
Differences in Subjective and Objective Cognitive Decline Outcomes Are Associated with Modifiable Protective Factors: A 4-Year Longitudinal Study

 , , and
, , and
Abstract
1. Introduction
2. Methods
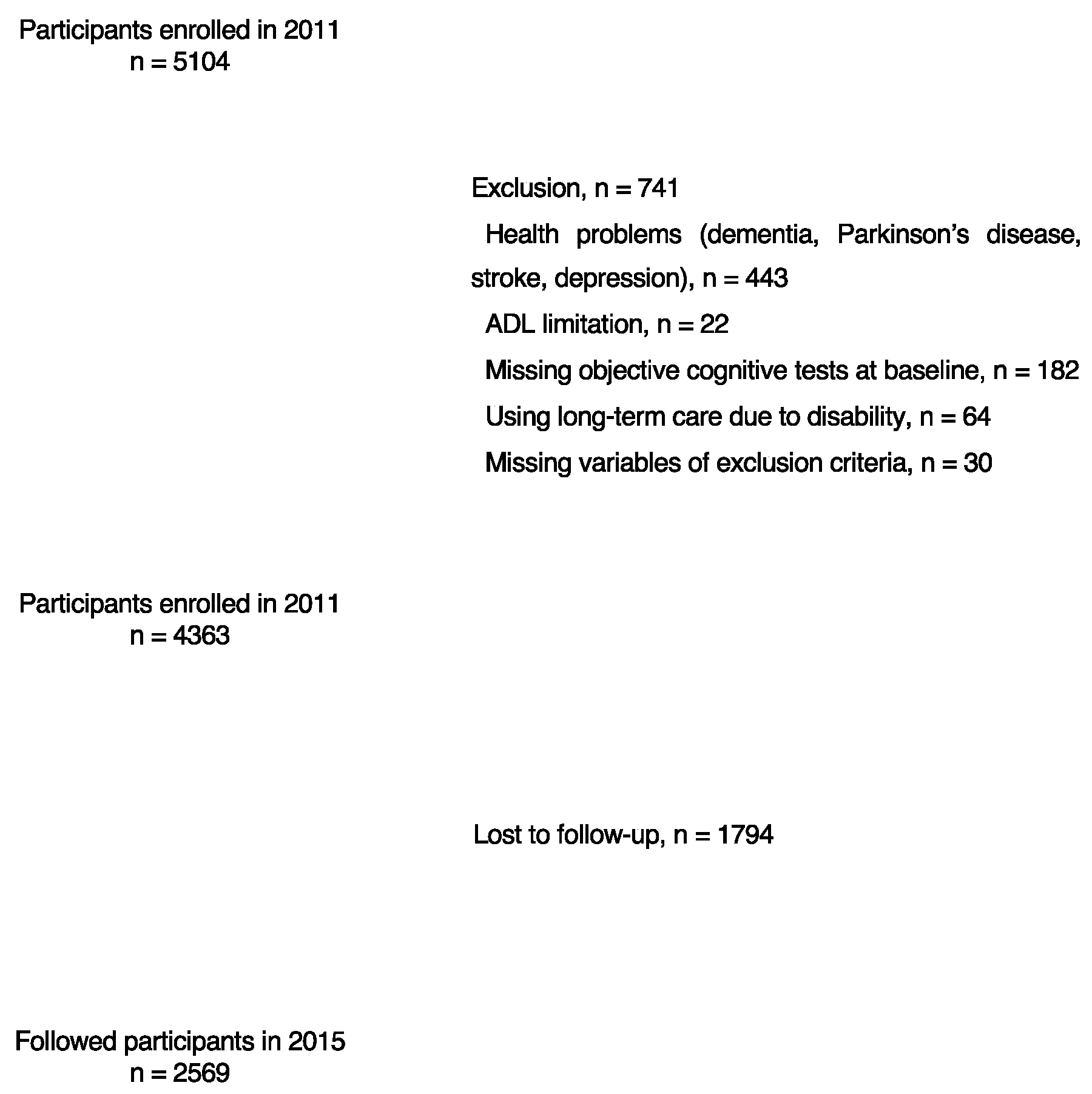
2.1. Study Sample and Design
2.2. Defining SCD and OCD
2.3. Protective and Risk Factors for Dementia
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jessen, F.; Amariglio, R.E.; Buckley, R.F.; van der Flier, W.M.; Han, Y.; Molinuevo, J.L.; Rabin, L.; Rentz, D.M.; Rodriguez-Gomez, O.; Saykin, A.J.; et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020, 19, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chetelat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Jessen, F.; Wiese, B.; Bachmann, C.; Eifflaender-Gorfer, S.; Haller, F.; Kölsch, H.; Luck, T.; Mösch, E.; van den Bussche, H.; Wagner, M.; et al. Prediction of dementia by subjective memory impairment: Effects of severity and temporal association with cognitive impairment. Arch. Gen. Psychiatry 2010, 67, 414–422. [Google Scholar] [CrossRef] [PubMed]
- van Harten, A.C.; Mielke, M.M.; Swenson-Dravis, D.M.; Hagen, C.E.; Edwards, K.K.; Roberts, R.O.; Geda, Y.E.; Knopman, D.S.; Petersen, R.C. Subjective cognitive decline and risk of MCI: The Mayo Clinic Study of Aging. Neurology 2018, 91, e300–e312. [Google Scholar] [CrossRef] [PubMed]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R., Jr.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Van Harten, A.C.; Smits, L.L.; Teunissen, C.E.; Visser, P.J.; Koene, T.; Blankenstein, M.A.; Scheltens, P.; van der Flier, W.M. Preclinical AD predicts decline in memory and executive functions in subjective complaints. Neurology 2013, 81, 1409–1416. [Google Scholar] [CrossRef]
- Wolfsgruber, S.; Polcher, A.; Koppara, A.; Kleineidam, L.; Froelich, L.; Peters, O.; Huell, M.; Ruether, E.; Wiltfang, J.; Maier, W. Cerebrospinal fluid biomarkers and clinical progression in patients with subjective cognitive decline and mild cognitive impairment. J. Alzheimer’s Dis. 2017, 58, 939–950. [Google Scholar] [CrossRef]
- Hessen, E.; Eckerström, M.; Nordlund, A.; Almdahl, I.S.; Stålhammar, J.; Bjerke, M.; Eckerström, C.; Göthlin, M.; Fladby, T.; Reinvang, I. Subjective cognitive impairment is a predominantly benign condition in memory clinic patients followed for 6 years: The Gothenburg-Oslo MCI Study. Dement. Geriatr. Cogn. Disord. Extra 2017, 7, 1–14. [Google Scholar] [CrossRef]
