
Non-Alcoholic Fatty Liver Disease and Risk of Macro- and Microvascular Complications in Patients with Type 2 Diabetes

 , , and
, , and
Abstract
:1. Introduction
2. Biological Link between Non-Alcoholic Fatty Liver Disease (NAFLD) and Cardiovascular Disease (CVD)
- (a)
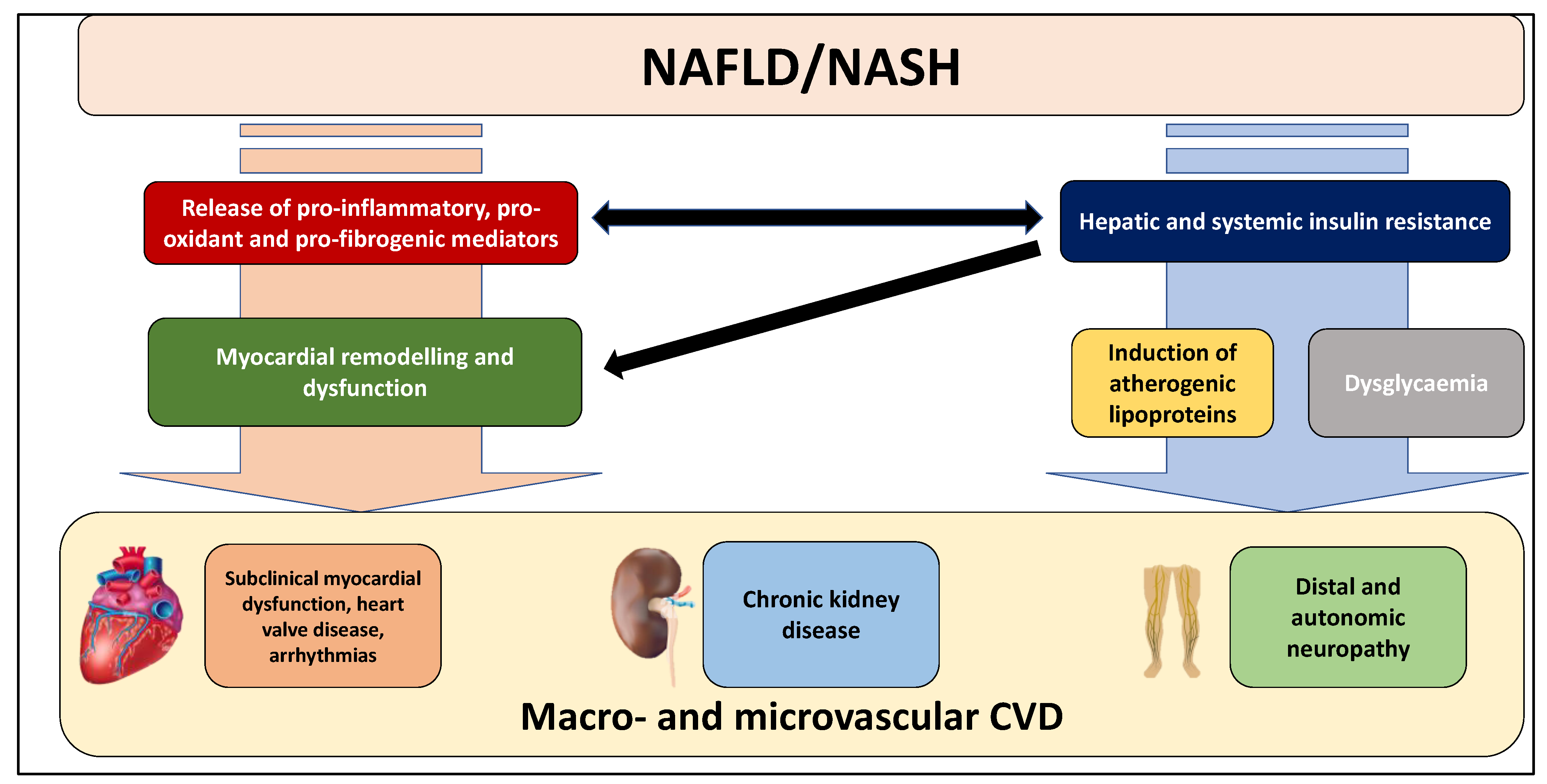
- hepatic lipid accumulation (e.g., di-acyl glycerol [DAG]) in NAFLD patients impairs insulin signalling, thereby conditioning insulin resistance (IR) through different mechanisms, including the inhibition of phosphorylation of insulin receptor substrate-1 (IRS-1) [18] and the activation of protein kinase C (PKC)-e that can inhibit the action of insulin receptor and promote the lipid accumulation [19]. In particular, hepatic and systemic insulin resistance is one of the primary mechanisms for inducing atherogenic lipoproteins and dysglycaemia. Notably, both atherogenic dyslipidemia and dysglycaemia mediate CVD risk in NAFLD patients with T2DM;
- (b)
- the release into the bloodstream of several pro-inflammatory (e.g., tumour necrosis factor-a [TNF-a], interleukin-6 [IL-6]), pro-oxidant and pro-coagulant factors (e.g., fibrinogen, factor VIII, plasminogen activator inhibitor-1) as well as pro-fibrogenic mediators. In particular, the synthesis of lipids, including DAG, may also contribute to the hepatic production of inflammatory cytokines and pro-coagulant factors [13,20,21,22];
- (c)
- the bidirectional relationship between NAFLD and hypertension [23]. Several observational studies and some meta-analyses have reported that patients with NAFLD have an increased risk of developing hypertension [24], thus suggesting that this association may partly mediate the relationship between NAFLD and cardiac complications and that that NAFLD may be a consequence, but also a cause of hypertension [23];
- (d)
- (e)
- chronic hyperglycemia induces an inflammatory and osteoblastic phenotype in valvular interstitial cells in experimental models of aortic valve sclerosis [27]. Increased valvular inflammation, through a systemic inflammatory state, could also mediate the increased cardiac valve sclerosis in NAFLD patients, independent of the presence of T2DM;
- (f)
- experimental data also indicate that NAFLD, mainly when advanced stages occur, may contribute to the activation of multiple pathways involved in the pathophysiology of CKD [10,28]. In this regard, atherogenic dyslipidaemia, hypertension, insulin resistance, oxidative stress and pro-inflammatory factors that, as mentioned above, are promoted and exacerbated by NAFLD status, may directly contribute to the vascular and renal damage [28]. Moreover, impaired activation of the renin-angiotensin system (RAS) may also contribute to the renovascular injury by inflammation pathways [28]. Finally, accumulating evidence also suggests a potential and independent association between PNPLA3 (patatin like phospholipase domain containing-3) rs738409, which is the most important polymorphism associated with NAFLD and its advanced forms [29], and kidney dysfunction [28].
3. Risk of Microvascular Complications
3.1. Chronic Kidney Disease (CKD)
3.2. Distal Symmetric Polyneuropathy and Autonomic Neuropathy
3.3. Diabetic Retinopathy
4. Risk of Macrovascular Complications
4.1. Sub-Clinical Myocardial Remodelling and Dysfunction, Heart Valve Diseases and Cardiac Arrhythmias
4.2. Fatal and Non-Fatal Cardiovascular Events
5. CVD Risk Assessment in Patients with NAFLD
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Lonardo, A.; Mantovani, A.; Lugari, S.; Targher, G. Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity. Ann Hepatol. 2020, 19, 359–366. [Google Scholar] [CrossRef]
- Sheka, A.C.; Adeyi, O.; Thompson, J.; Hameed, B.; Crawford, P.A.; Ikramuddin, S. Nonalcoholic Steatohepatitis: A Review. JAMA 2020, 323, 1175–1183. [Google Scholar] [CrossRef]
