
“Heart in DRESS”: Cardiac Manifestations, Treatment and Outcome of Patients with Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome: A Systematic Review

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
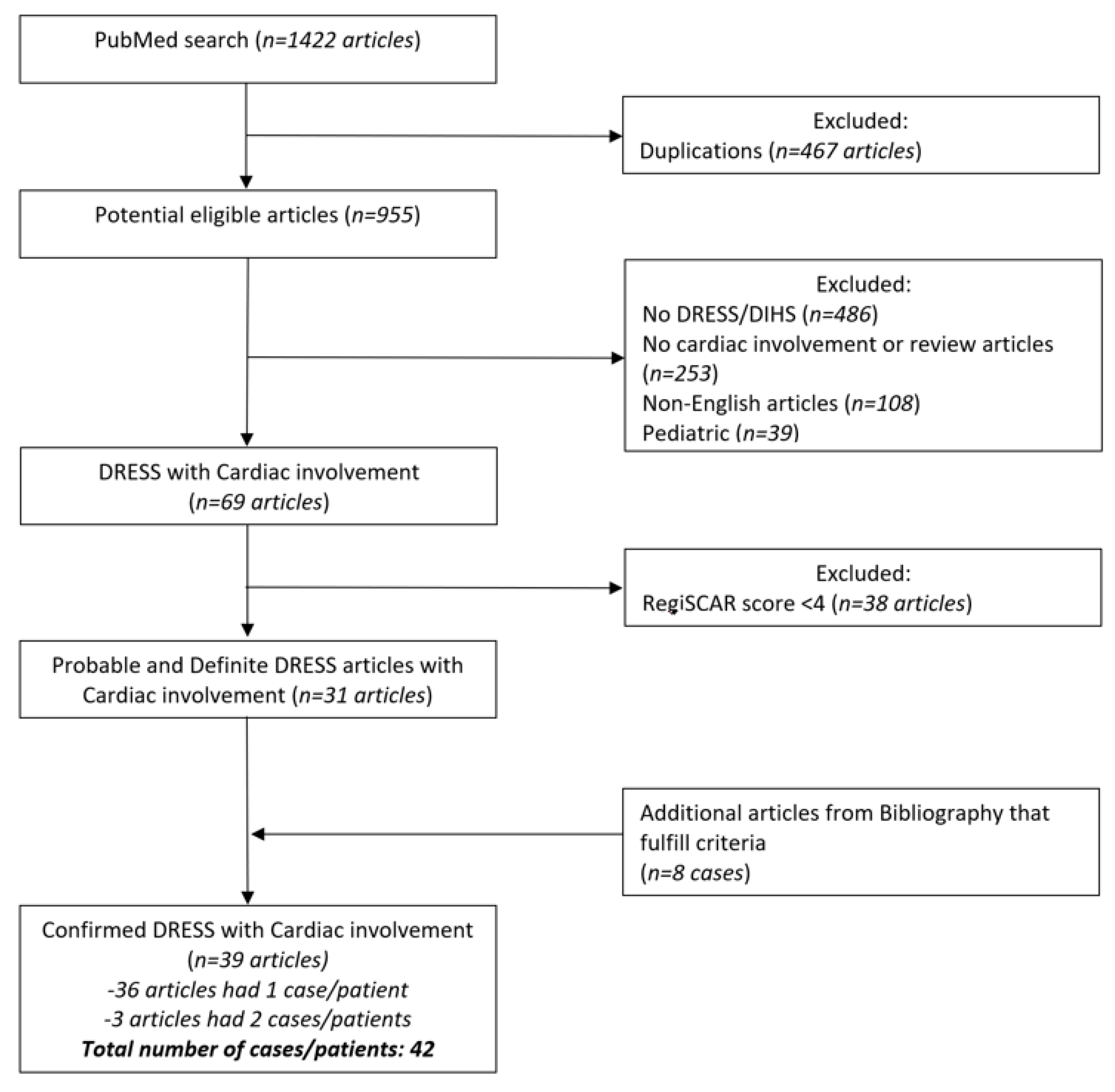
2. Materials and Methods
2.1. Definitions and Selection Criteria
2.2. Database and the Key Words (MeSH)
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Demographics and Co-Morbidities
3.2. Presentation and Latency Period
3.3. Putative Causative Agents
3.4. Cardiac Evaluation
3.5. Treatment and Outcome
4. Discussion
4.1. Age and Sex
4.2. Clinical Manifestations of Cardiac Involvement in DS—Rare Manifestation of a Rare Entity
4.3. DRESS Myocarditis Histopathology
4.4. Significance of Eosinophilia
4.5. Differential Diagnosis of Myocarditis Associated with Peripheral Eosinophilia
4.6. Extent of Other Visceral Organs Involvement
4.7. Medications and Latency
4.8. Treatment and Outcome
4.9. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sontheimer, R.D.; Houpt, K.R. DIDMOHS: A proposed consensus nomenclature for the drug-induced delayed multiorgan hypersensitivity syndrome. Arch. Dermatol. 1998, 134, 874–876. [Google Scholar] [CrossRef] [PubMed]
- Bocquet, H.; Bagot, M.; Roujeau, J.C. Drug-induced pseudolymphoma and drug hypersensitivity syndrome (Drug Rash with Eosinophilia and Systemic Symptoms: DRESS). Semin. Cutan. Med. Surg. 1996, 15, 250–257. [Google Scholar] [CrossRef]
- Cacoub, P.; Musette, P.; Descamps, V.; Meyer, O.; Speirs, C.; Finzi, L.; Roujeau, J.C. The DRESS syndrome: A literature review. Am. J. Med. 2011, 124, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Kardaun, S.H.; Sidoroff, A.; Valeyrie-Allanore, L.; Halevy, S.; Davidovici, B.B.; Mockenhaupt, M.; Roujeau, J.C. Variability in the clinical pattern of cutaneous side-effects of drugs with systemic symptoms: Does a DRESS syndrome really exist? Br. J. Dermatol. 2007, 156, 609–611. [Google Scholar] [CrossRef]
- Jevtic, D.; Dumic, I.; Nordin, T.; Singh, A.; Sulovic, N.; Radovanovic, M.; Jecmenica, M.; Milovanovic, T. Less known gastrointestinal manifestations of drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: A systematic review of the literature. J. Clin. Med. 2021, 10, 4287. [Google Scholar] [CrossRef]
- Taweesedt, P.T.; Nordstrom, C.W.; Stoeckel, J.; Dumic, I. Pulmonary manifestations of drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: A systematic review. BioMed Res. Int. 2019, 2019, 7863815. [Google Scholar] [CrossRef]
- Intarasupht, J.; Kanchanomai, A.; Leelasattakul, W.; Chantrarat, T.; Nakakes, A.; Tiyanon, W. Prevalence, risk factors, and mortality outcome in the drug reaction with eosinophilia and systemic symptoms patients with cardiac involvement. Int. J. Dermatol. 2018, 57, 1187–1191. [Google Scholar] [CrossRef]
- Husain, Z.; Reddy, B.Y.; Schwartz, R.A. DRESS syndrome: Part I. Clinical perspectives. J. Am. Acad. Dermatol. 2013, 68, 693.e1. [Google Scholar] [CrossRef]
- Kanai-Yoshizawa, S.; Sugiyama Kato, T.; Mancini, D.; Marboe, C.C. Hypersensitivity myocarditis and outcome after heart transplantation. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2013, 32, 553–559. [Google Scholar] [CrossRef]
