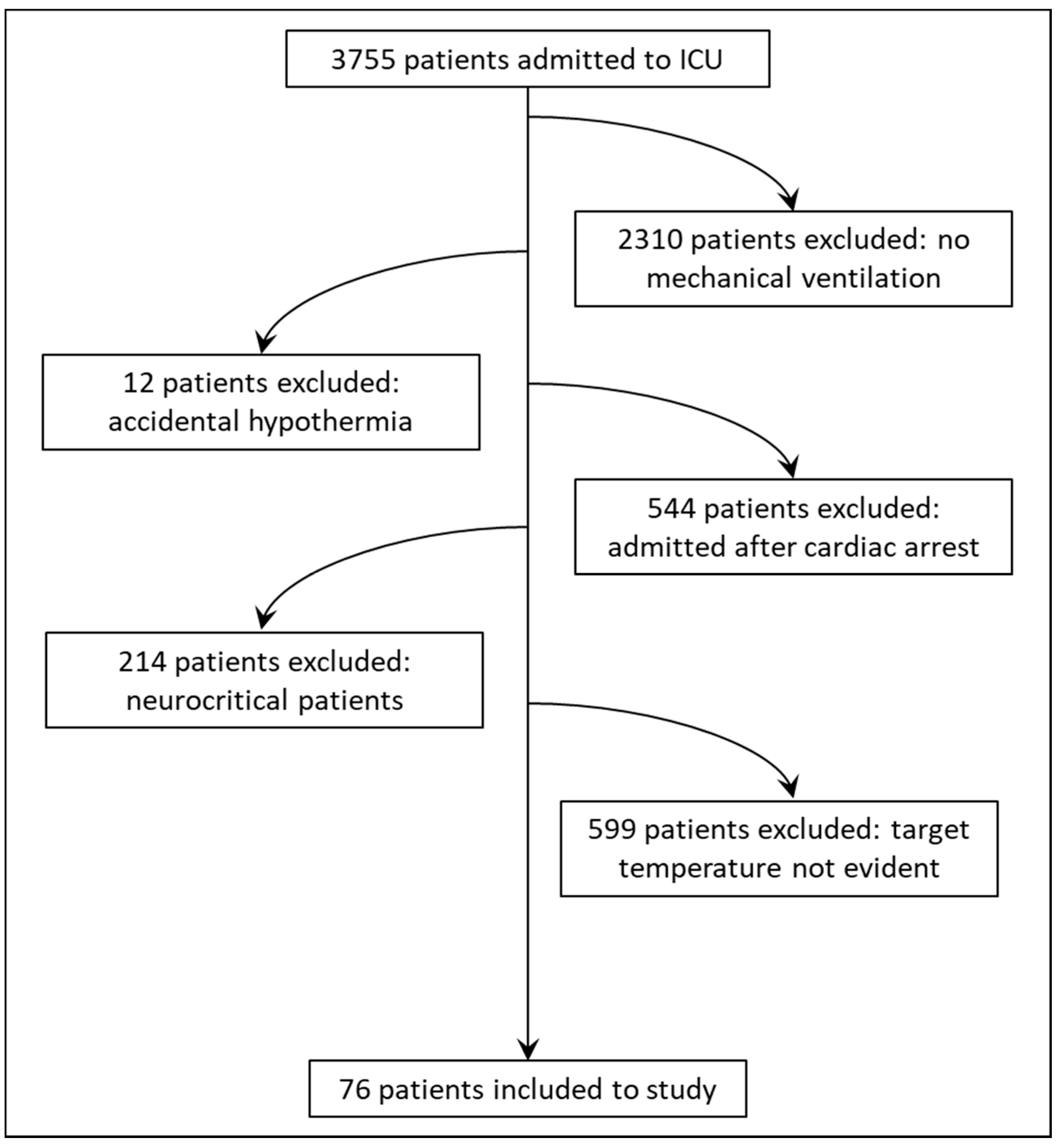
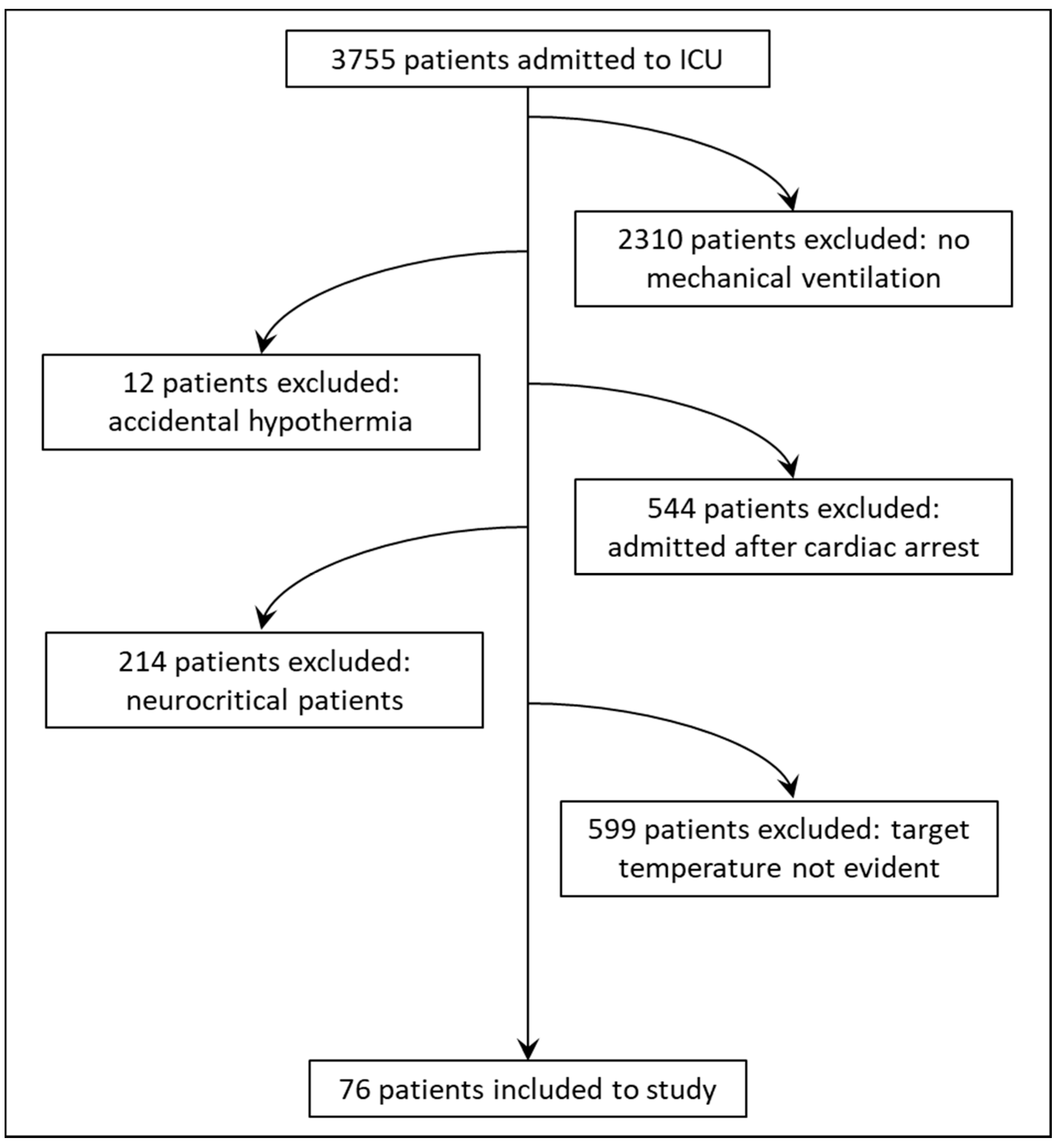
2.2. Study Population
2.3. Measurements
2.4. Statistical Analysis
3. Results
3.1. Time Outside the Target Temperature Range and ICU Course of Treatment
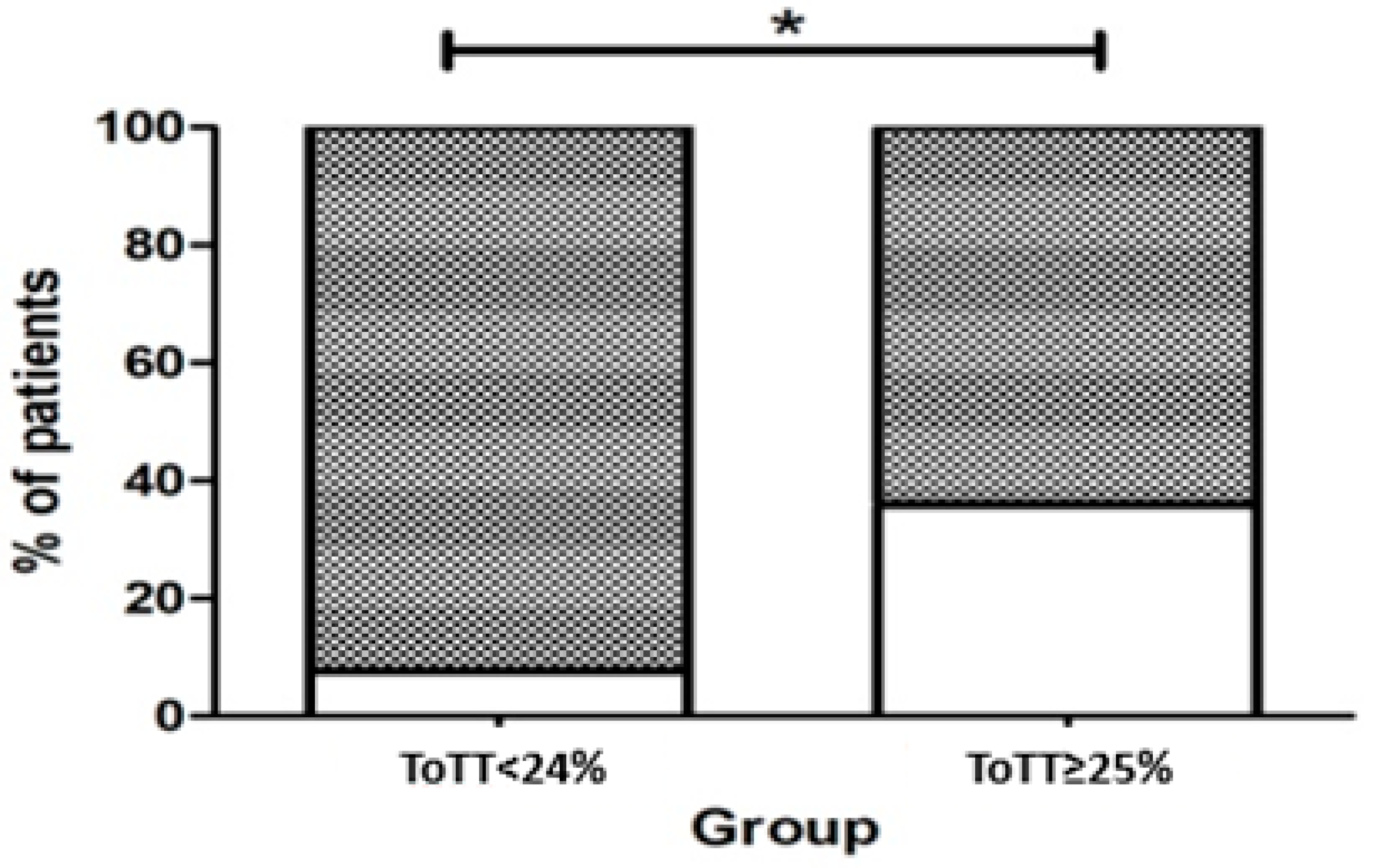
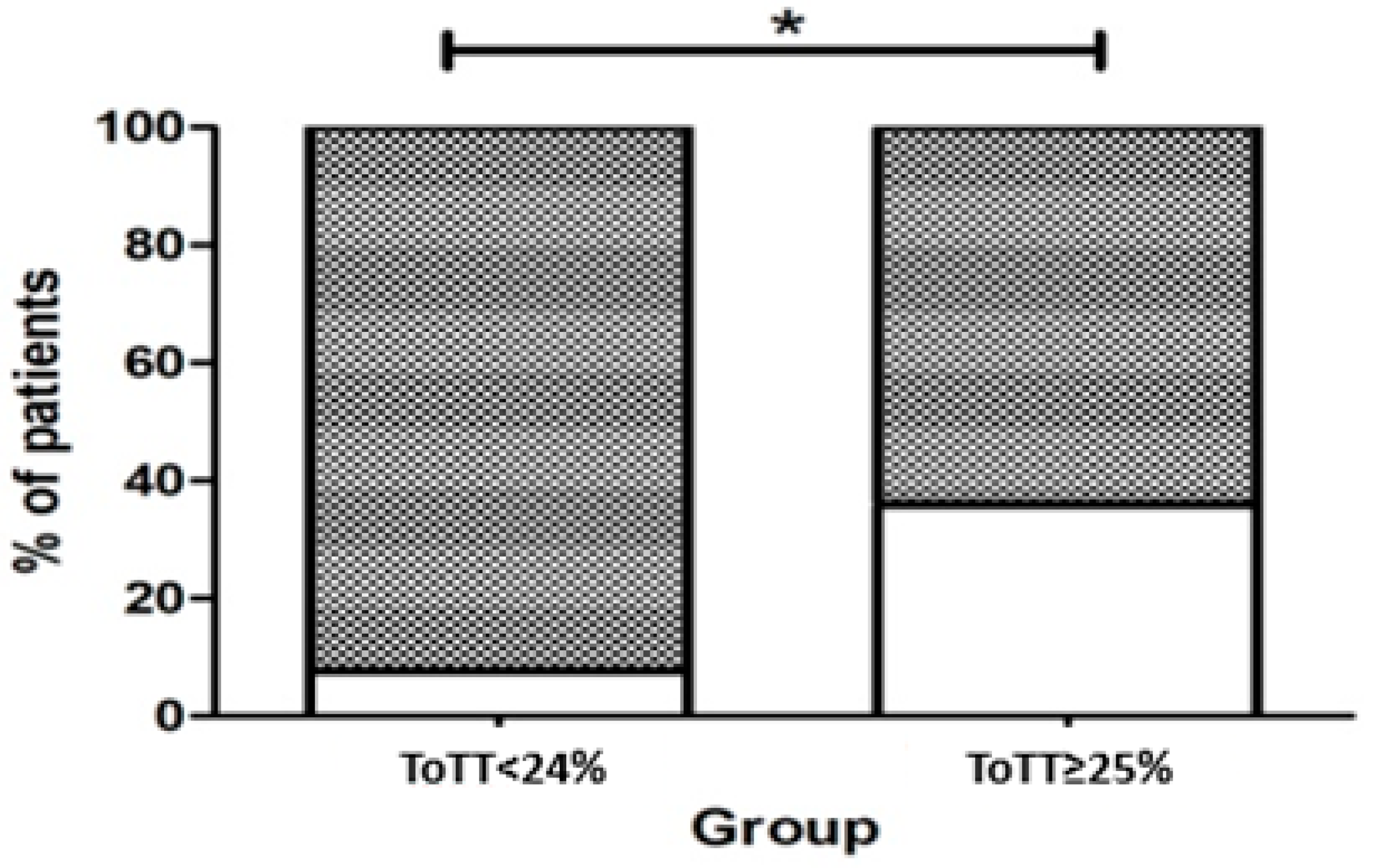
3.2. Association between Multidrug Resistant Pathogens and Time outside the Target Temperature
3.3. Other Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walter, E.J.; Hanna-Jumma, S.; Carraretto, M.; Forni, L. The pathophysiological basis and consequences of fever. Crit. Care 2016, 20, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laupland, K.B.; Shahpori, R.; Kirkpatrick, A.W.; Ross, T.; Gregson, D.B.; Stelfox, H.T. Occurrence and outcome of fever in critically ill adults. Crit. Care Med. 2008, 36, 1531–1535. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Sandroni, C.; Böttiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2021: Post-resuscitation care. Resuscitation 2021, 161, 220–269. [Google Scholar] [CrossRef] [PubMed]