- Byrne, C.D.; Patel, J.; Scorletti, E.; Targher, G. Tests for diagnosing and monitoring non-alcoholic fatty liver disease in adults. BMJ 2018, 362, k2734. [Google Scholar] [CrossRef] [Green Version]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.-F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus, P. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef]
- Ayada, I.; van Kleef, L.A.; Alferink, L.J.M.; Li, P.; de Knegt, R.J.; Pan, Q. Systematically comparing epidemiological and clinical features of MAFLD and NAFLD by meta-analysis: Focusing on the non-overlap groups. Liver Int. 2021, 42, 277–287. [Google Scholar] [CrossRef]
- Mantovani, A. MAFLD vs NAFLD: Where are we? Dig. Liver Dis. 2021, 53, 1368–1372. [Google Scholar] [CrossRef]
- Mantovani, A.; Dalbeni, A. NAFLD, MAFLD and DAFLD. Dig. Liver Dis. 2020, 52, 1519–1520. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62 (Suppl. S1), S47–S64. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Csermely, A.; Petracca, G.; Beatrice, G.; Corey, K.E.; Simon, T.G.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: An updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 903–913. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident diabetes mellitus: An updated meta-analysis of 501 022 adult individuals. Gut 2021, 70, 962–969. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Lonardo, A.; Schattenberg, J.M.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and risk of incident chronic kidney disease: An updated meta-analysis. Gut 2020, 71, 156–162. [Google Scholar] [CrossRef]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and increased risk of incident extrahepatic cancers: A meta-analysis of observational cohort studies. Gut 2021. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Insulin resistance, inflammation, and non-alcoholic fatty liver disease. Trends Endocrinol. Metab. 2008, 19, 371–379. [Google Scholar] [CrossRef]
- Cantley, J.L.; Yoshimura, T.; Camporez, J.P.G.; Zhang, D.; Jornayvaz, F.; Kumashiro, N.; Guebre-Egziabher, F.; Jurczak, M.; Kahn, M.; Guigni, B.; et al. CGI-58 knockdown sequesters diacylglycerols in lipid droplets/ER-preventing diacylglycerol-mediated hepatic insulin resistance. Proc. Natl. Acad. Sci. USA 2013, 110, 1869–1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Liu, J.; Zhou, F.; Li, H.; Zhang, X.-J.; She, Z.-G.; Lu, Z.; Cai, J.; Li, H. Nonalcoholic Fatty Liver Disease: An Emerging Driver of Cardiac Arrhythmia. Circ. Res. 2021, 128, 1747–1765. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Bai, L.; Zhang, X.; Li, H.; Cai, J. Nonalcoholic Fatty Liver Disease and Cardiac Remodeling Risk: Pathophysiological Mechanisms and Clinical Implications. Hepatology 2021, 74, 2839–2847. [Google Scholar] [CrossRef]
- Anstee, Q.M.; Mantovani, A.; Tilg, H.; Targher, G. Risk of cardiomyopathy and cardiac arrhythmias in patients with nonalcoholic fatty liver disease. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2017, 68, 335–352. [Google Scholar] [CrossRef]
- Ciardullo, S.; Grassi, G.; Mancia, G.; Perseghin, G. Nonalcoholic fatty liver disease and risk of incident hypertension: A systematic review and meta-analysis. Eur. J. Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Byrne, C.D.; Benfari, G.; Bonapace, S.; Simon, T.G.; Targher, G. Risk of Heart Failure in Patients With Nonalcoholic Fatty Liver Disease: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 79, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Alon, L.; Corica, B.; Raparelli, V.; Cangemi, R.; Basili, S.; Proietti, M.; Romiti, G.F. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Manduteanu, I.; Simionescu, D.; Simionescu, A.; Simionescu, M. Aortic valve disease in diabetes: Molecular mechanisms and novel therapies. J. Cell. Mol. Med. 2021, 25, 9483–9495. [Google Scholar] [CrossRef]