- Loner, C.A.; Crane, P.W. Use of emergency department extracorporeal membrane oxygenation for treatment of acute necrotizing myocarditis. Clin. Pract. Cases Emerg. Med. 2019, 3, 47–50. [Google Scholar] [CrossRef]
- Damsky, W.E.; Vesely, M.D.; Lee, A.I.; Choi, J.; Meyer, A.C.; Chen, M.; Ahmad, T.; King, B. Drug-induced hypersensitivity syndrome with myocardial involvement treated with tofacitinib. JAAD Case Rep. 2019, 5, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Morinaga, Y.; Abe, I.; Minamikawa, T.; Ueda, Y.; Nii, K.; Sakamoto, K.; Inoue, R.; Mitsutake, T.; Hanada, H.; Tsugawa, J.; et al. A case of drug-induced hypersensitivity syndrome induced by salazosulfapyridine combined with SIADH caused by interstitial pneumonia. Drug Discov. Ther. 2019, 13, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Van Kester, M.S.; Langeveld, T.J.C.; Bouwsma, H.; van Rees, J.B.; Holman, E.R.; Teng, Y.K.O.; van Zuuren, E.J. A breathtaking DRESS due to amoxicillin-clavulanate presenting as polymorphic eruption of the pregnancy. J. Eur. Acad. Dermatol. Venereol. 2018, 32, e436–e437. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, D.; Hiraoka, E.; Obunai, K.; Norisue, Y. Myocarditis associated with drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: A case report and review of the literature. Am. J. Case Rep. 2018, 19, 978–984. [Google Scholar] [CrossRef]
- Kowtoniuk, R.; Pinninti, M.; Tyler, W.; Doddamani, S. DRESS syndrome-associated acute necrotizing eosinophilic myocarditis with giant cells. BMJ Case Rep. 2018, 2018, bcr-2018. [Google Scholar] [CrossRef]
- James, J.; Sammour, Y.M.; Virata, A.R.; Nordin, T.A.; Dumic, I. Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome secondary to furosemide: Case report and review of literature. Am. J. Case Rep. 2018, 19, 163–170. [Google Scholar] [CrossRef]
- Hagiwara, H.; Fukushima, A.; Iwano, H.; Anzai, T. Refractory cardiac myocarditis associated with drug rash with eosinophilia and systemic symptoms syndrome due to anti-bipolar disorder drugs: A case report. Eur. Heart J. Case Rep. 2018, 2, yty100. [Google Scholar] [CrossRef]
- Thongsri, T.; Chularojanamontri, L.; Pichler, W.J. Cardiac involvement in DRESS syndrome. Asian Pac. J. Allergy Immunol. 2017, 35, 3–10. [Google Scholar]
- Menter, T.; Tzankov, A. Drug reaction, eosinophilia, and systemic symptoms (DRESS) syndrome associated with allopurinol leading to acute necrotizing eosinophilic myocarditis and death due to papillary muscle rupture. J. Allergy Clin. Immunol. Pract. 2016, 4, 1262–1264. [Google Scholar] [CrossRef]
- Hoogeveen, R.M.; van der Bom, T.; de Boer, H.H.; Thurlings, R.M.; Wind, B.S.; de Vries, H.J.C.; van Lent, A.U.; Beuers, U.; van der Wal, A.C.; Nellen, F.J. A lethal case of the dapsone hypersensitivity syndrome involving the myocardium. Neth. J. Med. 2016, 74, 89–92. [Google Scholar]
