
Inflammatory Markers and Episodic Memory Functioning in Depressive Disorders



Abstract
:1. Introduction
2. Materials and Methods
3. Results
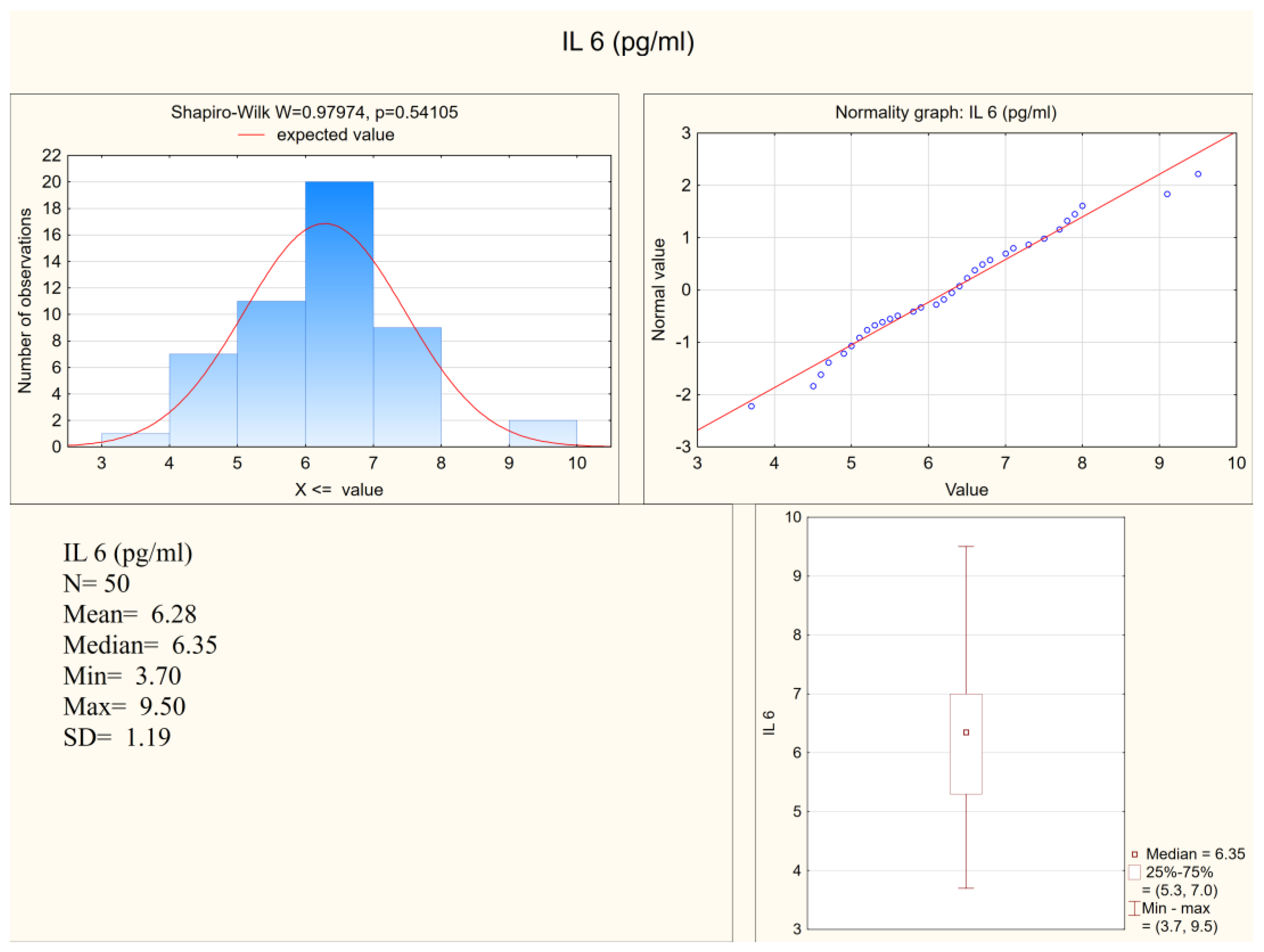
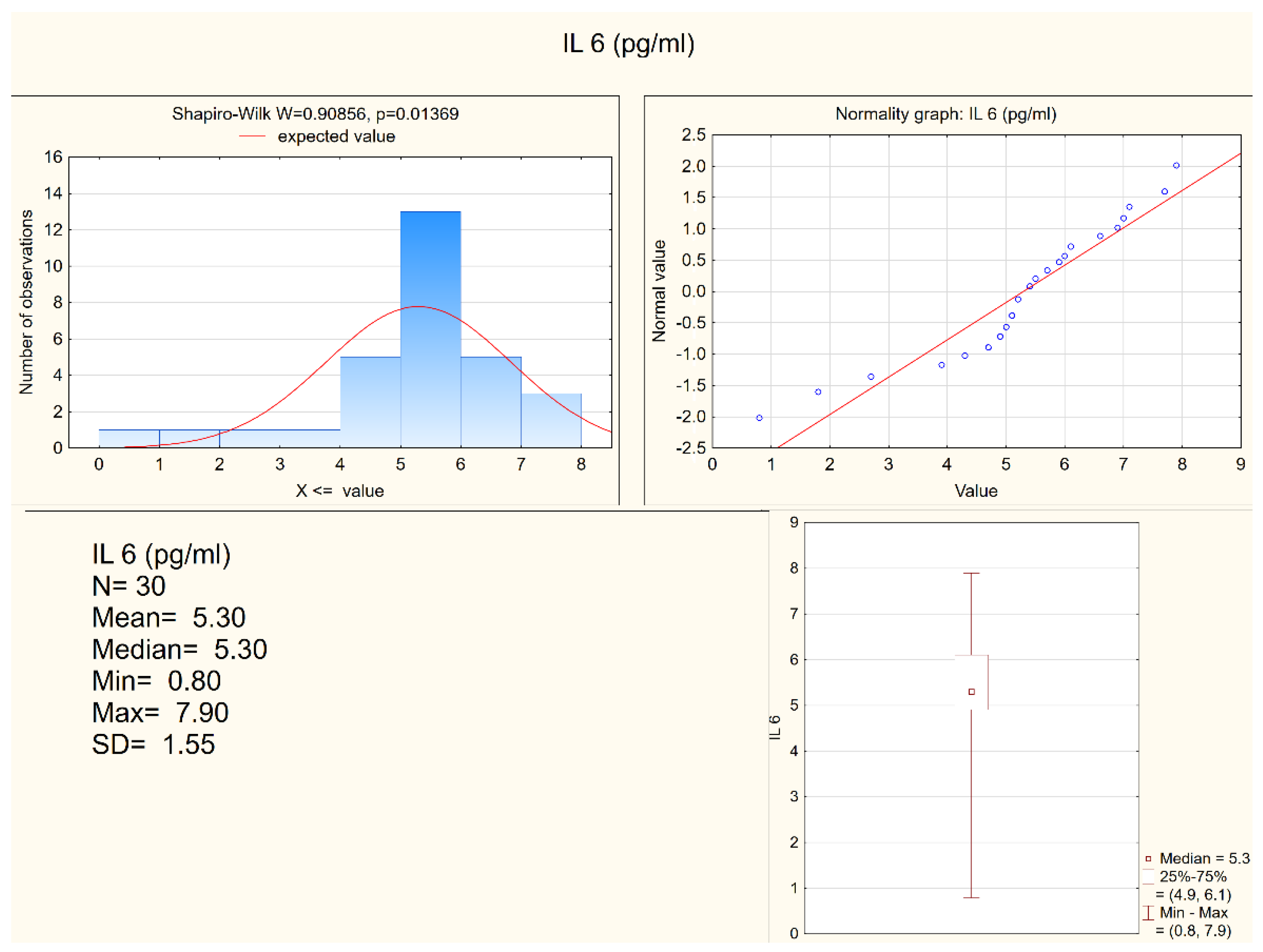
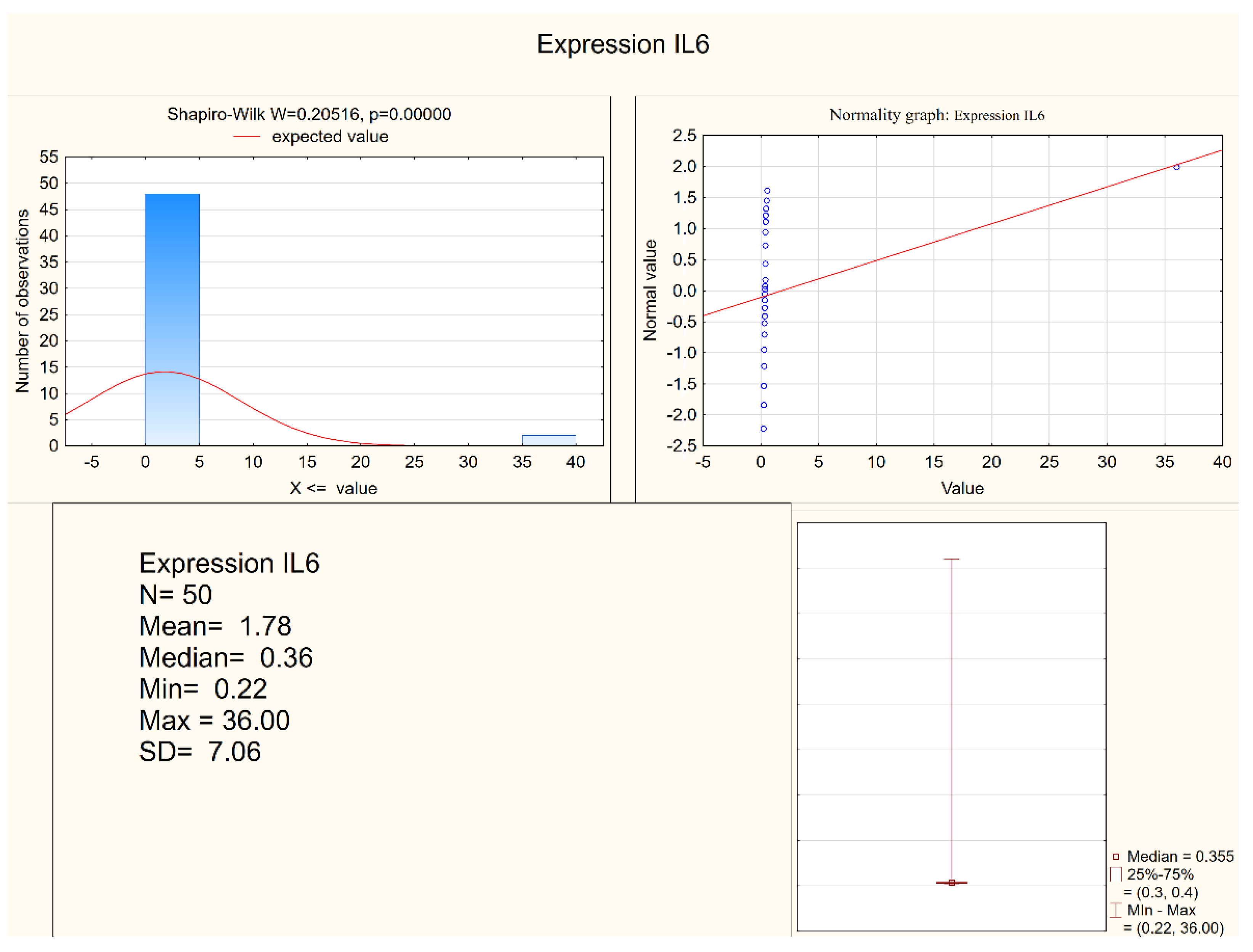
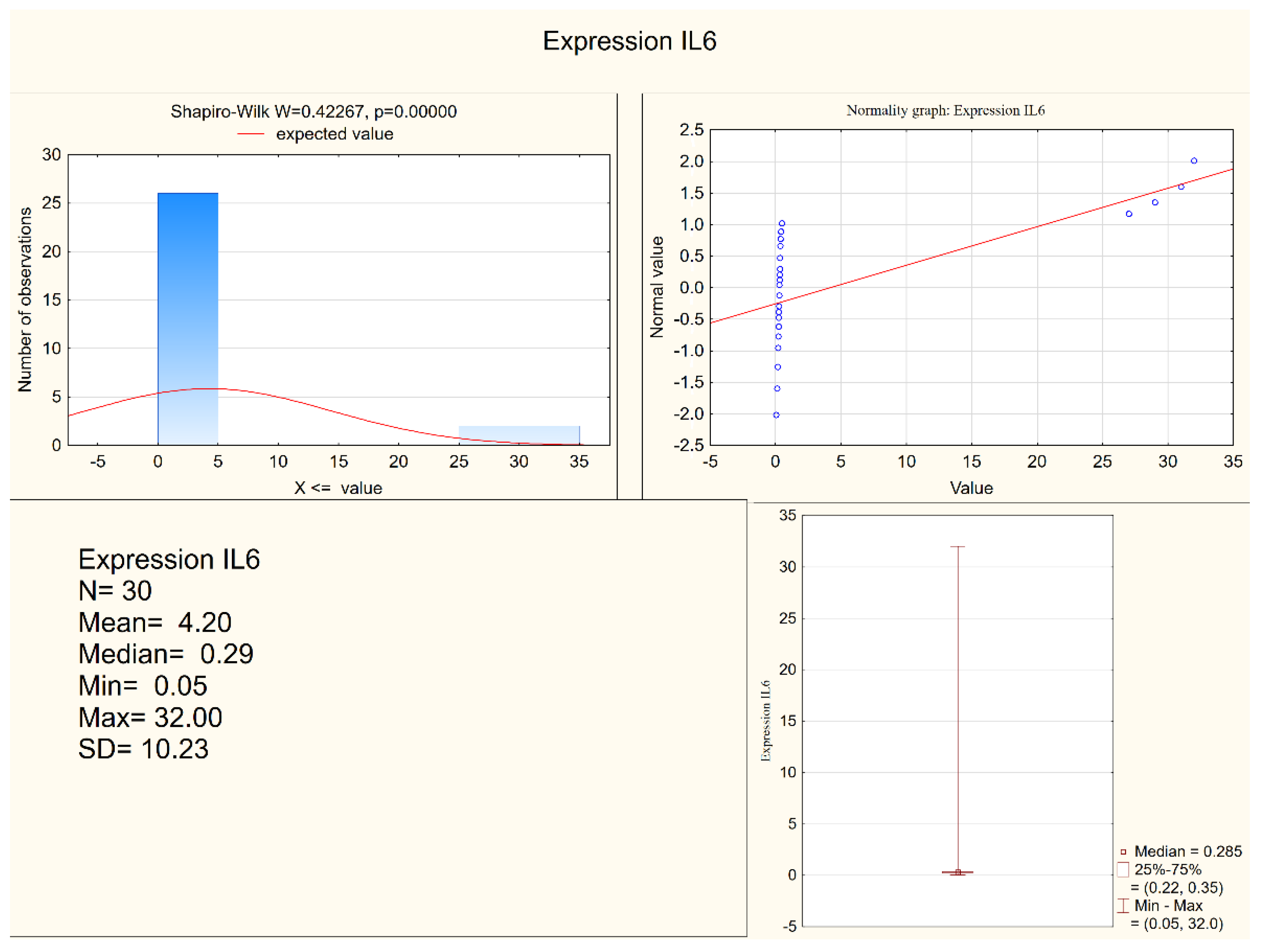
3.1. Inflammatory Markers
3.2. Memory Function
3.3. Correlations Coefficients among Serum Levels of Interleukins and Results in Memory Tests and Depression Severity
4. Discussion
5. Conclusions
- Increased serum levels of inflammatory markers IL-1 and IL-6 are observed among patients suffering from depression when compared to healthy controls.
- Episodic memory functioning, in terms of answering structured questions about the past, is deteriorated, in comparison to healthy control groups.
- Episodic memory functioning, in terms of free recalling of events, is not different when compared to healthy participants.
- Although the presented data confirm previous observations of increased levels of inflammatory markers among depressed patients, the collected data do not allow associating inflammatory imbalance with episodic memory functioning. The observed memory disturbances are not associated with changes in serum levels of examined inflammatory markers in a study group. However, in the healthy control, group we observed a reverse correlation between the serum level of IL-6 and free recalling of life events (only for a number of remembered events, not for an objective indicator). This might suggest that non-depressed subjects have more difficulties with free recollection of memories when there is a biochemical sign of an inflammatory process.
