
Effectiveness of Lifestyle Modification vs. Therapeutic, Preventative Strategies for Reducing Cardiovascular Risk in Primary Prevention—A Cohort Study

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
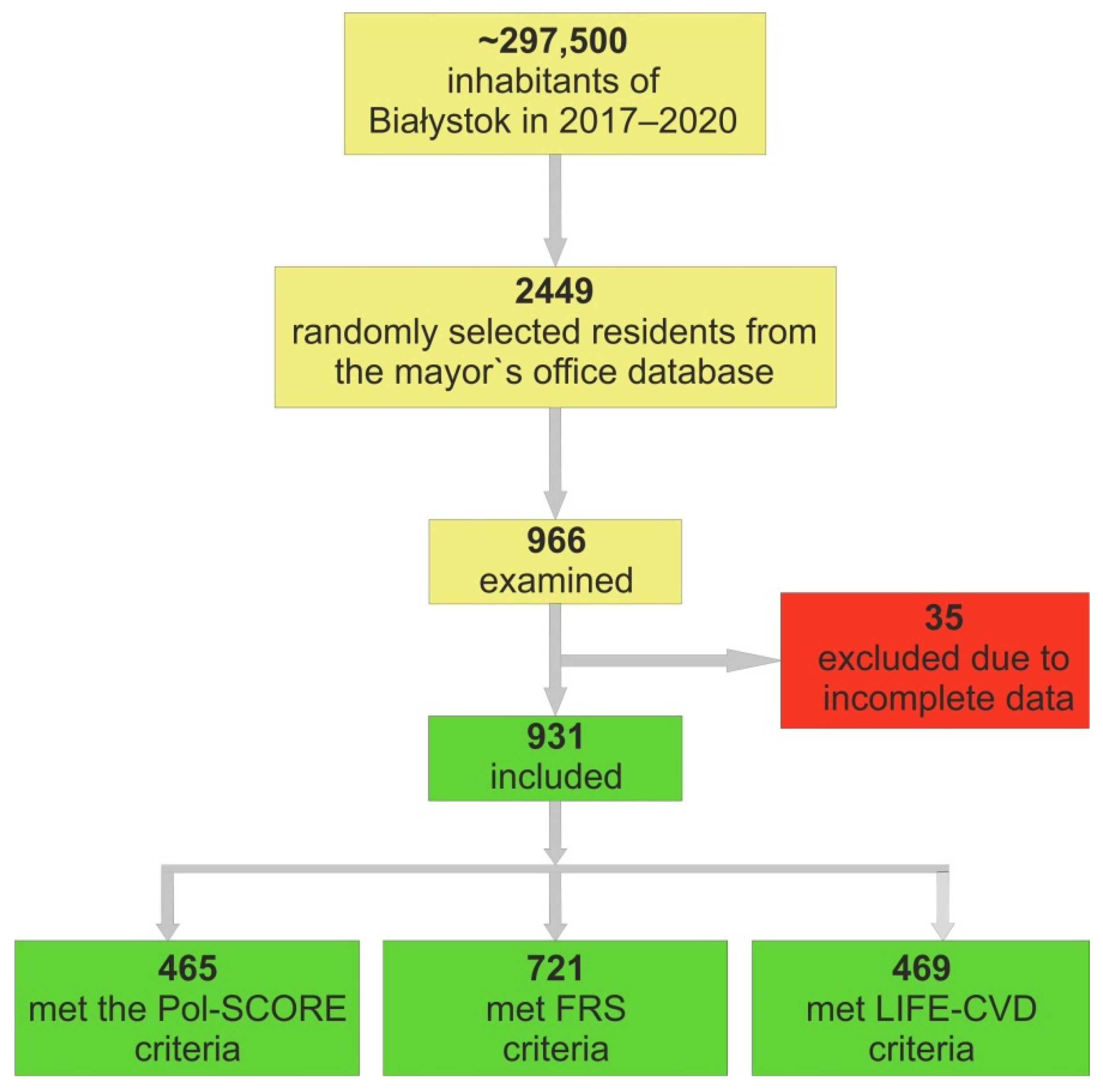
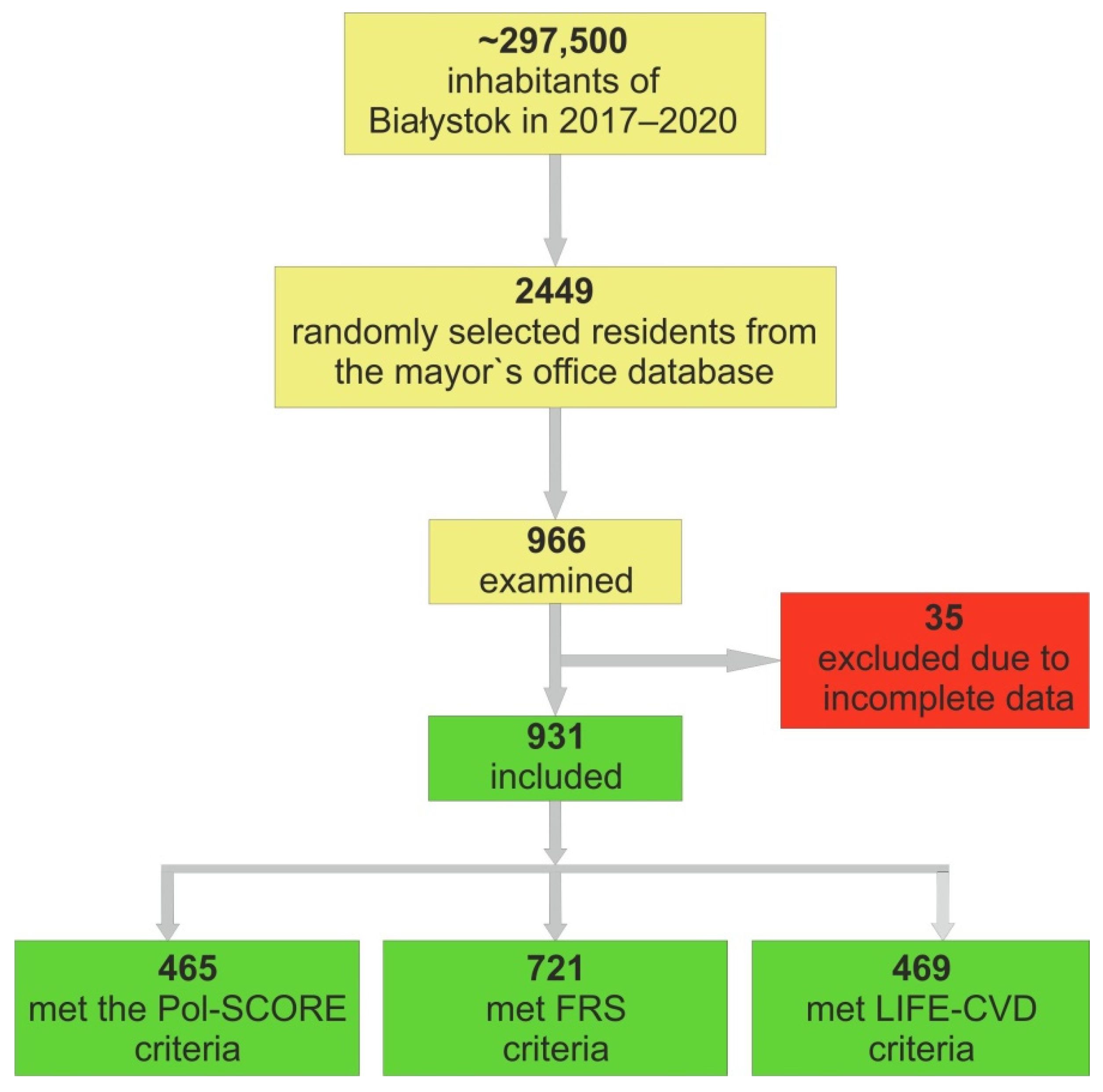
2.1. Recruitment of Bialystok PLUS Study Participants
2.2. Data Collection
2.3. Ethical Issues
2.4. Division into CV Risk Classes
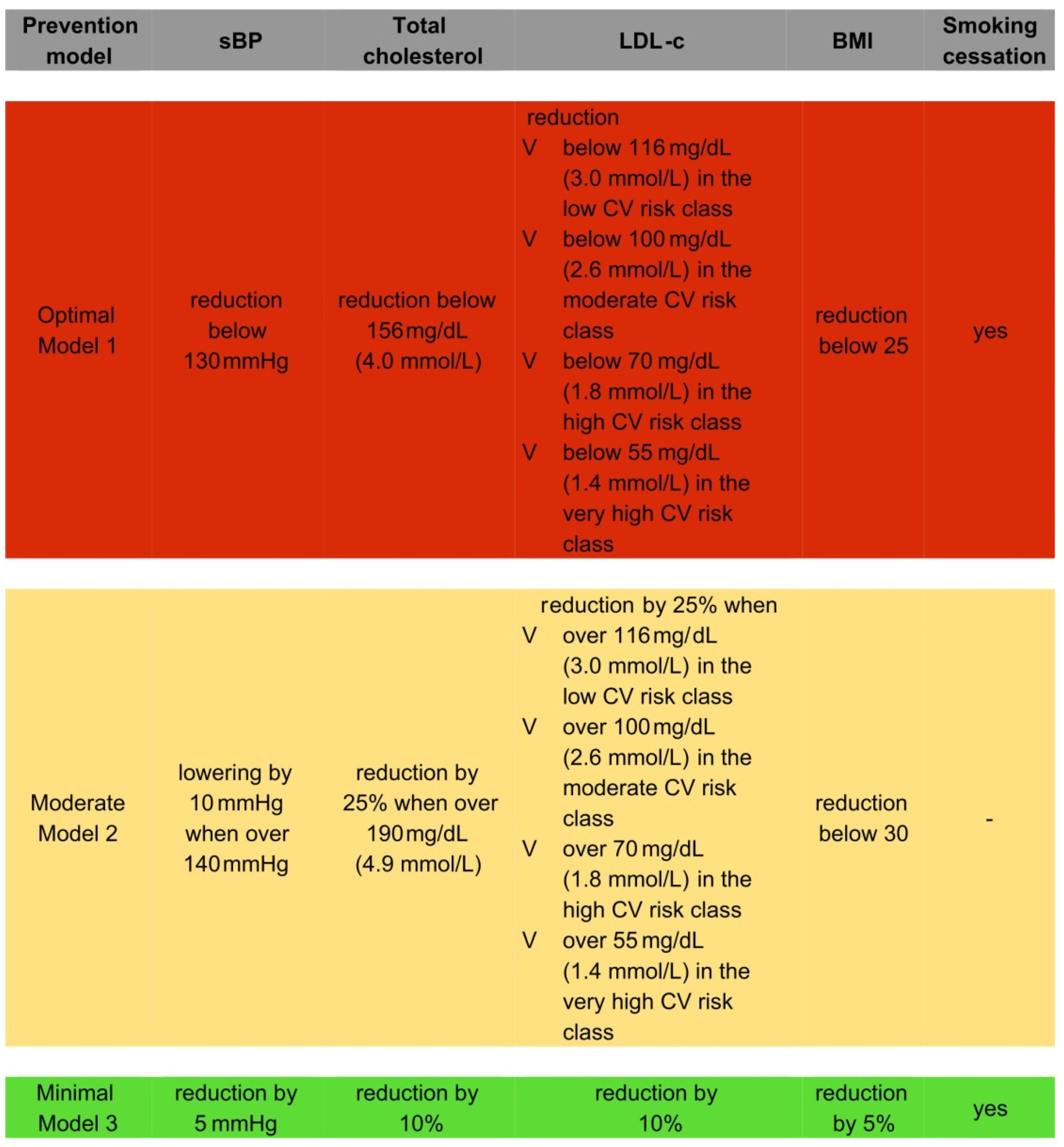
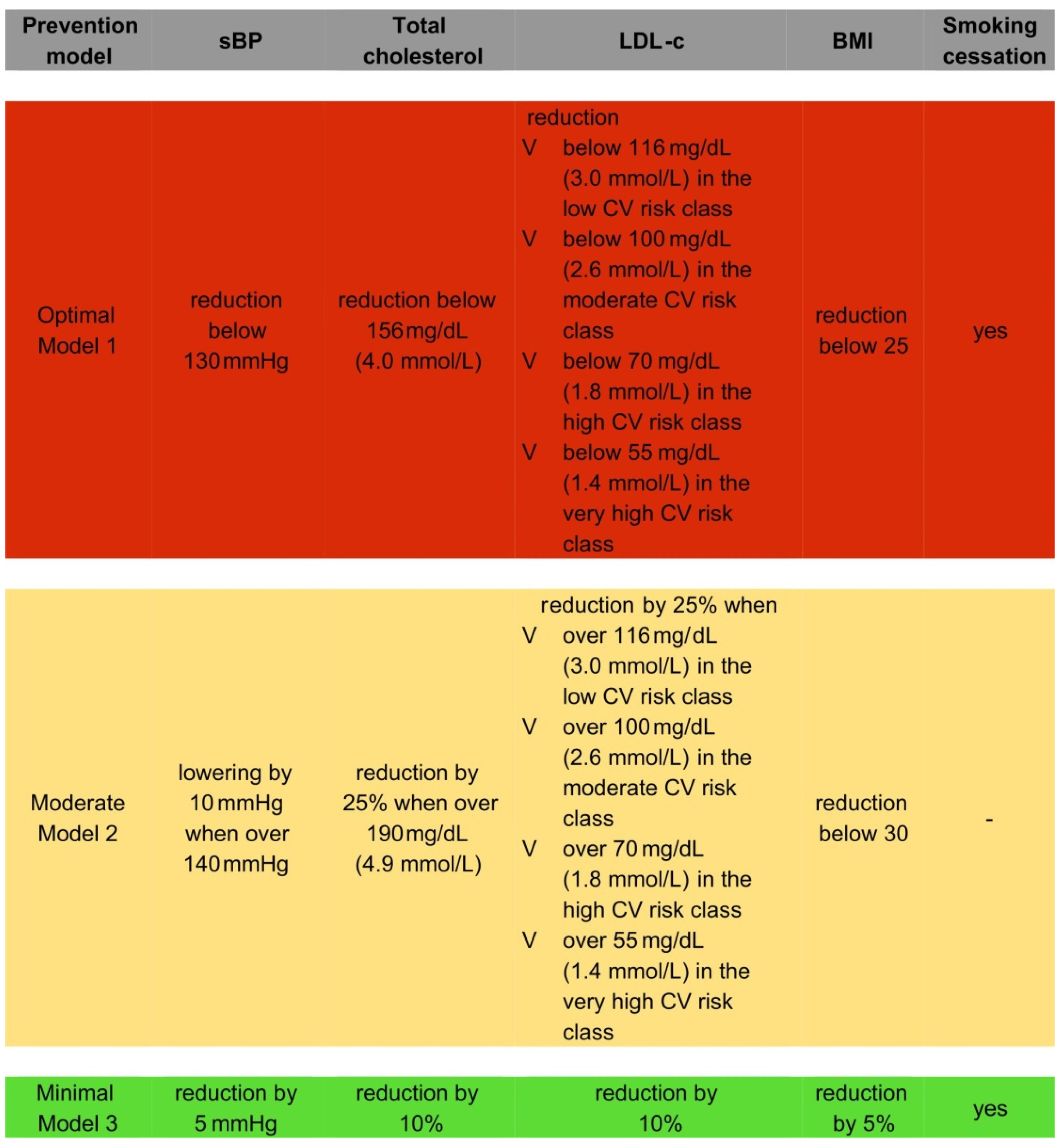
2.5. Designed Prevention Models
2.6. Calculators for the Assessment of CV Risk in Primary Prevention
2.7. The Estimation of the Number of the Local Inhabitants
2.8. Statistical Analysis
3. Results
4. Discussion
4.1. Prevention Strategies
4.2. Estimating the Effects of Preventative Models
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Townsend, N.; Nichols, M.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe 2015: Epidemiological update. Eur. Heart J. 2015, 36, 2673–2674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Ryden, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Primary prevention efforts are poorly developed in people at high cardiovascular risk: A report from the European Society of Cardiology EURObservational Research Programme EUROASPIRE V survey in 16 European countries. Eur. J. Prev. Cardiol. 2021, 28, 370–379. [Google Scholar] [CrossRef]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Ryden, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef]
- Jankowski, P.; Kosior, D.A.; Sowa, P.; Szostak-Janiak, K.; Koziel, P.; Krzykwa, A.; Sawicka, E.; Haberka, M.; Setny, M.; Kaminski, K.; et al. Secondary prevention of coronary artery disease in Poland. Results from the POLASPIRE survey. Cardiol. J. 2020, 27, 533–540. [Google Scholar] [CrossRef]
- Chlabicz, M.; Jamiolkowski, J.; Paniczko, M.; Sowa, P.; Szpakowicz, M.; Lapinska, M.; Jurczuk, N.; Kondraciuk, M.; Ptaszynska-Kopczynska, K.; Raczkowski, A.; et al. ECG Indices Poorly Predict Left Ventricular Hypertrophy and Are Applicable Only in Individuals with Low Cardiovascular Risk. J. Clin. Med. 2020, 9, 1364. [Google Scholar] [CrossRef]
- Chlabicz, M.; Jamiolkowski, J.; Laguna, W.; Sowa, P.; Paniczko, M.; Lapinska, M.; Szpakowicz, M.; Drobek, N.; Raczkowski, A.; Kaminski, K.A. A Similar Lifetime CV Risk and a Similar Cardiometabolic Profile in the Moderate and High Cardiovascular Risk Populations: A Population-Based Study. J. Clin. Med. 2021, 10, 1584. [Google Scholar] [CrossRef]
