
A Digital Health Application Allowing a Personalized Low-Glycemic Nutrition for the Prophylaxis of Migraine: Proof-of-Concept Data from a Retrospective Cohort Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Digital Nutrition Program
2.2. Data Collection
2.3. Data Analysis and Statistics
2.4. Subgroup Analyses
3. Results
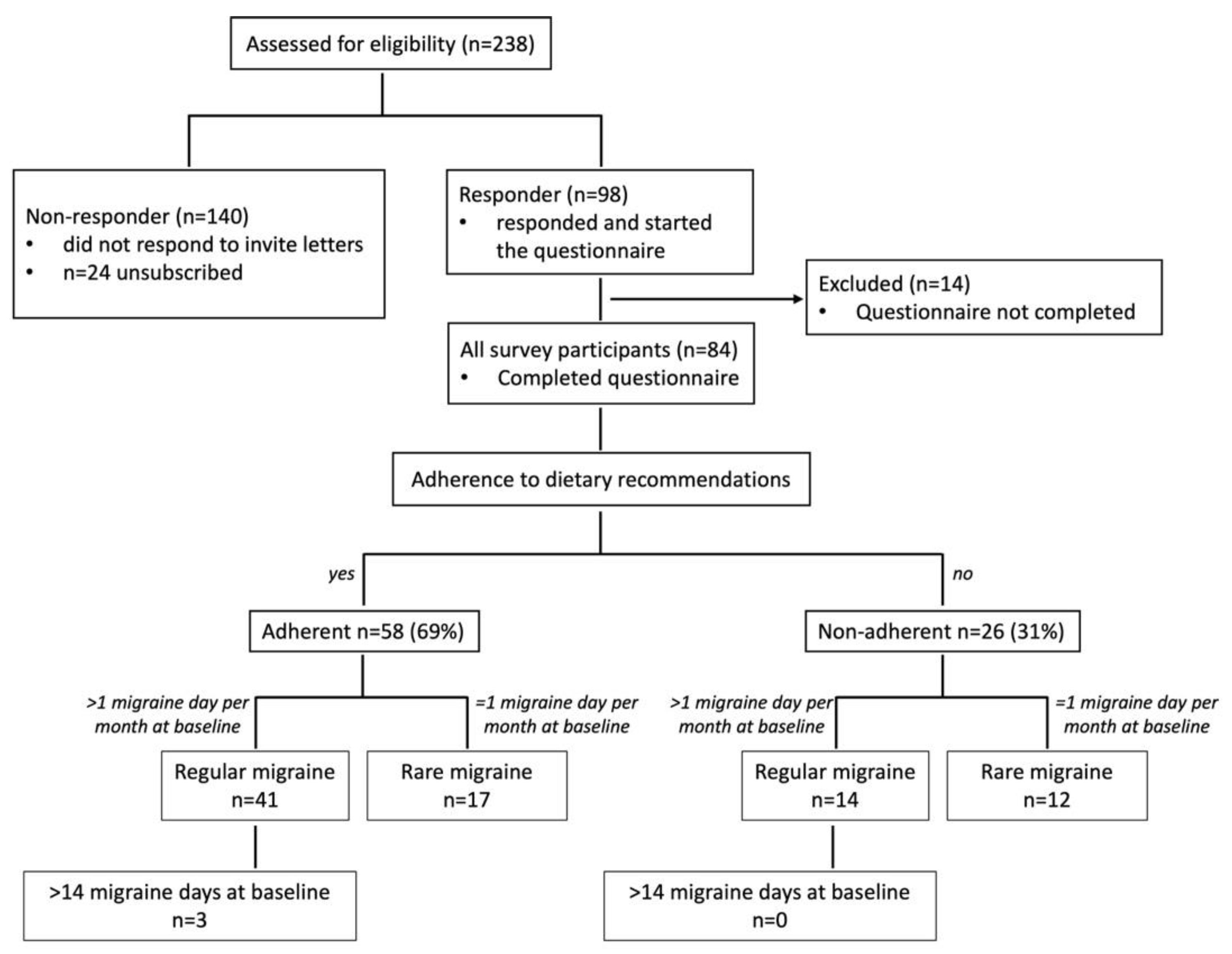
3.1. Cohort Description
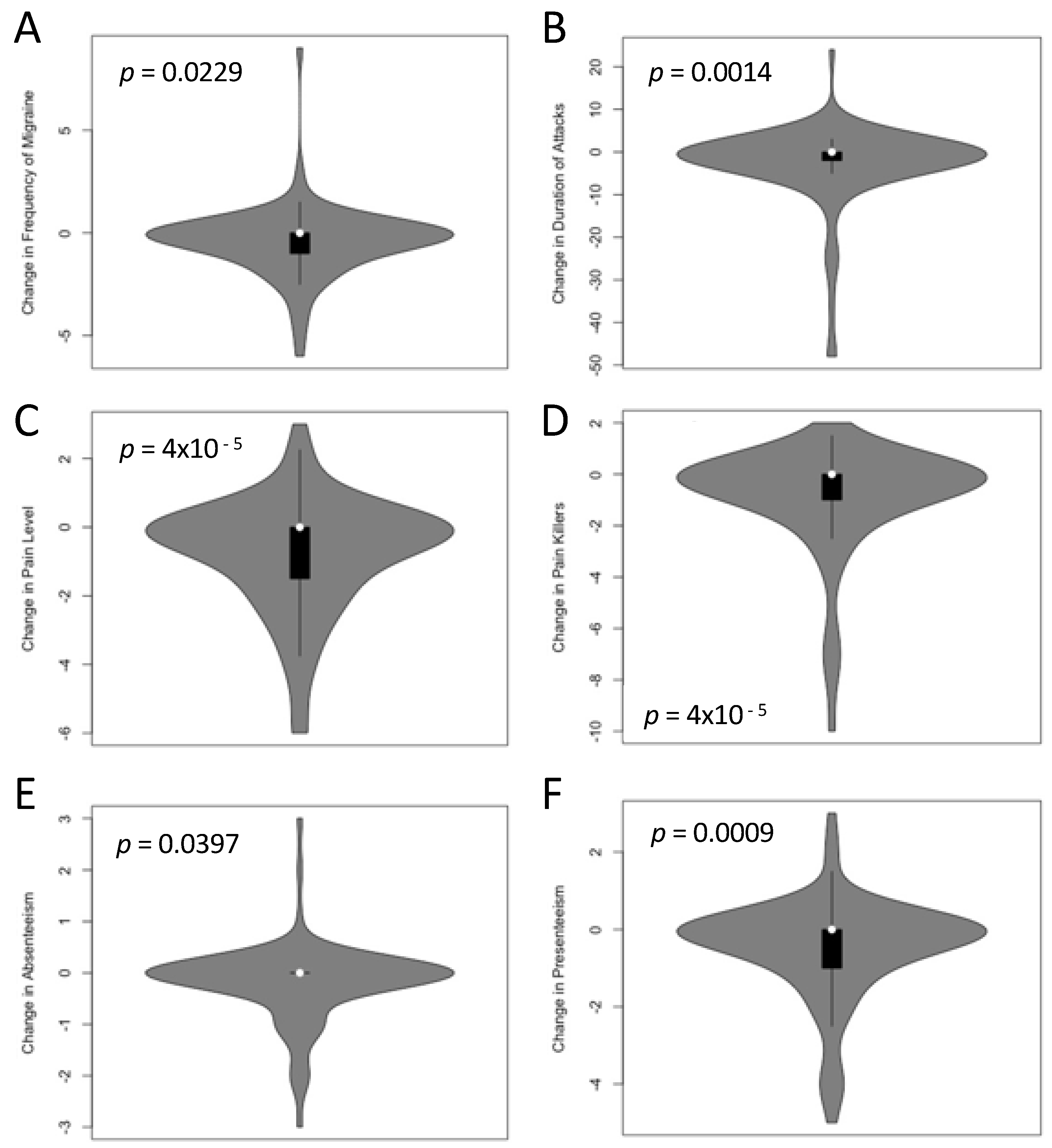
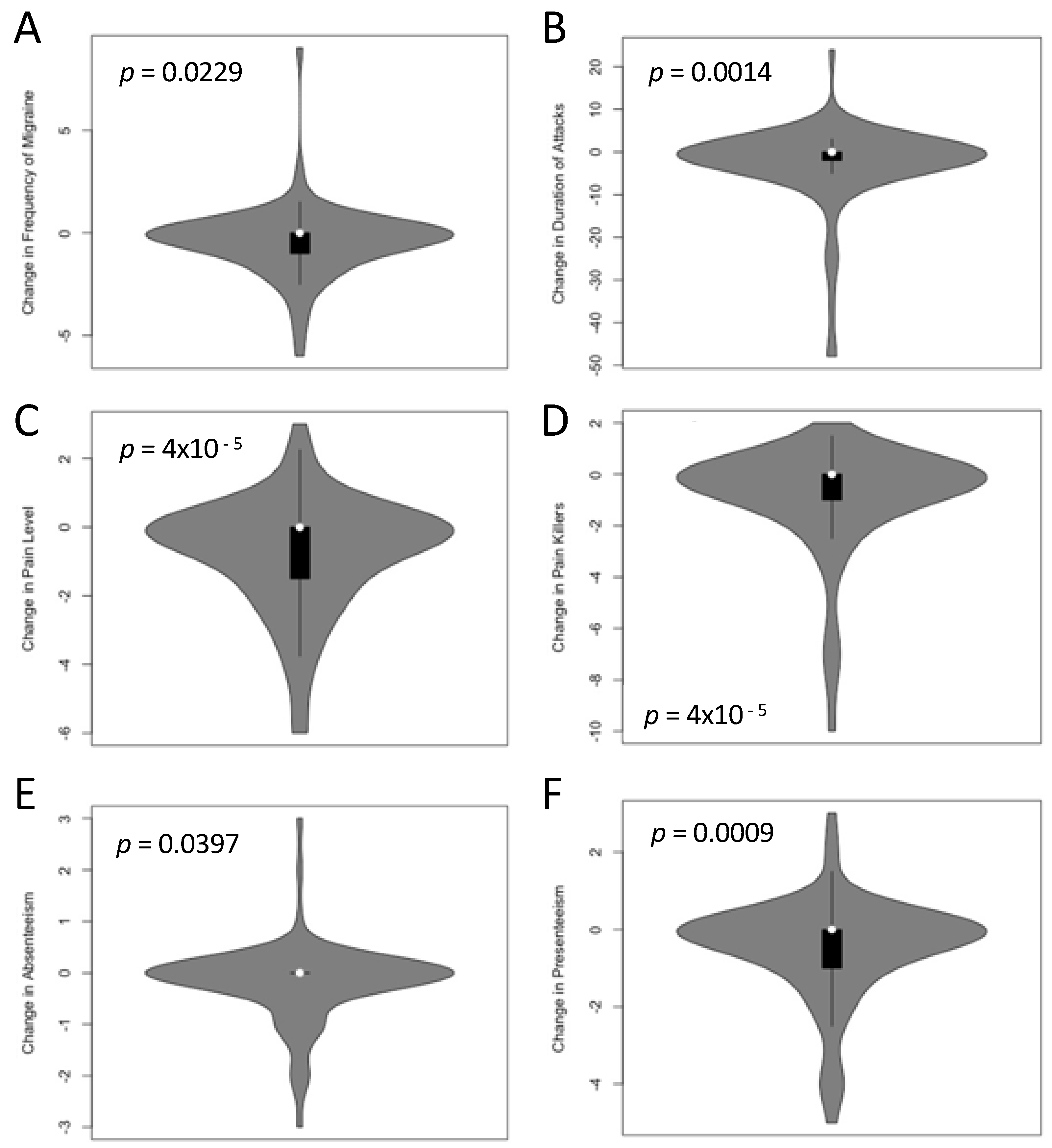
3.2. Migraine Symptoms after Receipt of the PLGN Report
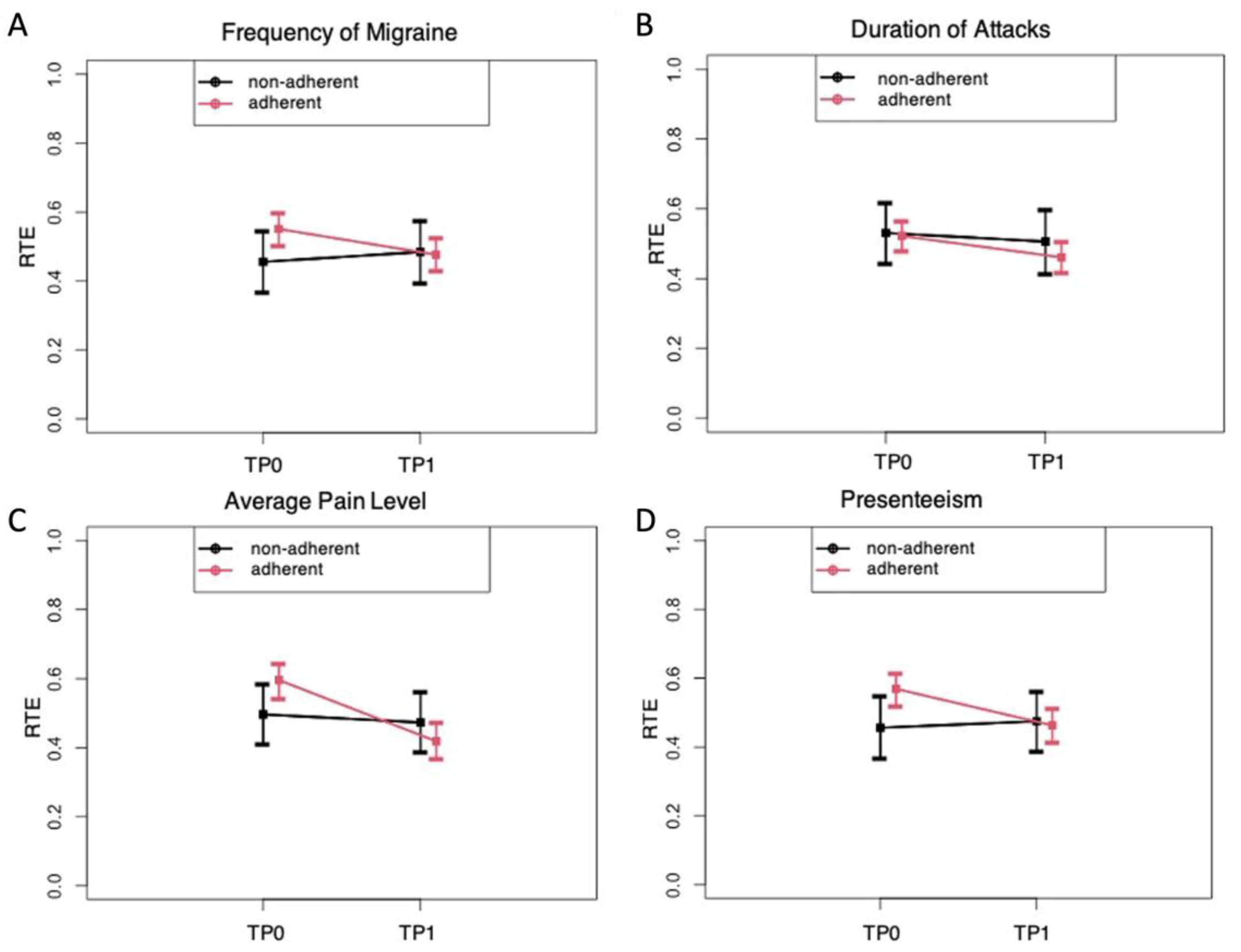
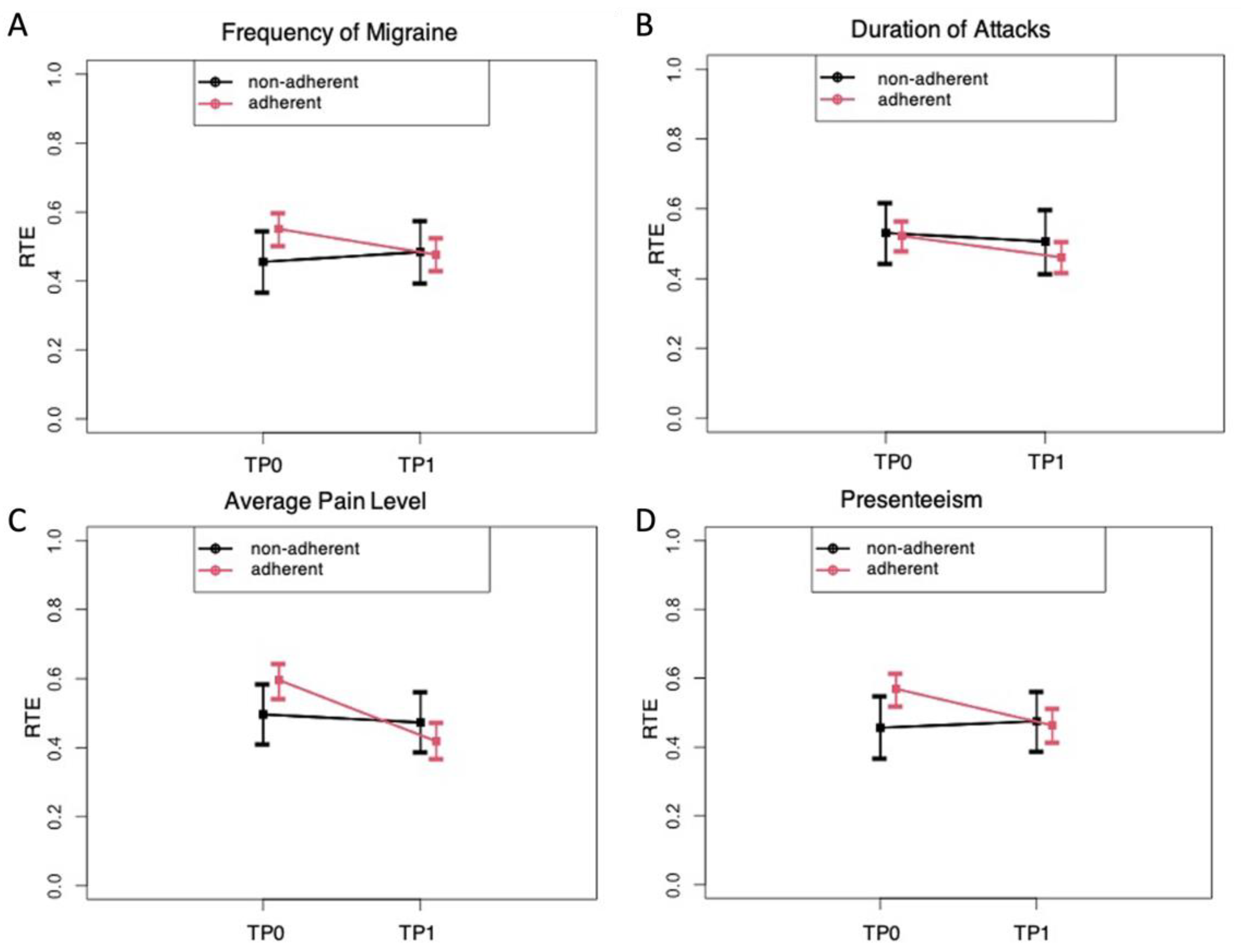
3.3. Impact of Adherence to the PLGN Report
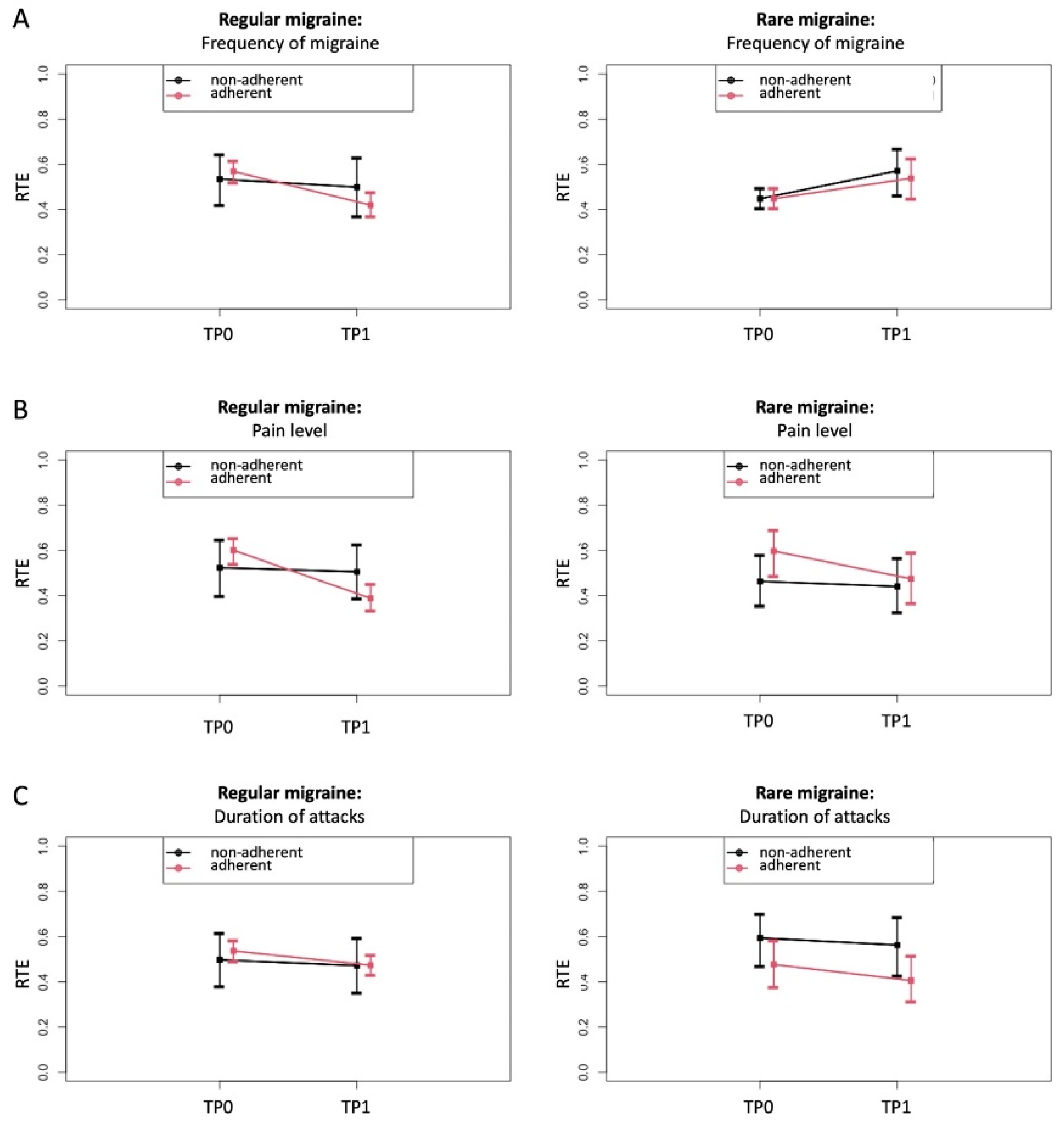
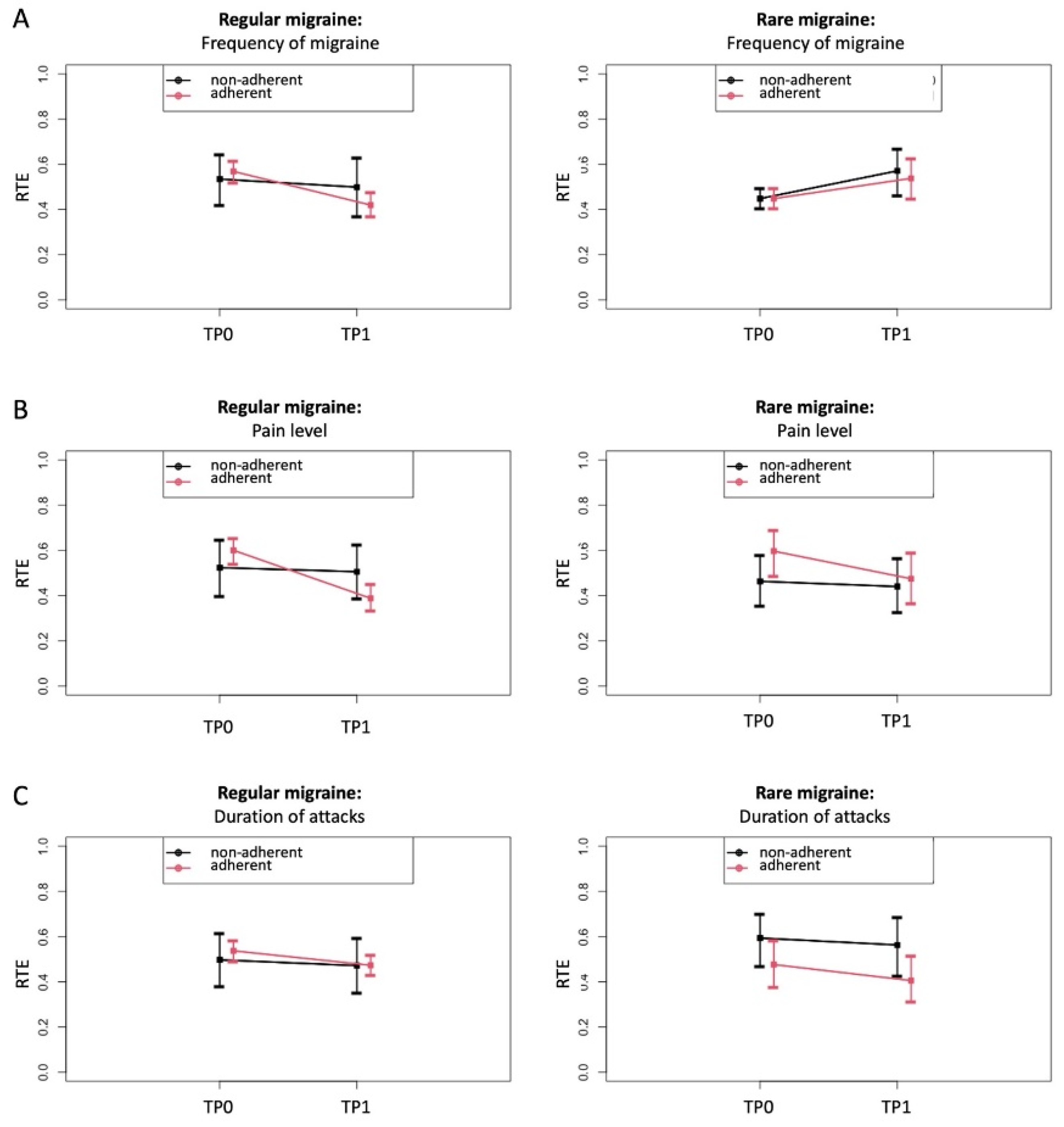
3.4. Impact of Baseline Migraine Frequency on Migraine Symptoms
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steiner, T.J.; Stovner, L.J.; Birbeck, G.L. Migraine: The seventh disabler. J. Headache Pain 2013, 14, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashina, M.; Katsarava, Z.; Do, T.P.; Buse, D.C.; Pozo-Rosich, P.; Özge, A.; Krymchantowski, A.V.; Lebedeva, E.R.; Ravishankar, K.; Yu, S.; et al. Migraine: Epidemiology and systems of care. Lancet 2021, 397, 1485–1495. [Google Scholar] [CrossRef]
- Steiner, T.J.; Saylor, D. The Global Burden of Headache. Skull Base 2018, 38, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Stovner, L.J.; Nichols, E.; Steiner, T.J.; Abd-Allah, F.; Abdelalim, A.; Al-Raddadi, R.M.; Ansha, M.G.; Barac, A.; Bensenor, I.M.; Doan, L.P. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 954–976. [Google Scholar] [CrossRef] [Green Version]
