
COVID-19 Vaccination Is Associated with a Better Outcome in Acute Ischemic Stroke Patients: A Retrospective Observational Study

 , , , , , ,
, , , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
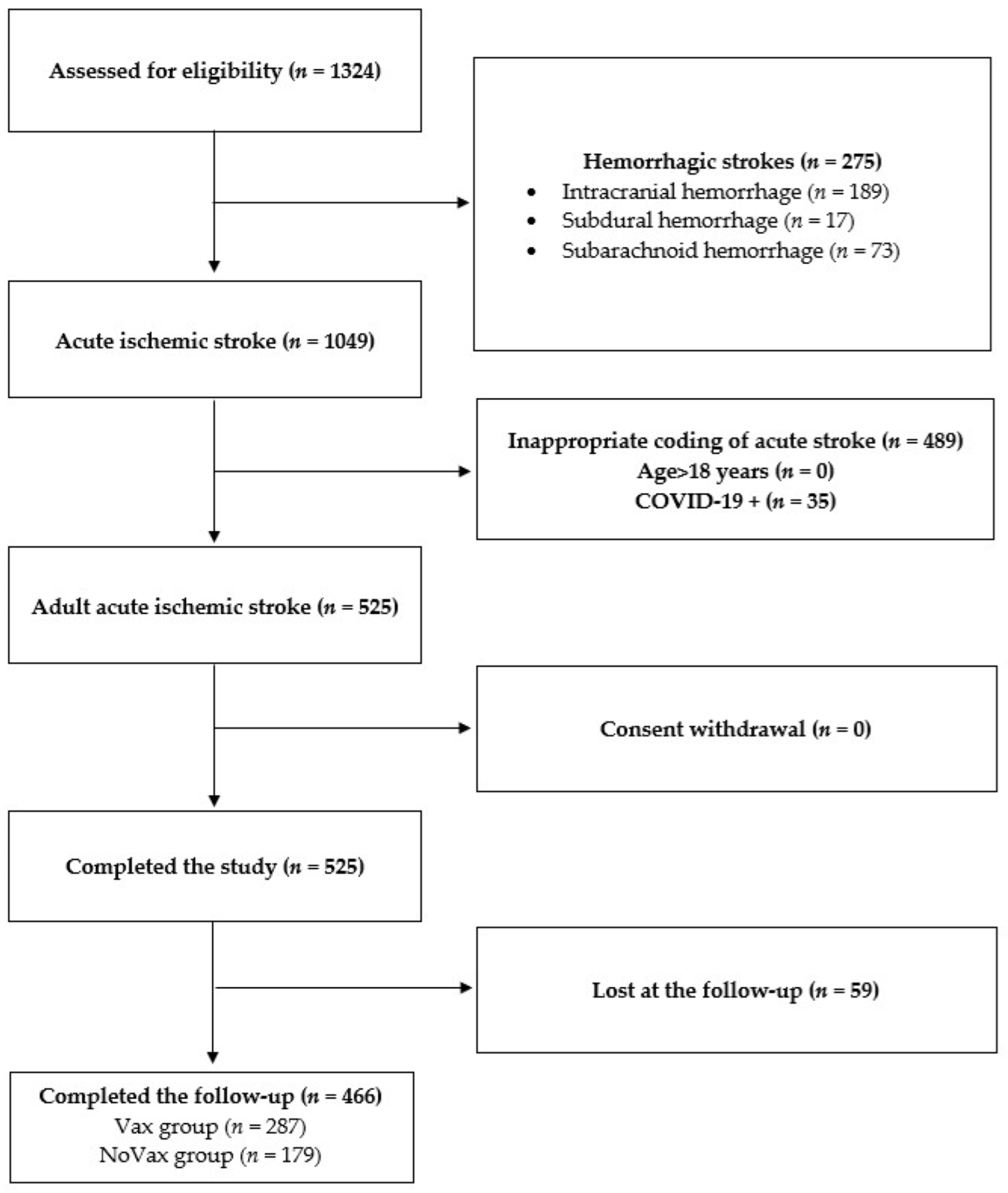
2.1. Study Design and Population