- Madden, L.K.; Hill, M.; May, T.L.; Human, T.; Guanci, M.M.K.; Jacobi, J.; Moreda, M.V.; Badjatia, N. The Implementation of Targeted Temperature Management: An Evidence-Based Guideline from the Neurocritical Care Society. Neurocrit. Care 2017, 27, 468–487. [Google Scholar] [CrossRef] [PubMed]
- Skok, K.; Duh, M.; Stožer, A.; Markota, A.; Gosak, M. Thermoregulation: A journey from physiology to computational models and the intensive care unit. WIREs Mech. Dis. 2021, 13, e1513. [Google Scholar] [CrossRef] [PubMed]
- Markota, A.; Gosak, M.; Duh, M.; Skok, K. Temperature management and its role in cardiac arrest patients—A review. Signa Vitae 2021, 1–8. [Google Scholar] [CrossRef]
- Young, P.J.; Prescott, H.C. When less is more in the active management of elevated body temperature of ICU patients. Intensive Care Med. 2019, 45, 1275–1278. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J.L.; Creten, D. Perceptions of fever among adults in a family practice setting. J. Fam. Pract. 1986, 22, 427–430. [Google Scholar]
- Gozzoli, V.; Schöttker, P.; Suter, P.M.; Ricou, B. Is it worth treating fever in intensive care unit patients? Preliminary results from a randomized trial of the effect of external cooling. Arch. Intern. Med. 2001, 161, 121–123. [Google Scholar] [CrossRef]
- Frazer, J.S.; Barnes, G.E.; Woodcock, V.; Flanagan, E.; Littlewood, T.; Stevens, R.J.; Fleming, S.; Ashdown, H.F. Variability in body temperature in healthy adults and in patients receiving chemotherapy: Prospective observational cohort study. J. Med. Eng. Technol. 2019, 43, 323–333. [Google Scholar] [CrossRef]
- Mackowiak, P.A.; Wasserman, S.S.; Levine, M.M. A Critical Appraisal of 98.6°F, the Upper Limit of the Normal Body Temperature, and Other Legacies of Carl Reinhold August Wunderlich. JAMA J. Am. Med. Assoc. 1992, 268, 1578–1580. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maekawa, T.; Kaneda, K.; Tsuruta, R.; Kuroda, Y.; Nagao, K.; Rinka, H.; Takahashi, T.; Yokota, H.; Shirai, S.I.; Hase, M.; et al. Precision and Safety of an Intravascular Temperature Management System for Postcardiac Arrest Syndrome Patients: A Multicenter Clinical Trial (COOL-ARREST JP). Ther. Hypothermia Temp. Manag. 2020, 10, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Glover, G.W.; Thomas, R.M.; Vamvakas, G.; Al-Subaie, N.; Cranshaw, J.; Walden, A.; Wise, M.P.; Ostermann, M.; Thomas-Jones, E.; Cronberg, T.; et al. Intravascular versus surface cooling for targeted temperature management after out-of-hospital cardiac arrest—An analysis of the TTM trial data. Crit. Care 2016, 20, 381. [Google Scholar] [CrossRef] [Green Version]
- Levy, S.B.; Bonnie, M. Antibacterial resistance worldwide: Causes, challenges and responses. Nat. Med. 2004, 10, S122–S129. [Google Scholar] [CrossRef]
- Small, P.M.; Tauber, M.G.; Hackbarth, C.J.; Sande, M.A. Influence of body temperature on bacterial growth rates in experimental pneumococcal meningitis in rabbits. Infect. Immun. 1986, 52, 484–487. [Google Scholar] [CrossRef] [Green Version]
- Mackowiak, P.A.; Marling-Cason, M.; Cohen, R.L. Effects of temperature on antimicrobial susceptibility of bacteria. J. Infect. Dis. 1982, 145, 550–553. [Google Scholar] [CrossRef]
- Boulamery, A.; Marouani, H.; Guilhaumou, R.; Rocher, E.; Simon, N.; Bruguerolle, B. Effects of hyperthermia on pharmacokinetics of ertapenem in rats. Fundam. Clin. Pharmacol. 2008, 22, 285–289. [Google Scholar] [CrossRef]
- Beovič, B.; Mrhar, A.; Karba, R.; Župančič, T.; Grabnar, I.; Belič, A.; Marolt-Gomišček, M. Influence of fever on the pharmacokinetics of ciprofloxacin. Int. J. Antimicrob. Agents 1999, 11, 81–85. [Google Scholar] [CrossRef]
- Owens, C.A. The value of fever therapy for gonorrhea. J. Am. Med. Assoc. 1936, 107, 1942–1946. [Google Scholar] [CrossRef]
- Nobelprize.org. Julius Wagner-Jauregg-Biographical. Available online: https://www.nobelprize.org/prizes/medicine/1927/wagner-jauregg/biographical/ (accessed on 11 December 2021).