- Wang, T.-Y.; Wang, R.-F.; Bu, Z.-Y.; Targher, G.; Byrne, C.D.; Sun, D.-Q.; Zheng, M.-H. Association of metabolic dysfunction-associated fatty liver disease with kidney disease. Nat. Rev. Nephrol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Valenti, L.; Romeo, S. Genetics and epigenetics of NAFLD and NASH: Clinical impact. J. Hepatol. 2017, 68, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. NAFLD as a driver of chronic kidney disease. J. Hepatol. 2020, 72, 785–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Zaza, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Bonora, E.; Targher, G. Nonalcoholic fatty liver disease increases risk of incident chronic kidney disease: A systematic review and meta-analysis. Metabolism 2017, 79, 64–76. [Google Scholar] [CrossRef]
- Ciardullo, S.; Ballabeni, C.; Trevisan, R.; Perseghin, G. Liver Stiffness, Albuminuria and Chronic Kidney Disease in Patients with NAFLD: A Systematic Review and Meta-Analysis. Biomolecules 2022, 12, 105. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Zusi, C.; Dalbeni, A.; Grani, G.; Buzzetti, E. Risk of Kidney Dysfunction IN Nafld. Curr. Pharm. Des. 2020, 26, 1045–1061. [Google Scholar] [CrossRef]
- Jang, H.R.; Kang, D.; Sinn, D.H.; Gu, S.; Cho, S.J.; Lee, J.E.; Huh, W.; Paik, S.W.; Ryu, S.; Chang, Y.; et al. Nonalcoholic fatty liver disease accelerates kidney function decline in patients with chronic kidney disease: A cohort study. Sci. Rep. 2018, 8, 4718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilar-Gomez, E.; Bertot, L.C.; Friedman, S.L.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Villa-Jimenez, O.; Vallin, S.L.-D.; Diago, M.; Adams, L.A.; Romero-Gómez, M.; et al. Improvement in liver histology due to lifestyle modification is independently associated with improved kidney function in patients with non-alcoholic steatohepatitis. Aliment. Pharmacol. Ther. 2016, 45, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Oniki, K.; Saruwatari, J.; Izuka, T.; Kajiwara, A.; Morita, K.; Sakata, M.; Otake, K.; Ogata, Y.; Nakagawa, K. Influence of the PNPLA3 rs738409 Polymorphism on Non-Alcoholic Fatty Liver Disease and Renal Function among Normal Weight Subjects. PLoS ONE 2015, 10, e0132640. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Taliento, A.; Zusi, C.; Baselli, G.A.; Prati, D.; Granata, S.; Zaza, G.; Colecchia, A.; Maffeis, C.; Byrne, C.D.; et al. PNPLA3 I148M gene variant and chronic kidney disease in type 2 diabetic patients with NAFLD: Clinical and experimental findings. Liver Int. 2020, 40, 1130–1141. [Google Scholar] [CrossRef]
- Sun, D.Q.; Zheng, K.I.; Xu, G.; Ma, H.L.; Zhang, H.Y.; Pan, X.Y.; Zhu, P.W.; Wang, X.D.; Targher, G.; Byrne, C.D.; et al. PNPLA3 rs738409 is associated with renal glomerular and tubular injury in NAFLD patients with persistently normal ALT levels. Liver Int. 2020, 40, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Zusi, C. PNPLA3 gene and kidney disease. Explor. Med. 2020, 1, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Mantovani, A.; Alisi, A.; Mosca, A.; Panera, N.; Byrne, C.D.; Nobili, V. Relationship Between PNPLA3 rs738409 Polymorphism and Decreased Kidney Function in Children With NAFLD. Hepatology 2019, 70, 142–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzuillo, P.; Di Sessa, A.; Guarino, S.; Capalbo, D.; Umano, G.R.; Pedullà, M.; La Manna, A.; Cirillo, G.; Del Giudice, E.M. Nonalcoholic fatty liver disease and eGFR levels could be linked by the PNPLA3 I148M polymorphism in children with obesity. Pediatr. Obes. 2019, 14, e12539. [Google Scholar] [CrossRef]
- Di Costanzo, A.; Pacifico, L.; D’Erasmo, L.; Polito, L.; Di Martino, M.; Perla, F.M.; Iezzi, L.; Chiesa, C.; Arca, M.; Costanzo, D.; et al. Nonalcoholic Fatty Liver Disease (NAFLD), But not Its Susceptibility Gene Variants, Influences the Decrease of Kidney Function in Overweight/Obese Children. Int. J. Mol. Sci. 2019, 20, 4444. [Google Scholar] [CrossRef] [Green Version]