- Micozzi, S.; Pinto, C.; Seoane, M.; Carbone, J.; Tornero, P. Giant cell myocarditis in hypersensitivity reactions: Is an early diagnose possible? Ann. Allergy Asthma Immunol. 2015, 115, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Ewart, D.; Garcia, S.; Peltola, J.; Vakil, K. Infiltrating a traveler’s heart: A unique presentation of acute heart failure. Am. J. Med. 2016, 129, e223–e226. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mancano, M.A. Risk factors for androgen deficiency with daily opioid use; co-trimoxazole and sudden cardiac death in patients receiving ACE inhibitors; Clindamycin-induced myelosuppression; Apixaban-induced diffuse alveolar hemorrhage; DRESS syndrome induced by allopurinol. Hosp. Pharm. 2015, 50, 189–193. [Google Scholar]
- Jeremic, I.; Vujasinovic-Stupar, N.; Terzic, T.; Damjanov, N.; Nikolic, M.; Bonaci-Nikolic, B. Fatal sulfasalazine-induced eosinophilic myocarditis in a patient with periodic fever syndrome. Med. Princ. Pract. Int. J. Kuwait Univ. Health Sci. Cent. 2015, 24, 195–197. [Google Scholar] [CrossRef] [PubMed]
- Favoccia, C.; Crimi, G.; Caimmi, S.; Rordorf, R. An unusual complication occurring after cardiac radiofrequency ablation: The devil wears DRESS. Eur. Heart J. 2016, 37, 2502. [Google Scholar] [CrossRef][Green Version]
- Wu, P.A.; Anadkat, M.J. Fever, eosinophilia, and death: A case of minocycline hypersensitivity. Cutis 2014, 93, 107–110. [Google Scholar]
- Kanno, K.; Sakai, H.; Yamada, Y.; Iizuka, H. Drug-induced hypersensitivity syndrome due to minocycline complicated by severe myocarditis. J. Dermatol. 2014, 41, 160–162. [Google Scholar] [CrossRef]
- Choi, H.G.; Byun, J.; Moon, C.H.; Yoon, J.H.; Yang, K.Y.; Park, S.C.; Han, C.J. Allopurinol-induced DRESS syndrome mimicking biliary obstruction. Clin. Mol. Hepatol. 2014, 20, 71–75. [Google Scholar] [CrossRef]
- Eppenberger, M.; Hack, D.; Ammann, P.; Rickli, H.; Maeder, M.T. Acute eosinophilic myocarditis with dramatic response to steroid therapy: The central role of echocardiography in diagnosis and follow-up. Tex. Heart Inst. J. 2013, 40, 326–330. [Google Scholar]
- De Campos, F.P.F.; de Lima, P.P.; Maragno, L.; Watanabe, F.T. Hepatic necrosis associated with drug-induced hypersensitivity syndrome. Autops. Case Rep. 2012, 2, 5–14. [Google Scholar] [CrossRef]
- Daoulah, A.; Alqahtani, A.A.; Ocheltree, S.R.; Alhabib, A.; Ocheltree, A.R. Acute myocardial infarction in a 56-year-old female patient treated with sulfasalazine. Am. J. Emerg. Med. 2012, 30, 638.e1. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, G.P.; Cafardi, J.A.; Groysman, V.; Pamboukian, S.V.; Kirklin, J.K.; Andea, A.A.; Hughey, L.C. Fulminant myocarditis as a late sequela of DRESS: Two cases. J. Am. Acad. Dermatol. 2011, 65, 889–890. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, K.K.; Bouchard, S.M.; Mohr, M.R.; Herre, J.M.; Salkey, K.S. Minocycline-induced drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome with persistent myocarditis. J. Am. Acad. Dermatol. 2010, 62, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.J.; He, F.T.; Jin, N.; Lou, J.X.; Cheng, H. Complete atrioventricular block associated with dapsone therapy: A rare complication of dapsone-induced hypersensitivity syndrome. J. Clin. Pharm. Ther. 2009, 34, 489–492. [Google Scholar] [CrossRef]