- The presented study has limitations, such as a relatively low number of participants, as well as of the control group, and a lack of prospective observations of depressed patients. Moreover, examining memories of life events is quite difficult since it is a strongly subjective matter. Therefore, the obtained results need to be treated with caution and should be confirmed in further research.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates (No. WHO/MSD/MER/2017.2); World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Osimo, E.F.; Baxter, L.J.; Lewis, G.; Jones, P.B.; Khandaker, G.M. Prevalence of low-grade inflammation in depression: A systematic review and meta-analysis of CRP levels. Psychol. Med. 2019, 49, 1958–1970. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Giuliani, F. The role of inflammation in depression and fatigue. Front. Immunol. 2019, 10, 1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valkanova, V.; Ebmeier, K.P.; Allan, C.L. CRP, IL-6 and depression: A systematic review and meta-analysis of longitudinal studies. J. Affect. Disord. 2013, 150, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Howren, M.B.; Lamkin, D.M.; Suls, J. Associations of depression with C-reactive protein, IL-1, and IL-6: A meta-analysis. Psychosom. Med. 2009, 71, 171–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So depression is an inflammatory disease but where does the inflammation comes form? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.K.; Na, K.S.; Myint, A.M.; Leonard, B.E. The role of pro-inflammatory cytokines in neuroinflammation, neurogenesis and the neuroendocrine system in major depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 64, 277–284. [Google Scholar] [CrossRef]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A meta-analysis of cytokines in major depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef]
- Hiles, S.A.; Baker, A.L.; de Malmanche, T.; Attia, J. A meta-analysis of differences in IL-6 and IL-10 between people with and without depression: Exploring the causes of heterogeneity. Brain Behav. Immun. 2012, 26, 1180–1188. [Google Scholar] [CrossRef]
- Gałecka, M.; Bliźniewska-Kowalska, K.; Orzechowska, A.; Szemraj, J.; Maes, M.; Berk, M.; Su, K.-P.; Gałecki, P. Inflammatory versus Anti-inflammatory Profiles in Major Depressive Disorders—The Role of IL-17, IL-21, IL-23, IL-35 and Foxp3. J. Pers. Med. 2021, 11, 66. [Google Scholar] [CrossRef]
- Roca, M.; Vives, M.; López-Navarro, E.; García-Campayo, J.; Gili, M. Cognitive impairments and depression: A critical review. Actas Esp. Psiquiatr. 2015, 43, 187–193. [Google Scholar] [PubMed]
- Trivedi, M.H.; Greer, T.L. Cognitive dysfunction in unipolar depression: Implications for treatment. J. Affect. Disord. 2014, 152–154, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Rock, P.L.; Poiser, J.P.; Riedel, W.J.; Blackwell, A.D. Cognitive impairment in depression: A systematic review and meta-analysis. Psychol. Med. 2014, 44, 2029–2040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDermott, L.M.; Ebmeier, K.P. A meta-analysis of depression severity and cognitive function. J. Affect. Disord. 2009, 119, 1–8. [Google Scholar] [CrossRef] [PubMed]
- International Classification of Diseases (ICD). 11th Revision. Available online: https://icd.who.int/browse11/l-m/en (accessed on 12 January 2022).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Jin, K.; Lu, J.; Yu, Z.; Shen, Z.; Li, H.; Mou, T.; Xuab, Y.; Huang, M. Linking peripheral IL-6, IL-1β and hypocretin-1 with cognitive impairment from major depression. J. Affect. Disord. 2020, 277, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; Au, B.; Ollis, L.; Schmitz, N. The association between C-reactive protein, Interleukin-6 and depression among older adults in the community: A systematic review and meta-analysis. Exp. Gerontol. 2018, 102, 109–132. [Google Scholar] [CrossRef] [PubMed]