- Zdrojewski, T.; Jankowski, P.; Bandosz, P.; Bartus, S.; Chwojnicki, K.; Drygas, W.; Gaciong, Z.; Hoffman, P.; Kalarus, Z.; Kazmierczak, J.; et al. A new version of cardiovascular risk assessment system and risk charts calibrated for Polish population. Kardiol. Pol. 2015, 73, 958–961. [Google Scholar] [CrossRef] [Green Version]
- Conroy, R.M.; Pyorala, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetiere, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- D’Agostino, R.B.S.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaspers, N.E.M.; Blaha, M.J.; Matsushita, K.; van der Schouw, Y.T.; Wareham, N.J.; Khaw, K.T.; Geisel, M.H.; Lehmann, N.; Erbel, R.; Jockel, K.H.; et al. Prediction of individualized lifetime benefit from cholesterol lowering, blood pressure lowering, antithrombotic therapy, and smoking cessation in apparently healthy people. Eur. Heart J. 2020, 41, 1190–1199. [Google Scholar] [CrossRef]
- Jaspers, N.E.M.; Ridker, P.M.; Dorresteijn, J.A.N.; Visseren, F.L.J. The prediction of therapy-benefit for individual cardiovascular disease prevention: Rationale, implications, and implementation. Curr. Opin. Lipidol. 2018, 29, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Kuzma, L.; Struniawski, K.; Pogorzelski, S.; Bachorzewska-Gajewska, H.; Dobrzycki, S. Gender Differences in Association between Air Pollution and Daily Mortality in the Capital of the Green Lungs of Poland-Population-Based Study with 2,953,000 Person-Years of Follow-Up. J. Clin. Med. 2020, 9, 2351. [Google Scholar] [CrossRef] [PubMed]
- Gierlotka, M.; Zdrojewski, T.; Wojtyniak, B.; Polonski, L.; Stokwiszewski, J.; Gasior, M.; Kozierkiewicz, A.; Kalarus, Z.; Wierucki, L.; Chlebus, K.; et al. Incidence, treatment, in-hospital mortality and one-year outcomes of acute myocardial infarction in Poland in 2009–2012--nationwide AMI-PL database. Kardiol. Pol. 2015, 73, 142–158. [Google Scholar] [CrossRef] [PubMed]
- Ptaszynska-Kopczynska, K.; Sobolewska, D.; Kozuch, M.; Dobrzycki, S.; Sobkowicz, B.; Hirnle, T.; Musial, W.J.; Kaminski, K.A. Efficacy of invasive treatment and the occurrence of cardiac rupture in acute ST-elevation myocardial infarction. Kardiol. Pol. 2011, 69, 795–800. [Google Scholar]
- Kubica, J.; Adamski, P.; Paciorek, P.; Ladny, J.R.; Kalarus, Z.; Banasiak, W.; Kochman, W.; Goracy, J.; Wozakowska-Kaplon, B.; Navarese, E.P.; et al. Treatment of patients with acute coronary syndrome: Recommendations for medical emergency teams: Focus on antiplatelet therapies. Updated experts’ standpoint. Cardiol. J. 2018, 25, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Niklas, A.; Marcinkowska, J.; Kozela, M.; Pajak, A.; Zdrojewski, T.; Drygas, W.; Piwonska, A.; Kwasniewska, M.; Kozakiewicz, K.; Tykarski, A. Blood pressure and cholesterol control in patients with hypertension and hypercholesterolemia: The results from the Polish multicenter national health survey WOBASZ II. Pol. Arch. Intern. Med. 2019, 129, 864–873. [Google Scholar] [CrossRef] [Green Version]
- Nawrocki, J.W.; Weiss, S.R.; Davidson, M.H.; Sprecher, D.L.; Schwartz, S.L.; Lupien, P.J.; Jones, P.H.; Haber, H.E.; Black, D.M. Reduction of LDL cholesterol by 25% to 60% in patients with primary hypercholesterolemia by atorvastatin, a new HMG-CoA reductase inhibitor. Arterioscler. Thromb. Vasc. Biol. 1995, 15, 678–682. [Google Scholar] [CrossRef]
- Materson, B.J.; Reda, D.J.; Cushman, W.C.; Massie, B.M.; Freis, E.D.; Kochar, M.S.; Hamburger, R.J.; Fye, C.; Lakshman, R.; Gottdiener, J.; et al. Single-drug therapy for hypertension in men. A comparison of six antihypertensive agents with placebo. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. N. Engl. J. Med. 1993, 328, 914–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niklas, A.; Flotynska, A.; Puch-Walczak, A.; Polakowska, M.; Topor-Madry, R.; Polak, M.; Piotrowski, W.; Kwasniewska, M.; Nadrowski, P.; Pajak, A.; et al. Prevalence, awareness, treatment and control of hypertension in the adult Polish population-Multi-center National Population Health Examination Surveys-WOBASZ studies. Arch. Med. Sci. 2018, 14, 951–961. [Google Scholar] [CrossRef]
- Elliott, P.; Stamler, J.; Nichols, R.; Dyer, A.R.; Stamler, R.; Kesteloot, H.; Marmot, M. Intersalt revisited: Further analyses of 24 hour sodium excretion and blood pressure within and across populations. Intersalt Cooperative Research Group. BMJ 1996, 312, 1249–1253. [Google Scholar] [CrossRef] [PubMed]
- Dattilo, A.M.; Kris-Etherton, P.M. Effects of weight reduction on blood lipids and lipoproteins: A meta-analysis. Am. J. Clin. Nutr. 1992, 56, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Zomer, E.; Gurusamy, K.; Leach, R.; Trimmer, C.; Lobstein, T.; Morris, S.; James, W.P.; Finer, N. Interventions that cause weight loss and the impact on cardiovascular risk factors: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 1001–1011. [Google Scholar] [CrossRef]