- Pursnani, A.; Yee, H.; Slater, W.; Sarswat, N. Hypersensitivity myocarditis associated with azithromycin exposure. Ann. Intern. Med. 2009, 150, 225–226. [Google Scholar] [CrossRef]
- Eshki, M.; Allanore, L.; Musette, P.; Milpied, B.; Grange, A.; Guillaume, J.C.; Chosidow, O.; Guillot, I.; Paradis, V.; Joly, P.; et al. Twelve-year analysis of severe cases of drug reaction with eosinophilia and systemic symptoms: A cause of unpredictable multiorgan failure. Arch. Dermatol. 2009, 145, 67–72. [Google Scholar] [CrossRef]
- Aigner, F.; Aigner, W.; Hoppichler, F.; Luef, G.; Bonatti, H. Diarrhea, negative t-waves, fever and skin rash, rare manifestation of carbamazepine hypersensitivity: A case report. Cases J. 2008, 1, 312. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Poh, K.K.; Mega, J.L.; Shepard, J.A.; Stone, J.R.; Frosch, M.P. Case records of the Massachusetts General Hospital. Case 36-2007. A 31-year-old woman with rash, fever, and hypotension. N. Engl. J. Med. 2007, 357, 2167–2178. [Google Scholar] [CrossRef]
- Teo, R.Y.; Tay, Y.K.; Tan, C.H.; Ng, V.; Oh, D.C. Presumed dapsone-induced drug hypersensitivity syndrome causing reversible hypersensitivity myocarditis and thyrotoxicosis. Ann. Acad. Med. Singap. 2006, 35, 833–836. [Google Scholar]
- Zaidi, A.N. Anticonvulsant hypersensitivity syndrome leading to reversible myocarditis. Can. J. Clin. Pharmacol. 2005, 12, e33–e40. [Google Scholar]
- Lee, C.W.; Mitchell, R.N.; Horan, R.F.; Castells, M.C. Cardiogenic shock and peripheral eosinophilia in a young woman. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 2005, 95, 229–233. [Google Scholar] [CrossRef]
- Ichiche, M.; Kiesch, N.; De Bels, D. DRESS syndrome associated with HHV-6 reactivation. Eur. J. Intern. Med. 2003, 14, 498–500. [Google Scholar] [CrossRef] [PubMed]
- Bagshaw, S.M.; Cload, B.; Gilmour, J.; Leung, S.T.; Bowen, T.J. Drug-induced rash with eosinophilia and systemic symptoms syndrome with bupropion administration. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 2003, 90, 572–575. [Google Scholar] [CrossRef]
- Chan, Y.C.; Tay, Y.K.; Ng, S.K. Allopurinol hypersensitivity syndrome and acute myocardial infarction—Two case reports. Ann. Acad. Med. Singap. 2002, 31, 231–233. [Google Scholar] [PubMed]
- Adachi, Y.; Yasumizu, R.; Hashimoto, F.; Otsuka, Y.; Okamura, A.; Kato, Y.; Oyaizu, H.; Ikebukuro, K.; Fukuhara, S.; Nakai, Y.; et al. An autopsy case of giant cell myocarditis probably due to a non-steroidal anti-inflammatory drug. Pathol. Int. 2001, 51, 113–117. [Google Scholar] [CrossRef]
- Arima, M.; Kanoh, T.; Yamasaki, A.; Matsuda, S.; Kasuya, H.; Sunayama, S.; Kawai, S.; Okada, R. Eosinophilic myocarditis associated with toxicodermia caused by phenobarbital. Jpn. Circ. J. 1998, 62, 132–135. [Google Scholar] [CrossRef][Green Version]
- Ishikawa, H.; Kaneko, H.; Watanabe, H.; Takagi, A.; Ming, Z.W. Giant cell myocarditis in association with drug-induced skin eruption. Acta Pathol. Jpn. 1987, 37, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Taliercio, C.P.; Olney, B.A.; Lie, J.T. Myocarditis related to drug hypersensitivity. Mayo Clin. Proc. 1985, 60, 463–468. [Google Scholar] [CrossRef]