- Sun, D.-Q.; Jin, Y.; Wang, T.-Y.; Zheng, K.I.; Rios, R.S.; Zhang, H.-Y.; Targher, G.; Byrne, C.D.; Yuan, W.-J.; Zheng, M.-H. MAFLD and risk of CKD. Metabolism 2021, 115, 154433. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Mu, B.; Guan, Y.; Liu, X.; Zhao, N.; Pan, D.; Wang, S. Assessment of the relationship between non-alcoholic fatty liver disease and diabetic complications. J. Diabetes Investig. 2016, 7, 889–894. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.H.; Burns, K.; Constantino, M.; Shackel, N.A.; Prakoso, E.; Wong, J.; Wu, T.; George, J.; McCaughan, G.W.; Twigg, S.M. An association of large-fibre peripheral nerve dysfunction with non-invasive measures of liver fibrosis secondary to non-alcoholic fatty liver disease in diabetes. J. Diabetes Complicat. 2015, 29, 1240–1247. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, R.; Airaghi, L.; Targher, G.; Serviddio, G.; Maffi, G.; Mantovani, A.; Maffeis, C.; Colecchia, A.; Villani, R.; Rinaldi, L.; et al. Liver fibrosis by FibroScan® independently of established cardiovascular risk parameters associates with macrovascular and microvascular complications in patients with type 2 diabetes. Liver Int. 2020, 40, 347–354. [Google Scholar] [CrossRef] [PubMed]
- LLv, W.-S.; Sun, R.-X.; Gao, Y.-Y.; Wen, J.-P.; Pan, R.-F.; Li, L.; Wang, J.; Xian, Y.-X.; Cao, C.-X.; Zheng, M. Nonalcoholic fatty liver disease and microvascular complications in type 2 diabetes. World J. Gastroenterol. 2013, 19, 3134–3142. [Google Scholar] [CrossRef]
- Kim, B.-Y.; Jung, C.-H.; Mok, J.-O.; Kang, S.K.; Kim, C.-H. Prevalences of diabetic retinopathy and nephropathy are lower in Korean type 2 diabetic patients with non-alcoholic fatty liver disease. J. Diabetes Investig. 2014, 5, 170–175. [Google Scholar] [CrossRef] [Green Version]
- Houghton, D.; Zalewski, P.; Hallsworth, K.; Cassidy, S.; Thoma, C.; Avery, L.; Slomko, J.; Hardy, T.; Burt, A.D.; Tiniakos, D.; et al. The degree of hepatic steatosis associates with impaired cardiac and autonomic function. J. Hepatol. 2019, 70, 1203–1213. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Mantovani, A.; Grander, C.; Foco, L.; Motta, B.; Byrne, C.D.; Pramstaller, P.P.; Tilg, H. Association between non-alcoholic fatty liver disease and impaired cardiac sympathetic/parasympathetic balance in subjects with and without type 2 diabetes—The Cooperative Health Research in South Tyrol (CHRIS)-NAFLD sub-study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 3464–3473. [Google Scholar] [CrossRef]
- Targher, G.; Bertolini, L.; Rodella, S.; Zoppini, G.; Lippi, G.; Day, C.; Muggeo, M. Non-alcoholic fatty liver disease is independently associated with an increased prevalence of chronic kidney disease and proliferative/laser-treated retinopathy in type 2 diabetic patients. Diabetologia 2008, 51, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Song, D.; Li, C.; Wang, Z.; Zhao, Y.; Shen, B.; Zhao, W. Association of non-alcoholic fatty liver disease with diabetic retinopathy in type 2 diabetic patients: A meta-analysis of observational studies. J. Diabetes Investig. 2021, 12, 1471–1479. [Google Scholar] [CrossRef]