- Zalli, A.; Jovanova, O.; Hoogendijk, W.J.G.; Tiemeier, H.; Carvalho, L.A. Low-grade inflammation predicts persistence of depressive symptoms. Psychopharmacology 2016, 233, 1669–1678. [Google Scholar] [CrossRef] [Green Version]
- Khandaker, G.M.; Zammit, S.; Burgess, S.; Lewis, G.; Jones, P.B. Association between a functional interleukin 6 receptor genetic variant and risk of depression and psychosis in a population-based birth cohort. Brain Behav. Immun. 2018, 69, 264–272. [Google Scholar] [CrossRef]
- Tegeler, C.; O’Sullivan, J.L.; Bucholtz, N.; Goldeck, D.; Pawelec, G.; Steinhagen-Thiessen, E.; Demuth, I. The inflammatory markers CRP, IL-6, and IL-10 are associated with cognitive function—data from the Berlin Aging Study II. Neurobiol. Aging 2016, 38, 112–117. [Google Scholar] [CrossRef]
- Ali, N.S.; Hashem, A.H.H.; Hassan, A.M.; Saleh, A.A.; El-Baz, H.N. Serum interleukin-6 is related to lower cognitive functioning in elderly patients with major depression. Aging Ment. Health 2018, 22, 655–661. [Google Scholar] [CrossRef]
- Mac Giollabhui, N.; Swistun, D.; Murray, S.; Moriarity, D.P.; Kautz, M.M.; Ellman, L.M.; Olino, T.M.; Coe, C.L.; Abramson, L.Y.; Alloy, L.B. Executive dysfunction in depression in adolescence: The role of inflammation and higher body mass. Psychol. Med. 2020, 50, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Charlton, R.A.; Lamar, M.; Zhang, A.; Ren, X.; Ajilore, O.; Pandey, G.N.; Kumar, A. Associations between pro-inflammatory cytokines, learning, and memory in late-life depression and healthy aging. Int. J. Geriatr. Psychiatry 2018, 33, 104–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belge, J.B.; Van Diermen, L.; Sabbe, B.; Morrens, M.; Coppens, V.; de Timary, P.; Constant, E.; Sienaert, P.; Schrijvers, D. Inflammatory Markers May Inform the Effects of Electroconvulsive Therapy on Cognition in Patients with Depression. Neuropsychobiology 2021, 80, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, H.; Mizoguchi, Y.; Kawaguchi, A.; Imamura, Y.; Matsushima, J.; Kunitake, H.; Maekawad, T.; Katod, T.A.; Asami, T.; Monji, A. Changes in interleukin-1 beta induced by rTMS are significantly correlated with partial improvement of cognitive dysfunction in treatment-resistant depression: A pilot study. Psychiatry Res. 2020, 289, 112995. [Google Scholar] [CrossRef] [PubMed]
- Atique-Ur-Rehman, H.; Neill, J.C. Cognitive dysfunction in major depression: From assessment to novel therapies. Pharmacol. Ther. 2019, 202, 53–71. [Google Scholar] [CrossRef]
- Huang, M.H.; Chen, M.H.; Hsu, J.W.; Huang, K.L.; Tsai, S.J.; Su, T.P.; Bai, Y.M. Inflammation, cognitive dysfunction, and suicidal ideation among patients with major depression. CNS Spectr. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Young, K.D.; Drevets, W.C.; Dantzer, R.; Teague, T.K.; Bodurka, J.; Savitz, J. Kynurenine pathway metabolites are associated with hippocampal activity during autobiographical memory recall in patients with depression. Brain Behav. Immun. 2016, 56, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, M.A.; Pleydell-Pearce, C.W. The construction of autobiographical memories in the self-memory system. Psychol Rev. 2000, 107, 261–288. [Google Scholar] [CrossRef] [PubMed]
- Maruszewski, T. Pamięć autobiograficzna-nowe dane. Neuropsychiatr. Neuropsychol. 2010, 5, 122–129. [Google Scholar]
- Brittlebank, A.D.; Scott, J.; Williams, G.; Mark, J.; Ferrier, I.N. Autobiographical memory in depression: A state or trait marker? BJPsych 1993, 162, 118–121. [Google Scholar] [CrossRef]
- Wesnes, K.A.; Hopkins, S.C.; Brooker, H.J.; Koblan, K.S. Differences in memory function between 5-HT1A receptor genotypesin patients with major depressive disorder. CNS Spectr. 2016, 19, 1–6. [Google Scholar]
- Videbech, P.; Ravnkilde, B. Hippocampal volume and depression. A meta-analysis of MRI studies. Am. J. Psychiatry 2004, 161, 1957–1966. [Google Scholar] [CrossRef] [PubMed]