- Domenech, M.; Roman, P.; Lapetra, J.; Garcia de la Corte, F.J.; Sala-Vila, A.; de la Torre, R.; Corella, D.; Salas-Salvado, J.; Ruiz-Gutierrez, V.; Lamuela-Raventos, R.M.; et al. Mediterranean diet reduces 24-hour ambulatory blood pressure, blood glucose, and lipids: One-year randomized, clinical trial. Hypertension 2014, 64, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Cornelissen, V.A.; Smart, N.A. Exercise training for blood pressure: A systematic review and meta-analysis. J. Am. Heart Assoc. 2013, 2, e004473. [Google Scholar] [CrossRef] [Green Version]
- Corso, L.M.; Macdonald, H.V.; Johnson, B.T.; Farinatti, P.; Livingston, J.; Zaleski, A.L.; Blanchard, A.; Pescatello, L.S. Is Concurrent Training Efficacious Antihypertensive Therapy? A Meta-analysis. Med. Sci. Sports Exerc. 2016, 48, 2398–2406. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S. Impact of progressive resistance training on lipids and lipoproteins in adults: Another look at a meta-analysis using prediction intervals. Prev. Med. 2009, 49, 473–475. [Google Scholar] [CrossRef]
- Ferket, B.S.; van Kempen, B.J.; Heeringa, J.; Spronk, S.; Fleischmann, K.E.; Nijhuis, R.L.; Hofman, A.; Steyerberg, E.W.; Hunink, M.G. Personalized prediction of lifetime benefits with statin therapy for asymptomatic individuals: A modeling study. PLoS Med. 2012, 9, e1001361. [Google Scholar] [CrossRef] [Green Version]
- Ma, M.; Dollar, K.M.; Kibler, J.L.; Sarpong, D.; Samuels, D. The effects of priming on a public health campaign targeting cardiovascular risks. Prev. Sci. 2011, 12, 333–338. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | Total Population n = 931 |
|---|---|
| Age, years | 49.1 ± 15.5 |
| Male sex, n | 402 (43.2) |
| BPs, mmHg | 124.4 ± 17.7 |
| BPd, mmHg | 81.7 ± 10.1 |
| BP ≥ 140 and/or ≥90 mmHg | 253 (27.2) |
| HR, bpm | 72.3 ± 10.9 |
| Fasting glucose, mg/dL | 102.1 ± 21.0 |
| OGTT 120 min glucose, mg/dL | 124.3 ± 39.7 |
| HbA1c, % | 5.5 ± 0.7 |
| TC, mg/dL | 192.5 ± 40.8 |
| LDL-C, mg/dL | 124.4 ± 37.8 |
| HDL-C, mg/dL | 62.6 ± 17.3 |
| TG, mg/dL | 113.2 ± 77.6 |
| hs-CRP, mg/l | 1.7 ± 4.2 |
| Creatinine, μmol/L | 70.9 ± 14.9 |
| CrCl, mL/min | 115.0 ± 40.7 |
| LVEF Biplane, % | 58.5 ± 5.7 |
| BMI, kg/m2 | 26.8 ± 5.0 |
| BMI < 25 kg/m2 | 330 (35.4) |
| BMI 25–29.99 kg/m2 | 352 (37.8) |
| BMI ≥ 30 kg/m2 | 249 (26.7) |
| History of hypertension | 275 (29.6) |
| Undiagnosed hypertension * | 107 (11.5) |
| History of hypercholesterolemia | 290 (31.1) |
| Undiagnosed hypercholesterolemia ** | 399 (42.9) |
| History of diabetes | 71 (7.6) |
| Undiagnosed diabetes *** | 57 (6.1) |
| Currently smoking | 186 (20.1) |
| Prevention Strategy | Scales | CV Risk Classes | n | Average Risk (%) Mean (95% CI) |
|---|---|---|---|---|
| Baseline | Pol-SCORE | Low | 126 | 0.51 (0.47–0.55) |
| Moderate | 201 | 2.50 (2.35–2.65) | ||
| High | 90 | 6.10 (5.62–6.58) | ||
| Very high | 48 | 15.29 (13.60–16.98) | ||
| Total | 465 | 3.98 (3.54–4.42) | ||
| FRS—Lipids | Low | 319 | 2.40 (2.22–2.58) | |
| Moderate | 205 | 8.55 (7.94–9.16) | ||
| High | 113 | 13.18 (12.08–14.28) | ||
| Very high | 84 | 24.53 (23.10–25.96) | ||
| Total | 721 | 8.42 (7.82–9.02) | ||
| FRS—BMI | Low | 319 | 3.15 (2.91–3.39) | |
| Moderate | 205 | 11.84 (11.02–12.66) | ||
| High | 113 | 17.59 (16.06–19.12) | ||
| Very high | 84 | 27.54 (26.55–28.53) | ||
| Total | 721 | 10.73 (10.03–11.43) | ||
| LIFE-CVD 10-year risk | Low | 70 | 1.32 (1.16–1.48) | |
| Moderate | 182 | 3.24 (3.04–3.44) | ||
| High | 114 | 4.98 (4.68–5.29) | ||
| Very high | 103 | 10.09 (9.17–11.01) | ||
| Total | 469 | 4.88 (4.53–5.24) | ||
| LIFE-CVD lifetime risk | Low | 70 | 11.46 (10.66–12.27) | |
| Moderate | 182 | 16.42 (15.45–17.39) | ||
| High | 114 | 17.76 (16.22–19.30) | ||
| Very high | 103 | 22.37 (20.40–24.34) | ||
| Total | 469 | 17.31 (16.56–18.07) |
| Prevention Strategy | Scales | CV Risk Classes | n | Average Risk (%) Mean (95% CI) | The Absolute Value of the Reduction from Baseline Risk (%) Mean (95% CI) |
|---|---|---|---|---|---|
| Model 1 Optimal | Pol-SCORE | Low | 126 | 0.37 (0.34–0.40) | −0.14 (0.12–0.16) |
| Moderate | 201 | 1.69 (1.57–1.81) | −0.81 (0.71–0.91) | ||
| High | 90 | 3.71 (3.30–4.12) | −2.40 (2.07–2.73) | ||
| Very high | 48 | 6.66 (5.94–7.38) | −8.63 (7.16–10.10) | ||
| Total | 465 | 2.24 (2.03–2.45) | −1.74 (1.46–2.02) | ||
| FRS—Lipids | Low | 319 | 1.59 (1.49–1.69) | −0.82 (0.71–0.93) | |
| Moderate | 205 | 5.42 (5.03–5.81) | −3.13 (2.76–3.50) | ||
| High | 113 | 7.67 (6.86–8.48) | −5.51 (4.81–6.21) | ||
| Very high | 84 | 14.55 (13.03–16.07) | −9.98 (8.73–11.23) | ||
| Total | 721 | 5.14 (4.75–5.53) | −3.28 (2.97–3.59) | ||
| FRS—BMI | Low | 319 | 2.47 (2.32–2.62) | −0.69 (0.55–0.83) | |
| Moderate | 205 | 9.03 (8.43–9.63) | −2.81 (2.33–3.29) | ||
| High | 113 | 13.17 (11.90–14.44) | −4.43 (3.64–5.22) | ||
| Very high | 84 | 22.23 (20.72–23.74) | −5.31 (4.15–6.47) | ||
| Total | 721 | 8.31 (7.74–8.88) | −2.42 (2.15–2.69) | ||
| LIFE-CVD 10-year risk | Low | 70 | 1.08 (0.95–1.21) | −0.23 (0.17–0.30) | |
| Moderate | 182 | 2.28 (2.13–2.43) | −0.96 (0.85–1.07) | ||
| High | 114 | 2.69 (2.45–2.93) | −2.29 (2.05–2.53) | ||
| Very high | 103 | 3.77 (3.43–4.10) | −6.32 (5.49–7.15) | ||
| Total | 469 | 2.53 (2.39–2.66) | −2.35 (2.07–2.63) | ||
| LIFE-CVD lifetime risk | Low | 70 | 9.71 (9.06–10.35) | −1.76 (1.34–2.17) | |
| Moderate | 182 | 11.82 (11.18–12.46) | −4.60 (4.04–5.16) | ||
| High | 114 | 9.25 (8.66–9.84) | −8.51 (7.25–9.76) | ||
| Very-high | 103 | 8.67 (8.03–9.32) | −13.70 (11.93–15.46) | ||
| Total | 469 | 10.19 (9.83–10.54) | −7.12 (6.47–7.78) | ||
| Model 2 Moderate | Pol-SCORE | Low | 126 | 0.44 (0.40–0.48) | −0.07 (0.06–0.08) |
| Moderate | 201 | 2.12 (1.98–2.26) | −0.38 (0.33–0.43) | ||
| High | 90 | 4.85 (4.42–5.28) | −1.26 (1.07–1.45) | ||
| Very high | 48 | 11.16 (9.91–12.41) | −4.13 (3.46–4.80) | ||
| Total | 465 | 3.13 (2.80–3.46) | −0.85 (0.72–0.98) | ||
| FRS—Lipids | Low | 319 | 2.01 (1.87–2.15) | −0.40 (0.34–0.46) | |
| Moderate | 205 | 6.98 (6.46–7.50) | −1.57 (1.34–1.80) | ||
| High | 113 | 10.24 (9.33–11.15) | −2.94 (2.52–3.36) | ||
| Very high | 84 | 20.57 (18.99–22.15) | −3.96 (3.27–4.65) | ||
| Total | 721 | 6.88 (6.37–7.39) | −1.54 (1.38–1.70) | ||
| FRS—BMI | Low | 319 | 3.07 (2.85–3.29) | −0.08 (0.05–0.11) | |
| Moderate | 205 | 11.30 (10.53–12.07) | −0.54 (0.38–0.70) | ||
| High | 113 | 16.66 (15.21–18.11) | −0.93 (0.68–1.18) | ||
| Very high | 84 | 26.83 (25.74–27.92) | −0.71 (0.40–1.02) | ||
| Total | 721 | 10.31 (9.64–10.98) | −0.42 (0.35–0.49) | ||
| LIFE-CVD 10-year risk | Low | 70 | 1.11 (0.99–1.24) | −0.20 (0.16–0.25) | |
| Moderate | 182 | 2.66 (2.48–2.83) | −0.58 (0.52–0.65) | ||
| High | 114 | 3.82 (3.56–4.08) | −1.16 (1.05–1.28) | ||
| Very high | 103 | 7.18 (6.57–7.79) | −2.91 (2.54–3.27) | ||
| Total | 469 | 3.70 (3.46–3.95) | −1.18 (1.05–1.30) | ||
| LIFE-CVD lifetime risk | Low | 70 | 9.83 (9.21–10.45) | −1.63 (1.31–1.95) | |
| Moderate | 182 | 13.50 (12.77–14.23) | −2.92 (2.59–3.26) | ||
| High | 114 | 13.48 (12.51–14.46) | −4.27 (3.64–4.90) | ||
| Very high | 103 | 16.28 (14.98–17.58) | −6.09 (5.32–6.86) | ||
| Total | 469 | 13.56 (13.05–14.06) | −3.75 (3.46–4.05) | ||
| Model 3 Minimal | Pol-SCORE | Low | 126 | 0.38 (0.35–0.41) | −0.13 (0.11–0.15) |
| Moderate | 201 | 1.87 (1.74–2.00) | −0.63 (0.55–0.71) | ||
| High | 90 | 4.60 (4.17–5.03) | −1.50 (1.25–1.75) | ||
| Very high | 48 | 10.28 (9.20–11.36) | −5.01 (3.71–6.31) | ||
| Total | 465 | 2.87 (2.57–3.17) | −1.11 (0.92–1.30) | ||
| FRS—Lipids | Low | 319 | 1.69 (1.56–1.82) | −0.71 (0.62–0.80) | |
| Moderate | 205 | 6.29 (5.82–6.76) | −2.26 (1.98–2.54) | ||
| High | 113 | 9.84 (8.91–10.77) | −3.34 (2.86–3.82) | ||
| Very high | 84 | 19.71 (18.09–21.33) | −4.82 (3.83–5.81) | ||
| Total | 721 | 6.38 (5.88–6.88) | −2.04 (1.85–2.23) | ||
| FRS—BMI | Low | 319 | 2.43 (2.26–2.60) | −0.72 (0.60–0.84) | |
| Moderate | 205 | 9.51 (8.81–10.21) | −2.33 (1.93–2.73) | ||