- Targher, G.; Bertolini, L.; Padovani, R.; Rodella, S.; Tessari, R.; Zenari, L.; Day, C.; Arcaro, G. Prevalence of Nonalcoholic Fatty Liver Disease and Its Association With Cardiovascular Disease Among Type 2 Diabetic Patients. Diabetes Care 2007, 30, 1212–1218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D. Clinical Review: Nonalcoholic fatty liver disease: A novel cardiometabolic risk factor for type 2 diabetes and its complications. J. Clin. Endocrinol. Metab. 2013, 98, 483–495. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Byrne, C.D.; Tilg, H. NAFLD and increased risk of cardiovascular disease: Clinical associations, pathophysiological mechanisms and pharmacological implications. Gut 2020, 69, 1691–1705. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Pernigo, M.; Bergamini, C.; Bonapace, S.; Lipari, P.; Pichiri, I.; Bertolini, L.; Valbusa, F.; Barbieri, E.; Zoppini, G.; et al. Nonalcoholic Fatty Liver Disease Is Independently Associated with Early Left Ventricular Diastolic Dysfunction in Patients with Type 2 Diabetes. PLoS ONE 2015, 10, e0135329. [Google Scholar] [CrossRef]
- Borges-Canha, M.; Neves, J.S.; Libânio, D.; Von-Hafe, M.; Vale, C.; Araújo-Martins, M.; Leite, A.R.; Pimentel-Nunes, P.; Carvalho, D.; Leite-Moreira, A. Association between nonalcoholic fatty liver disease and cardiac function and structure—a meta-analysis. Endocrine 2019, 66, 467–476. [Google Scholar] [CrossRef]
- VanWagner, L.B.; Wilcox, J.E.; Ning, H.; Lewis, C.E.; Carr, J.J.; Rinella, M.E.; Shah, S.J.; Lima, J.A.C.; Lloyd-Jones, D.M. Longitudinal Association of Non-Alcoholic Fatty Liver Disease With Changes in Myocardial Structure and Function: The CARDIA Study. J. Am. Hear Assoc. 2020, 9, e014279. [Google Scholar] [CrossRef]
- Dong, Y.; Huang, D.; Sun, L.; Wang, Y.; Li, Y.; Chang, W.; Li, G.; Cui, H. Assessment of left ventricular function in type 2 diabetes mellitus patients with non-alcoholic fatty liver disease using three-dimensional speckle-tracking echocardiography. Anatol. J. Cardiol. 2020, 23, 41–48. [Google Scholar] [CrossRef]
- Chang, W.; Wang, Y.; Sun, L.; Yu, N.; Li, Y.; Li, G. Evaluation of left atrial function in type 2 diabetes mellitus patients with nonalcoholic fatty liver disease by two-dimensional speckle tracking echocardiography. Echocardiography 2019, 36, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Pernigo, M.; Bergamini, C.; Bonapace, S.; Lipari, P.; Valbusa, F.; Bertolini, L.; Zenari, L.; Pichiri, I.; Dauriz, M.; et al. Heart valve calcification in patients with type 2 diabetes and nonalcoholic fatty liver disease. Metabolism 2015, 64, 879–887. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Targher, G.; Zoppini, G.; Cicoira, M.; Bonapace, S.; Negri, C.; Stoico, V.; Faggiano, P.; Vassanelli, C.; Bonora, E. Aortic and Mitral Annular Calcifications Are Predictive of All-Cause and Cardiovascular Mortality in Patients With Type 2 Diabetes. Diabetes Care 2012, 35, 1781–1786. [Google Scholar] [CrossRef] [Green Version]
- Minhas, A.M.; Usman, M.S.; Khan, M.S.; Fatima, K.; Mangi, M.A.; Illovsky, M.A. Link Between Non-Alcoholic Fatty Liver Disease and Atrial Fibrillation: A Systematic Review and Meta-Analysis. Cureus 2017, 9, e1142. [Google Scholar] [CrossRef] [Green Version]
- Wijarnpreecha, K.; Boonpheng, B.; Thongprayoon, C.; Jaruvongvanich, V.; Ungprasert, P. The association between non-alcoholic fatty liver disease and atrial fibrillation: A meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2017, 41, 525–532. [Google Scholar] [CrossRef]
- Mantovani, A.; Dauriz, M.; Sandri, D.; Bonapace, S.; Zoppini, G.; Tilg, H.; Byrne, C.D.; Targher, G. Association between non-alcoholic fatty liver disease and risk of atrial fibrillation in adult individuals: An updated meta-analysis. Liver Int. 2019, 39, 758–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, H.; Liu, X.; Cheng, F. Relationship between non-alcoholic fatty liver disease and cardiac arrhythmia: A systematic review and meta-analysis. J. Int. Med. Res. 2021, 49, 3000605211047074. [Google Scholar] [CrossRef]