- Ang, C.C.; Wang, Y.S.; Yoosuff, E.L.; Tay, Y.K. Retrospective analysis of drug-induced hypersensitivity syndrome: A study of 27 patients. J. Am. Acad. Dermatol. 2010, 63, 219–227. [Google Scholar] [CrossRef]
- Brambatti, M.; Matassini, M.V.; Adler, E.D.; Klingel, K.; Camici, P.G.; Ammirati, E. Eosinophilic myocarditis: Characteristics, treatment, and outcomes. J. Am. Coll. Cardiol. 2017, 70, 2363–2375. [Google Scholar] [CrossRef]
- Ginsberg, F.; Parrillo, J.E. Eosinophilic myocarditis. Heart Fail. Clin. 2005, 1, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Kuchynka, P.; Palecek, T.; Masek, M.; Cerny, V.; Lambert, L.; Vitkova, I.; Linhart, A. Current diagnostic and therapeutic aspects of eosinophilic myocarditis. BioMed Res. Int. 2016, 2016, 2829583. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Brooks, E.G. Giant cell myocarditis: A brief review. Arch. Pathol. Lab. Med. 2016, 140, 1429–1434. [Google Scholar] [CrossRef] [PubMed]
- Blauwet, L.A.; Cooper, L.T. Myocarditis. Prog. Cardiovasc. Dis. 2010, 52, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T., Jr.; Berry, G.J.; Shabetai, R. Idiopathic giant-cell myocarditis—Natural history and treatment. N. Engl. J. Med. 1997, 336, 1860–1866. [Google Scholar] [CrossRef]
- Bourgeois, G.P.; Cafardi, J.A.; Groysman, V.; Hughey, L.C. A review of DRESS-associated myocarditis. J. Am. Acad. Dermatol. 2012, 66, e229–e236. [Google Scholar] [CrossRef]
- Kardaun, S.H.; Sekula, P.; Valeyrie-Allanore, L.; Liss, Y.; Chu, C.Y.; Creamer, D.; Sidoroff, A.; Naldi, L.; Mockenhaupt, M.; Roujeau, J.C. Drug reaction with eosinophilia and systemic symptoms (DRESS): An original multisystem adverse drug reaction. Results from the prospective RegiSCAR study. Br. J. Dermatol. 2013, 169, 1071–1080. [Google Scholar] [CrossRef]
- Mizukawa, Y.; Hirahara, K.; Kano, Y.; Shiohara, T. Drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms severity score: A useful tool for assessing disease severity and predicting fatal cytomegalovirus disease. J. Am. Acad. Dermatol. 2019, 80, 670–678.e2. [Google Scholar] [CrossRef]
- Moriwaki, K.; Dohi, K.; Omori, T.; Tanimura, M.; Sugiura, E.; Nakamori, S.; Sawai, T.; Imanaka-Yoshida, K.; Yamada, N.; Ito, M. A survival case of fulminant right-side dominant eosinophilic myocarditis. Int. Heart J. 2017, 58, 459–462. [Google Scholar] [CrossRef][Green Version]
- Peretto, G.; Sala, S.; Rizzo, S.; De Luca, G.; Campochiaro, C.; Sartorelli, S.; Benedetti, G.; Palmisano, A.; Esposito, A.; Tresoldi, M.; et al. Arrhythmias in myocarditis: State of the art. Heart Rhythm 2019, 16, 793–801. [Google Scholar] [CrossRef]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar] [PubMed]
- Ammirati, E.; Cipriani, M.; Lilliu, M.; Sormani, P.; Varrenti, M.; Raineri, C.; Petrella, D.; Garascia, A.; Pedrotti, P.; Roghi, A.; et al. Survival and left ventricular function changes in fulminant versus nonfulminant acute myocarditis. Circulation 2017, 136, 529–545. [Google Scholar] [CrossRef] [PubMed]