| High | 113 | 14.70 (13.23–16.17) | −2.89 (2.25–3.53) | ||
| Very high | 84 | 24.89 (23.54–26.24) | −2.64 (1.74–3.54) | ||
| Total | 721 | 8.98 (8.34–9.62) | −1.74 (1.54–1.94) | ||
| LIFE-CVD 10-year risk | Low | 70 | 1.03 (0.90–1.15) | −0.29 (0.24–0.35) | |
| Moderate | 182 | 2.48 (2.32–2.64) | −0.76 (0.68–0.85) | ||
| High | 114 | 3.81 (3.56–4.06) | −1.17 (1.02–1.33) | ||
| Very high | 103 | 7.64 (6.82–8.46) | −2.45 (2.15–2.75) | ||
| Total | 469 | 3.71 (3.42–3.99) | −1.16 (1.05–1.26) | ||
| LIFE-CVD lifetime risk | Low | 70 | 9.26 (8.54–9.97) | −2.21 (1.96–2.45) | |
| Moderate | 182 | 13.19 (12.33–14.06) | −3.23 (2.98–3.47) | ||
| High | 114 | 14.12 (12.81–15.43) | −3.64 (3.20–4.07) | ||
| Very high | 103 | 17.65 (15.91–19.40) | −4.72 (4.17–5.26) | ||
| Total | 469 | 13.79 (13.14–14.44) | −3.49 (3.29–3.69) |
| Prevention Strategy | CV Risk Classes | n | Probability of Survival Free of Heart Attack or Stroke—Increase in Life Years in Relation to the Baseline Mean (95% CI) |
|---|---|---|---|
| Model 1 Optimal | Low | 70 | 0.97 (0.68–1.27) |
| Moderate | 182 | 1.58 (1.38–1.77) | |
| High | 114 | 2.40 (2.06–2.73) | |
| Very high | 103 | 3.06 (2.66–3.46) | |
| Total | 469 | 2.01 (1.85–2.17) | |
| Model 2 Moderate | Low | 70 | 0.59 (0.47–0.72) |
| Moderate | 182 | 0.71 (0.63–0.79) | |
| High | 114 | 0.95 (0.81–1.10) | |
| Very high | 103 | 1.08 (0.92–1.25) | |
| Total | 469 | 0.83 (0.77–0.90) | |
| Model 3 Minimal | Low | 70 | 1.06 (0.80–1.32) |
| Moderate | 182 | 1.17 (1.01–1.34) | |
| High | 114 | 1.21 (0.98–1.45) | |
| Very high | 103 | 1.37 (1.12–1.63) | |
| Total | 469 | 1.21 (1.10–1.32) |
| SCORES | Baseline | Model 1 | Model 2 | Model 3 | |
|---|---|---|---|---|---|
| Pol-SCORE | Deceased | 3963 | 2177 | 3095 | 2815 |
| Survivors | - | 1786 | 868 | 1148 | |
| FRS—Lipids | First CVD event within 10 years | 13,148 | 7987 | 10,734 | 9880 |
| Stay free of developing the first CVD event within 10 years | - | 5161 | 2414 | 3268 | |
| FRS—BMI | First CVD event within 10 years | 16,727 | 12,835 | 16,069 | 13,927 |
| Stay free of developing the first CVD event within 10 years | - | 3892 | 658 | 2800 | |
| LIFE-CVD 10-year risk | First MI, stroke, or CV death within 10 years | 4934 | 2534 | 3738 | 3748 |
| Stay free of developing the first CVD event within 10 years | - | 2400 | 1196 | 1186 | |
| LIFE-CVD lifetime risk | First MI, stroke, or CV death within lifetime | 17,461 | 10,186 | 13,640 | 13,899 |
| Stay free of developing the first CVD event within lifetime | - | 7275 | 3821 | 3562 |
| Variable | Total Population | Cardiovascular Risk Class | |||
