

Tracheal Intubation during Advanced Life Support Using Direct Laryngoscopy versus Glidescope® Videolaryngoscopy by Clinicians with Limited Intubation Experience: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- Comparison of direct laryngoscopy to Glidescope® videolaryngoscopy (either conventional Glidescope® or Glidescope® Ranger) for tracheal intubation
- Randomized and quasi-randomized controlled trials
- Clinicians had limited experience in tracheal intubation, defined as less than 10 intubations per year
- Adult patients or adult-sized manikins
- Contained any outcome of interest (first-pass success rate, and/or time to intubation, and/or hands-off time during CPR)
2.2. Information Sources and Search Strategy
2.3. Study Selection
2.4. Data Collection and Data Items
2.5. Risk of Bias in Individual Studies
2.6. Data Synthesis and Analysis
- Intubations performed in the clinical setting
- Intubations performed in a simulation setting, using manikins
- Intubations performed in a simulation setting, using manikins with a difficult airway scenario
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Certainty of Evidence across Studies
3.4. Risk of Bias within Studies
3.5. Outcomes
3.5.1. Intubation First-Pass Success Rate
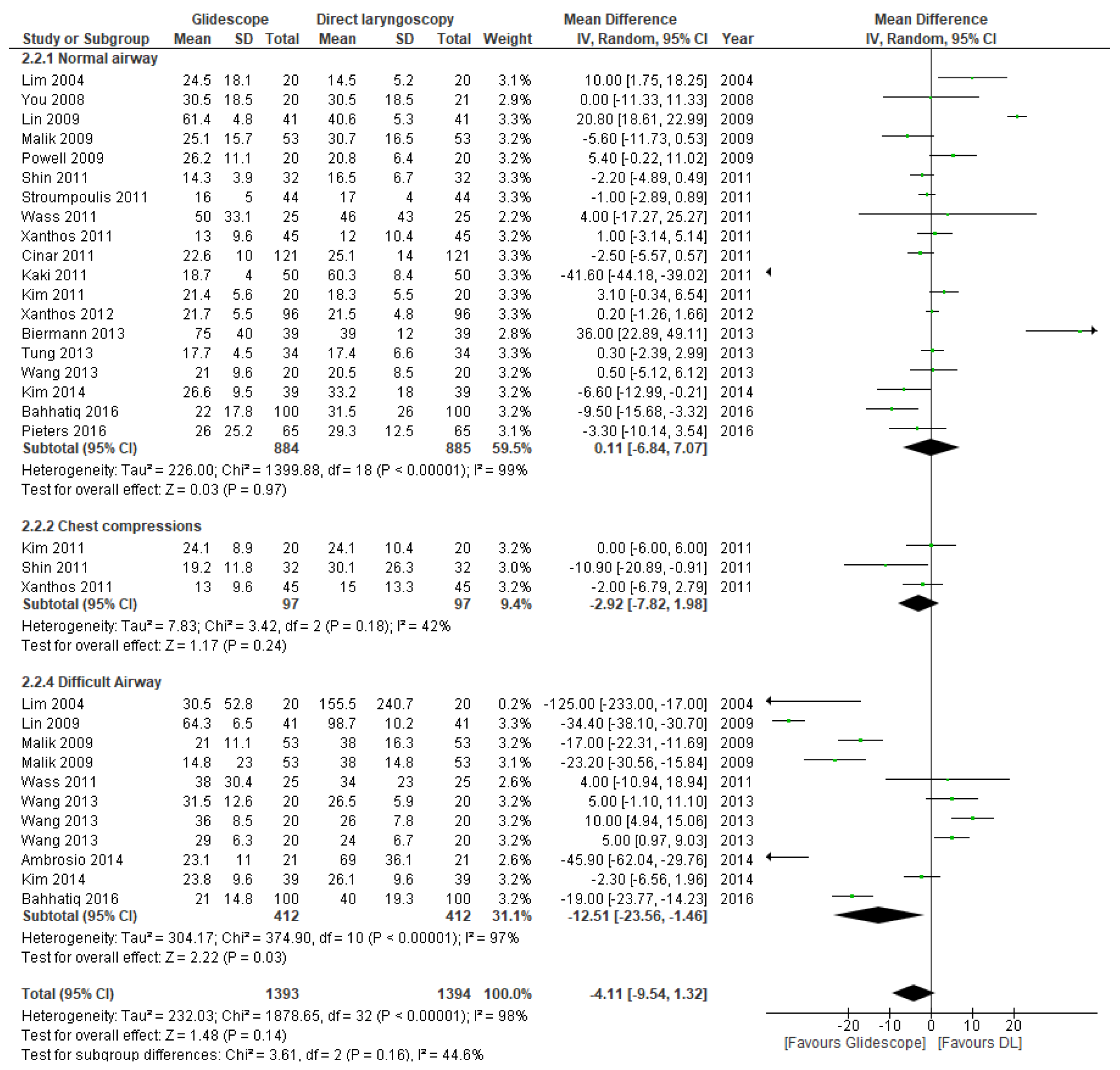
3.5.2. Time to Intubation
3.5.3. Intubation during Cardiopulmonary Resuscitation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Liaison Committee on Resuscitation (ILCOR). COVID-19—Practical Guidance for Implementation. Available online: https://www.ilcor.org/covid-19 (accessed on 31 January 2022).
- Somri, M.; Gaitini, L.; Gat, M.; Sonallah, M.; Paz, A.; Gómez-Ríos, M. Cardiopulmonary Resuscitation during the COVID-19 pandemic. Do supraglottic airways protect against aerosol-generation? Resuscitation 2020, 157, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.E.; Roppolo, L.P.; Fowler, R.L. Prehospital endotracheal intubation: Elemental or detrimental? Crit. Care 2015, 19, 121. [Google Scholar] [CrossRef] [PubMed]
- Crewdson, K.; Lockey, D.J.; Røislien, J.; Lossius, H.M.; Rehn, M. The success of pre-hospital tracheal intubation by different pre-hospital providers: A systematic literature review and meta-analysis. Crit. Care 2017, 21, 31. [Google Scholar] [CrossRef] [PubMed]
- Pilbery, R. How do paramedics learn and maintain the skill of tracheal intubation? A rapid evidence review. Br. Paramed. J. 2018, 3, 7–21. [Google Scholar] [CrossRef]
- Buis, M.L.; Maissan, I.M.; Hoeks, S.E.; Klimek, M.; Stolker, R.J. Defining the learning curve for endotracheal intubation using direct laryngoscopy: A systematic review. Resuscitation 2016, 99, 63–71. [Google Scholar] [CrossRef]
- Kim, S.Y.; Park, S.O.; Kim, J.W.; Sung, J.; Lee, K.R.; Lee, Y.H.; Hong, D.Y.; Baek, K.J. How much experience do rescuers require to achieve successful tracheal intubation during cardiopulmonary resuscitation? Resuscitation 2018, 133, 187–192. [Google Scholar] [CrossRef]
- Deakin, C.D.; King, P.; Thompson, F. Prehospital advanced airway management by ambulance technicians and paramedics: Is clinical practice sufficient to maintain skills? Emerg. Med. J. 2009, 26, 888–891. [Google Scholar] [CrossRef]
- Dyson, K.; Bray, J.E.; Smith, K.; Bernard, S.; Straney, L.; Nair, R.; Finn, J. Paramedic Intubation Experience Is Associated With Successful Tube Placement but Not Cardiac Arrest Survival. Ann. Emerg. Med. 2017, 70, 382–390.e1. [Google Scholar] [CrossRef]
- Mort, T.C. Emergency tracheal intubation: Complications associated with repeated laryngoscopic attempts. Anesth. Analg. 2004, 99, 607–613. [Google Scholar] [CrossRef]
- Chrimes, N.; Higgs, A.; Hagberg, C.A.; Baker, P.A.; Cooper, R.M.; Greif, R.; Kovacs, G.; Law, J.A.; Marshall, S.D.; Myatra, S.N.; et al. Preventing unrecognised oesophageal intubation: A consensus guideline from the Project for Universal Management of Airways and international airway societies. Anaesthesia 2022. [online ahead of print]. [Google Scholar] [CrossRef]
- Wang, H.E.; Simeone, S.J.; Weaver, M.D.; Callaway, C.W. Interruptions in cardiopulmonary resuscitation from paramedic endotracheal intubation. Ann. Emerg. Med. 2009, 54, 645–652.e1. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. (Eds.) GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations; Updated October 2013; The GRADE Working Group: Singapore, 2013. [Google Scholar]
- Lim, Y.; Lim, T.J.; Liu, E.H.C. Ease of intubation with the GlideScope or Macintosh laryngoscope by inexperienced operators in simulated difficult airways. Can. J. Anesth. 2004, 51, 641–642. [Google Scholar] [CrossRef]
- Lin, P.C.; Ong, J.; Lee, C.-L.; Chen, T.-Y.; Lee, Y.; Lai, H.-Y. Comparisons of the GlideScope and Macintosh laryngoscope in tracheal intubation by medical students on fresh human cadavers. Tzu Chi Med. J. 2009, 21, 147–150. [Google Scholar] [CrossRef]
- Malik, M.A.; Hassett, P.; Carney, J.; Higgins, B.D.; Harte, B.H.; Laffey, J.G. A comparison of the Glidescope, Pentax AWS, and Macintosh laryngoscopes when used by novice personnel: A manikin study. Can. J. Anaesth. 2009, 56, 802–811. [Google Scholar] [CrossRef]
- Powell, L.; Andrzejowski, J.; Taylor, R.; Turnbull, D. Comparison of the performance of four laryngoscopes in a high-fidelity simulator using normal and difficult airway. Br. J. Anaesth. 2009, 103, 755–760. [Google Scholar] [CrossRef][Green Version]
- You, J.S.; Park, S.; Chung, S.P.; Park, Y.S.; Park, J.W. The usefulness of the GlideScope video laryngoscope in the education of conventional tracheal intubation for the novice. Emerg. Med. J. 2009, 26, 109–111. [Google Scholar] [CrossRef]
- Cinar, O.; Cevik, E.; Yildirim, A.O.; Yasar, M.; Kilic, E.; Comert, B. Comparison of GlideScope video laryngoscope and intubating laryngeal mask airway with direct laryngoscopy for endotracheal intubation. Eur J. Emerg. Med. 2011, 18, 117–120. [Google Scholar] [CrossRef]
- Kaki, A.M.; Almarakbi, W.A.; Fawzi, H.M.; Boker, A.M. Use of Airtraq, C-Mac, and Glidescope laryngoscope is better than Macintosh in novice medical students’ hands: A manikin study. Saudi J. Anaesth. 2011, 5, 376–381. [Google Scholar] [CrossRef]
- Kim, Y.M.; Kang, H.G.; Kim, J.H.; Chung, H.S.; Yim, H.W.; Jeong, S.H. Direct versus video laryngoscopic intubation by novice prehospital intubators with and without chest compressions: A pilot manikin study. Prehosp. Emerg. Care 2011, 15, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Wass, T.C.; Jacob, A.K.; Kopp, S.L.; Torscher, L.C. A prospective randomized high fidelity simulation center based side-by-side comparison analyzing the success and ease of conventional versus new generation video laryngoscope technology by inexperienced laryngoscopists. Signa Vitae J. Intesive Care Emerg. Med. 2011, 6, 36–45. [Google Scholar]
- Shin, D.H.; Choi, P.C.; Han, S.K. Tracheal intubation during chest compressions using Pentax-AWS (®), GlideScope (®), and Macintosh laryngoscope: A randomized crossover trial using a mannequin. Can. J. Anaesth. 2011, 58, 733–739. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stroumpoulis, K.; Xanthos, T.; Bassiakou, E.; Iacovidou, N.; Koudouna, E.; Michaloliakou, C.; Papadimitriou, L. Macintosh and Glidescope® performance by Advanced Cardiac Life Support providers: A manikin study. Minerva Anestesiol. 2011, 77, 11–16. [Google Scholar] [PubMed]
- Xanthos, T.; Stroumpoulis, K.; Bassiakou, E.; Koudouna, E.; Pantazopoulos, I.; Mazarakis, A.; Demestiha, T.; Iacovidou, N. Glidescope(®) videolaryngoscope improves intubation success rate in cardiac arrest scenarios without chest compressions interruption: A randomized cross-over manikin study. Resuscitation 2011, 82, 464–467. [Google Scholar] [CrossRef] [PubMed]
- Xanthos, T.; Bassiakou, E.; Koudouna, E.; Stroumpoulis, K.; Vlachos, I.; Johnson, E.O.; Vasileiou, P.; Papalois, A.; Iacovidou, N. Inexperienced nurses and doctors are equally efficient in managing the airway in a manikin model. Heart Lung 2012, 41, 161–166. [Google Scholar] [CrossRef]
- Biermann, H.; van der Heiden, E.; Beishuizen, A.; Girbes, A.R.J.; de Waard, M.C. Endotracheal intubation by inexperienced registrars in internal medicine: A comparison of video-laryngoscopy versus direct laryngoscopy. Neth. J. Crit. Care 2013, 17, 7–9. [Google Scholar]
- Tung, A.; Griesdale, D.E. Comparing the novel GlideScope Groove videolaryngoscope with conventional videolaryngoscopy: A randomized mannequin study of novice providers. J. Clin. Anesth. 2013, 25, 644–650. [Google Scholar] [CrossRef]
- Wang, P.K.; Huang, C.C.; Lee, Y.; Chen, T.Y.; Lai, H.Y. Comparison of 3 video laryngoscopes with the Macintosh in a manikin with easy and difficult simulated airways. Am. J. Emerg. Med. 2013, 31, 330–338. [Google Scholar] [CrossRef]
- Ambrosio, A.; Pfannenstiel, T.; Bach, K.; Cornelissen, C.; Gaconnet, C.; Brigger, M.T. Difficult airway management for novice physicians: A randomized trial comparing direct and video-assisted laryngoscopy. Otolaryngol. Head Neck Surg. 2014, 150, 775–778. [Google Scholar] [CrossRef]
- Kim, W.; Choi, H.J.; Lim, T.; Kang, B.S. Can the new McGrath laryngoscope rival the GlideScope Ranger portable video laryngoscope? A randomized manikin study. Am. J. Emerg. Med. 2014, 32, 1225–1229. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bahathiq, A.O.; Abdelmontaleb, T.H.; Newigy, M.K. Learning and performance of endotracheal intubation by paramedical students: Comparison of GlideScope (®) and intubating laryngeal mask airway with direct laryngoscopy in manikins. Indian J. Anaesth. 2016, 60, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Pieters, B.M.; Wilbers, N.E.; Huijzer, M.; Winkens, B.; van Zundert, A.A. Comparison of seven videolaryngoscopes with the Macintosh laryngoscope in manikins by experienced and novice personnel. Anaesthesia 2016, 71, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, C.M.; Kanazi, G.E.; Al Alami, A.; Rameh, C.; El-Khatib, M.F. Tracheal intubation following training with the GlideScope compared to direct laryngoscopy. Anaesthesia 2010, 65, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, Y.; Otsuka, Y.; Seo, N. GlideScope videolaryngoscope reduces the incidence of erroneous esophageal intubation by novice laryngoscopists. J. Anesth. 2010, 24, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Nouruzi-Sedeh, P.; Schumann, M.; Groeben, H. Laryngoscopy via Macintosh blade versus GlideScope: Success rate and time for endotracheal intubation in untrained medical personnel. Anesthesiology 2009, 110, 32–37. [Google Scholar] [CrossRef]
- Park, S.O.; Kim, J.W.; Na, J.H.; Lee, K.H.; Lee, K.R.; Hong, D.Y.; Baek, K.J. Video laryngoscopy improves the first-attempt success in endotracheal intubation during cardiopulmonary resuscitation among novice physicians. Resuscitation 2015, 89, 188–194. [Google Scholar] [CrossRef]
- Reade, M.C.; Delaney, A.; Bailey, M.J.; Angus, D.C. Bench-to-bedside review: Avoiding pitfalls in critical care meta-analysis--funnel plots, risk estimates, types of heterogeneity, baseline risk and the ecologic fallacy. Crit. Care 2008, 12, 220. [Google Scholar] [CrossRef]
- Rai, M.R.; Popat, M.T. Evaluation of airway equipment: Man or manikin? Anaesthesia 2011, 66, 529. [Google Scholar] [CrossRef]
- Arulkumaran, N.; Lowe, J.; Ions, R.; Mendoza, M.; Bennett, V.; Dunser, M.W. Videolaryngoscopy versus direct laryngoscopy for emergency orotracheal intubation outside the operating room: A systematic review and meta-analysis. Br. J. Anaesth. 2018, 120, 712–724. [Google Scholar] [CrossRef]
- Griesdale, D.E.; Liu, D.; McKinney, J.; Choi, P.T. Glidescope® video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: A systematic review and meta-analysis. Can. J. Anaesth. 2012, 59, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Shimada, N.; Hirabayashi, Y.; Otsuka, Y.; Urayama, M.; Yokotsuka, C.; Yamanaka, A.; Takeuchi, M. GlideScope Ranger: Clinical assessment of the performance in 100 patients. Masui 2011, 60, 1314–1316. [Google Scholar]
- Soar, J.; Berg, K.M.; Andersen, L.W.; Böttiger, B.W.; Cacciola, S.; Callaway, C.W.; Couper, K.; Cronberg, T.; D’Arrigo, S.; Deakin, C.D.; et al. Adult Advanced Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2020, 156, A80–A119. [Google Scholar] [CrossRef]
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djärv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation 2021, 161, 115–151. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.E.; Yealy, D.M. How many attempts are required to accomplish out-of-hospital endotracheal intubation? Acad. Emerg. Med. 2006, 13, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Benger, J.R.; Kirby, K.; Black, S.; Brett, S.J.; Clout, M.; Lazaroo, M.J.; Nolan, J.P.; Reeves, B.C.; Robinson, M.; Scott, L.J.; et al. Effect of a Strategy of a Supraglottic Airway Device vs Tracheal Intubation During Out-of-Hospital Cardiac Arrest on Functional Outcome: The AIRWAYS-2 Randomized Clinical Trial. JAMA 2018, 320, 779–791. [Google Scholar] [CrossRef]
- Murphy, D.L.; Bulger, N.E.; Harrington, B.M.; Skerchak, J.A.; Counts, C.R.; Latimer, A.J.; Yang, B.Y.; Maynard, C.; Rea, T.D.; Sayre, M.R. Fewer tracheal intubation attempts are associated with improved neurologically intact survival following out-of-hospital cardiac arrest. Resuscitation 2021, 167, 289–296. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical studies | ||||||
| First author, year | Country of origin | Number of patients | Randomized per group | Operators | Training | Patients |
| Nouruzi, 2009 [38] | Essen, Germany | 200 | DL: 100 GS: 100 | Students (paramedic, nurse & medical) | Manikin training | ASA 1–2 predicted non difficult airway |
| Ayoub, 2010 [36] | Beirut, Lebanon | 42 | DL: 21 GS: 21 | Medical students | Manikin training | ASA 1–2 predicted non difficult airway |
| Hirabayashi, 2010 [37] | Shimotsuke, Japan | 200 | DL: 100 GS: 100 | Non-anaesthesia residents | Short demonstration and 5–6 practices on a manikin | ASA 1–2 predicted non difficult airway |
| Park, 2015 [39] | Seoul, Republic of Korea | 83 | DL: 34 GS: 49 | Inexperienced emergency physicians | Airway session of 8 h | CPR patients |
| 4 | 525 | DL: 255 GS: 270 | ||||
| Manikin studies | ||||||
| First author, year | Country of origin | Number of intubations | Randomized per group | Operators | Training | Scenario |
| Lim, 2004 [16] | Singapore | 80 | DL: 20 GS: 20 | Medical students | Instructions and 3 min practice | Normal airway CL grade 3 |
| You, 2009 [20] | Ulsan, Korea | 41 | DL: 20 GS: 21 | Medical students | Lecture of 30 min | Normal airway |
| Lin, 2009 [17] | Hualien, Taiwan | 164 | DL: 41 GS: 41 | Medical students | Instructions and 5 attempts with both devices | Normal airway CL grade 3 |
| Malik, 2009 [18] | Galway, Ireland | 318 | DL: 53 * GS: 53 * | Medical students | Instruction of 5 min and 5 attempts | Normal airway Cervical immobilisation Pharyngeal obstruction |
| Powell, 2009 [19] | Sheffield, UK | 42 | DL: 21 GS: 21 | Non-anaesthesists | Individual standard demonstration | Normal airway |
| Cinar, 2011 [21] | Ankara, Turkey | 242 | DL: 121 GS: 121 | Paramedic students | Lecture and demonstration | Normal airway |
| Kaki, 2011 [22] | Jeddah, Saudi Arabia | 100 | DL: 50 GS: 50 | Non-anaesthesists | Standardized instruction and practice | Normal airway |
| Kim, 2011 [23] | Seoul, Republic of Korea | 80 | DL: 20 GS: 20 | Paramedic students | Training of one hour | Normal airway CPR on the floor |
| Shin, 2011 [25] | Seoul, Republic of Korea | 128 | DL: 32 GS: 32 | Interns with <10 tracheal intubations | Instruction of 20 min and 3 intubations on a manikin | Normal airway Chest compressions |
| Stroumpoulis, 2011 [26] | Athens, Greece | 88 | DL: 44 GS: 44 | ACLS providers | Brief presentation and 5 min of practice | Normal airway |
| Wass, 2011 [24] | Rochester, USA | 100 | DL: 25 GS: 25 | Medical students | Tutorial of 5–10 min | Normal airway Pharyngeal obstruction |
| Xanthos, 2011 [27] | Athens, Greece | 180 | DL: 45 GS: 45 | Doctors inexperienced in airway management | Instruction of 20 min and practice on manikin | Normal airway Chest compressions |
| Xanthos, 2012 [28] | Athens, Greece | 192 | DL: 96 GS: 96 | Medical and nursing graduates | Instruction of 20 min and practice on manikin | Normal airway |
| Biermann, 2013 [29] | Amsterdam, the Netherlands | 78 | DL: 39 GS: 39 | Unexperienced registrars in internal medicine | Explanation and demonstration | Normal airway |
| Tung, 2013 [30] | Vancouver, Canada | 68 | DL: 34 GS: 34 | Medical students | Standardized video instruction and 10 min of practice | Normal airway |
| Wang, 2013 [31] | Hualien, Taiwan | 120 | DL: 20 GS: 20 | Medical students | Demonstration of 3–5 min and practice 1–3 times on bodies | Normal airway On the floor Cervical immobilisation Cervical immobilisation on the floor |
| Ambrosio, 2014 [32] | San Diego, USA | 40 | DL: 19 GS: 21 | First-year non anaesthesia residents | Manikin training, ended upon 1 successfull intubation with both DL and Glidescope® | CL grade 3 + cervical immobilisation |
| Kim, 2014 [33] | Seoul, Republic of Korea | 156 | DL: 39 GS: 39 | Medical students | 5 intubations | Normal airway Cervical immobilisation |
| Bahhatiq, 2016 [34] | Makkah Mukarramah, Saudi Arabia | 200 | DL: 50 GS: 50 | Paramedic students | Lecture of one hour, demonstration of 10 min and practice one time | Normal airway Cervical immobilisation |
| Pieters, 2016 [35] | Nijmegen, the Netherlands | 130 | DL: 65 GS: 65 | Medical students | Demonstration of 5 min, no practice | Normal airway |
| 20 | 2547 | DL: 1273 GS: 1274 | ||||
| Successful First Intubation Attempt | Time to Intubation (sec.) +/- SD | |||||
|---|---|---|---|---|---|---|
| First Author, Year | Direct Laryngoscopy | Glidescope® | P | Direct Laryngoscopy | Glidescope® | P |
| Clinical studies | ||||||
| Nouruzi, 2009 [38] | 51/100 (51.0%) | 93/100 (93.0%) | p < 0.001 | 89.0 +/- 35.0 | 63.0 +/- 30.0 | p < 0.01 |
| Ayoub, 2010 [36] | 3/21 (14.3%) | 10/21 (47.6%) | p = 0.04 | 70.7 +/- 7.50 | 59.3 +/- 4.4 | p = 0.006 |
| Hirabayashi, 2010 [37] | 77/100 (77.0%) | 94/100 (94.0%) | p = 0.03 | 72.0 +/- 47.0 | 64.0 +/- 33.0 | p = 0.13 |
| Park, 2015 [39] | 19/34 (55.9%) | 45/49 (91.8%) | p < 0.001 | 62.0 +/- 40.0 | 37.0 +/- 19.3 | p < 0.001 |
| Manikin with normal airway | ||||||
| Lim, 2004 [16] | 19/20 (95.0%) | 20/20 (100%) | p = 1 | 14.5 +/- 5.20 | 24.5 +/- 18.1 | p = 0.02 |
| You, 2009 [20] | 11/21 (55.0%) | 12/20 (57.0%) | p > 0.05 | 30.5 +/- 18.5 | 26.6 +/- 14.3 | p = 0.35 |
| Lin, 2009 [17] | 36/41 (87.8%) | 35/41 (85.3%) | p = 1 | 40.6 +/- 5.30 | 61.4 +/- 4.80 | p < 0.001 |
| Malik, 2009 * [18] | 49/53 (92.4%) | 51/53 (96.2%) | p = 0.68 | 30.7 +/- 16.5 | 25.1 +/- 15.7 | p = 0.08 |
| Powell, 2009 [19] | 18/20 (90.0%) | 20/20 (100%) | p = 0.49 | 20.8 +/- 6.40 | 26.2 +/- 11.1 | p = 0.07 |
| Cinar, 2011 [21] | 95/121 (78.5%) | 111/121 (91.7%) | p = 0.006 | 25.1 +/- 14.0 | 22.6 +/- 10.0 | p = 0.11 |
| Kaki, 2011 [22] | 37/50 (74.0%) | 50/50 (100%) | p < 0.001 | 60.3 +/- 8.40 | 18.7 +/- 0.40 | p < 0.001 |
| Kim, 2011 [23] | 18/20 (90.0%) | 16/20 (80.0%) | p = 0.15 | 18.3 +/- 5.50 | 21.4 +/- 5.60 | p = 0.24 |
| Shin, 2011 [25] | 31/32 (96.9%) | 32/32 (100%) | p = 0.36 | 16.5 +/- 6.70 | 14.3 +/- 3.90 | p = 0.03 |
| Stroumpoulis, 2011 [26] | 12/44 (27.3%) | 29/44 (65.9%) | p < 0.001 | 17.0 +/- 4.00 | 16.0 +/- 5.00 | p > 0.05 |
| Wass, 2011 [24] | 20/25 (80.0%) | 25/25 (100%) | p = 0.05 | 46.0 +/- 43.0 | 50.0 +/- 33.1 | p = 0.71 |
| Xanthos, 2011 [27] | 33/45 (73.3%) | 45/45 (100%) | p = 0.001 | 12.0 +/- 10.4 | 13.0 +/- 9.60 | p = 0.64 |
| Xanthos, 2012 [28] | 26/96 (27.1%) | 28/96 (29.1%) | p = 0.87 | 21.5 +/- 4.80 | 21.7 +/- 5.50 | p = 0.79 |
| Biermann, 2013 [29] | 27/39 (69.2%) | 36/39 (92.3%) | p = 0.02 | 39.0 +/- 12.0 | 75.0 +/- 40.0 | p < 0.001 |
| Tung, 2013 [30] | 30/34 (88.2%) | 34/34 (100%) | p = 0.11 | 17.4 +/- 6.60 | 17.7 +/- 4.50 | p = 0.45 |
| Wang, 2013 [31] | 20/20 (100%) | 19/20 (95.0%) | p = 1 | 20.5 +/- 8.50 | 21.0 +/- 9.60 | p = 0.86 |
| Kim, 2014 [33] | 34/39 (87.1%) | 23/29 (58.9%) | p = 0.008 | 33.2 +/-18.0 | 26.6 +/- 9.50 | p = 0.18 |
| Bahhatiq, 2016 [34] | 68/100 (68.0%) | 91/100 (91.0%) | p < 0.001 | 31.5 +/- 26.0 | 22.0 +/- 17.8 | p < 0.001 |
| Pieters, 2016 [35] | 51/65 (78.4%) | 58/65 (89.2%) | p = 0.1 | 29.3 +/- 12.5 | 26.0 +/- 25.2 | p = 0.35 |
| Manikin with chest compressions | ||||||
| Shin, 2011 [25] | 24/32 (75.0%) | 31/32 (96.9%) | p = 0.01 | 30.1 +/- 26.3 | 19.2 +/- 11.8 | p = 0.006 |
| Xanthos, 2011 [27] | 20/45 (44.4%) | 43/45 (95.6%) | p < 0.001 | 15.0 +/- 13.3 | 13.0 +/- 9.60 | p = 0.42 |
| Manikin with chest compressions on the floor | ||||||
| Kim, 2011 [23] | 15/20 (75.0%) | 17/20 (85.0%) | p = 0.69 | 24.1 +/- 10.4 | 24.1 +/- 8.90 | p = 0.99 |
| Manikin with CL grade 3 | ||||||
| Lim, 2004 [16] | 14/20 (70.0%) | 19/20 (95.0%) | p = 0.09 | 156 +/- 241 | 30.5 +/- 52.8 | p < 0.001 |
| Lin, 2009 [17] | 18/41 (43.9%) | 36/41 (87.8%) | p < 0.001 | 98.7 +/- 10.2 | 64.3 +/- 6.50 | p < 0.001 |
| Manikin with cervical immobilisation | ||||||
| Malik, 2009 [18] | 47/53 (88.7%) | 49/53 (92.5%) | p = 0.74 | 38.0 +/- 14.8 | 23.0 +/- 14.8 | p < 0.001 |
| Wang, 2013 [31] | 20/20 (100%) | 17/20 (85.0%) | p = 0.23 | 26.5 +/- 5.90 | 31.5 +/- 12.6 | p = 0.12 |
| Kim, 2014 [33] | 34/39 (87.1%) | 35/39 (89.7%) | p = 0.72 | 26.1 +/- 9.60 | 23.8 +/- 9.60 | p = 0.49 |
| Bahhatiq, 2016 [34] | 60/100 (60.0%) | 88/100 (88.0%) | p < 0.001 | 40.0 +/- 19.3 | 21.0 +/- 14.8 | p < 0.001 |
| Manikin with cervical immobilisation on the floor | ||||||
| Wang, 2013 [31] | 19/20 (95.0%) | 18/20 (90.0%) | p = 1 | 26.0 +/- 7.80 | 36.0 +/- 8.50 | p < 0.001 |
| Manikin with cervical immobilisation and CL grade 3 | ||||||
| Ambrosio, 2014 [32] | 9/19 (47.7%) | 21/21 (100%) | p < 0.001 | 69.0 +/- 36.1 | 23.1 +/- 11.0 | p < 0.001 |
| Manikin with pharyngeal obstruction | ||||||
| Malik, 2009 [18] | 33/53 (62.3%) | 48/53 (90.6%) | p = 0.001 | 38.0 +/- 16.3 | 21.0 +/- 11.1 | p < 0.001 |
| Wass, 2011 [24] | 23/25 (92.0%) | 25/25 (100%) | p = 0.49 | 34.0 +/- 23.0 | 38.0 +/- 30.4 | p = 0.60 |
| