
Suicidal Ideation and Suicide-Attempt-Related Hospitalizations among People with Alzheimer’s Disease (AD) and AD-Related Dementias in the United States during 2016–2018

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
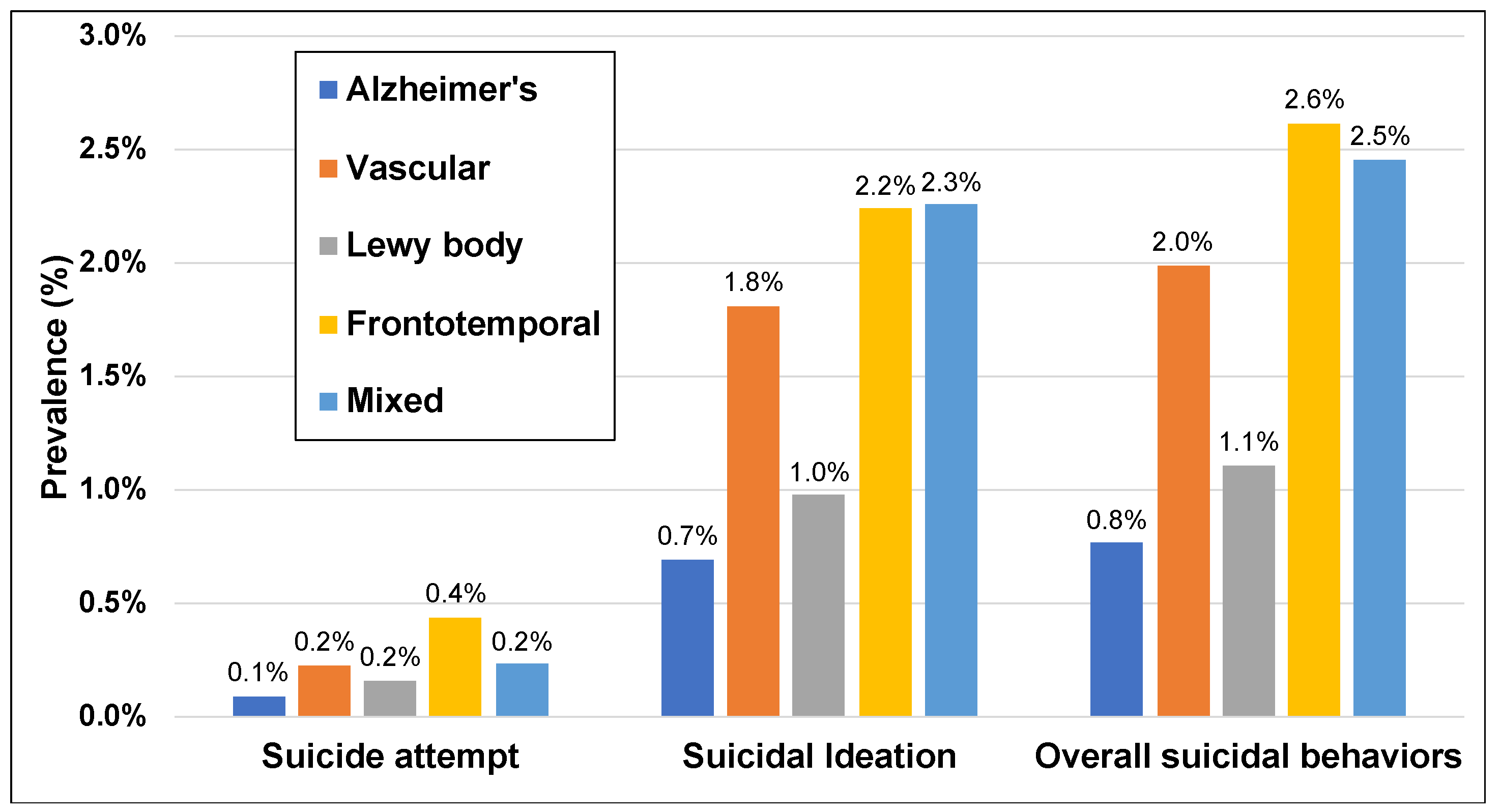
3.1. Frequency of Suicidal-Behavior-Related Hospitalizations in Dementia Subtypes
3.2. Demographic and Clinical Characteristics
3.3. Associations between Patient Factors and Suicidal-Behavior-Related Hospitalizations
3.4. Modes of Harm in Suicide Attempts
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Charles, S.T.; Carstensen, L.L. Social and emotional aging. Annu. Rev. Psychol. 2010, 61, 383–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Orden, K.; Conwell, Y. Suicides in late life. Curr. Psychiatry Rep. 2011, 13, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Hedegaard, H.; Curtin, S.; Warner, M. Centers for Disease Control and Prevention. National Center for Health Statistics. Increase in Suicide Mortality in the United States, 1999–2018. Nchs Data Brief No. 362. Available online: https://www.cdc.gov/nchs/products/databriefs/db362.html (accessed on 15 May 2021).
- Phillips, J.A. A changing epidemiology of suicide? The influence of birth cohorts on suicide rates in the united states. Soc. Sci. Med. 2014, 114, 151–160. [Google Scholar] [CrossRef]
- Balasubramaniam, M. Rational suicide in elderly adults: A clinician’s perspective. J. Am. Geriatr. Soc. 2018, 66, 998–1001. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.A. Major depressive disorder, suicidal behaviour, bipolar disorder, and generalised anxiety disorder among emerging adults with and without chronic health conditions. Epidemiol. Psychiatr. Sci. 2016, 25, 462–474. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Lee, K.S.; Han, E. Suicide risk within 1 year of dementia diagnosis in older adults: A nationwide retrospective cohort study. J. Psychiatry Neurosci. 2021, 46, E119–E127. [Google Scholar] [CrossRef] [PubMed]
- Schmutte, T.; Olfson, M.; Maust, D.T.; Xie, M.; Marcus, S.C. Suicide risk in first year after dementia diagnosis in older adults. Alzheimers Dement. 2021; in press. [Google Scholar] [CrossRef]
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and management of dementia: Review. JAMA 2019, 322, 1589–1599. [Google Scholar] [CrossRef]
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.-T.; Prina, M. World Alzheimer Report 2015—The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015. [Google Scholar]
- Chiu, M.J.; Chen, T.F.; Yip, P.K.; Hua, M.S.; Tang, L.Y. Behavioral and psychologic symptoms in different types of dementia. J. Formos Med. Assoc. 2006, 105, 556–562. [Google Scholar] [CrossRef] [Green Version]
- Lai, A.X.; Kaup, A.R.; Yaffe, K.; Byers, A.L. High occurrence of psychiatric disorders and suicidal behavior across dementia subtypes. Am. J. Geriatr. Psychiatry 2018, 26, 1191–1201. [Google Scholar] [CrossRef]
- Taylor, W.D.; Aizenstein, H.J.; Alexopoulos, G.S. The vascular depression hypothesis: Mechanisms linking vascular disease with depression. Mol. Psychiatry 2013, 18, 963–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKhann, G.M.; Albert, M.S.; Grossman, M.; Miller, B.; Dickson, D.; Trojanowski, J.Q. Clinical and pathological diagnosis of frontotemporal dementia: Report of the work group on frontotemporal dementia and pick’s disease. Arch. Neurol. 2001, 58, 1803–1809. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Sullivan, J.L.; Amodeo, K.; Lunde, A.; Tsuang, D.W.; Reger, M.A.; Conwell, Y.; Ritter, A.; Bang, J.; Onyike, C.U.; et al. Suicide and lewy body dementia: Report of a lewy body dementia association working group. Int. J. Geriatr. Psychiatry 2021, 36, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Migliorelli, R.; Tesón, A.; Sabe, L.; Petracca, G.; Petracchi, M.; Leiguarda, R.; Starkstein, S.E. Anosognosia in alzheimer’s disease: A study of associated factors. J. Neuropsychiatry Clin. Neurosci. 1995, 7, 338–344. [Google Scholar] [PubMed]
- Reed, B.R.; Jagust, W.J.; Coulter, L. Anosognosia in alzheimer’s disease: Relationships to depression, cognitive function, and cerebral perfusion. J. Clin. Exp. Neuropsychol. 1993, 15, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Oliva, E.M.; Bowe, T.; Tavakoli, S.; Martins, S.; Lewis, E.T.; Paik, M.; Wiechers, I.; Henderson, P.; Harvey, M.; Avoundjian, T.; et al. Development and applications of the veterans health administration’s stratification tool for opioid risk mitigation (storm) to improve opioid safety and prevent overdose and suicide. Psychol. Serv. 2017, 14, 34–49. [Google Scholar] [CrossRef] [PubMed]
- Walkup, J.T.; Townsend, L.; Crystal, S.; Olfson, M. A systematic review of validated methods for identifying suicide or suicidal ideation using administrative or claims data. Pharmacoepidemiol. Drug Saf. 2012, 21, 174–182. [Google Scholar] [CrossRef]
- Clinical Classifications Software Refined (CCSR). Healthcare Costs and Utilization Project. Agency for Healthcare Research and Quality. Available online: https://www.hcup-us.ahrq.gov/toolssoftware/ccsr/ccs_refined.jsp (accessed on 1 January 2022).
- Berry, S.D.; Ngo, L.; Samelson, E.J.; Kiel, D.P. Competing risk of death: An important consideration in studies of older adults. J. Am. Geriatr. Soc. 2010, 58, 783–787. [Google Scholar] [CrossRef] [Green Version]
- Tsirigotis, K.; Gruszczynski, W.; Tsirigotis, M. Gender differentiation in methods of suicide attempts. Med. Sci. Monit. 2011, 17, PH65–PH70. [Google Scholar] [CrossRef] [Green Version]
- Haerian, K.; Salmasian, H.; Friedman, C. Methods for identifying suicide or suicidal ideation in ehrs. AMIA Annu. Symp. Proc. 2012, 2012, 1244–1253. [Google Scholar]
- Anderson, H.D.; Pace, W.D.; Brandt, E.; Nielsen, R.D.; Allen, R.R.; Libby, A.M.; West, D.R.; Valuck, R.J. Monitoring suicidal patients in primary care using electronic health records. J. Am. Board Fam. Med. 2015, 28, 65–71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| AD | VaD | LBD | FTD | Mixed | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ADRD population with suicidal behavior | N = 5592 | N = 5035 | N = 578 | N = 370 | N = 963 | |||||
| Age, mean (SD) | 77.0 | 0.3 | 71.7 | 0.4 | 71.9 | 0.9 | 68.3 | 1.0 | 77.4 | 0.6 |
| Female sex, n (%) | 3190 | 57.0% | 2502 | 49.7% | 230 | 39.8% | 173 | 46.8% | 525 | 54.5% |
| Median household income, n (%) | ||||||||||
| Q1 (lowest income) | 1671 | 29.9% | 1594 | 31.7% | 146 | 25.3% | 82 | 22.2% | 284 | 29.5% |
| Q2 | 1493 | 26.7% | 1332 | 26.5% | 146 | 25.3% | 96 | 26.0% | 256 | 26.6% |
| Q3 | 1274 | 22.8% | 1087 | 21.6% | 145 | 25.1% | 102 | 27.6% | 211 | 21.9% |
| Q4 (highest income) | 1076 | 19.2% | 947 | 18.8% | 132 | 22.8% | 82 | 22.2% | 199 | 20.7% |
| Mental health conditions, n (%) | ||||||||||
| Depression | 3836 | 68.6% | 3525 | 70.0% | 387 | 67.0% | 247 | 66.8% | 680 | 70.6% |
| Anxiety | 2238 | 40.0% | 2107 | 41.8% | 235 | 40.7% | 164 | 44.3% | 436 | 45.3% |
| Psychotic disorders | 1526 | 27.3% | 1392 | 27.6% | 196 | 33.9% | 116 | 31.4% | 284 | 29.5% |
| Bipolar disorder | 709 | 12.7% | 772 | 15.3% | 98 | 17.0% | 70 | 18.9% | 126 | 13.1% |
| Personality disorder | 207 | 3.7% | 247 | 4.9% | 25 | 4.3% | 27 | 7.3% | 227 | 23.6% |
| PTSD | 146 | 2.6% | 210 | 4.2% | 17 | 2.9% | 20 | 5.4% | 21 | 2.2% |
| ADHD | 119 | 2.1% | 145 | 2.9% | 16 | 2.8% | 17 | 4.6% | 24 | 2.5% |
| Other comorbidities, n (%) | ||||||||||
| Hypertension | 4219 | 75.4% | 3935 | 78.2% | 418 | 72.3% | 239 | 64.6% | 783 | 81.3% |
| Hyperlipidemia | 2727 | 48.8% | 2571 | 51.1% | 255 | 44.1% | 152 | 41.1% | 539 | 56.0% |
| Diabetes | 1695 | 30.3% | 1779 | 35.3% | 158 | 27.3% | 96 | 25.9% | 286 | 29.7% |
| Chronic kidney disease | 1591 | 28.5% | 1628 | 32.3% | 161 | 27.9% | 76 | 20.5% | 685 | 71.1% |
| Ischemic heart disease | 1468 | 26.3% | 1536 | 30.5% | 137 | 23.7% | 64 | 17.3% | 297 | 30.8% |
| Thyroid disease | 1333 | 23.8% | 1072 | 21.3% | 128 | 22.1% | 87 | 23.5% | 224 | 23.3% |
| Chronic pulmonary disease | 1089 | 19.5% | 1054 | 20.9% | 71 | 12.3% | 55 | 14.9% | 160 | 16.6% |
| Rheumatoid or osteoarthritis | 1070 | 19.1% | 818 | 16.2% | 57 | 9.9% | 42 | 11.4% | 180 | 18.7% |
| Atrial fibrillation | 878 | 15.7% | 882 | 17.5% | 76 | 13.1% | 40 | 10.8% | 187 | 19.4% |
| Congestive heart failure | 721 | 12.9% | 788 | 15.7% | 57 | 9.9% | 32 | 8.6% | 120 | 12.5% |
| Substance-use disorder | 321 | 5.7% | 558 | 11.1% | 38 | 6.6% | 35 | 9.5% | 193 | 20.0% |
| Alcohol-use disorder | 320 | 5.7% | 480 | 9.5% | 27 | 4.7% | 24 | 6.5% | 50 | 5.2% |
| Asthma | 271 | 4.8% | 250 | 5.0% | 32 | 5.5% | 21 | 5.7% | 51 | 5.3% |
| Mobility Disorder | 222 | 4.0% | 462 | 9.2% | 43 | 7.4% | 13 | 3.5% | 37 | 3.8% |
| Liver disorders | 122 | 2.2% | 161 | 3.2% | 21 | 3.6% | ** | ** | 66 | 6.9% |
| Covariate | OR | 95% CI |
|---|---|---|
| Dementia subtype | ||
| Alzheimer’s disease | Reference | Reference |
| Vascular | 1.85 | 1.69–2.01 |
| Lewy body | 0.97 | 0.85–1.10 |
| Frontotemporal | 1.35 | 1.13–1.62 |
| Mixed | 2.27 | 2.02–2.54 |
| Age (per 5 years) | 0.85 | 0.85–0.87 |
| Female sex | 0.77 | 0.73–0.81 |
| Median household income, n (%) | ||
| Q1 (lowest income) | Reference | |
| Q2 | 1.02 | 0.94–1.11 |
| Q3 | 1.02 | 0.94–1.11 |
| Q4 (highest income) | 1.00 | 0.88–1.36 |
| Mental health conditions, n (%) | ||
| Depression | 6.80 | 6.35–7.30 |
| Psychotic disorders | 2.77 | 2.56–3.00 |
| Bipolar disorder | 2.72 | 2.52–2.94 |
| Personality disorder | 2.47 | 2.12–2.90 |
| ADHD | 1.63 | 1.32–2.94 |
| Anxiety | 1.55 | 1.44–1.66 |
| PTSD | 1.43 | 1.23–1.67 |
| Other comorbidities, n (%) | ||
| Substance-use disorders | 2.17 | 1.95–2.41 |
| Alcohol-use disorder | 1.78 | 1.61–1.98 |
| Diabetes | 1.03 | 0.98–1.08 |
| Hypertension | 1.02 | 0.96–1.08 |
| Thyroid disease | 1.06 | 0.99–1.12 |
| Asthma | 1.03 | 0.92–1.15 |
| Hyperlipidemia | 0.97 | 0.92–1.02 |
| Atrial fibrillation | 0.85 | 0.78–0.93 |
| Ischemic heart disease | 1.03 | 0.97–1.09 |
| Rheumatoid or osteoarthritis | 0.96 | 0.89–1.02 |
| Chronic pulmonary disease | 0.95 | 0.89–1.01 |
| Liver disorders | 0.70 | 0.60–0.82 |
| Chronic kidney disease | 0.65 | 0.62–0.69 |
| Congestive heart failure | 0.68 | 0.63–0.74 |
| Mobility Disorder | 0.52 | 0.47–0.58 |
| Method of Harm | N | % |
|---|---|---|
| Medications or drugs | 1166 | 89.2% |
| Weapons (knives, firearms, etc.) | 231 | 17.7% |
| Asphyxiation (hanging, carbon monoxide) | 33 | 2.5% |
| Mechanical harms (falling, vehicles) | 28 | 2.1% |
| Alcohol or other harmful substances | 20 | 1.5% |
| Detailed Method of Harm Descriptions | N | % |
|---|---|---|
| Poisoning by benzodiazepines | 233 | 17.8% |
| Suicide attempt (not specified) | 224 | 17.1% |
| Self-harm by other specified means | 160 | 12.2% |
| Poisoning by 4-aminophenol (acetaminophen) | 102 | 7.8% |
| Poisoning by other opioids | 91 | 7.0% |
| Intentional self-harm by knife | 85 | 6.5% |
| Poisoning by other antiepileptic and sedative-hypnotic drugs | 79 | 6.0% |
| Intentional self-harm by other sharp objects | 60 | 4.6% |
| Intentional self-harm by unspecified sharp objects | 56 | 4.3% |
| Poisoning by unspecified drugs, medicaments, and biological substances | 54 | 4.1% |
| Poisoning by other antipsychotics and neuroleptics | 52 | 4.0% |
| Poisoning by selective serotonin reuptake inhibitors | 48 | 3.7% |
| Poisoning by selective serotonin and norepinephrine reuptake inhibitors | 40 | 3.1% |
| Poisoning by beta-adrenoreceptor antagonists | 39 | 3.0% |
| Poisoning by aspirin | 31 | 2.4% |
| Poisoning by other drugs, medicaments, and biological substances | 27 | 2.1% |
| Poisoning by other antihypertensive drugs | 25 | 1.9% |
| Toxic effect of ethanol | 23 | 1.8% |
| Poisoning by other synthetic narcotics | 22 | 1.7% |
| Poisoning by antiallergic and antiemetic drugs | 22 | 1.7% |
| Poisoning by tricyclic antidepressants | 20 | 1.5% |
| Poisoning by propionic acid derivatives | 19 | 1.5% |
| Poisoning by calcium-channel blockers | 19 | 1.5% |
| Poisoning by angiotensin-converting-enzyme inhibitors | 19 | 1.5% |
| Poisoning by other parasympathomimetics [cholinergics] | 18 | 1.4% |
| Poisoning by other antidepressants | 16 | 1.2% |
| Poisoning by tetracycline antidepressants | 15 | 1.1% |
| Asphyxiation due to hanging | 15 | 1.1% |
| Intentional self-harm by jumping from a high place | 15 | 1.1% |
| Poisoning by antithyroid drugs | 14 | 1.1% |
| Poisoning by unspecified synthetic narcotics | 14 | 1.1% |
| Poisoning by antiparkinsonism drugs | 13 | 1.0% |
| Poisoning by antihyperlipidemic and antiarteriosclerotic drugs | 13 | 1.0% |
| Poisoning by thyroid hormones | 12 | 0.9% |
| Other causes | 273 | 20.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alipour-Haris, G.; Armstrong, M.J.; Sullivan, J.L.; Suryadevara, U.; Rouhizadeh, M.; Brown, J.D. Suicidal Ideation and Suicide-Attempt-Related Hospitalizations among People with Alzheimer’s Disease (AD) and AD-Related Dementias in the United States during 2016–2018. J. Clin. Med. 2022, 11, 943. https://doi.org/10.3390/jcm11040943
Alipour-Haris G, Armstrong MJ, Sullivan JL, Suryadevara U, Rouhizadeh M, Brown JD. Suicidal Ideation and Suicide-Attempt-Related Hospitalizations among People with Alzheimer’s Disease (AD) and AD-Related Dementias in the United States during 2016–2018. Journal of Clinical Medicine. 2022; 11(4):943. https://doi.org/10.3390/jcm11040943
Chicago/Turabian StyleAlipour-Haris, Golnoosh, Melissa J. Armstrong, Jennifer L. Sullivan, Uma Suryadevara, Masoud Rouhizadeh, and Joshua D. Brown. 2022. "Suicidal Ideation and Suicide-Attempt-Related Hospitalizations among People with Alzheimer’s Disease (AD) and AD-Related Dementias in the United States during 2016–2018" Journal of Clinical Medicine 11, no. 4: 943. https://doi.org/10.3390/jcm11040943
APA StyleAlipour-Haris, G., Armstrong, M. J., Sullivan, J. L., Suryadevara, U., Rouhizadeh, M., & Brown, J. D. (2022). Suicidal Ideation and Suicide-Attempt-Related Hospitalizations among People with Alzheimer’s Disease (AD) and AD-Related Dementias in the United States during 2016–2018. Journal of Clinical Medicine, 11(4), 943. https://doi.org/10.3390/jcm11040943