2.2. Clinical Evaluation
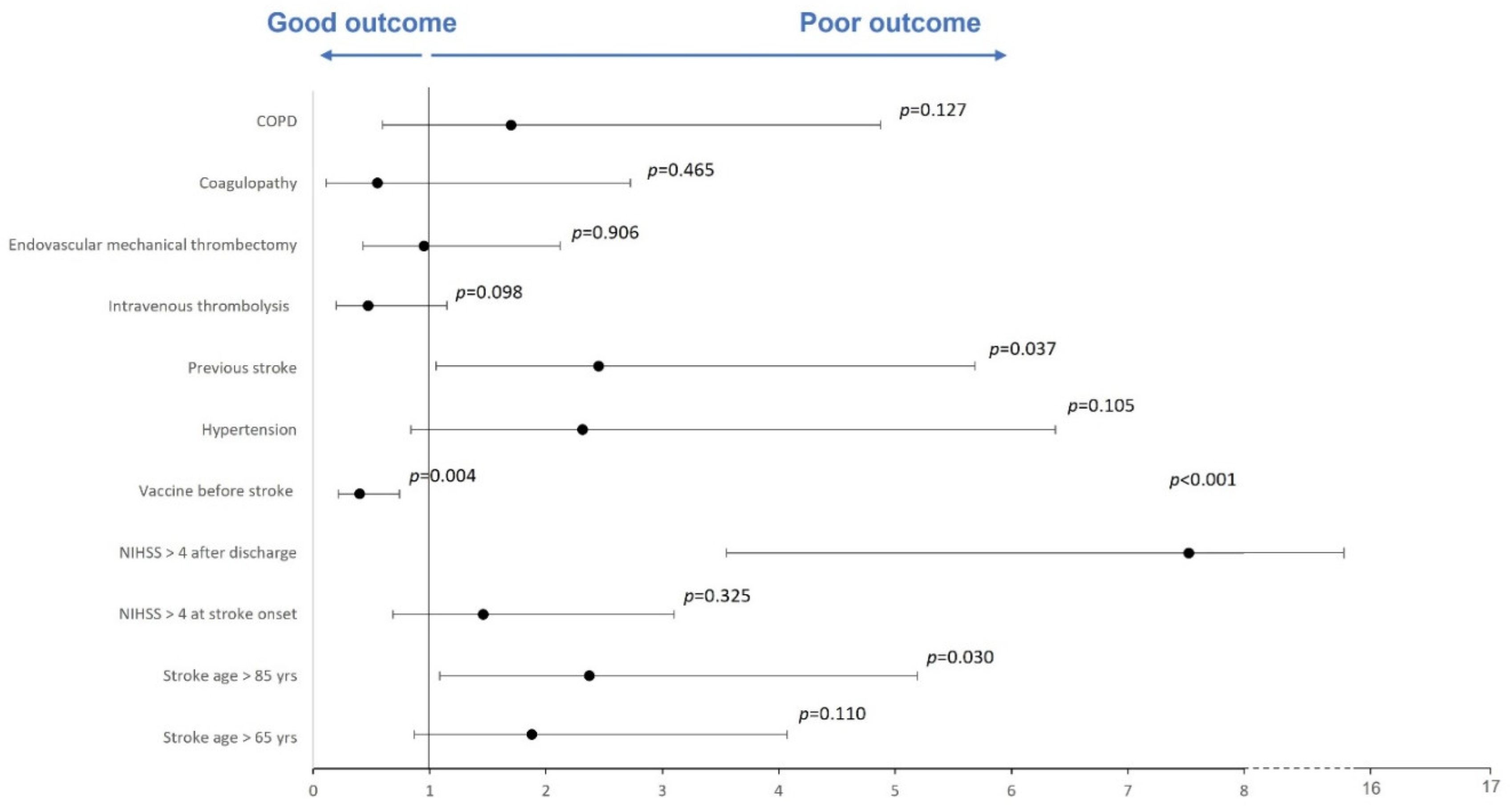
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johns Hopkins University & Medicine, Coronavirus Resource Center. COVID-19 Map. Available online: https://coronavirus.jhu.edu/map.html (accessed on 15 September 2022).