- Naiman, M.; Markota, A.; Hegazy, A.; Dingley, J.; Kulstad, E. Retrospective Analysis of Esophageal Heat Transfer for Active Temperature Management in Post-cardiac Arrest, Refractory Fever, and Burn Patients. Mil. Med. 2018, 183, 162–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, P.; Saxena, M.; Bellomo, R.; Freebairn, R.; Hammond, N.; van Haren, F.; Holliday, M.; Henderson, S.; Mackle, D.; McArthur, C.; et al. Acetaminophen for Fever in Critically Ill Patients with Suspected Infection. N. Engl. J. Med. 2015, 373, 2215–2224. [Google Scholar] [CrossRef] [PubMed]
- Sakkat, A.; Alquraini, M.; Aljazeeri, J.; Farooqi, M.A.M.; Alshamsi, F.; Alhazzani, W. Temperature control in critically ill patients with fever: A meta-analysis of randomized controlled trials. J. Crit. Care 2021, 61, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Zhu, J.; Yin, C.; Zhu, J.; Zhu, T.; Liu, L. Effects of target temperature management on the outcome of septic patients with fever. Biomed. Res. Int. 2017, 2017, 3906032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, F.; Nam, D.N.; Wang, Z.; Cai, Y.; Rogiers, P.; Vincent, J.L. Fever control in septic shock: Beneficial or harmful? Shock 2005, 23, 516–520. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic (n = 76) | Value |
|---|---|
| Demographics, severity of illness and outcome data | |
| Age in years (mean ± SD) | 64.4 ± 12.5 |
| BMI kg/m2 (mean ± SD) | 27.5 ± 3.9 |
| ICU LOS days (mean ± SD) | 21.8 ± 15.4 |
| APACHE II on admission (mean ± SD) | 26.1 ± 8.3 |
| Vasoactive-inotropic score max. (mean ± SD) | 85.0 ± 36.8 |
| Outcome of death in ICU (%) | 35 (46.1) |
| Core body temperature and temperature management data | |
| Temperature on admission (mean ± SD) | 38.0 ± 1.0 |
| Fever (>38.3 °C) prevalence N (%) | 62 (82) |
| Temperature before TTM (mean ± SD) | 40.0 ± 0.4 |
| ECD N (%) | 22 (28.9) |
| TTM duration in days (mean ± SD) | 5.0 ± 1.9 |
| Max. core body temperature during TTM (°C) (mean ± SD) | 39.2 ± 0.38 |
| % of ToTT (mean ± SD) | 27.5 ± 10.1 |
| % of time above 39 °C during TTM | 16.9 ± 7.4 |
| RRT N (%) | 28 (36.8) |
| Procedures–pharmacological therapy | |
| Acetaminophen g/day (mean ± SD) | 2.1 ± 0.93 |
| Noradrenaline max dose mcg/kg/h (mean ± SD) | 0.83 ± 0.23 |
| Procedures–mechanical ventilation | |
| PEEP max during TTM cmH2O (mean ± SD) | 11.5 ± 1.5 |
| FiO2 max during TTM % (mean ± SD) | 51.2 ± 10.8 |
| MV max during TTM L/min (mean ± SD) | 11.6 ± 2.4 |
| Complications, multidrug resistant pathogens | |
| Sacral pressure sores N (%) | 25 (32.9) |
| Upper GIT bleeding N (%) | 6 (7.9) |
| Erythrocyte transfusion number of bags (mean ± SD) | 2.8 ± 2,7 |
| MDRP present N (%) | 49 (75.4) |
| Parameter | β | Lower CI95 | Upper CI95 | p Value | Pbonferroni |
|---|---|---|---|---|---|
| Outcome of death (value: NO) | 0.134 | −0.962 | 1.231 | 0.810 | 1 |
| Acetaminophen | 1.62 | 0.747 | 2.49 | 2.8 × 10−4 | 0.00476 |
| Noradrenaline on day 1 of TTM | −0.411 | −2.209 | 1.387 | 0.654 | 1 |
| Noradrenaline during TTM | 0.253 | −1.987 | 2.492 | 0.825 | 1 |
| Noradrenaline last day of TTM | −7.275 | −13.743 | −0.807 | 0.027 | 0.459 |
| PEEP on day 1 of TTM | −0.165 | −0.428 | 0.098 | 0.219 | 1 |
| PEEP during TTM | −0.143 | −0.482 | 0.196 | 0.408 | 1 |
| PEEP last day of TTM | 0.020 | −0.273 | 0.313 | 0.893 | 1 |
| FiO2 on day 1 of TTM | 0.005 | −0.039 | 0.049 | 0.818 | 1 |