- Mondini, S.; Pucci, V.; Montemurro, S.; Rumiati, R.I. Protective factors for subjective cognitive decline individuals: Trajectories and changes in a longitudinal study with Italian elderly. Eur. J. Neurol. 2022, 29, 691–697. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Lee, S.; Doi, T.; Lee, S.; Tsutsumimoto, K.; Harada, K.; Hotta, R.; Bae, S.; Nakakubo, S.; et al. Impact of Cognitive Frailty on Daily Activities in Older Persons. J. Nutr. Health Aging 2016, 20, 729–735. [Google Scholar] [CrossRef]
- Jia, F.; Li, Y.; Li, M.; Cao, F. Subjective Cognitive Decline, Cognitive Reserve Indicators, and the Incidence of Dementia. J. Am. Med. Dir. Assoc. 2020, 22, 1449–1455. e4. [Google Scholar] [CrossRef] [PubMed]
- Jester, D.J.; Andel, R.; Cechova, K.; Laczo, J.; Lerch, O.; Markova, H.; Nikolai, T.; Vyhnalek, M.; Hort, J. Cognitive Phenotypes of Older Adults with Subjective Cognitive Decline and Amnestic Mild Cognitive Impairment: The Czech Brain Aging Study. J. Int. Neuropsychol. Soc. 2021, 27, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Shimada, H.; Park, H.; Doi, T.; Yoshida, D.; Uemura, K.; Tsutsumimoto, K.; Suzuki, T. Evaluation of multidimensional neurocognitive function using a tablet personal computer: Test-retest reliability and validity in community-dwelling older adults. Geriatr. Gerontol. Int. 2013, 13, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Park, H.; Doi, T.; Lee, S. Validity of the National Center for Geriatrics and Gerontology-Functional Assessment Tool and Mini-Mental State Examination for detecting the incidence of dementia in older Japanese adults. Geriatr. Gerontol. Int. 2017, 17, 2383–2388. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Ito, T.; Lee, S.; Park, H.; et al. Combined prevalence of frailty and mild cognitive impairment in a population of elderly Japanese people. J. Am. Med. Dir. Assoc. 2013, 14, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- O’Bryant, S.E.; Humphreys, J.D.; Smith, G.E.; Ivnik, R.J.; Graff-Radford, N.R.; Petersen, R.C.; Lucas, J.A. Detecting dementia with the mini-mental state examination in highly educated individuals. Arch. Neurol. 2008, 65, 963–967. [Google Scholar] [CrossRef]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Nunez, C.; Gallagher, D.; Visser, M.; Pi-Sunyer, F.X.; Wang, Z.; Heymsfield, S.B. Bioimpedance analysis: Evaluation of leg-to-leg system based on pressure contact footpad electrodes. Med. Sci. Sports Exerc. 