- Klok, F.A.; Pai, M.; Huisman, M.V.; Makris, M. Vaccine-induced immune thrombotic thrombocytopenia. Lancet Haematol. 2022, 9, e73–e80. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, M.; Waliszewska-Prosół, M.; Koutsokera, M.; Robotti, M.; Straburzyński, M.; Apostolakopoulou, L.; Capizzi, M.; Çibuku, O.; Ambat, F.D.F.; Frattale, I.; et al. Headache onset after vaccination against SARS-CoV-2: A systematic literature review and meta-analysis. J. Headache Pain 2022, 23, 41. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 nCoV-19) COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 2348–2360. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Jerald Sadoff, M.D.; Glenda Gray, M.B.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV-2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Jabagi, M.J.; Botton, J.; Bertrand, M.; Weill, A.; Farrington, P.; Zureik, M.; Dray-Spira, R. Myocardial Infarction, Stroke, and Pulmonary Embolism After BNT162b2 mRNA COVID-19 Vaccine in People Aged 75 Years or Older. JAMA 2022, 327, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in a nationwide setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Whiteley, W.N.; Ip, S.; Cooper, J.A.; Bolton, T.; Keene, S.; Walker, V.; Denholm, R.; Akbari, A.; Omigie, E.; Hollings, S.; et al. Association of COVID-19 vaccines ChAdOx1 and BNT162b2 with major venous, arterial, or thrombocytopenic events: A population-based cohort study of 46 million adults in England. PLoS Med. 2022, 19, e1003926. [Google Scholar] [CrossRef]
- Brott, T.; Adams, H.P., Jr.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V.; et al. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Banks, J.L.; Marotta, C.A. Outcomes validity and reliability of the modified Rankin scale: Implications for stroke clinical trials: A literature review and synthesis. Stroke 2007, 38, 1091–1096. [Google Scholar] [CrossRef]
- Appelros, P.; Nydevik, I.; Viitanen, M. Poor outcome after first-ever stroke: Predictors for death, dependency, and recurrent stroke within the first year. Stroke 2003, 34, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef]
- Ewer, K.J.; Barrett, J.R.; Belij-Rammerstorfer, S.; Sharpe, H.; Makinson, R.; Morter, R.; Flaxman, A.; Wright, D.; Bellamy, D.; Bittaye, M.; et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 2021, 27, 270–278. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, P.S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Keech, C.; Albert, G.; Cho, I.; Robertson, A.; Reed, P.; Neal, S.; Plested, J.S.; Zhu, M.; Cloney-Clark, S.; Zhou, H.; et al. Phase 1–2 trial of a SARS-CoV-2 recombinant spike protein nanoparticle vaccine. N. Engl. J. Med. 2020, 383, 2320–2332. [Google Scholar] [CrossRef]
- Sahin, U.; Muik, A.; Derhovanessian, E.; Vogler, I.; Kranz, L.M.; Vormehr, M.; Baum, A.; Pascal, K.; Quandt, J.; Maurus, D.; et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature 2020, 586, 594–599. [Google Scholar] [CrossRef]
- Stephenson, K.E.; Le Gars, M.; Sadoff, J.; de Groot, A.M.; Heerwegh, D.; Truyers, C.; Atyeo, C.; Loos, C.; Chandrashekar, A.; McMahan, K.; et al. Immunogenicity of the Ad26.COV-2.S vaccine for COVID-19. JAMA 2021, 325, 1535–1544. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, P.G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Volzke, J.; Subin, B.; Müller, S.; Sombetzki, M.; Reisinger, E.C.; Müller-Hilke, B. Single-dose SARS-CoV-2 vaccinations with either BNT162b2 or AZD1222 induce disparate Th1 responses and IgA production. BMC Med. 2022, 20, 29. [Google Scholar] [CrossRef]
