

Factors Influencing the Survival Rate of Teeth and Implants in Patients after Tumor Therapy to the Head and Neck Region—Part 2: Implant Survival

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tumor Therapy
2.2. Dental Treatment in Relation to Radiotherapy
2.3. Dental Treatment after TT
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Characterization of the Study Cohort
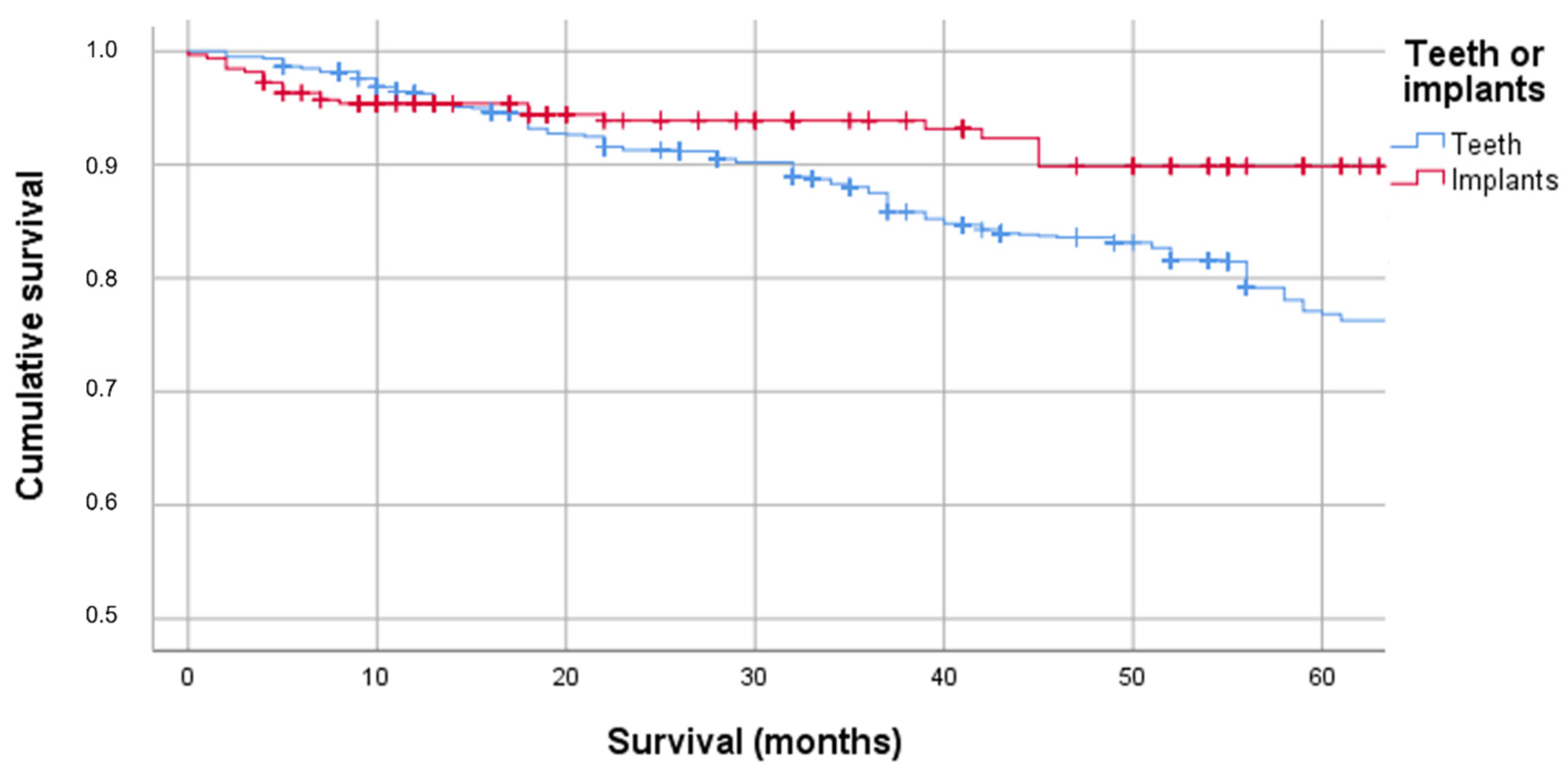
3.2. Survival of Teeth and Implants after TT
3.3. Factors Influencing Implant Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marker, P.; Siemssen, S.J.; Bastholt, L. Osseointegrated implants for prosthetic rehabilitation after treatment of cancer of the oral cavity. Acta Oncol. 1997, 36, 37–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, J.B.; Thariat, J.; Bensadoun, R.J.; Barasch, A.; Murphy, B.A.; Kolnick, L.; Popplewell, L.; Maghami, E. Oral complications of cancer and cancer therapy: From cancer treatment to survivorship. CA A Cancer J. Clin. 2012, 62, 400–422. [Google Scholar] [CrossRef] [PubMed]
- Abed, H.; Reilly, D.; Burke, M.; Daly, B. Patients with head and neck cancers’ oral health knowledge, oral health-related quality of life, oral health status, and adherence to advice on discharge to primary dental care: A prospective observational study. Spéc. Care Dent. 2019, 39, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Schweyen, R.; Hey, J.; Fränzel, W.; Vordermark, D.; Hildebrandt, G.; Kuhnt, T. Radiation related caries: Etiology and possible preventive strategies. What should the radiotherapist know? Strahlenther. Onkol. 2012, 188, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Hey, J.; Seidel, J.; Schweyen, R.; Paelecke-Habermann, Y.; Vordermark, D.; Gernhardt, C.R.; Kuhnt, T. The influence of parotid gland sparing on radiation damages of dental hard tissues. Clin. Oral Investig. 2013, 17, 1619–1625. [Google Scholar] [CrossRef]
- Jansma, J.; Vissink, A.; Spijkervet, F.K.; Roodenburg, J.L.; Panders, A.K.; Vermey, A.; Szabó, B.G.; Johannes’S-Gravenmade, E. Protocol for the prevention and treatment of oral sequelae resulting from head and neck radiation therapy. Cancer 1992, 70, 2171–2180. [Google Scholar] [CrossRef]
- Sammartino, G.; Marenzi, G.; Cioffi, I.; Teté, S.; Mortellaro, C. Implant therapy in irradiated patients. J. Craniofacial Surg. 2011, 22, 443–445. [Google Scholar] [CrossRef]
- Misch, C.E.; Perel, M.L.; Wang, H.L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant success, survival, and failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Gröbe, A.; Heiland, M.; Ebker, T. Impact of Dental Implant Surface Modifications on Osseointegration. BioMed Res. Int. 2016, 2016, 6285620. [Google Scholar] [CrossRef] [Green Version]