- Milne, A.M.; MacQueen, G.M.; Hall, G.B. Abnormal hippocampal activation in patients with extensive history of major depression. An fMRI study. J. Psychiatry Neurosci. 2012, 37, 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marsland, A.L.; Gianaros, P.J.; Abramowitch, S.M.; Manuck, S.B.; Hariri, A.R. Interleukin—6 Covaries Inversely with Grey Matter Volume in Middle Aged Adults. Biol. Psychiatry 2008, 64, 484–490. [Google Scholar] [CrossRef] [Green Version]
- Bruno, A.; Dolcetti, E.; Rizzo, F.R.; Fresegna, D.; Musella, A.; Gentile, A.; de Vito, F.; Caioli, S.; Guadalupi, L.; Bullitta, S.; et al. Inflammation-associated synaptic alterations as shared threads in depression and multiple sclerosis. Front. Cell. Neurosci. 2020, 14, 169. [Google Scholar] [CrossRef]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The bidirectional relationship of depression and inflammation: Double trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef]
- Gałecka, M.; Bliźniewska-Kowalska, K.; Maes, M.; Su, K.P.; Gałecki, P. Update on the neurodevelopmental theory of depression: Is there any ‘unconscious code’? Pharmacol. Rep. 2020, 73, 1–11. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Study Group |
|---|---|
| Number of patients | 50 |
| Age | 46.34 ± 11.18 |
| Number of hospitalizations | 2.06 ± 2.11 |
| Male/Female | 40/10 |
| Living in a big city/small city | 34/16 |
| Smokers/non-smokers | 32/18 |
| Education secondary education level/higher level | 39/11 |
| Parameters Associated with Severity of Depression | |
| Years of psychiatric treatment | 4.73 ± 6.25 |
| Result in HDRS | 18.27 ± 7.2 |
| Demographic Characteristics | Study Group |
|---|---|
| Number of participants | 37 |
| Age | 40.2 ± 16.42 |
| Male/Female | 28/9 |
| Living in a big city/small city | 30/7 |
| Smokers/non-smokers | 8/29 |
| Education secondary education level/higher level | 11/26 |
| Name of a Marker | Medium | Median | Min | Max | SD |
|---|---|---|---|---|---|
| IL-1 β (pg/mL) | 10.75 | 11.0 | 7.8 | 13.2 | 1.45 |
| Expression IL1 β | 2.47 | 0.73 | 0.47 | 88.0 | 12.34 |
| Il-6 (pg/mL) | 6.28 | 6.35 | 3.7 | 9.5 | 1.18 |
| Expression IL6 | 1.78 | 0.36 | 0.22 | 36.0 | 7.06 |
| Name of a Marker | Medium | Median | Min | Max | SD |
|---|---|---|---|---|---|
| IL-1 (pg/mL) | 8.28 | 8.05 | 4.80 | 11.10 | 1.38 |
| Expression IL1 β | 5.31 | 0.67 | 0.29 | 69.00 | 16.95 |
| Il-6 (pg/mL) | 5.30 | 5.30 | 0.80 | 7.90 | 1.54 |
| Expression IL6 | 4.20 | 0.29 | 0.05 | 32.00 | 10.22 |
| Name of a Marker | N | Mean | Med | Min | Max | SD | Skewness | Mann-Whitney U Test | p Value |
|---|---|---|---|---|---|---|---|---|---|
| IL-1 (pg/mL) | 80.00 | 9.83 | 9.80 | 4.80 | 13.20 | 1.86 | −0.20 | 5.77 | 0.00 |
| Expression IL1 β | 80.00 | 3.53 | 0.70 | 0.29 | 88.00 | 14.21 | 5.09 | 1.89 | 0.06 |
| Il-6 (pg/mL) | 80.00 | 5.91 | 5.95 | 0.80 | 9.50 | 1.40 | −0.62 | 2.76 | 0.01 |
| Expression IL6 β | 80.00 | 2.69 | 0.33 | 0.05 | 36.00 | 8.40 | 3.36 | 2.88 | 0.00 |
| Name of a Parameter | Medium | Median | Min | Max | SD |
|---|---|---|---|---|---|
| Task 1 Memories of social events | 6.93 | 7.00 | 0.00 | 25.00 | 5.32 |
| Task 2 Indicator | 0.40 | 0.32 | 0.00 | 1.73 | 0.31 |
| Total score episodic memory | 22.02 | 22.00 | 0.00 | 33.00 | 7.17 |
| Name of a Parameter | Medium | Median | Min | Max | SD |
|---|---|---|---|---|---|
| Task 1 Number of memories of social events | 7.16 | 7.00 | 0.00 | 37.00 | 6.31 |
| Task 2 Indicator | 0.51 | 0.47 | 0.00 | 1.21 | 0.33 |
| Total score episodic memory | 27.54 | 27.00 | 16.00 | 35.00 | 4.11 |
| Memory Parameter | N | Mean | Med | Min | Max | SD | Skewness | Mann–Whitney U Test | p Value |
|---|---|---|---|---|---|---|---|---|---|
| Task 1 Number of memories of social events | 80.00 | 7.04 | 7.00 | 0.00 | 37.00 | 5.77 | 2.11 | 0.19 | 0.85 |
