
Prognostic Role of Pre-Treatment Metabolic Parameters and Sarcopenia Derived by 2-[18F]-FDG PET/CT in Elderly Mantle Cell Lymphoma

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. 2-[18F]-FDG PET/CT Imaging and Interpretation
2.3. Sarcopenia Analysis
2.4. Statistical Analysis
3. Results
3.1. Patients Features
3.2. Sarcopenic Analysis
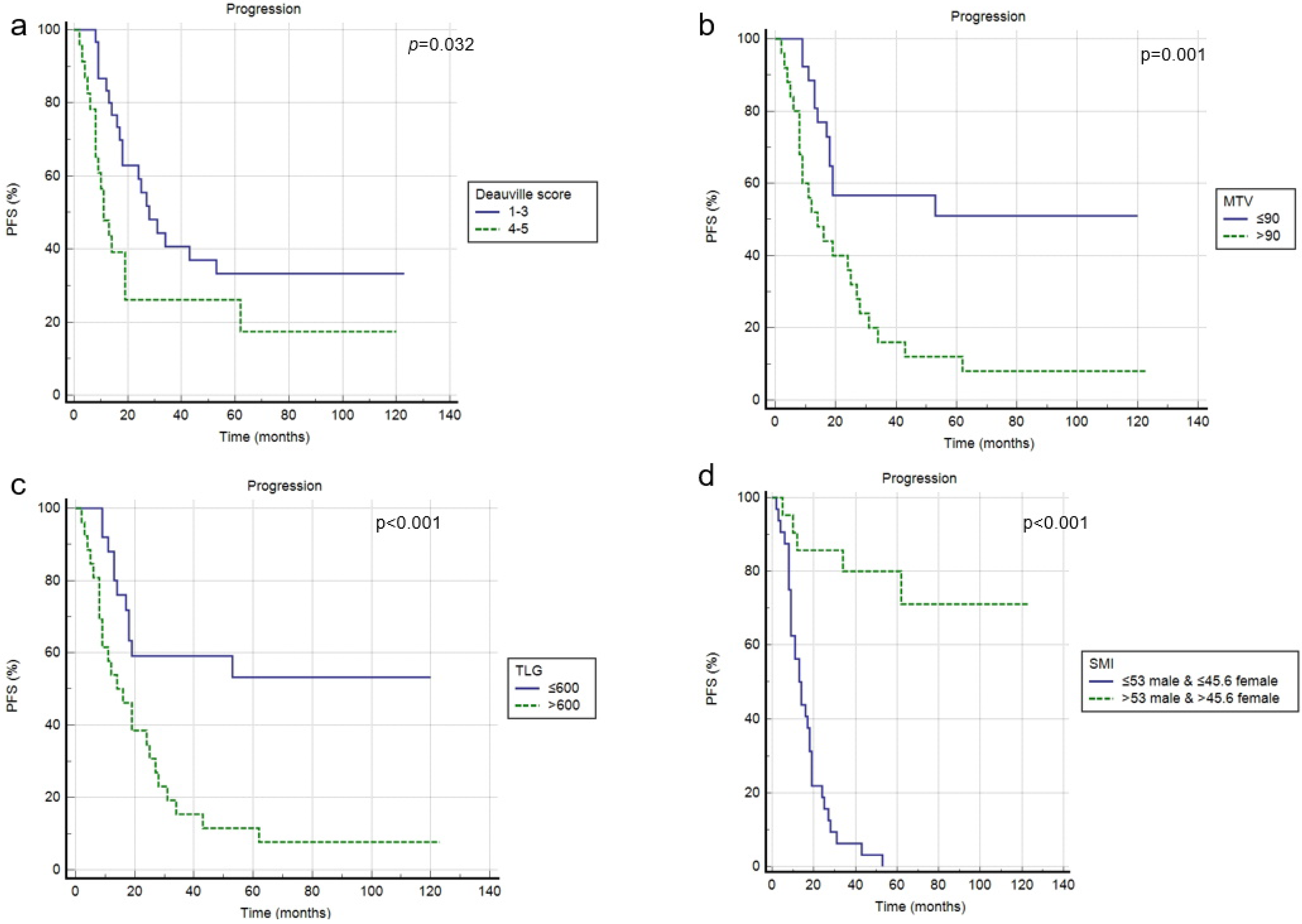
3.3. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.A.; Stein, H.; Thiele, J. World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues; IARC Press: Lyon, France, 2008. [Google Scholar]
- Maddocks, K. Update on Mantle cell lymphoma. Blood 2018, 132, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Lynch, D.T.; Koya, S.; Acharya, U. Mantle Cell Lymphoma. 9 August 2021. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Doordujin, J.K.; Kluin-Nelemans, H. Mangement of mantle cell lymphoma in the elderly patient. Clin. Interv. Aging 2013, 8, 1229–1236. [Google Scholar]
- Hoster, E.; Dreyling, M.; Klapper, W.; Gisselbrecht, C.; van Hoof, A.; Kluin-Nelemans, H.C.; Pfreundschuh, M.; Reiser, M.; Metzner, B.; Einsele, H.; et al. A new prognostic index (MIPI) for patients with advanced-stage mantle cell lymphoma. Blood 2008, 111, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.J.; Fayad, L.; Romaguera, J. Mantle Cell International Prognostic Index (MIPI) not prognostic after R-hyper-CVAD. Blood 2008, 112, 2583–2584. [Google Scholar] [CrossRef]
- Albano, D.; Treglia, G.; Gazzilli, M.; Cerudelli, E.; Giubbini, R.; Bertagna, F. 18F-FDG PET or PET/CT in Mantle Cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2020, 20, 422–430. [Google Scholar] [CrossRef]
- Mato, A.R.; Svodoba, J.; Feldman, T.; Zielonka, T.; Agress, H.; Panush, D.; Miller, M.; Toth, P.; Lizotte, P.M.; Nasta, S.; et al. Post-treatment (not interim) positron emission tomography-computed tomography scan status is highly predictive of outcome in mantle cell lymphoma patients treated with R-HyperCVAD. Cancer 2012, 118, 3565–3570. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bosio, G.; Bianchetti, N.; Pagani, C.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in mantle cell lymphoma. Ann. Nucl. Med. 2019, 33, 449–458. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Riedl, C.C.; Kumar, A.; Gibbs, P.; Weber, M.; Tal, I.; Schilksy, J.; Schoder, H. Radiomic features of glucose metabolism enable prediction of outcome in mantle cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2760–2769. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- Albano, D.; Dondi, F.; Ravanelli, M.; Tucci, A.; Farina, D.; Giubbini, R.; Treglia, G.; Bertagna, F. Prognostic Role of “Radiological” Sarcopenia in Lymphoma: A Systematic Review. Clin. Lymphoma Myeloma Leuk. 2021. [Google Scholar] [CrossRef] [PubMed]
- Zilioli, V.R.; Albano, D.; Arcari, A.; Merli, F.; Coppola, A.; Besutti, G.; Marcheselli, L.; Gramegna, D.; Muzi, C.; Manicone, M.; et al. Clinical and prognostic role of sarcopenia in elderly patients with classical Hodgkin lymphoma: A multicentre experience. J. Cachexia Sarcopenia Muscle 2021, 12, 1042–1055. [Google Scholar] [CrossRef]
- Burkart, M.; Schieber, M.; Basu, S.; Shah, P.; Venugopal, P.; Borgia, J.A.; Gordon, L.; Karmali, R. Evaluation of the impact of cachexia on clinical outcomes in aggressive lymphoma. Br. J. Haematol. 2019, 186, 45–53. [Google Scholar] [CrossRef]
- Karmali, R.; Alrifai, T.; Fughhi, I.A.M.; Shah, P.; Venugopal, P.; Borgia, J.A.; Gordon, L.; Karmali, R. Impact of cachexia on outcomes in aggressive lymphomas. Ann. Hematol. 2017, 96, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Iukuridze, A.; The, J.B.; Mascarenhas, K.; Herrera, A.; McCune, J.S.; Zain, J.M.; Mostoufi-Moab, S.; McCormack, S.; Slavin, T.P.; et al. Abnormal body composition is a predic- tor of adverse outcomes after autologous haematopoietic cell transplantation. J. Cachexia Sarcopenia Muscle 2020, 11, 962–972. [Google Scholar] [CrossRef] [PubMed]
- Caram, M.V.; Bellile, E.L.; Englesbe, M.J.; Terjimanian, M.; Wang, S.C.; Griggs, J.J.; Couriel, D. Sarcopenia is associated with autologous transplant-related outcomes in patients with lymphoma. Leuk. Lymphoma 2015, 56, 2855–2862. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of imaging in the staging and response assessment of lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Kamarajah, S.K.; Bundred, J.; Tan, B.H.L. Body composition assessment and sarcopenia in patients with gastric cancer: A systematic review and meta-analysis. Gastric Cancer 2019, 22, 10–22. [Google Scholar] [CrossRef]
- Deng, H.Y.; Zha, P.; Peng, L.; Hou, L.; Huang, K.L.; Li, X.Y. Preoperative sarcopenia is a predictor of poor prognosis of esophageal cancer after esophagectomy: A comprehensive systematic review and meta-analysis. Dis. Esophagus 2019, 32, doy115. [Google Scholar] [CrossRef] [PubMed]