| FiO2 during TTM | 0.011 | −0.039 | 0.061 | 0.663 | 1 |
| FiO2 last day of TTM | −0.020 | −0.103 | 0.064 | 0.646 | 1 |
| MV max during TTM | 0.131 | −0.159 | 0.421 | 0.375 | 1 |
| Sacral pressure sores (value: NO) | 0.159 | −0.928 | 1.245 | 0.775 | 1 |
| GIT bleeding (value: NO) | −0.807 | −2.864 | 1.250 | 0.442 | 1 |
| Erythrocyte transfusion num of bags | −0.122 | −0.360 | 0.116 | 0.316 | 1 |
| Max core body temperature | −1.690 | −3.256 | −0.125 | 0.034 | 0.629 |
| % of time above 39 °C during TTM | 0.025 | −0.044 | 0.094 | 0.479 | 1 |
| Tracheal Aspirates (n of Positive Patients = 24) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Genus | Klebsiella | Enterococcus | Enterobacter | Pseudomonas | Acinetobacter | Staphylococcus | Candida | Proteus | Citrobacter | Raoultella | Stenotrophomonas | N |
| Number | 10 | 4 | 5 | 11 | 9 | 2 | 2 | 1 | 2 | 2 | 1 | 49 |
| % | 20.4 | 8.2 | 10.2 | 22.4 | 18.4 | 4.1 | 4.1 | 2.0 | 4.1 | 4.1 | 2.0 | |
| Nasopharynx swabs (n of positive patients = 23) | ||||||||||||
| Number | 6 | 3 | 1 | 6 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 20 |
| % | 30 | 15 | 5 | 30 | 10 | 10 | 0 | 0 | 0 | 0 | 0 | |
| Rectal swabs (n of positive patients = 23) | ||||||||||||
| Number | 12 | 9 | 9 | 9 | 3 | 2 | 0 | 0 | 3 | 0 | 0 | 47 |
| % | 25.5 | 19.1 | 19.1 | 19.1 | 6.4 | 4.3 | 0.0 | 0.0 | 6.4 | 0.0 | 0.0 | |
| Intravascular catheters (n of positive patients = 2) | ||||||||||||
| Number | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 |
| % | 0 | 50 | 50 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| All samples | ||||||||||||
| Number | 28 | 17 | 16 | 26 | 14 | 6 | 2 | 1 | 5 | 2 | 1 | 118 |
| % | 23.7 | 14.4 | 13.6 | 22.0 | 11.9 | 5.1 | 1.7 | 0.8 | 4.2 | 1.7 | 0.8 | |
| Parameter | β | Lower CI95 | Upper CI95 | p Value | Pbonferroni |
|---|---|---|---|---|---|
| ToTT (binomial) (value: NO) | 2.273 | 0.531 | 4.015 | 0.011 | 0.021 |
| Parameter | β | Lower CI95 | Upper CI95 | p Value | Pbonferroni |
|---|---|---|---|---|---|
| ToTT (binomial) (value: YES) | −5.613 | −8.441 | −2.785 | 1 × 10−4 | 2 × 10−4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markota, A.; Skok, K.; Kalamar, Ž.; Fluher, J.; Gorenjak, M. Better Control of Body Temperature Is Not Associated with Improved Hemodynamic and Respiratory Parameters in Mechanically Ventilated Patients with Sepsis. J. Clin. Med. 2022, 11, 1211. https://doi.org/10.3390/jcm11051211
Markota A, Skok K, Kalamar Ž, Fluher J, Gorenjak M. Better Control of Body Temperature Is Not Associated with Improved Hemodynamic and Respiratory Parameters in Mechanically Ventilated Patients with Sepsis. Journal of Clinical Medicine. 2022; 11(5):1211. https://doi.org/10.3390/jcm11051211
Chicago/Turabian StyleMarkota, Andrej, Kristijan Skok, Žiga Kalamar, Jure Fluher, and Mario Gorenjak. 2022. "Better Control of Body Temperature Is Not Associated with Improved Hemodynamic and Respiratory Parameters in Mechanically Ventilated Patients with Sepsis" Journal of Clinical Medicine 11, no. 5: 1211. https://doi.org/10.3390/jcm11051211
APA StyleMarkota, A., Skok, K., Kalamar, Ž., Fluher, J., & Gorenjak, M. (2022). Better Control of Body Temperature Is Not Associated with Improved Hemodynamic and Respiratory Parameters in Mechanically Ventilated Patients with Sepsis. Journal of Clinical Medicine, 11(5), 1211. https://doi.org/10.3390/jcm11051211