- Escher, F.; Pietsch, H.; Aleshcheva, G.; Wenzel, P.; Fruhwald, F.; Stumpf, C.; Westermann, D.; Bauersachs, J.; Enseleit, F.; Ruschitzka, F.; et al. Evaluation of myocardial gene expression profiling for superior diagnosis of idiopathic giant-cell myocarditis and clinical feasibility in a large cohort of patients with acute cardiac decompensation. J. Clin. Med. 2020, 9, 2689. [Google Scholar] [CrossRef]
- Lassner, D.; Kühl, U.; Siegismund, C.S.; Rohde, M.; Elezkurtaj, S.; Escher, F.; Tschöpe, C.; Gross, U.M.; Poller, W.; Schultheiss, H.P. Improved diagnosis of idiopathic giant cell myocarditis and cardiac sarcoidosis by myocardial gene expression profiling. Eur. Heart J. 2014, 35, 2186–2195. [Google Scholar] [CrossRef]
- Li, H.; Dai, Z.; Wang, B.; Huang, W. A case report of eosinophilic myocarditis and a review of the relevant literature. BMC Cardiovasc. Disord. 2015, 15, 15. [Google Scholar] [CrossRef] [PubMed]
- Ogbogu, P.U.; Rosing, D.R.; Horne, M.K., III. Cardiovascular manifestations of hypereosinophilic syndromes. Immunol. Allergy Clin. North Am. 2007, 27, 457–475. [Google Scholar] [CrossRef]
- Sheikh, H.; Siddiqui, M.; Uddin, S.M.M.; Haq, A.; Yaqoob, U. The clinicopathological profile of eosinophilic myocarditis. Cureus 2018, 10, e3677. [Google Scholar] [CrossRef]
- Arustamyan, M.; Hoosain, J.; Mattson, J.; Hasni, S.F.; Cho, S.H.; Gorodin Kiliddar, P. Loeffler endocarditis: A manifestation of hypereosinophilic syndrome. CASE Cardiovasc. Imaging Case Rep. 2020, 4, 74–77. [Google Scholar] [CrossRef]
- Butterfield, J.H.; Kane, G.C.; Weiler, C.R. Hypereosinophilic syndrome: Endomyocardial biopsy versus echocardiography to diagnose cardiac involvement. Postgrad. Med. 2017, 129, 517–523. [Google Scholar] [CrossRef]
- Largeau, B.; Agier, M.S.; Beau-Salinas, F.; Pariente, A.; Maruani, A.; Vial, T.; Jonville-Béra, A.P. Specific features of amoxicillin-associated drug reaction with eosinophilia and systemic symptoms syndrome: A nationwide study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2415–2420. [Google Scholar] [CrossRef]
- Thambidorai, S.K.; Korlakunta, H.L.; Arouni, A.J.; Hunter, W.J.; Holmberg, M.J. Acute eosinophilic myocarditis mimicking myocardial infarction. Tex. Heart Inst. J. 2009, 36, 355–357. [Google Scholar] [PubMed]
- Pereira, C.M.; Vaz, M.; Kotha, S.; Santosh, N.H. Dapsone hypersensitivity syndrome with myocarditis. J. Assoc. Physicians India 2014, 62, 728–731. [Google Scholar] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [PubMed]


{kind=link}
| Demographic Characteristics | ||||
|---|---|---|---|---|
| Gender | Age range (years) | Mean age (years) | ||
| Female | 26 (61.9%) | 19–78 | 41.8 | |
| Male | 16 (38.1%) | 22–84 | 44.5 | |
| Total | 42 (100%) | 19–84 | 42.9 | |
| Race | ||||
| Not reported | 25 (59.5%) | |||
| Asian | 9 (21.4%) | |||
| Caucasian | 5 (12%) | |||
| African-American | 3 (7.1%) | |||
| Co-morbidities | ||||
| None | 19 (45.2%) | |||
| Rheumatologic | 9 (21.4%) | |||
| Hypertension | 7 (16.7%) | |||
| Oncologic | 3 (7.1%) | |||
| Infectious | 2 (4.8%) | |||
| Other, less common (total) | 8 (19%) | |||
| Visceral organs involved | ||||
| Heart only | 7 (16.7%) | |||