- Bonafede, M.; Sapra, S.; Shah, N.; Tepper, S.; Cappell, K.; Desai, P. Direct and Indirect Healthcare Resource Utilization and Costs Among Migraine Patients in the United States. Headache J. Head Face Pain 2018, 58, 700–714. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Diener, H.-C.; Holle-Lee, D.; Nägel, S.; Dresler, T.; Gaul, C.; Göbel, H.; Heinze-Kuhn, K.; Jürgens, T.; Kropp, P.; Meyer, B.; et al. Treatment of migraine attacks and prevention of migraine: Guidelines by the German Migraine and Headache Society and the German Society of Neurology. Clin. Transl. Neurosci. 2019, 3. [Google Scholar] [CrossRef] [Green Version]
- Steiner, T.J.; Jensen, R.; Katsarava, Z.; Linde, M.; MacGregor, E.A.; Osipova, V.; Paemeleire, K.; Olesen, J.; Peters, M.; Martelletti, P. Aids to management of headache disorders in primary care (2nd edition): On behalf of the European Headache Federation and Lifting The Burden: The Global Campaign against Headache. J. Headache Pain 2019, 20, 57. [Google Scholar] [CrossRef]
- Society, A.H. The American headache society position statement on integrating new migraine treatments into clinical practice. Headache J. Head Face Pain 2018, 59, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Ashina, M.; Buse, D.C.; Ashina, H.; Pozo-Rosich, P.; Peres, M.F.P.; Lee, M.J.; Terwindt, G.M.; Singh, R.H.; Tassorelli, C.; Do, T.P.; et al. Migraine: Integrated approaches to clinical management and emerging treatments. Lancet 2021, 397, 1505–1518. [Google Scholar] [CrossRef]
- Hepp, Z.; Dodick, D.W.; Varon, S.F.; Chia, J.; Matthew, N.; Gillard, P.; Hansen, R.N.; Devine, E.B. Persistence and switching patterns of oral migraine prophylactic medications among patients with chronic migraine: A retrospective claims analysis. Cephalalgia 2016, 37, 470–485. [Google Scholar] [CrossRef]
- Woolley, J.M.; Bonafede, M.M.; Maiese, B.A.; Lenz, R.A. Migraine Prophylaxis and Acute Treatment Patterns Among Commercially Insured Patients in the United States. Headache J. Head Face Pain 2017, 57, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.-C.; Förderreuther, S.; Gaul, C.; Giese, F.; Hamann, T.; Holle-Lee, D.; Jürgens, T.P.; Kamm, K.; Kraya, T.; Lampl, C.; et al. Prevention of migraine with monoclonal antibodies against CGRP or the CGRP receptor. Neurol. Res. Pract. 2020, 2, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacco, S.; Bendtsen, L.; Ashina, M.; Reuter, U.; Terwindt, G.; Mitsikostas, D.D.; Martelletti, P. European headache federation guideline on the use of monoclonal antibodies acting on the calcitonin gene related peptide or its receptor for migraine prevention. J. Headache Pain 2019, 20, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiseo, C.; Ornello, R.; Pistoia, F.; Sacco, S. How to integrate monoclonal antibodies targeting the calcitonin gene-related peptide or its receptor in daily clinical practice. J. Headache Pain 2019, 20, 49. [Google Scholar] [CrossRef] [Green Version]
- Puledda, F.; Shields, K. Non-Pharmacological Approaches for Migraine. Neurotherapeutics 2018, 15, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Kelman, L. The Triggers or Precipitants of the Acute Migraine Attack. Cephalalgia 2007, 27, 394–402. [Google Scholar] [CrossRef]
- Fukui, P.T.; Gonçalves, T.R.T.; Strabelli, C.G.; Lucchino, N.M.F.; Matos, F.C.; Dos Santos, J.P.M.; Zukerman, E.; Zukerman-Guendler, V.; Mercante, J.P.; Masruha, M.R.; et al. Trigger factors in migraine patients. Arq. Neuro-Psiquiatr. 2008, 66, 494–499. [Google Scholar] [CrossRef] [Green Version]
- Peatfield, R.C.; Glover, V.; Littlewood, J.T.; Sandler, M.; Rose, F.C. The Prevalence of Diet-Induced Migraine. Cephalalgia 1984, 4, 179–183. [Google Scholar] [CrossRef]
- Marcus, D.A.; Scharff, L.; Turk, D.C.; Gourley, L.M. A Double-Blind Provocative Study Chocolate as a Trigger of Headache. Cephalalgia 1997, 17, 855–862. [Google Scholar] [CrossRef]
- Di Vincenzo, A.; Beghetto, M.; Vettor, R.; Tana, C.; Rossato, M.; Bond, D.S.; Pagano, C. Effects of Surgical and Non-surgical Weight Loss on Migraine Headache: A Systematic Review and Meta-Analysis. Obes. Surg. 2020, 30, 2173–2185. [Google Scholar] [CrossRef] [PubMed]
- Gray, P.A.; Burtness, H.I. Hypoglycemic Headache. Endocrinology 1935, 19, 549–560. [Google Scholar] [CrossRef]
- Gross, E.C.; Lisicki, M.; Fischer, D.; Sándor, P.S.; Schoenen, J. The metabolic face of migraine—From pathophysiology to treatment. Nat. Rev. Neurol. 2019, 15, 627–643. [Google Scholar] [CrossRef] [PubMed]
- Bongiovanni, D.; Benedetto, C.; Corvisieri, S.; Del Favero, C.; Orlandi, F.; Allais, G.; Sinigaglia, S.; Fadda, M. Effectiveness of ketogenic diet in treatment of patients with refractory chronic migraine. Neurol. Sci. 2021, 42, 3865–3870. [Google Scholar] [CrossRef]
- Evcili, G. Early and Long Period Follow-up Results of Low-Glycemic Index Diet for Migraine Prophylaxis. AGRI 2018, 30, 8–11. [Google Scholar] [CrossRef]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [Green Version]
- Berry, S.E.; Valdes, A.M.; Drew, D.A.; Asnicar, F.; Mazidi, M.; Wolf, J.; Capdevila, J.; Hadjigeorgiou, G.; Davies, R.; Al Khatib, H.; et al. Human postprandial responses to food and potential for precision nutrition. Nat. Med. 2020, 26, 964–973. [Google Scholar] [CrossRef]
- Bunner, A.E.; Agarwal, U.; Gonzales, J.F.; Valente, F.; Barnard, N.D. Nutrition intervention for migraine: A randomized crossover trial. J. Headache Pain 2014, 15, 69. [Google Scholar] [CrossRef] [Green Version]
- Razeghi Jahromi, S.; Ghorbani, Z.; Martelletti, P.; Lampl, C.; Togha, M. Association of Diet and Headache. J. Headache Pain 2019, 20, 106. [Google Scholar] [CrossRef] [Green Version]
- Tassorelli, C.; Diener, H.-C.; Dodick, D.W.; Silberstein, S.D.; Lipton, R.B.; Ashina, M.; Becker, W.J.; Ferrari, M.D.; Goadsby, P.J.; Pozo-Rosich, P.; et al. Guidelines of the International Headache Society for controlled trials of preventive treatment of chronic migraine in adults. Cephalalgia 2018, 38, 815–832. [Google Scholar] [CrossRef]
- Stewart, W.F.; Lipton, R.B.; Whyte, J.; Dowson, A.; Kolodner, K.; Liberman, J.N.; Sawyer, J. An international study to assess reliability of the Migraine Disability Assessment (MIDAS) score. Neurology 1999, 53, 988. [Google Scholar] [CrossRef]
- Stewart, W.F.; Lipton, R.B.; Kolodner, K.B.; Sawyer, J.; Lee, C.; Liberman, J.N. Validity of the Migraine Disability Assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain 2000, 88, 41–52. [Google Scholar] [CrossRef]
- Caremark Inc Migraine Disability Assessment (MIDAS) Questionnaire. Available online: https://eprovide.mapi-trust.org/instruments/migraine-disability-assessment (accessed on 1 June 2021).
- Coeytaux, R.R.; Kaufman, J.; Chao, R.; Mann, J.D.; DeVellis, R.F. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J. Clin. Epidemiol. 2006, 59, 374–380. [Google Scholar] [CrossRef]
- QualityMetric Inc. HIT-6TM—Headache Impact TestTM. Available online: https://eprovide.mapi-trust.org/instruments/headache-impact-test (accessed on 1 June 2021).
- Brunner, E.; Domhof, S.; Langer, F. Nonparametric Analysis of Longitudinal Data in Factorial Experiments; John Wiley & Sons: New York, NY, USA, 2002; ISBN 047144166X. [Google Scholar]
- Porst, M.; Wengler, A.; Leddin, J.; Neuhauser, H.; Katsarava, Z.; Von Der Lippe, E.; Anton, A.; Ziese, T.; Rommel, A. Migraine and Tension-Type Headache in Germany. Prevalence and Disease Severity from the BURDEN 2020 Burden of Disease Study. J. Health Monit. 2020, 5, 1–24. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Evers, S. International Classification of Headache Disorders—ICHD-4 alpha. Cephalalgia 2020, 40, 887–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luedtke, K.; Basener, A.; Bedei, S.; Castien, R.; Chaibi, A.; Falla, D.; Fernández-De-Las-Peñas, C.; Gustafsson, M.; Hall, T.; Jull, G.; et al. Outcome measures for assessing the effectiveness of non-pharmacological interventions in frequent episodic or chronic migraine: A Delphi study. BMJ Open 2020, 10, e029855. [Google Scholar] [CrossRef] [Green Version]
- Goadsby, P.J.; Reuter, U.; Hallström, Y.; Broessner, G.; Bonner, J.H.; Zhang, F.; Sapra, S.; Picard, H.; Mikol, D.D.; Lenz, R.A. A Controlled Trial of Erenumab for Episodic Migraine. N. Engl. J. Med. 2017, 377, 2123–2132. [Google Scholar] [CrossRef]
- Han, L.; Liu, Y.; Xiong, H.; Hong, P. CGRP monoclonal antibody for preventive treatment of chronic migraine: An update of meta-analysis. Brain Behav. 2019, 9, e01215. [Google Scholar] [CrossRef] [PubMed]
- Mulleners, W.M.; Kim, B.-K.; Láinez, M.J.A.; Lanteri-Minet, M.; Pozo-Rosich, P.; Wang, S.; Tockhorn-Heidenreich, A.; Aurora, S.K.; Nichols, R.M.; Yunes-Medina, L.; et al. Safety and efficacy of galcanezumab in patients for whom previous migraine preventive medication from two to four categories had failed (CONQUER): A multicentre, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. 2020, 19, 814–825. [Google Scholar] [CrossRef]
- Reuter, U.; Goadsby, P.; Lanteri-Minet, M.; Wen, S.; Hours-Zesiger, P.; Ferrari, M.D.; Klatt, J. Efficacy and tolerability of erenumab in patients with episodic migraine in whom two-to-four previous preventive treatments were unsuccessful: A randomised, double-blind, placebo-controlled, phase 3b study. Lancet 2018, 392, 2280–2287. [Google Scholar] [CrossRef] [Green Version]
- Flint, A.; Gregersen, N.T.; Gluud, L.L.; Møller, B.K.; Raben, A.; Tetens, I.; Verdich, C.; Astrup, A. Associations between postprandial insulin and blood glucose responses, appetite sensations and energy intake in normal weight and overweight individuals: A meta-analysis of test meal studies. Br. J. Nutr. 2007, 98, 17–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, A.; Chiba, T.; Morishita, T.; Nakamura, A.; Inui, T.; Yamatani, T.; Kadowaki, S.; Chihara, K.; Fukase, M.; Fujita, T. Calcitonin Gene--Related Peptide and Induction of Hyperglycemia in Conscious Rats In Vivo. Diabetes 1990, 39, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Durham, P.L. Calcitonin Gene-Related Peptide (CGRP) and Migraine. Headache J. Head Face Pain 2006, 46, S3–S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siva, Z.O.; Uludüz, D.; Keskin, F.E.; Erenler, F.; Balci, H.; Uygunoğlu, U.; Saip, S.; Göksan, B.; Siva, A.; Balcı, H. Determinants of glucose metabolism and the role of NPY in the progression of insulin resistance in chronic migraine. Cephalalgia 2017, 38, 1773–1781. [Google Scholar] [CrossRef] [PubMed]
- Fava, A.; Pirritano, D.; Consoli, D.; Plastino, M.; Casalinuovo, F.; Cristofaro, S.; Colica, C.; Ermio, C.; De Bartolo, M.; Opipari, C.; et al. Chronic migraine in women is associated with insulin resistance: A cross-sectional study. Eur. J. Neurol. 2013, 21, 267–272. [Google Scholar] [CrossRef]
- Rivera-Mancilla, E.; Al-Hassany, L.; Villalón, C.M.; MaassenVanDenBrink, A. Metabolic Aspects of Migraine: Association with Obesity and Diabetes Mellitus. Front. Neurol. 2021, 12, 686398. [Google Scholar] [CrossRef]
- Fagherazzi, G.; El Fatouhi, D.; Fournier, A.; Gusto, G.; Mancini, F.R.; Balkau, B.; Boutron-Ruault, M.-C.; Kurth, T.; Bonnet, F. Associations Between Migraine and Type 2 Diabetes in Women: Findings from the E3N Cohort Study. JAMA Neurol. 2019, 76, 257. [Google Scholar] [CrossRef]
- Alp, R.; Selek, Ş.; Ilhan Alp, S.; Taşkin, A.; Koçyiǧit, A. Oxidative and Antioxidative Balance in Patients of Migraine. Eur. Rev. Med. Pharmacol. Sci. 2010, 14, 877–882. [Google Scholar]
- Ceriello, A.; Bortolotti, N.; Motz, E.; Pieri, C.; Marra, M.; Tonutti, L.; Lizzio, S.; Feletto, F.; Catone, B.; Taboga, C. Meal-induced oxidative stress and low-density lipoprotein oxidation in diabetes: The possible role of hyperglycemia. Metab. Clin. Exp. 1999, 48, 1503–1508. [Google Scholar] [CrossRef]
- Ceriello, A.; Quagliaro, L.; Catone, B.; Pascon, R.; Piazzola, M.; Bais, B.; Marra, G.; Tonutti, L.; Taboga, C.; Motz, E. Role of Hyperglycemia in Nitrotyrosine Postprandial Generation. Diabetes Care 2002, 25, 1439–1443. [Google Scholar] [CrossRef] [Green Version]
- Coutinho, M.; Gerstein, H.C.; Wang, Y.; Yusuf, S. The relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care 1999, 22, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Levitan, E.; Song, Y.; Ford, E.S.; Liu, S. Is Nondiabetic Hyperglycemia a Risk Factor for Cardiovascular Disease?: A meta-analysis of prospective studies. Arch. Intern. Med. 2004, 164, 2147–2155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vega-López, S.; Venn, B.J.; Slavin, J.L. Relevance of the Glycemic Index and Glycemic Load for Body Weight, Diabetes, and Cardiovascular Disease. Nutrients 2018, 10, 1361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwingshackl, L.; Hoffmann, G. Long-term effects of low glycemic index/load vs. high glycemic index/load diets on parameters of obesity and obesity-associated risks: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Kristo, A.S.; Matthan, N.R.; Lichtenstein, A.H. Effect of Diets Differing in Glycemic Index and Glycemic Load on Cardiovascular Risk Factors: Review of Randomized Controlled-Feeding Trials. Nutrients 2013, 5, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.E.; Faurot, K.R.; Palssson, O.S.; MacIntosh, B.A.; Suchindran, C.; Honvoh, G.; Gaylord, S.; Ramsden, C.E.; Mann, J.D. Comparing prospective headache diary and retrospective four-week headache questionnaire over 20 weeks: Secondary data analysis from a randomized controlled trial. Cephalalgia 2020, 40, 1523–1531. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Description of All Survey Participants | |||
|---|---|---|---|
| Number | Percentage | ||
| Sample size | 84 | 100% | |
| Female participants | 76 | 90.5% | |
| Participants with frequent medical care with GP/neurologist | 48 | 57.1% | |
| Participants with concomitant tension-type headache | 47 | 56,0% | |
| Participants with prophylactic medication (beta blocker, amitriptylin, flunarizin, topiramat, valproate) | 7 | 8.3% | |
| Participants with CGRP antibody treatment | 1 | 1.2% | |
| Participants with Magnesium intake | 13 | 15.5% | |
| Participants with painkiller intake (NSAR, metamizol, paracetamol) | 70 | 83.3% | |
| Participants with intake of triptanes | 25 | 29.8% | |
| mean ± SD | median (IQR) | min; max | |
| Age [years] | 42.6 ± 10.7 | 45.0 (15.5) | 18; 62 |
| Body Mass Index [kg/m2] | 27.4 ± 6.4 | 26.3 (6.9) | 18.0; 50.6 |
| Time of diagnosed migraine disease [years] | 19.7 ± 11.3 | 19.0 (20.0) | 1; 42 |
| Time between program participation and survey [weeks] | 52.4 ± 28.7 | 58.7 (43.4) | 5.7; 118.0 |
| Frequency of migraine [days per month] | 3.5 ± 4.3 | 2.0 (2.5) | 1; 28 |
| Average pain level [1–10] | 7.2 ± 1.5 | 7.0 (2.0) | 3; 10 |
| Duration of migraine attacks [hours] | 21.6 ± 23.0 | 11.0 (23.5) | 1; 96 |
| painkiller intake [days per month] | 3.4 ± 4.0 | 2.0 (3.0) | 0; 20 |
| Absenteeism [days per month] | 1.0 ± 1.6 | 0.0 (1.0) | 0; 10 |
| Presenteeism [days per month] | 3.1 ± 3.9 | 2.0 (3.0) | 0; 28 |
| Sample Size n = 84 | Mean ± SD | Median (IQR) | Min; Max |
|---|---|---|---|
| Frequency of migraine [days per month] | 3.0 ± 4.0 | 2.0 (2.0) | 0; 28 |
| change from TP0 to TP1 | −0.4 ± 1.7 | 0.0 (1.0) | −6; 9 |
| Pain level [1–10] | 6.4 ± 1.8 | 7.0 (3.0) | 1; 10 |
| change from TP0 to TP1 | −0.8 ± 1.6 | 0.0 (1.5) | -6; 3 |
| Duration of migraine attacks [hours] | 18.7 ± 20.1 | 8.0 (20.0) | 1; 72 |
| change from TP0 to TP1 | −3.1 ± 9.9 | 0.0 (2.0) | −48; 24 |
| Painkiller intake [days per month] | 2.5 ± 3.1 | 1.0 (1.0) | 0; 15 |
| change from TP0 to TP1 | −0.9 ± 2.1 | 0.0 (1.0) | −10; 2 |
| Absenteeism [days per month] | 0.8 ± 1.5 | 0.0 (1.0) | 0; 10 |
| change from TP0 to TP1 | −0.2 ± 0.8 | 0.0 (0.0) | −3; 3 |
| Presenteeism [days per month] | 2.6 ± 3.8 | 1.0 (2.0) | 0; 28 |
| change from TP0 to TP1 | −0.5 ± 1.3 | 0.0 (1.0) | −5; 3 |
| Sample Size n = 58 | Mean ± SD | Median (IQR) | Min; Max |
|---|---|---|---|
| Frequency of migraine [days per month] | 3.0 ± 4.3 | 2.0 (2.0) | 0; 28 |
| change from TP0 to TP1 | −0.8 ± 1.5 | 0.0 (2.0) | −6; 3 |
| Pain level [1–10] | 6.3 ± 1.8 | 6.0 (3.0) | 1; 10 |