- Mintziras, I.; Miligkos, M.; Wachter, S.; Manoharan, J.; Maurer, E.; Bartsch, D.K. Sarcopenia and sarcopenic obesity are significantly associated with poorer overall survival in patients with pancreatic cancer: Systematic review and meta-analysis. Int. J. Surg. 2018, 59, 19–26. [Google Scholar] [CrossRef]
- Sun, G.; Li, Y.; Peng, Y.; Lu, D.; Zhang, F.; Cui, X.; Zhang, Q.; Li, Z. Can sarcopenia be a predictor of prognosis for patients with non-metastatic colorectal cancer? A systematic review and meta-analysis. Int. J. Colorectal. Dis. 2018, 33, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Wienke, A. Sarcopenia predicts overall survival in patients with malignant hematological diseases: A meta-analysis. Clin. Nutr. 2021, 40, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Fielding, R.; Visser, M.; van Loon, L.J.; Rolland, Y.; Orwoll, E.; Reid, K.; Boonen, S.; Dere, W.; Epstein, S.; et al. Tools in the assessment of sarcopenia. Calcif. Tissue Int. 2013, 93, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Sinelnikov, A.; Qu, C.; Fetzer, D.T.; Pelletier, J.S.; Dunn, M.A.; Tsung, A.; Furlan, A. Measurement of skeletal muscle area: Comparison of CT and MR imaging. Eur. J. Radiol. 2016, 85, 1716–1721. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Camoni, L.; Rinaldi, R.; Tucci, A.; Zilioli, V.R.; Muzi, C.; Ravanelli, M.; Farina, D.; Coppola, A.; Camalori, M.; et al. Comparison between skeletal muscle and adipose tissue measurements with high-dose CT and low-dose attenuation correction CT of 18F-FDG PET/CT in elderly Hodgkin lymphoma patients: A two-centre validation. Br. J. Radiol. 2021, 94, 20200672. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Wang, M. Blastoid Mantle Cell Lymphoma. Hematol. Oncol. Clin. N. Am. 2020, 34, 941–956. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Laudicella, R.; Ferro, P.; Allocca, M.; Abenavoli, E.; Buschiazzo, A.; Castellino, A.; Chiaravalloti, A.; Cuccaro, A.; Cuppari, L.; et al. The Role of 18F-FDG PET/CT in Staging and Prognostication of Mantle Cell Lymphoma: An Italian Multicentric Study. Cancers 2019, 11, 1831. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients n (%) | Average ± SD (Range) | |
|---|---|---|
| Age (years) | 72.7 ± 5.6 (66–88) | |
| Sex male | 39 (74%) | |
| Sex female | 14 (26%) | |
| BMI | 26.15 ± 4.4 (16.8–34.8) | |
| Tumor stage at diagnosis (Ann Arbor) | ||
| I | 0 (0%) | |
| II | 4 (7.5%) | |
| III | 4 (7.5%) | |
| IV | 45 (85%) | |
| B symptoms | 10 (19%) | |
| Blastoid variant | 7 (13%) | |
| Bulky disease | 6 (11%) | |