- Gupta, S.; Su, H.; Agrawal, S. Immune Response to SARS-CoV-2 Vaccine in 2 Men. Int. Arch. Allergy Immunol. 2022, 183, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Chamorro, A.; Meisel, A.; Planas, A.M.; Urra, X.; van de Beek, D.; Veltkamp, R. The immunology of acute stroke. Nat. Rev. Neurol. 2012, 8, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Akter, F.; Qin, L.; Cheng, J.; Guo, M.; Yao, S.; Jian, Z.; Liu, R.; Wu, S. Adaptive Immunity Regulation and Cerebral Ischemia. Front. Immunol. 2020, 11, 689. [Google Scholar] [CrossRef]
- Vogelgesang, A.; Dressel, A. Immunological consequences of ischemic stroke: Immunosuppression and autoimmunity. J. Neuroimmunol. 2011, 231, 105–110. [Google Scholar] [CrossRef]
- Whiteley, W.; Chong, W.L.; Sengupta, A.; Sandercock, P. Blood markers for the prognosis of ischemic stroke: A systematic review. Stroke 2009, 40, e380–e389. [Google Scholar] [CrossRef]
- Santamaría-Cadavid, M.; Rodríguez-Castro, E.; Rodríguez-Yáñez, M.; Arias-Rivas, S.; López-Dequidt, I.; Pérez-Mato, M.; Rodríguez-Pérez, M.; López-Loureiro, I.; Hervella, P.; Campos, F.; et al. Regulatory T cells participate in the recovery of ischemic stroke patients. BMC Neurol. 2020, 20, 68. [Google Scholar] [CrossRef]
- Chen, F.; Qi, Z.; Luo, Y.; Hinchliffe, T.; Ding, G.; Xia, Y.; Ji, X. Non-pharmaceutical therapies for stroke: Mechanisms and clinical implications. Prog. Neurobiol. 2014, 115, 246–269. [Google Scholar] [CrossRef]
- Liu, Z.-J.; Chen, C.; Li, X.-R.; Ran, Y.-Y.; Xu, T.; Zhang, Y.; Geng, X.-K.; Zhang, Y.; Du, H.-S.; Leak, R.K.; et al. Remote Ischemic Preconditioning-Mediated Neuroprotection against Stroke is Associated with Significant Alterations in Peripheral Immune Responses. CNS Neurosci. Ther. 2016, 22, 43–52. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Features and Risk Factors | VAX (n = 287) | NoVAX (n = 179) | p-Value |
|---|---|---|---|
| Age, median (years, IQR) § | 77 (14) | 74.5 (22) | 0.072 |
| Sex, male, n (%) † | 161 (56) | 89.5 (50) | 0.311 |
| Other vaccines (previous 3 years), n (%) † | 135 (47) | 71 (40) | 0.451 |
| Risk Factors | |||
| Hypertension, n (%) † | 258 (90) | 143 (80) | 0.009 |
| Diabetes mellitus, n (%) † | 66 (23) | 34 (19) | 0.421 |
| Hyperlipidemia, n (%) † | 109 (38) | 64 (36) | 0.698 |
| Cigarette smoking, n (%) † | 20 (7) | 21 (12) | 0.102 |
| Obesity, n (%) † | 11 (4) | 7 (4) | 1.000 |
| COPD, n (%) ‡ | 28 (10) | 5 (3) | 0.018 |
| Renal failure, n (%) † | 17 (6) | 12 (7) | 0.802 |
| Atrial fibrillation, n (%) † | 54 (19) | 30 (17) | 0.577 |
| Previous stroke, n (%) † | 34 (12) | 21 (12) | 0.891 |
| Coagulopathy, n (%) ‡ | 5 (2) | 11 (6) | 0.028 |
| Valvular heart disease, n (%) † | 20 (7) | 13 (7) | 0.952 |
| Cardiopathy, n (%) † | 51 (18) | 39 (22) | 0.522 |
| Patent foramen ovale, n (%) ‡ | 6 (2) | 10 (6) | 0.220 |
| Cancer, n (%) † | 29 (10) | 18 (10) | 0.926 |
| Vaccine Type | |||
| BNT162b2, n (%) | 207 (72) | ||
| ChAdOx1-S, n (%) | 43 (15) | ||
| Ad26.COV-2.S, n (%) | 12 (4) | ||
| Spikevax, n (%) | 25 (9) | ||
| Clinical Assessment and Procedures | |||
| Intravenous thrombolysis, n (%) † | 37 (13) | 21 (12) | 0.824 |
| Endovascular mechanical thrombectomy, n (%) † | 48 (17) | 29 (16) | 0.765 |
| NIHSS at stroke onset, median (IQR) § | 3 (7) | 3 (7) | 0.920 |
| NIHSS after discharge, median (IQR) § | 1 (4) | 2 (6) | <0.001 |
| mRS after 3 months, median (IQR) § | 1 (2) | 2 (4) | <0.001 |
| mRS 3–6, n (%) † | 97 (34) | 87 (49) | 0.006 |
| Death, n (%) † | 20 (7) | 43 (24) | <0.001 |
| COVID-19 during 3-month follow-up, n (%) † | 20 (7) | 16 (9) | 0.340 |