1997, 29, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Katayama, O.; Lee, S.; Bae, S.; Makino, K.; Shinkai, Y.; Chiba, I.; Harada, K.; Shimada, H. Lifestyle Activity Patterns Related to Physical Frailty and Cognitive Impairment in Urban Community-Dwelling Older Adults in Japan. J. Am. Med. Dir. Assoc. 2020, 22, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Nakakubo, S.; Doi, T.; Tsutsumimoto, K.; Kurita, S.; Ishii, H.; Shimada, H. Sleep duration and progression to sarcopenia in Japanese community-dwelling older adults: A 4 year longitudinal study. J. Cachexia Sarcopenia Muscle 2021, 12, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A. Geriatric Depression Scale. Psychopharmacol. Bull 1988, 24, 709–711. [Google Scholar]
- Katayama, O.; Lee, S.; Bae, S.; Makino, K.; Shinkai, Y.; Chiba, I.; Harada, K.; Shimada, H. Modifiable Risk Factor Possession Patterns of Dementia in Elderly with MCI: A 4-Year Repeated Measures Study. J. Clin. Med. 2020, 9, 1076. [Google Scholar] [CrossRef]
- Otsuka, R.; Nishita, Y.; Nakamura, A.; Kato, T.; Ando, F.; Shimokata, H.; Arai, H. Basic lifestyle habits and volume change in total gray matter among community dwelling middle-aged and older Japanese adults. Prev. Med. 2022, 161, 107149. [Google Scholar] [CrossRef]
- Tsutsumimoto, K.; Doi, T.; Shimada, H.; Makizako, H.; Hotta, R.; Nakakubo, S.; Suzuki, T. Combined Effect of Slow Gait Speed and Depressive Symptoms on Incident Disability in Older Adults. J. Am. Med. Dir. Assoc. 2016, 17, 123–127. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307 e302. [Google Scholar] [CrossRef]
- Ma, Y.; Liang, L.; Zheng, F.; Shi, L.; Zhong, B.; Xie, W. Association Between Sleep Duration and Cognitive Decline. JAMA Netw. Open. 2020, 3, e2013573. [Google Scholar] [CrossRef]
- Gallassi, R.; Oppi, F.; Poda, R.; Scortichini, S.; Stanzani Maserati, M.; Marano, G.; Sambati, L. Are subjective cognitive complaints a risk factor for dementia? Neurol Sci 2010, 31, 327–336. [Google Scholar] [CrossRef]
- Nunes, T.; Fragata, I.; Ribeiro, F.; Palma, T.; Maroco, J.; Cannas, J.; Secca, M.; Menezes, C.; Carmo, I.; Cunha, G.; et al. The outcome of elderly patients with cognitive complaints but normal neuropsychological tests. J. Alzheimers Dis. 2010, 19, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [PubMed]