- Giudice, A.; Bennardo, F.; Antonelli, A.; Barone, S.; Wagner, F.; Fortunato, L.; Traxler, H. Influence of clinician’s skill on primary implant stability with conventional and piezoelectric preparation techniques: An ex-vivo study. J. Biol. Regul. Homeost. Agents 2020, 34, 739–745. [Google Scholar]
- Attanasio, F.; Antonelli, A.; Brancaccio, Y.; Averta, F.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dent. J. 2020, 21, 21. [Google Scholar] [CrossRef] [PubMed]
- Wolf, F.; Spoerl, S.; Gottsauner, M.; Klingelhöffer, C.; Spanier, G.; Kolbeck, C.; Reichert, T.E.; Hautmann, M.G.; Ettl, T. Significance of site-specific radiation dose and technique for success of implant-based prosthetic rehabilitation in irradiated head and neck cancer patients-A cohort study. Clin. Implant Dent. Relat. Res. 2021, 23, 444–455. [Google Scholar] [CrossRef] [PubMed]
- Yerit, K.C.; Posch, M.; Seemann, M.; Hainich, S.; Dörtbudak, O.; Turhani, D.; Ozyuvaci, H.; Watzinger, F.; Ewers, R. Implant survival in mandibles of irradiated oral cancer patients. Clin. Oral Implant. Res. 2006, 17, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Chávez, E.M.; Wong, L.M.; Subar, P.; Young, D.A.; Wong, A. Dental care for geriatric and special needs populations. Dent. Clin. N. Am. 2018, 62, 245–267. [Google Scholar] [CrossRef]
- Shugaa-Addin, B.; Al-Shamiri, H.M.; Al-Maweri, S.; Tarakji, B. The effect of radiotherapy on of dental implants in head and neck cancer patients. J. Clin. Exp. Dent. 2016, 8, 194–200. [Google Scholar] [CrossRef]
- Schweyen, R.; Reich, W.; Vordermark, D.; Kuhnt, T.; Wienke, A.; Hey, J. Factors Influencing the Survival Rate of Teeth and Implants in Patients after Tumor Therapy to the Head and Neck Region—Part 1: Tooth Survival. J. Clin. Med. 2022, 11, 6222. [Google Scholar] [CrossRef]
- Grötz, K.A. Zahnärztliche Betreuung von Patienten mit tumortherapeutischer Kopf-Hals- Bestrahlung. Dtsch Zahnarztl Z 2002, 57, 509–511. [Google Scholar]
- Kuhnt, T.; Stang, A.; Wienke, A.; Vordermark, D.; Schweyen, R.; Hey, J. Potential risk factors for jaw osteoradionecrosis after radiotherapy for head and neck cancer. Radiat. Oncol. 2016, 11, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulaiman, F.; Huryn, J.M.; Zlotolow, I.M. Dental extractions in the irradiated head and neck patient: A retrospective analysis of Memorial Sloan-Kettering Cancer Center protocols, criteria, and end results. J. Oral Maxillofac. Surg. 2003, 61, 1123–1131. [Google Scholar] [CrossRef]
- Witter, D.J.; van Palenstein Helderman, W.H.; Creugers, N.H.; Käyser, A.F. The shortened dental arch concept and its implications for oral health care. Community Dent. Oral Epidemiol. 1999, 27, 249–258. [Google Scholar] [CrossRef]