- Donnellan, E.; Cotter, T.G.; Wazni, O.M.; Elshazly, M.B.; Kochar, A.; Wilner, B.; Patel, D.; Kanj, M.; Hussein, A.; Baranowski, B.; et al. Impact of Nonalcoholic Fatty Liver Disease on Arrhythmia Recurrence Following Atrial Fibrillation Ablation. JACC Clin. Electrophysiol. 2020, 6, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Valbusa, F.; Bonapace, S.; Bertolini, L.; Zenari, L.; Pichiri, I.; Mantovani, A.; Zoppini, G.; Bonora, E.; Barbieri, E.; et al. Association of nonalcoholic fatty liver disease with QTc interval in patients with type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Rigolon, R.; Pichiri, I.; Bonapace, S.; Morani, G.; Zoppini, G.; Bonora, E.; Targher, G. Nonalcoholic fatty liver disease is associated with an increased risk of heart block in hospitalized patients with type 2 diabetes mellitus. PLoS ONE 2017, 12, e0185459. [Google Scholar] [CrossRef]
- Mantovani, A. Nonalcoholic Fatty Liver Disease (NAFLD) and Risk of Cardiac Arrhythmias: A New Aspect of the Liver-heart Axis. J. Clin. Transl. Hepatol. 2017, 5, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Rigamonti, A.; Bonapace, S.; Bolzan, B.; Pernigo, M.; Morani, G.; Franceschini, L.; Bergamini, C.; Bertolini, L.; Valbusa, F.; et al. Nonalcoholic Fatty Liver Disease Is Associated With Ventricular Arrhythmias in Patients With Type 2 Diabetes Referred for Clinically Indicated 24-Hour Holter Monitoring. Diabetes Care 2016, 39, 1416–1423. [Google Scholar] [CrossRef] [Green Version]
- Mantovani, A.; Scorletti, E.; Mosca, A.; Alisi, A.; Byrne, C.D.; Targher, G. Complications, morbidity and mortality of nonalcoholic fatty liver disease. Metabolism 2020, 111, 154170. [Google Scholar] [CrossRef]
- Paik, J.M.; Henry, L.; De Avila, L.; Younossi, E.; Racila, A.; Younossi, Z.M. Mortality Related to Nonalcoholic Fatty Liver Disease Is Increasing in the United States. Hepatol. Commun. 2019, 3, 1459–1471. [Google Scholar] [CrossRef] [Green Version]
- Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease is a risk factor for cardiovascular and cardiac diseases: Further evidence that a holistic approach to treatment is needed. Gut 2021. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Lonardo, A.; Byrne, C.D. Nonalcoholic fatty liver disease and chronic vascular complications of diabetes mellitus. Nat. Rev. Endocrinol. 2018, 14, 99–114. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Morrison, A.E.; Zaccardi, F.; Khunti, K.; Davies, M.J. Causality between non-alcoholic fatty liver disease and risk of cardiovascular disease and type 2 diabetes: A meta-analysis with bias analysis. Liver Int. 2019, 39, 557–567. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhong, G.-C.; Tan, H.-Y.; Hao, F.-B.; Hu, J.-J. Nonalcoholic fatty liver disease and mortality from all causes, cardiovascular disease, and cancer: A meta-analysis. Sci. Rep. 2019, 9, 11124. [Google Scholar] [CrossRef] [Green Version]
- Simon, T.G.; Roelstraete, B.; Khalili, H.; Hagström, H.; Ludvigsson, J.F. Mortality in biopsy-confirmed nonalcoholic fatty liver disease: Results from a nationwide cohort. Gut 2021, 70, 1375–1382. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Björnsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated With Long-term Outcomes of Patients With Nonalcoholic Fatty Liver Disease. Gastroenterology 2015, 149, 389–397.e10. [Google Scholar] [CrossRef] [Green Version]
- Ekstedt, M.; Hagström, H.; Nasr, P.; Fredrikson, M.; Stål, P.; Kechagias, S.; Hultcrantz, R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015, 61, 1547–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Targher, G.; Corey, K.E.; Byrne, C.D. NAFLD, and cardiovascular and cardiac diseases: Factors influencing risk, prediction and treatment. Diabetes Metab. 2020, 47, 101215. [Google Scholar] [CrossRef]
- Kim, D.; Konyn, P.; Sandhu, K.K.; Dennis, B.B.; Cheung, A.C.; Ahmed, A. Metabolic dysfunction-associated fatty liver disease is associated with increased all-cause mortality in the United States. J. Hepatol. 2021, 75, 1284–1291. [Google Scholar] [CrossRef]
- Mantovani, A.; Valenti, L. A call to action for fatty liver disease. Liver Int. 2021, 41, 1182–1185. [Google Scholar] [CrossRef]
- Mantovani, A.; Dalbeni, A. Treatments for NAFLD: State of Art. Int. J. Mol. Sci. 2021, 22, 2350. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C.D.; Targher, G. Efficacy of peroxisome proliferator-activated receptor agonists, glucagon-like peptide-1 receptor agonists, or sodium-glucose cotransporter-2 inhibitors for treatment of non-alcoholic fatty liver disease: A systematic review. Lancet Gastroenterol. Hepatol. 2022. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C.D.; Scorletti, E.; Mantzoros, C.S.; Targher, G. Efficacy and safety of anti-hyperglycaemic drugs in patients with non-alcoholic fatty liver disease with or without diabetes: An updated systematic review of randomized controlled trials. Diabetes Metab. 2020, 46, 427–441. [Google Scholar] [CrossRef] [PubMed]
- Dufour, J.-F.; Caussy, C.; Loomba, R. Combination therapy for non-alcoholic steatohepatitis: Rationale, opportunities and challenges. Gut 2020, 69, 1877–1884. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Author, Ref. | Main Study Characteristics | Main Results |
|---|---|---|
| Fatal and non-fatal cardiovascular events | ||
| Targher G et al. J. Hepatol. 2016; 65: 589–600. | 16 observational studies were included for a total of 34,043 individuals with and without T2DM | NAFLD was associated with an increased risk of fatal and/or non-fatal CVD (random-effects odds ratio 1.64, 95% confidence interval 1.26–2.13). Patients with more severe forms of NAFLD were also more likely to develop fatal and non-fatal CVD events (random-effects odds ratio 2.58; 95% confidence interval 1.78–3.75) |
| Morrison AE et al. Liver Int. 2019; 39: 557–567. | 13 observational studies were included | NAFLD was not associated with an increased risk of CVD (random-effects risks ratio 1.48, 95% confidence interval 0.96–2.29) |
| Liu Y et al. Sci Rep. 2019; 9: 11124 | 14 observational studies were included for a total of 498,501 individuals with and without T2DM | NAFLD was associated with an increased risk of all-cause mortality (random-effects hazard ratio 1.34; 95% confidence interval 1.17–1.54), but not with an increased risk of CVD (random-effects hazard ratio 1.13; 95% confidence interval 0.92–1.38) |
| Mantovani A et al. Lancet Gastroenterol Hepatol. 2021; 6: 903–913 | 36 longitudinal studies were included for a total of 5,802,226 middle-aged individuals with and without T2DM | NAFLD was associated with an increased risk of fatal or non-fatal CVD events (random-effects hazard ratio 1.45, 95% confidence interval 1.31–1.61). This risk increased progressively across the severity of NAFLD, especially the stage of fibrosis (random-effects hazard ratio 2.50, 95% confidence interval 1.68–3.72) |
| Alon L et al. Eur J Prev Cardiol. 2021 Dec 22: zwab212. doi: 10.1093/eurjpc/zwab212. | 20 observational studies were included | NAFLD was associated with an increased risk of myocardial infarction (random-effects odds ratio 1.66, 95% confidence interval 1.39–1.99), ischemic stroke (random-effects odds ratio 1.41, 95% confidence interval 1.29–1.55), atrial fibrillation (random-effects odds ratio 1.27, 95% confidence interval 1.18–1.37), and heart failure (random-effects odds ratio 1.62, 95% confidence interval 1.43–1.84) |
| Cardiac function and structure | ||
| Borges-Canha M et al. Endocrine 2019; 66: 467–476. | 16 observational studies were included | NAFLD was associated with increased risk of (a) higher left ventricle mass and ratios between left ventricle mass and both height and body surface area; (b) higher left ventricular end diastolic diameter; (c) higher left atrium diameter and ratio between left atrial volume and body surface area; (d) higher posterior wall and septum thickness; (e) lower E/A wave ratio; (f) higher E/E′ ratio; (g) longer deceleration time and (h) longer relaxation time |