| Hospitalization for COVID-19 during follow-up, n (%) † | 3 (1) | 9 (5) | 0.029 |
| Demographic Features and Risk Factors | mRS 0–2 (n = 289) | mRS 3–6 (n = 177) | p-Value |
|---|---|---|---|
| Age, median (years, IQR) § | 74 (22) | 79 (13) | <0.001 |
| Stroke age >65 years, n (%) † | 196 (68) | 155 (88) | <0.001 |
| Stroke age >85 years, n (%) † | 49 (17) | 54 (31) | <0.001 |
| Sex, male, n (%) † | 159 (55) | 88 (50) | 0.452 |
| Vaccine before stroke, n (%) † | 191 (66) | 92 (52) | 0.007 |
| Other vaccines (previous 3 years), n (%) † | 122 (42) | 84 (47) | 0.624 |
| Risk Factors | |||
| Hypertension, n (%) † | 235 (81) | 166 (94) | 0.005 |
| Diabetes mellitus, n (%) † | 58 (20) | 42 (24) | 0.562 |
| Hyperlipidemia, n (%) † | 101 (34) | 71 (40) | 0.078 |
| Cigarette smoking, n (%) † | 29 (10) | 12 (7) | 0.314 |
| Obesity, n (%) ‡ | 6 (2) | 12 (7) | 0.026 |
| COPD, n (%) † | 17 (6) | 16 (10) | 0.133 |
| Renal failure, n (%) † | 14 (5) | 15 (9) | 0.259 |
| Atrial fibrillation, n (%) † | 43 (15) | 41 (23) | 0.057 |
| Previous stroke, n (%) ‡ | 14 (5) | 41 (23) | 0.037 |
| Coagulopathy, n (%) ‡ | 11 (4) | 5 (3) | 0.522 |
| Valvular heart disease, n (%) † | 17 (6) | 16 (9) | 0.683 |
| Cardiopathy, n (%) † | 55 (19) | 35 (20) | 0.825 |
| Patent foramen ovale, n (%) ‡ | 12 (6) | 4 (2) | 0.004 |
| Cancer, n (%) ‡ | 22 (8) | 25 (14) | 0.091 |
| Clinical Assessment and Procedures | |||
| Intravenous thrombolysis, n (%) † | 38 (13) | 21 (12) | 0.756 |
| Endovascular mechanical thrombectomy, n (%) † | 40 (14) | 37 (21) | 0.098 |
| NIHSS2 at stroke onset, median (IQR) § | 2 (5) | 6 (11) | <0.001 |
| NIHSS after discharge, median (IQR) § | 1 (2) | 5 (10) | <0.001 |
| NIHSS > 4 at stroke onset, n (%) † | 95 (33) | 120 (68) | <0.001 |
| NIHSS > 4 after discharge, n (%) † | 37 (13) | 106 (60) | <0.001 |
| COVID-19 during 3-month follow-up, n (%) † | 23 (8) | 9 (7) | 0.815 |
| Hospitalization for COVID-19 during follow-up, n (%) ‡ | 3 (1) | 9 (5) | 0.039 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, P.A.; Bellavia, S.; Scala, I.; Colò, F.; Broccolini, A.; Antonica, R.; Vitali, F.; Angeloni, B.M.; Brunetti, V.; Di Iorio, R.; et al. COVID-19 Vaccination Is Associated with a Better Outcome in Acute Ischemic Stroke Patients: A Retrospective Observational Study. J. Clin. Med. 2022, 11, 6878. https://doi.org/10.3390/jcm11236878
Rizzo PA, Bellavia S, Scala I, Colò F, Broccolini A, Antonica R, Vitali F, Angeloni BM, Brunetti V, Di Iorio R, et al. COVID-19 Vaccination Is Associated with a Better Outcome in Acute Ischemic Stroke Patients: A Retrospective Observational Study. Journal of Clinical Medicine. 2022; 11(23):6878. https://doi.org/10.3390/jcm11236878
Chicago/Turabian StyleRizzo, Pier Andrea, Simone Bellavia, Irene Scala, Francesca Colò, Aldobrando Broccolini, Riccardo Antonica, Francesca Vitali, Benedetta Maria Angeloni, Valerio Brunetti, Riccardo Di Iorio, and et al. 2022. "COVID-19 Vaccination Is Associated with a Better Outcome in Acute Ischemic Stroke Patients: A Retrospective Observational Study" Journal of Clinical Medicine 11, no. 23: 6878. https://doi.org/10.3390/jcm11236878
APA StyleRizzo, P. A., Bellavia, S., Scala, I., Colò, F., Broccolini, A., Antonica, R., Vitali, F., Angeloni, B. M., Brunetti, V., Di Iorio, R., Monforte, M., Della Marca, G., Calabresi, P., Luigetti, M., & Frisullo, G. (2022). COVID-19 Vaccination Is Associated with a Better Outcome in Acute Ischemic Stroke Patients: A Retrospective Observational Study. Journal of Clinical Medicine, 11(23), 6878. https://doi.org/10.3390/jcm11236878