| Heart and 1–2 | 30 (71.4%) | |||
| Heart and 3 or more | 5 (11.9%) | |||
| Clinical presentation | ||||
| Arrhythmia | 25 (59.5%) | |||
| Dyspnea | 23 (54.8%) | |||
| Hypotension/Shock | 18 (42.9%) | |||
| Chest pain | 16 (38.1%) | |||
| Cardiac arrest | 5 (11.9%) | |||
| Syncope | 3 (7.1%) | |||
| Timing of cardiac symptoms | ||||
| On initial presentation | 29 (69%) | |||
| Delayed | 12 (28.6%) | |||
| Unknown | 1 (2.4%) | |||
| Latency | Mean (days): | Range (days): | Statistical significance | |
| Drug to DRESS symptoms latency | 34.7 ±22 | 5–91 | p < 0.05 | |
| Recovered patients | 40.7 ± 23 | 10–91 | ||
| Patients who died | 26.7 ± 18 | 5–61 | ||
| Drug to cardiac symptoms latency | 70.1 ± 63 | 13–371 | p > 0.05 | |
| Recovered patients | 58.7 ± 27 | 28–108 | ||
| Patients who died | 82.9 ± 22 | 13–371 | ||
| ECG findings | ||||
| Normal or not reported | 12 (28.6%) | |||
| Abnormal | 30 (71.4%) | |||
| Sinus Tachycardia | 14 (33.4%) | |||
| ST elevation | 11 (26.2%) | |||
| Fascicular blocks (right and left) | 8 (19%) | |||
| ST depression & T inversions | 5 (11.9%) | |||
| Atrio-ventricular block | 3 (7.1%) | |||
| Atrial fibrillation | 3 (7.1%) | |||
| Ventricular arrhythmia | 3 (7.1%) | |||
| Bradycardia | 2 (4.8%) | |||
| Echocardiography findings | ||||
| LVEF < 50% (mean: 27.05 ± 13.2%; range:10–50) | 19 (45.2%) | |||
| Pericardial effusion | 17 (40.5%) | |||
| Regional wall motion abnormalities | 11 (26.2%) | |||
| LV hypertrophy | 4 (9.5%) | |||
| Cardiac MRI | ||||
| Performed | 5 (11.9%) | |||
| Delayed (hyper)enhancement | 3 (60%) | |||
| Normal finding | 2 (40%) | |||
| Histopathological examination | ||||
| Endomyocardial biopsy/Autopsy | 22 (52.4%) | |||
| ANEM | 9 (40.1%) | |||
| Eosinophilic myocarditis | 6 (27.3%) | |||
| GCM | 4 (18.2%) | |||
| Mixed infiltrate | 2 (9.1%) | |||
| Uncertain | 1 (4.5%) | |||
| Outcome | ||||
| Recovered | 23 (54.8%) | |||
| Death | 19 (45.2%) | |||
| Univariate Regression Analysis | |||
|---|---|---|---|
| Variable | p Value | OR | 95% CI for OR |
| Age | 0.035 | 0.872 | 0.768–0.990 |
| Sex | 0.228 | 12.808 | 0.203–808.796 |
| Comorbidities | 0.266 | 0.022 | 0.000–18.361 |
| Pulse | 0.133 | 3.719 | 0.670–20.630 |
| Allopurinol | 0.119 | 6.581 | 0.614–70.524 |
| Minocycline | 0.196 | 0.296 | 0.047–1.874 |
| Latency | 0.028 | 1.162 | 1.016–1.139 |
| AEC | 0.125 | 1.001 | 1.000–1.002 |
| LVEF | 0.876 | 1.006 | 0.937–1.079 |
| Culprit Medication | Number of Cases |
|---|---|
| Minocycline | 8 (19%) |
| Allopurinol | 5 (11.9%) |
| Dapsone | 3 (7.1%) |
| Sulfasalazine | 3 (7.1%) |
| Lamotrigine | 2 (4.8%) |
| Amoxicillin-Clavulanate, Azithromycin, Bisoprolol, Bupropion, Carbamazepine, Furosemide, Modafinil, Phenytoin, Chlorthalidone, Loxoprofen, Salazosulfapyridine | Each in 1 case (2.4%) |
| Suspected polypharmacy | 10 (24%) |
| Ciprofloxacin vs. Scopolamine vs. Dipyrone vs. Diclofenac | |
| Anticonvulsants (Phenytoin, Valproic acid or Carbamazepine) | |
| Amitriptyline vs. Diclofenac vs. Lorazepam | |
| Captopril vs. Bisoprolol | |
| Cefaclor vs. NSAID | |
| Colchicine vs. Allopurinol | |
| Lithium vs. Quetiapine | |
| Phenobarbital vs. Phenytoin | |
| Phenobarbital vs. Phenytoin vs. Metharbital | |
| Trimethoprim/Sulfamethoxazole vs. Zonisamide |
| Therapeutic Options | Number of Cases | |
|---|---|---|
| Immunomodulators | ||
| Steroids | 42 (100%) | |
| Antihistamines | 11 (26.2%) | |
| Steroid sparing therapies | 26 (61.9%) | |
| Cyclosporine | 5 (11.9%) | |
| IVIG | 5 (11.9%) | |
| Mycophenolate-mofetil | 5 (11.9%) | |
| Methotrexate | 2 (4.8%) | |
| Azathioprine | 2 (4.8%) | |
| Tofacitinib | 2 (4.8%) | |
| Colchicine | 1 (2.4%) | |
| Mepolizumab | 1 (2.4%) | |
| Rituximab | 1 (2.4%) | |
| Plasmapheresis | 1 (2.4%) | |
| OKT-3 | 1 (2.4%) | |
| Anti-thymocyte globulin | 1 (2.4%) | |
| Cardiac Specific therapies | ||
| Vasopressors/Inotropic agents | 9 (21.4%) | |
| Intra-aortic balloon pump | 5 (11.9%) | |
| Pericardiocentesis | 3 (7.1%) | |
| ECMO | 3 (7.1%) | |
| LVAD | 1 (2.4%) | |
| Cardiac transplant | 1 (2.4%) | |
| Disease Category | Specific Disease/Comment |
|---|---|
| Allergic/hypersensitivity reactions to medications | DRESS syndrome, smallpox vaccination, dobutamine |
| Infectious Disease | Parasitic infections (Toxocara canis, Toxoplasma gondii, Trichinella spiralis, Trypanosoma cruzi, Echinococcus spp., Strongyloides stercoralis) |
| Neoplastic | Leukemia and lymphoma |
| Paraneoplastic | Carcinoma of biliary tract and lungs |
| Idiopathic | Hypereosinophilic syndrome, Loeffler endomyocardial fibrosis, tropical endomyocardial fibrosis |
| Vasculitis | Eosinophilic granulomatosis with polyangiitis |
| Allograft rejection | Heart transplant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radovanovic, M.; Jevtic, D.; Calvin, A.D.; Petrovic, M.; Paulson, M.; Rueda Prada, L.; Sprecher, L.; Savic, I.; Dumic, I. “Heart in DRESS”: Cardiac Manifestations, Treatment and Outcome of Patients with Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome: A Systematic Review. J. Clin. Med. 2022, 11, 704. https://doi.org/10.3390/jcm11030704
Radovanovic M, Jevtic D, Calvin AD, Petrovic M, Paulson M, Rueda Prada L, Sprecher L, Savic I, Dumic I. “Heart in DRESS”: Cardiac Manifestations, Treatment and Outcome of Patients with Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome: A Systematic Review. Journal of Clinical Medicine. 2022; 11(3):704. https://doi.org/10.3390/jcm11030704
Chicago/Turabian StyleRadovanovic, Milan, Djordje Jevtic, Andrew D. Calvin, Marija Petrovic, Margaret Paulson, Libardo Rueda Prada, Lawrence Sprecher, Ivana Savic, and Igor Dumic. 2022. "“Heart in DRESS”: Cardiac Manifestations, Treatment and Outcome of Patients with Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome: A Systematic Review" Journal of Clinical Medicine 11, no. 3: 704. https://doi.org/10.3390/jcm11030704
APA StyleRadovanovic, M., Jevtic, D., Calvin, A. D., Petrovic, M., Paulson, M., Rueda Prada, L., Sprecher, L., Savic, I., & Dumic, I. (2022). “Heart in DRESS”: Cardiac Manifestations, Treatment and Outcome of Patients with Drug Reaction with Eosinophilia and Systemic Symptoms Syndrome: A Systematic Review. Journal of Clinical Medicine, 11(3), 704. https://doi.org/10.3390/jcm11030704