| Cardiac arrhythmias | ||
| Minhas AM et al. Cureus 2017; 9: e1142. | 3 observational studies were included for a total of 1,044 with NAFLD and 1,016 without NAFLD | Patients with NAFLD had a higher risk of AF (random-effects odds ratio 2.47, 95% confidence interval 1.30–4.66) |
| Wijarnpreecha K et al. Clin Res Hepatol Gastroenterol. 2017; 41: 525–532 | 5 observational studies (2 cross-sectional ones and 3 cohort ones) were included for a total of 238,129 participants with and without T2DM | Patients with NAFLD had a higher risk of AF (random-effects risks ratio 2.06, 95% confidence interval 1.10–3.85) |
| Mantovani A. et al. Liver Int. 2019; 39: 758–769 | 9 observational studies (5 cross-sectional ones and 4 cohort ones) were included for a total of 364,919 individuals with and without T2DM | NAFLD was associated with an increased risk of prevalent AF (random-effects odds ratio 2.07, 95% confidence interval 1.38–3.10). Conversely, NAFLD was associated with increased risk of incident AF only in T2DM patients (random-effects hazard ratio 4.96, 95% confidence interval 1.42–17.3). |
| Gong H et al. J. Int. Med. Res. 2021; 49: 3000605211047074 | 19 observational studies were included for a total of 7,012,960 individuals with and without T2DM | NAFLD was associated with higher risks of AF (random-effects odds ratio 1.71, 95% confidence interval 1.14–2.57), prolonged QT interval (random-effects odds ratio 2.86, 95% confidence interval 1.64–4.99), premature atrial/ventricular contraction (random-effects odds ratio 2.53, 95% confidence interval 1.70–3.78) and heart block (random-effects odds ratio 2.65, 95% confidence interval 1.88–3.72) |
| Chronic kidney disease (CKD) | ||
| Mantovani A et al. Metabolism 2018; 79: 64–76 | 9 observational studies were included for a total of 96,595 individuals with and without T2DM | NAFLD was associated with a higher risk of incident CKD (random-effects hazard ratio 1.37, 95% confidence interval 1.20–1.53). Patients with severe forms of NAFLD were more likely to develop incident CKD (random-effects hazard ratio 1.50, 95% confidence interval 1.25–1.74) |
| Mantovani A et al. Gut 2022; 71: 156–162 | 13 observational studies were included for a total of 1,222,032 individuals with and without T2DM | NAFLD was associated with an increased risk of incident CKD (random-effects hazard ratio 1.43, 95% confidence interval 1.33–1.54) |
| Cardiovascular risk factors |
|
| Physical examination |
|
| Laboratory tests |
|
| Cardiovascular examination tests |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, A.; Dalbeni, A.; Beatrice, G.; Cappelli, D.; Gomez-Peralta, F. Non-Alcoholic Fatty Liver Disease and Risk of Macro- and Microvascular Complications in Patients with Type 2 Diabetes. J. Clin. Med. 2022, 11, 968. https://doi.org/10.3390/jcm11040968
Mantovani A, Dalbeni A, Beatrice G, Cappelli D, Gomez-Peralta F. Non-Alcoholic Fatty Liver Disease and Risk of Macro- and Microvascular Complications in Patients with Type 2 Diabetes. Journal of Clinical Medicine. 2022; 11(4):968. https://doi.org/10.3390/jcm11040968
Chicago/Turabian StyleMantovani, Alessandro, Andrea Dalbeni, Giorgia Beatrice, Davide Cappelli, and Fernando Gomez-Peralta. 2022. "Non-Alcoholic Fatty Liver Disease and Risk of Macro- and Microvascular Complications in Patients with Type 2 Diabetes" Journal of Clinical Medicine 11, no. 4: 968. https://doi.org/10.3390/jcm11040968
APA StyleMantovani, A., Dalbeni, A., Beatrice, G., Cappelli, D., & Gomez-Peralta, F. (2022). Non-Alcoholic Fatty Liver Disease and Risk of Macro- and Microvascular Complications in Patients with Type 2 Diabetes. Journal of Clinical Medicine, 11(4), 968. https://doi.org/10.3390/jcm11040968