- Epstein, J.B.; Chin, E.A.; Jacobson, J.J.; Rishiraj, B.; Le, N. The relationships among fluoride, cariogenic oral flora, and salivary flow rate during radiation therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1998, 86, 286–292. [Google Scholar] [CrossRef]
- Bacher, H.; Schweyen, R.; Kuhnt, T.; Leplow, B.; Hey, J. Use of a patient information leaflet on oro-dental care during radiotherapy. Patient Prefer. Adherence 2020, 14, 1751–1759. [Google Scholar] [CrossRef] [PubMed]
- Kielbassa, A.M.; Hinkelbein, W.; Hellwig, E.; Meyer-Luckel, H. Radiation-related damage to dentition. Lancet Oncol. 2006, 7, 326–335. [Google Scholar] [CrossRef]
- Grötz, K.A.; Riesenbeck, D.; Brahm, R.; Seegenschmiedt, M.H.; al-Nawas, B.; Dörr, W.; Kutzner, J.; Willich, N.; Thelen, M.; Wagner, W. Chronic radiation effects on dental hard tissue (radiation caries). Classification and therapeutic strategies. Strahlenther. Onkol. 2001, 177, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Asikainen, P.; Klemetti, E.; Kotilainen, R.; Vuillemin, T.; Sutter, F.; Voipio, H.M.; Kullaa, A. Osseointegration of dental implants in bone irradiated with 40, 50 or 60 gy doses. An experimental study with beagle dogs. Clin. Oral Implant. Res. 1998, 9, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Nicoletti, G.; Soutar, D.S.; Jackson, M.S.; Wrench, A.A.; Robertson, G. Chewing and swallowing after surgical treatment for oral cancer: Functional evaluation in 196 selected cases. Plast. Reconstr. Surg. 2004, 114, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Burlage, F.R.; Coppes, R.P.; Meertens, H.; Stokman, M.A.; Vissink, A. Parotid and submandibular/sublingual salivary flow during high dose radiotherapy. Radiother. Oncol. 2001, 61, 271–274. [Google Scholar] [CrossRef]
- Dawes, C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J. Dent. Res. 1987, 66, 648–653. [Google Scholar] [CrossRef]
- Hey, J.; Setz, J.; Gerlach, R.; Janich, M.; Hildebrandt, G.; Vordermark, D.; Gernhardt, C.R.; Kuhnt, T. Parotid gland-recovery after radiotherapy in the head and neck region--36 months follow-up of a prospective clinical study. Radiat. Oncol. 2011, 6, 125. [Google Scholar] [CrossRef] [Green Version]