| LDH ≤ 245 | 34 (64%) | |
| >245 | 19 (36%) | |
| β 2 microglobulin ≤ 2.8 | 35 (66%) | |
| >2.8 | 18 (34%) | |
| Ki-67 score ≤ 15% | 22 (44%) | |
| >15% | 28 (56%) | |
| MIPI score ≤ 2 | 12 (23%) | |
| (>2) | 41 (77%) | |
| SUVbw | 9.6 ± 5.3 (3.3–27) | |
| SUVlbm | 7.4 ± 4.4 (2.4–22.3) | |
| SUVbsa | 2.4 ± 1.4 (0.9–7.3) | |
| Lesion to BP SUVmax ratio | 6.2 ± 8.8 (1.7–54) | |
| Lesion to liver SUVmax ratio | 5.3 ± 6.8 (1–44) | |
| tMTV | 358 ± 481 (3–1800) | |
| tTLG | 2023 ± 3147 (10–20,088) | |
| SMI | 49.9 ± 7.7 (36.3–67) | |
| for male | 53.1 ± 6.3 (39–67) | |
| for female | 42 ± 3.4 (36.3–46.3) |
| Sarcopenia n = 32 | Not Sarcopenia n = 21 | p Value | |
|---|---|---|---|
| Male:Female | 21:13 | 18:1 | 0.001 |
| Age (mean ± SD) | 73.4 ± 5.7 | 71.4 ± 5.2 | 0.338 |
| BMI | 25.8 | 26.6 | 0.801 |
| Tumor stage advanced | 29 (91%) | 19 (90%) | 0.985 |
| Bulky disease | 4 (12.5%) | 2 (10%) | 0.745 |
| Splenomegaly | 14 (44%) | 6 (29%) | 0.093 |
| Blastoid variant | 7 (22%) | 0 (0%) | 0.021 |
| LDH (mean ± SD) | 276 ± 264 | 208 ± 83 | 0.257 |
| β 2 microglobulin (mean ± SD) | 4.5 ± 5.5 | 2.44 ± 2 | 0.526 |
| MIPI score > 2 | 10 (31%) | 5 (24%) | 0.288 |
| Complete metabolic response | 17 (57%) | 13 (62%) | 0.537 |
| SUVbw (mean ± SD) | 8.7 ± 4.9 | 10.8 ± 5.7 | 0.139 |
| SUVlbm (mean ± SD) | 6.7 ± 4 | 8.35 ± 4.8 | 0.144 |
| SUVbsa (mean ± SD) | 2.2 ± 1.3 | 2.7 ± 1.6 | 0.160 |
| Lesion to BP SUVmax ratio (mean ± SD) | 4.7 ± 5.7 | 6.3 ± 10 | 0.411 |
| Lesion to liver SUVmax ratio (mean ± SD) | 5.4 ± 4.8 | 7.4 ± 9 | 0.402 |
| tMTV (mean ± SD) | 470 ± 57 | 192 ± 34 | 0.040 |
| tTLG (mean ± SD) | 2726 ± 378 | 985 ± 138 | 0.033 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| p Value | HR (95% CI) | p Value | HR (95% CI) | |
| PFS | ||||
| Sex | 0.299 | 1.358 (0.500–2.333) | ||
| Age | 0.298 | 1.225 (0.284–2.585) | ||
| MIPI score | 0.582 | 1.989 (0.500–4.212) | ||
| LDH level | 0.121 | 0.610 (0.292–1.154) | ||
| Β2 microglobulin | 0.895 | 1.053 (0.476–2.333) | ||
| Bulky disease | 0.458 | 0.124 (0.102–1.715) | ||
| Splenomegaly | 0.248 | 1.582 (0.123–3.002) | ||
| Blastoid variant | 0.015 | 1.292 (1.101–1.500) | 0.102 | 1.250 (0.888–1.650) |
| Deauville score | 0.032 | 2.155 (1.068–4.351) | 0.042 | 2.255 (1.250–3.690) |
| SUVbw * | 0.555 | 1.446 (0.759–3.042) | ||
| SUVlbm * | 0.434 | 1.111 (0.534–2.126) | ||
| SUVbsa * | 0.331 | 1.459 (0.339–2.856) | ||
| L-L SUV R * | 0.450 | 1.107 (0.756–2.122) | ||
| L-BP SUV R * | 0.324 | 1.222 (0.444–4.235) | ||