| Task 2 Indicator | 87.00 | 0.45 | 0.39 | 0.00 | 1.73 | 0.32 | 1.31 | −1.86 | 0.06 |
| Total score episodic memory | 87.00 | 24.37 | 25.00 | 0.00 | 35.00 | 6.63 | −0.96 | −3.78 | 0.00 |
| Study Group | Spearman’s Rank Order Correlation MD Removed in Pairs The Marked Correlation Coefficients Are Significant p < 0.05000 | |||
|---|---|---|---|---|
| N | R | t-Student Test t (N-2) | p | |
| IL 1β (pg/mL) and HDRS score | 48 | −0.136 | −0.934 | 0.355 |
| IL 1 β (pg/mL) and total score episodic memory | 50 | 0.203 | 1.436 | 0.158 |
| IL 1 β (pg/mL) and years of psychiatric treatment | 45 | −0.045 | −0.293 | 0.771 |
| IL 1 β (pg/mL) and number of events on “lifeline” | 50 | 0.026 | 0.179 | 0.859 |
| IL 1 β (pg/mL) and indicator | 50 | 0.085 | 0.593 | 0.556 |
| Expression IL1 β and HDRS score | 48 | 0.076 | 0.516 | 0.608 |
| Expression IL1 β and total score episodic memory | 50 | 0.037 | 0.254 | 0.801 |
| Expression IL1 β and years of psychiatric treatment | 45 | 0.152 | 1.007 | 0.320 |
| Expression IL1 β and number of events on “lifeline” | 50 | −0.152 | −1.068 | 0.291 |
| Expression IL1 β and indicator | 50 | −0.050 | −0.347 | 0.730 |
| IL 6 and HDRS score | 48 | −0.136 | −0.930 | 0.357 |
| IL 6 and total score episodic memory | 50 | 0.047 | 0.323 | 0.748 |
| IL 6 and years of psychiatric treatment | 45 | 0.225 | 1.516 | 0.137 |
| IL 6 and number of events on “lifeline” | 50 | −0.111 | −0.774 | 0.443 |
| IL 6 and indicator | 50 | −0.021 | −0.148 | 0.883 |
| Expression IL6 and HDRS score | 48 | −0.244 | −1.708 | 0.094 |
| Expression IL6 and total score episodic memory | 50 | −0.097 | −0.672 | 0.505 |
| Expression IL6 and years of psychiatric treatment | 45 | 0.029 | 0.191 | 0.849 |
| Expression IL6 and number of events on “lifeline” | 50 | 0.013 | 0.088 | 0.931 |
| Expression IL6 and indicator | 50 | 0.099 | 0.691 | 0.493 |
| Healthy Control Group | Spearman’s Rank Order Correlation MD Removed in Pairs The Marked Correlation Coefficients Are Significant p < 0.05000 | |||
|---|---|---|---|---|
| N | R | t-Student Test | p | |
| IL 1 β (pg/mL) and total score episodic memory | 30 | −0.079 | −0.421 | 0.677 |
| IL 1 β (pg/mL) and number of events on “lifeline” | 30 | −0.062 | −0.326 | 0.747 |
| IL 1 β (pg/mL) and indicator | 30 | −0.002 | −0.009 | 0.993 |
| Expression IL1 β and total score episodic memory | 30 | 0.276 | 1.521 | 0.139 |
| Expression IL1 β and number of events on “lifeline” | 30 | 0.051 | 0.268 | 0.791 |
| Expression IL1 β and indicator | 30 | 0.238 | 1.294 | 0.206 |
| IL 6 and total score episodic memory | 30 | −0.104 | −0.554 | 0.584 |
| IL 6 and number of events on “lifeline” | 30 | −0.457 | −2.718 | 0.011 |
| IL 6 and indicator | 30 | −0.360 | −2.045 | 0.050 |
| Expression IL6 and total score episodic memory | 30 | −0.129 | −0.686 | 0.498 |
| Expression IL6 and n number of events on “lifeline” | 30 | 0.112 | 0.594 | 0.557 |
| Expression IL6 and indicator | 30 | 0.047 | 0.251 | 0.803 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wachowska, K.; Szemraj, J.; Śmigielski, J.; Gałecki, P. Inflammatory Markers and Episodic Memory Functioning in Depressive Disorders. J. Clin. Med. 2022, 11, 693. https://doi.org/10.3390/jcm11030693
Wachowska K, Szemraj J, Śmigielski J, Gałecki P. Inflammatory Markers and Episodic Memory Functioning in Depressive Disorders. Journal of Clinical Medicine. 2022; 11(3):693. https://doi.org/10.3390/jcm11030693
Chicago/Turabian StyleWachowska, Katarzyna, Janusz Szemraj, Janusz Śmigielski, and Piotr Gałecki. 2022. "Inflammatory Markers and Episodic Memory Functioning in Depressive Disorders" Journal of Clinical Medicine 11, no. 3: 693. https://doi.org/10.3390/jcm11030693
APA StyleWachowska, K., Szemraj, J., Śmigielski, J., & Gałecki, P. (2022). Inflammatory Markers and Episodic Memory Functioning in Depressive Disorders. Journal of Clinical Medicine, 11(3), 693. https://doi.org/10.3390/jcm11030693