- Wei, L.J.; Lin, D.J.; Weissfeld, L. Regression analysis of multivariate incomplete failure time data by modeling marginal distributions. J. Am. Stat. Assoc. 1989, 84, 1065–1073. [Google Scholar] [CrossRef]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Curi, M.M.; Condezo, A.F.B.; Ribeiro, K.D.C.B.; Cardoso, C.L. Long-term success of dental implants in patients with head and neck cancer after radiation therapy. Int. J. Oral Maxillofac. Surg. 2018, 47, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Doll, C.; Nack, C.; Raguse, J.D.; Stricker, A.; Duttenhoefer, F.; Nelson, K.; Nahles, S. Survival analysis of dental implants and implant-retained prostheses in oral cancer patients up to 20 years. Clin. Oral Investig. 2015, 19, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Zen Filho, E.V.; Tolentino Ede, S.; Santos, P.S. Viability of dental implants in head and neck irradiated patients: A systematic review. Head Neck 2016, 38, 2229–2240. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Epstein, J.B.; Sroussi, H. Hyposalivation in elderly patients. J. Can. Dent. Assoc. 2006, 72, 841–846. [Google Scholar]
- Muñoz-González, C.; Vandenberghe-Descamps, M.; Feron, G.; Canon, F.; Labouré, H.; Sulmont- Rossé, C. Association between salivary hypofunction and food consumption in the elderlies. A systematic literature review. J. Nutr. Health Aging 2018, 22, 407–419. [Google Scholar] [CrossRef]
- Ettl, T.; Weindler, J.; Gosau, M.; Müller, S.; Hautmann, M.; Zeman, F.; Koller, M.; Papavasileiou, D.; Bürgers, R.; Driemel, O.; et al. Impact of radiotherapy on implant-based prosthetic rehabilitation in patients with head and neck cancer: A prospective observational study on implant survival and quality of life-Preliminary results. J. Cranio-Maxillofac. Surg. 2016, 44, 1453–1462. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, S.; De Angelis, F.; Ciolfi, A.; Quarato, A.; Piccoli, L.; Pompa, G.; Brauner, E. Timing for implant placement in patients treated with radiotherapy of head and neck. Clin. Ter. 2019, 170, e345–e351. [Google Scholar]
- Ch’ng, S.; Skoracki, R.J.; Selber, J.C.; Yu, P.; Martin, J.W.; Hofstede, T.M.; Chambers, M.S.; Liu, J.; Hanasono, M.M. Osseointegrated implant-based dental rehabilitation in head and neck reconstruction patients. Head Neck 2016, 38 (Suppl. 1), E321–E327. [Google Scholar] [CrossRef]
- ArRejaie, A.S.; Al-Aali, K.A.; Alrabiah, M.; Vohra, F.; Mokeem, S.A.; Basunbul, G.; Alrahlah, A.; Abduljabbar, T. Proinflammatory cytokine levels and peri-implant parameters among cigarette smokers, individuals vaping electronic cigarettes, and non-smokers. J. Periodontol. 2019, 90, 367–374. [Google Scholar] [CrossRef]
- Javed, F.; Rahman, I.; Romanos, G.E. Tobacco-product usage as a risk factor for dental implants. Periodontol. 2000 2019, 81, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Kovács, A.F. Influence of chemotherapy on endosteal implant survival and success in oral cancer patients. Int. J. Oral Maxillofac. Surg. 2001, 30, 144–147. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Localization | ICD-10 | UICC-Stadium | Number (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV A | IV B | IV C | n.d. | |||