- Kremen, W.S.; Beck, A.; Elman, J.A.; Gustavson, D.E.; Reynolds, C.A.; Tu, X.M.; Sanderson-Cimino, M.E.; Panizzon, M.S.; Vuoksimaa, E.; Toomey, R.; et al. Influence of young adult cognitive ability and additional education on later-life cognition. Proc. Natl. Acad. Sci. USA 2019, 116, 2021–2026. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.R.; Peng, S.; Coleman, M.E.; Apostolova, L.G.; Perry, B.L. Do subjective or objective cognitive measures better predict social network type among older adults? Biodemography Soc. Biol. 2022, 67, 84–97. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Sahakian, B.J.; Kang, J.; Langley, C.; Zhang, W.; Xie, C.; Xiang, S.; Yu, J.; Cheng, W.; Feng, J. The brain structure and genetic mechanisms underlying the nonlinear association between sleep duration, cognition and mental health. Nat. Aging 2022, 2, 425–437. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Reisberg, B.; Shulman, M.B.; Torossian, C.; Leng, L.; Zhu, W. Outcome over seven years of healthy adults with and without subjective cognitive impairment. Alzheimers Dement. 2010, 6, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Prichep, L.S.; John, E.R.; Ferris, S.H.; Rausch, L.; Fang, Z.; Cancro, R.; Torossian, C.; Reisberg, B. Prediction of longitudinal cognitive decline in normal elderly with subjective complaints using electrophysiological imaging. Neurobiol. Aging 2006, 27, 471–481. [Google Scholar] [CrossRef]
- Luck, T.; Riedel-Heller, S.G.; Luppa, M.; Wiese, B.; Wollny, A.; Wagner, M.; Bickel, H.; Weyerer, S.; Pentzek, M.; Haller, F.; et al. Risk factors for incident mild cognitive impairment-results from the German Study on Ageing, Cognition and Dementia in Primary Care Patients (AgeCoDe). Acta Psychiatr. Scand. 2010, 121, 260–272. [Google Scholar] [CrossRef]


{kind=link}
| Total | Missing | Followed Participants | Lost at Follow-Up | |||
|---|---|---|---|---|---|---|
| n = 4363 | Number | n = 2569 | n = 1794 | p | Cohen’s d | |
| Age, y | 71.7 ± 5.3 | 0 | 70.9 ± 4.6 | 72.9 ± 6.1 | <0.001 * | −0370 |
| Sex, female % | 2239 (51.3) | 0 | 1322 (51.5) | 917 (51.1) | 0.823 | |
| Heart disease, yes % | 699 (16.0) | 0 | 401 (15.6) | 298 (16.6) | 0.375 | |
| Hypertension, yes % | 1963 (45.0) | 0 | 1086 (42.3) § | 876 (48.8) ‡ | <0.001 † | |
| Diabetes, yes % | 573 (13.1) | 0 | 313 (12.2) § | 260 (14.5) ‡ | 0.026 † | |
| Medications, number | 1.9 ± 2.0 | 0 | 1.8 ± 1.9 | 2.1 ± 2.1 | <0.001 * | −0.164 |
| BMI, kg/m2 | 23.4 ± 3.1 | 25 | 23.4 ± 2.9 | 23.4 ± 3.3 | 0.462 | −0.023 |
| Albumin, mg/dL | 4.3 ± 0.3 | 30 | 4.3 ± 0.2 | 4.3 ± 0.3 | <0.001 * | 0.193 |
| Total cholesterol, mg/dL | 208.8 ± 33.5 | 30 | 209.4 ± 32.4 | 207.8 ± 35.0 | 0.120 | −0.012 |