| change from TP0 to TP1 | −1.0 ± 1.8 | 0.0 (2.0) | −6; 2 |
| Duration of migraine attacks [hours] | 18.4 ± 20.9 | 8.0 (20.0) | 1; 72 |
| change from TP0 to TP1 | −4.2 ± 10.7 | 0.0 (2.0) | −48; 4 |
| Painkiller intake [days per month] | 2.6 ± 3.2 | 1.0 (1.3) | 0; 15 |
| change from TP0 to TP1 | −1.0 ± 2.1 | 0.0 (1.0) | −8; 2 |
| Absenteeism [days per month] | 0.7 ± 1.1 | 0.0 (1.0) | 0; 5 |
| change from TP0 to TP1 | −0.3 ± 0.8 | 0.0 (0.0) | −3; 2 |
| Presenteeism [days per month] | 2.7 ± 4.3 | 1.0 (2.0) | 0; 28 |
| change from TP0 to TP1 | −0.8 ± 1.4 | 0.0 (0.0) | −5; 3 |
| Sample Size n = 26 | Mean ± SD | Median (IQR) | Min; Max |
|---|---|---|---|
| Frequency of migraine [days per month] | 3.0 ± 3.1 | 2.0 (2.0) | 1; 10 |
| change from TP0 to TP1 | 0.3 ± 1.8 | 0.0 (0.0) | −1; 9 |
| Pain level [1–10] | 6.7 ± 1.6 | 7.0 (1.8) | 3; 10 |
| change from TP0 to TP1 | −0.1 ± 1.1 | 0.0 (0.0) | −2; 3 |
| Duration of migraine attacks [hours] | 19.4 ± 18.6 | 11.0 (23.0) | 2; 72 |
| change from TP0 to TP1 | −0.8 ± 7.5 | 0.0 (0.0) | −26; 24 |
| Painkiller intake [days per month] | 2.3 ± 3.1 | 1.0 (1.0) | 0; 10 |
| change from TP0 to TP1 | −0.6 ± 2.1 | 0.0 (0.0) | −10; 0 |
| Absenteeism [days per month] | 1.0 ± 2.1 | 0.0 (1.0) | 0; 10 |
| change from TP0 to TP1 | 0.1 ± 0.6 | 0.0 (0.0) | −1; 3 |
| Presenteeism [days per month] | 2.5 ± 2.8 | 1.5 (2.0) | 0; 10 |
| change from TP0 to TP1 | 0.1 ± 0.5 | 0.0 (0.0) | −1; 2 |
| Sample Size n = 40 | Mean ± SD | Median (IQR) | Min; Max |
|---|---|---|---|
| Frequency of migraine [days per month] | 3.8 ± 5.0 | 2.0 (3.0) | 1; 28 |
| change from TP0 to TP1 | −1.3 ± 1.5 | −1.0 (2.0) | −6; 0 |
| Pain level [1–10] | 6.3 ± 1.6 | 6.0 (2.0) | 3; 10 |
| change from TP0 to TP1 | −1.1 ± 1.6 | −0.5 (2.0) | −6; 1 |
| Duration of migraine attacks [hours] | 24.1 ± 22.7 | 20.0 (43.3) | 1; 72 |
| change from TP0 to TP1 | −5.7 ± 12.5 | 0.0 (4.0) | −48; 0 |
| painkiller intake [days per month] | 3.2 ± 3.6 | 2.0 (3.0) | 0; 15 |
| change from TP0 to TP1 | −1.4 ± 2.2 | 0.0 (2.0) | −8; 0 |
| Absenteeism [days per month] | 0.8 ± 1.3 | 0.0 (1.0) | 0; 5 |
| change from TP0 to TP1 | −0.5 ± 0.8 | 0.0 (1.0) | −3; 0 |
| Presenteeism [days per month] | 3.3 ± 4.9 | 2.0 (2.3) | 0; 28 |
| change from TP0 to TP1 | −1.0 ± 1.4 | 0.0 (2.0) | −5; 0 |
| Sample Size n = 14 | Mean ± SD | Median (IQR) | Min; Max |
|---|---|---|---|
| Frequency of migraine [days per month] | 4.0 ± 3.4 | 2.5 (2.0) | 1; 10 |
| change from TP0 to TP1 | −0.1 ± 0.4 | 0.0 (0.0) | −1; 0 |
| Pain level [1–10] | 7.0 ± 1.4 | 7.0 (1.8) | 5; 10 |
| change from TP0 to TP1 | −0.1 ± 1.2 | 0.0 (0.0) | −2; 3 |
| Duration of migraine attacks [hours] | 20.3 ± 15.4 | 24.0 (20.5) | 2; 48 |
| change from TP0 to TP1 | −1.2 ± 3.5 | 0.0 (0.0) | −12; 2 |
| painkiller intake [days per month] | 3.6 ± 3.6 | 2.0 (2.5) | 0; 10 |
| change from TP0 to TP1 | −0.3 ± 0.8 | 0.0 (0.0) | −2; 0 |
| Absenteeism [days per month] | 1.2 ± 2.6 | 0.5 (1.0) | 0; 10 |
| change from TP0 to TP1 | 0.0 ± 0.0 | 0.0 (0.0) | 0; 0 |
| Presenteeism [days per month] | 3.0 ± 3.2 | 2.0 (2.0) | 0; 10 |
| change from TP0 to TP1 | 0.0 ± 0.0 | 0.0 (0.0) | 0; 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schröder, T.; Kühn, G.; Kordowski, A.; Jahromi, S.R.; Gendolla, A.; Evers, S.; Gaul, C.; Thaçi, D.; König, I.R.; Sina, C. A Digital Health Application Allowing a Personalized Low-Glycemic Nutrition for the Prophylaxis of Migraine: Proof-of-Concept Data from a Retrospective Cohort Study. J. Clin. Med. 2022, 11, 1117. https://doi.org/10.3390/jcm11041117
Schröder T, Kühn G, Kordowski A, Jahromi SR, Gendolla A, Evers S, Gaul C, Thaçi D, König IR, Sina C. A Digital Health Application Allowing a Personalized Low-Glycemic Nutrition for the Prophylaxis of Migraine: Proof-of-Concept Data from a Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(4):1117. https://doi.org/10.3390/jcm11041117
Chicago/Turabian StyleSchröder, Torsten, Gianna Kühn, Anna Kordowski, Soodeh Razeghi Jahromi, Astrid Gendolla, Stefan Evers, Charly Gaul, Diamant Thaçi, Inke Regina König, and Christian Sina. 2022. "A Digital Health Application Allowing a Personalized Low-Glycemic Nutrition for the Prophylaxis of Migraine: Proof-of-Concept Data from a Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 4: 1117. https://doi.org/10.3390/jcm11041117
APA StyleSchröder, T., Kühn, G., Kordowski, A., Jahromi, S. R., Gendolla, A., Evers, S., Gaul, C., Thaçi, D., König, I. R., & Sina, C. (2022). A Digital Health Application Allowing a Personalized Low-Glycemic Nutrition for the Prophylaxis of Migraine: Proof-of-Concept Data from a Retrospective Cohort Study. Journal of Clinical Medicine, 11(4), 1117. https://doi.org/10.3390/jcm11041117