| Nasopharynx | C11, C30, and C31 | 0 | 1 | 0 | 2 | 2 | 0 | 2 | 7 (5.9) |
| Tonsil | C09 and C10 | 0 | 2 | 1 | 6 | 4 | 0 | 1 | 14 (11.9) |
| Tongue base | C01 | 0 | 2 | 1 | 4 | 0 | 0 | 1 | 8 (6.8) |
| Oral cavity | C00, C02-C06, and C08 | 9 | 13 | 11 | 12 | 6 | 1 | 5 | 57 (48.3) |
| Cheek/parotid gland | C06 and C07 | 3 | 1 | 3 | 1 | 0 | 0 | 0 | 8 (6.8) |
| Larynx/hypopharynx | C12, C13, and C32 | 0 | 5 | 4 | 7 | 0 | 0 | 0 | 16 (13.6) |
| Others | C41, C49, C80, and D18 | 1 | 0 | 0 | 2 | 2 | 0 | 3 | 8 (6.8) |
| Number (percent) | 13 (11.0) | 23 (19.5) | 21 (17.8) | 34 (28.8) | 14 (11.9) | 1 (0.8) | 12 (10.2) | 118 (100) | |
| Variable | Reference | Hazard Ratio | 95% CI | p-Value | |
|---|---|---|---|---|---|
| Age | - | 1.024 | 0.970 | 1.081 | 0.384 |
| Sex | Male | 4.106 | 1.357 | 12.423 | 0.012 |
| SFR | - | 1.637 | 0.706 | 3.797 | 0.251 |
| RT | No RT | 0.347 | 0.094 | 1.282 | 0.113 |
| Nicotine abuse | No nicotine abuse | 2.670 | 0.847 | 8.417 | 0.094 |
| Implant position | Mandible | 1.830 | 0.816 | 4.103 | 0.143 |
| Intraoral defect | No intraoral defect | 9.117 | 0.878 | 94.720 | 0.064 |
| Implant site | Autogenous bone | 0.367 | 0.078 | 1.738 | 0.207 |
| Chemotherapy | No chemotherapy | 4.127 | 1.240 | 13.738 | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schweyen, R.; Reich, W.; Jevnikar, P.; Kuhnt, T.; Wienke, A.; Hey, J. Factors Influencing the Survival Rate of Teeth and Implants in Patients after Tumor Therapy to the Head and Neck Region—Part 2: Implant Survival. J. Clin. Med. 2022, 11, 6319. https://doi.org/10.3390/jcm11216319
Schweyen R, Reich W, Jevnikar P, Kuhnt T, Wienke A, Hey J. Factors Influencing the Survival Rate of Teeth and Implants in Patients after Tumor Therapy to the Head and Neck Region—Part 2: Implant Survival. Journal of Clinical Medicine. 2022; 11(21):6319. https://doi.org/10.3390/jcm11216319
Chicago/Turabian StyleSchweyen, Ramona, Waldemar Reich, Peter Jevnikar, Thomas Kuhnt, Andreas Wienke, and Jeremias Hey. 2022. "Factors Influencing the Survival Rate of Teeth and Implants in Patients after Tumor Therapy to the Head and Neck Region—Part 2: Implant Survival" Journal of Clinical Medicine 11, no. 21: 6319. https://doi.org/10.3390/jcm11216319
APA StyleSchweyen, R., Reich, W., Jevnikar, P., Kuhnt, T., Wienke, A., & Hey, J. (2022). Factors Influencing the Survival Rate of Teeth and Implants in Patients after Tumor Therapy to the Head and Neck Region—Part 2: Implant Survival. Journal of Clinical Medicine, 11(21), 6319. https://doi.org/10.3390/jcm11216319