| Education, y | 11.4 ± 2.5 | 0 | 11.7 ± 2.5 | 11.0 ± 2.5 | <0.001 * | 0.199 |
| MMSE score | 26.5 ± 2.4 | 0 | 26.8 ± 2.3 | 26.1 ± 2.5 | <0.001 * | 0.216 |
| Word list memory, composite score | 11.2 ± 2.9 | 0 | 11.6 ± 2.7 | 10.6 ± 3.0 | <0.001 * | 0.365 |
| TMT-A, seconds | 20.9 ± 6.2 | 0 | 19.9 ± 5.1 | 22.2 ± 7.3 | <0.001 * | −0.374 |
| TMT-B, seconds | 42.5 ± 17.1 | 0 | 39.6 ± 14.9 | 46.5 ± 19.1 | <0.001 * | −0.410 |
| SDST, score | 38.6 ± 8.1 | 0 | 40.1 ± 7.4 | 36.4 ± 8.5 | <0.001 * | 0.480 |
| Grip strength, kg | 27.0 ± 7.9 | 192 | 27.6 ± 7.8 | 26.2 ± 8.0 | <0.001 * | 0.178 |
| Walking speed, m/sec | 1.2 ± 0.2 | 6 | 1.2 ± 0.2 | 1.2 ± 0.2 | <0.001 * | 0.421 |
| Sleep duration, minutes | 461.9 ± 73.8 | 0 | 455.4 ± 67.9 | 471.2 ± 80.6 | <0.001 * | −0.216 |
| GDS, score | 2.7 ± 2.5 | 13 | 2.4 ± 2.3 | 3.2 ± 2.6 | <0.001 * | −0.299 |
| Do you have any hobbies or sports activities? no (%) | 1138 (26.1) | 8 | 523 (20.4) § | 615 (34.4) ‡ | <0.001 † | |
| Do you read books or newspapers? no (%) | 168 (3.9) | 1 | 71 (2.8) § | 97 (5.4)‡ | <0.001 † | |
| Do you drive a car? no (%) | 1218 (27.9) | 5 | 593 (23.1) § | 625 (34.9) ‡ | <0.001 † | |
| Do you use a personal computer? no (%) | 2852 (65.4) | 1 | 1544 (60.1) § | 1308 (72.9) ‡ | <0.001 † | |
| Do you engage in activities that use your brain (shogi, learning, etc.)? no (%) | 2178 (50.0) | 9 | 1205 (47.0) § | 973 (54.4) ‡ | <0.001 † | |
| Do you operate a video/DVD player? no (%) | 2022 (46.4) | 3 | 1120 (43.6) § | 902 (50.3) ‡ | <0.001 † | |
| Are you a board member or secretary of a neighborhood association, senior citizens’ club, or non-profit organization? no (%) | 2940 (67.5) | 8 | 1613 (62.9) § | 1327 (74.1) ‡ | <0.001 † | |
| Do you engage in any activities related to environmental beautification (e.g., cleaning up parks)? no (%) | 2962 (67.9) | 1 | 1643 (64.0) § | 1319 (73.6) ‡ | <0.001 † | |
| Do you sometimes visit your friends? no (%) | 551 (12.6) | 4 | 272 (10.6) § | 279 (15.6) ‡ | <0.001 † | |
| Do you have a friend to call? no (%) | 253 (5.8) | 10 | 144 (5.6) | 109 (6.1) | 0.504 | |
| Protective factors, n | 13.4 ± 2.8 | 194 | 14.0 ± 2.6 | 12.6 ± 2.9 | <0.001 * | 0.493 |
| Normal Cognition | SCD-Only | OCD-Only | SCD and OCD | ||||
|---|---|---|---|---|---|---|---|
| n = 955 | n = 2044 | n = 386 | n = 978 | p | η2 | Post-Hoc | |
| Age, y | 71.1 ± 4.8 | 71.4 ± 5.2 | 72 ± 5.4 | 73 ± 5.8 | <0.001 * | 0.018 | N < O < SO |
| Sex, female % | 509 (53.3) | 1083 (53.0) ‡ | 176 (45.6) § | 471 (48.2) § | 0.005 | ||
| Heart disease, yes % | 122 (12.8) § | 351 (17.2) | 46 (11.9) § | 180 (18.4) ‡ | 0.585 | ||
| Hypertension, yes % | 423 (44.3) | 893 (43.7) | 176 (45.6) | 470 (48.1) ‡ | 0.866 | ||
| Diabetes, yes % | 108 (11.3) | 281 (13.7) | 41 (10.6) | 143 (14.6) | 0.058 | ||
| Medications, number | 1.7 ± 1.8 | 1.9 ± 2.0 | 1.9 ± 1.9 | 2.2 ± 2.1 | <0.001 * | 0.007 | N, S, O < SO |
| BMI, kg/m2 | 23.4 ± 3.1 | 23.3 ± 3.1 | 23.8 ± 3.3 | 23.4 ± 3.1 | 0.084 | 0.002 | |
| Albumin, mg/dL | 4.4 ± 0.3 | 4.3 ± 0.3 | 4.3 ± 0.2 | 4.3 ± 0.3 | <0.001 * | 0.008 | SO < S < N |
| Total cholesterol, mg/dL | 211.6 ± 33.4 | 209.4 ± 33.5 | 206.3 ± 30.9 | 205.5 ± 34.4 | 0.009 * | 0.004 | SO < S; O, SO < N |
| Education, y | 11.6 ± 2.4 | 11.7 ± 2.5 | 11.1 ± 2.4 | 10.9 ± 2.5 | <0.001 * | 0.018 | O, SO < N, S |
| MMSE score | 27.2 ± 1.9 | 27.3 ± 1.8 | 24.6 ± 2.5 | 24.8 ± 2.6 | <0.001 * | 0.241 | O, SO < N, S |
| Word list memory, composite score | 12.0 ± 2.4 | 11.9 ± 2.5 | 9.8 ± 2.9 | 9.5 ± 3.0 | <0.001 * | 0.150 | O, SO < N, S |
| TMT-A, seconds | 19.1 ± 3.9 | 19.3 ± 4.3 | 24.2 ± 7.6 | 24.7 ± 8.3 | <0.001 * | 0.160 | N, S < O, SO |
| TMT-B, seconds | 35.7 ± 9.6 | 36.1 ± 10.2 | 55.0 ± 19.9 | 57.3 ± 20.7 | <0.001 * | 0.315 | N, S < O, SO |
| SDST, score | 41.1 ± 6.9 | 40.7 ± 7.1 | 34.5 ± 7.9 | 33.2 ± 8.1 | <0.001 * | 0.177 | SO < O < N, S |
| Grip strength, kg | 27.1 ± 7.7 | 27.3 ± 7.9 | 27.4 ± 8.3 | 26.4 ± 8.1 | 0.041 * | 0.002 | SO < S |
| Walking speed, m/sec | 1.2 ± 0.2 | 1.2 ± 0.2 | 1.2 ± 0.2 | 1.1 ± 0.2 | <0.001 * | 0.029 | SO < O < N, S |
| Sleep duration, minutes | 459.8 ± 67.8 | 457.3 ± 69.2 | 464.9 ± 84.9 | 472.4 ± 82.5 | <0.001 * | 0.007 | N, S < SO |
| GDS, score | 1.8 ± 1.9 | 2.9 ± 2.5 | 2.2 ± 2.1 | 3.5 ± 2.7 | <0.001 * | 0.060 | N < O < S < SO |
| Do you have any hobbies or sports activities? no (%) | 222 (23.3) § | 482 (23.6) § | 131 (33.9) ‡ | 303 (31.0) ‡ | <0.001 † | ||
| Do you read books or newspapers? no (%) | 26 (2.7) § | 60 (2.9) § | 16 (4.1) | 66 (6.7) ‡ | <0.001 † | ||
| Do you drive a car? no (%) | 252 (26.4) | 517 (25.3) § | 119 (30.9) | 330 (33.7) ‡ | <0.001 † | ||
| Do you use a personal computer? no (%) | 606 (63.5) | 1233 (60.4) § | 286 (74.1) ‡ | 727 (74.3) ‡ | <0.001 † | ||
| Do you engage in activities that use your brain (shogi, learning, etc.)? no (%) | 413 (43.3) § | 980 (48.0) § | 190 (49.2) | 595 (61.0) ‡ | <0.001 † | ||
| Do you operate a video/DVD player? no (%) | 413 (43.2) § | 879 (43.0) § | 203 (52.7) ‡ | 527 (53.9) ‡ | <0.001 † | ||
| Are you a board member or secretary of a neighborhood association, senior citizens’ club, or non-profit organization? no (%) | 631 (66.1) | 1318 (64.6) § | 272 (70.6) | 719 (73.7) ‡ | <0.001 † | ||
| Do you engage in any activities related to environmental beautification (e.g., cleaning up parks)? no (%) | 665 (69.6) | 1327 (65.0) § | 282 (73.1) ‡ | 688 (70.3) | 0.001 † | ||
| Do you sometimes visit your friends? no (%) | 107 (11.2) | 236 (11.6) § | 58 (15.0) | 150 (15.4) ‡ | 0.006 † | ||
| Do you have a friend to call? no (%) | 41 (4.3) § | 101 (4.9) § | 32 (8.4) ‡ | 79 (8.1) ‡ | <0.001 † | ||
| Protective factors, n | 13.8 ± 2.6 | 13.7 ± 2.7 | 13.0 ± 2.8 | 12.5 ± 2.8 | <0.001 * | 0.038 | SO < O < N, S |
| Crude Model | Adjusted Model | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | |
| Normal cognition | 1.00 | 1.00 | ||||
| SCD-only | 1.09 | 0.84–1.43 | 0.520 | 1.08 | 0.80–1.45 | 0.608 |
| OCD-only | 4.80 | 3.33–6.91 | <0.001 | 4.00 | 2.64–6.07 | <0.001 |
| SCD and OCD | 4.45 | 3.34–5.93 | <0.001 | 3.12 | 2.22–4.37 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katayama, O.; Lee, S.; Bae, S.; Makino, K.; Chiba, I.; Harada, K.; Morikawa, M.; Tomida, K.; Shimada, H. Differences in Subjective and Objective Cognitive Decline Outcomes Are Associated with Modifiable Protective Factors: A 4-Year Longitudinal Study. J. Clin. Med. 2022, 11, 7441. https://doi.org/10.3390/jcm11247441
Katayama O, Lee S, Bae S, Makino K, Chiba I, Harada K, Morikawa M, Tomida K, Shimada H. Differences in Subjective and Objective Cognitive Decline Outcomes Are Associated with Modifiable Protective Factors: A 4-Year Longitudinal Study. Journal of Clinical Medicine. 2022; 11(24):7441. https://doi.org/10.3390/jcm11247441
Chicago/Turabian StyleKatayama, Osamu, Sangyoon Lee, Seongryu Bae, Keitaro Makino, Ippei Chiba, Kenji Harada, Masanori Morikawa, Kouki Tomida, and Hiroyuki Shimada. 2022. "Differences in Subjective and Objective Cognitive Decline Outcomes Are Associated with Modifiable Protective Factors: A 4-Year Longitudinal Study" Journal of Clinical Medicine 11, no. 24: 7441. https://doi.org/10.3390/jcm11247441
APA StyleKatayama, O., Lee, S., Bae, S., Makino, K., Chiba, I., Harada, K., Morikawa, M., Tomida, K., & Shimada, H. (2022). Differences in Subjective and Objective Cognitive Decline Outcomes Are Associated with Modifiable Protective Factors: A 4-Year Longitudinal Study. Journal of Clinical Medicine, 11(24), 7441. https://doi.org/10.3390/jcm11247441