| tMTV * | 0.001 | 3.190 (1.568–6.374) | 0.039 | 2.833 (1.053–7.619) |
| tTLG * | <0.001 | 3.258 (1.638–6.479) | 0.022 | 2.075 (0.889–4.843) |
| SMI * | <0.001 | 0.125 (0.062–0.253) | <0.001 | 0.031 (0.007–0.132) |
| R-BAC vs other | 0.401 | 0.852 (0.222–1.589) | ||
| OS | ||||
| Sex | 0.211 | 1.666 (0.389–5.026) | ||
| Age | 0.375 | 1.389 (0.445–3.005) | ||
| MIPI score | 0.690 | 0.987 (0.666–1.589) | ||
| LDH level | 0.480 | 0.825 (0.450–1.454) | ||
| Β2 microglobulin | 0.333 | 0.858 (0.420–1.689) | ||
| Bulky disease | 0.387 | 1.258 (0.555–2.297) | ||
| Splenomegaly | 0.222 | 1.359 (0.801–1.987) | ||
| Blastoid variant | 0.342 | 0.659 (0.350–1.259) | ||
| Deauville score | 0.402 | 1.404 (0.596–3.310) | ||
| SUVbw * | 0.453 | 0.816 (0.464–1.408) | ||
| SUVlbm * | 0.160 | 0.698 (0.368–1.179) | ||
| SUVbsa * | 0.207 | 0.677 (0.363–1.245) | ||
| L-L SUV R * | 0.125 | 0.689 (0.376–1.127) | ||
| L-BP SUV R * | 0.307 | 0.631 (0.306–1.452) | ||
| tMTV * | 0.028 | 0.374 (0.172–0.811) | 0.129 | 0.563 (0.105–1.009) |
| tTLG * | 0.049 | 0.448 (0.207–0.970) | 0.062 | 0.550 (0.102–1.120) |
| SMI * | 0.262 | 1.574 (0.736–3.365) | ||
| R-BAC vs. other | 0.396 | 0.701 (0.386–1.499) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albano, D.; Pasinetti, N.; Dondi, F.; Giubbini, R.; Tucci, A.; Bertagna, F. Prognostic Role of Pre-Treatment Metabolic Parameters and Sarcopenia Derived by 2-[18F]-FDG PET/CT in Elderly Mantle Cell Lymphoma. J. Clin. Med. 2022, 11, 1210. https://doi.org/10.3390/jcm11051210
Albano D, Pasinetti N, Dondi F, Giubbini R, Tucci A, Bertagna F. Prognostic Role of Pre-Treatment Metabolic Parameters and Sarcopenia Derived by 2-[18F]-FDG PET/CT in Elderly Mantle Cell Lymphoma. Journal of Clinical Medicine. 2022; 11(5):1210. https://doi.org/10.3390/jcm11051210
Chicago/Turabian StyleAlbano, Domenico, Nadia Pasinetti, Francesco Dondi, Raffaele Giubbini, Alessandra Tucci, and Francesco Bertagna. 2022. "Prognostic Role of Pre-Treatment Metabolic Parameters and Sarcopenia Derived by 2-[18F]-FDG PET/CT in Elderly Mantle Cell Lymphoma" Journal of Clinical Medicine 11, no. 5: 1210. https://doi.org/10.3390/jcm11051210
APA StyleAlbano, D., Pasinetti, N., Dondi, F., Giubbini, R., Tucci, A., & Bertagna, F. (2022). Prognostic Role of Pre-Treatment Metabolic Parameters and Sarcopenia Derived by 2-[18F]-FDG PET/CT in Elderly Mantle Cell Lymphoma. Journal of Clinical Medicine, 11(5), 1210. https://doi.org/10.3390/jcm11051210