|---|---|---|---|---|---|
| Low | Moderate | High | Very High | ||
| Local population | 204,511 | 98,378 | 44,434 | 26,476 | 35,223 |
| History of hypertension | 58,283 | 7173 | 15,995 | 12,394 | 22,721 |
| Uncontrolled BP in patients diagnosed with hypertension * | 41,934 | 4767 | 11,286 | 8644 | 17,237 |
| Undiagnosed hypertension | 77,746 | 40,470 | 19,782 | 8409 | 9085 |
| History of hypercholesterolemia | 60,829 | 12,521 | 20,005 | 11,669 | 16,634 |
| Uncontrolled lipid profile in patients with diagnosed hypercholesterolemia ** | 53,370 | 10,504 | 15,674 | 10,996 | 16,196 |
| Undiagnosed hypercholesterolemia *** | 91,293 | 36,790 | 22,168 | 14,175 | 18,160 |
| History of diabetes | 15,220 | 512 | 3720 | 2930 | 8058 |
| Uncontrolled glucose in patients diagnosed with diabetes **** | 4493 | 256 | 457 | 1119 | 2661 |
| Undiagnosed diabetes ***** | 522 | 0 | 257 | 265 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chlabicz, M.; Jamiołkowski, J.; Łaguna, W.; Dubatówka, M.; Sowa, P.; Łapińska, M.; Szpakowicz, A.; Zieleniewska, N.; Zalewska, M.; Raczkowski, A.; et al. Effectiveness of Lifestyle Modification vs. Therapeutic, Preventative Strategies for Reducing Cardiovascular Risk in Primary Prevention—A Cohort Study. J. Clin. Med. 2022, 11, 688. https://doi.org/10.3390/jcm11030688
Chlabicz M, Jamiołkowski J, Łaguna W, Dubatówka M, Sowa P, Łapińska M, Szpakowicz A, Zieleniewska N, Zalewska M, Raczkowski A, et al. Effectiveness of Lifestyle Modification vs. Therapeutic, Preventative Strategies for Reducing Cardiovascular Risk in Primary Prevention—A Cohort Study. Journal of Clinical Medicine. 2022; 11(3):688. https://doi.org/10.3390/jcm11030688
Chicago/Turabian StyleChlabicz, Małgorzata, Jacek Jamiołkowski, Wojciech Łaguna, Marlena Dubatówka, Paweł Sowa, Magda Łapińska, Anna Szpakowicz, Natalia Zieleniewska, Magdalena Zalewska, Andrzej Raczkowski, and et al. 2022. "Effectiveness of Lifestyle Modification vs. Therapeutic, Preventative Strategies for Reducing Cardiovascular Risk in Primary Prevention—A Cohort Study" Journal of Clinical Medicine 11, no. 3: 688. https://doi.org/10.3390/jcm11030688
APA StyleChlabicz, M., Jamiołkowski, J., Łaguna, W., Dubatówka, M., Sowa, P., Łapińska, M., Szpakowicz, A., Zieleniewska, N., Zalewska, M., Raczkowski, A., & Kamiński, K. A. (2022). Effectiveness of Lifestyle Modification vs. Therapeutic, Preventative Strategies for Reducing Cardiovascular Risk in Primary Prevention—A Cohort Study. Journal of Clinical Medicine, 11(3), 688. https://doi.org/10.3390/jcm11030688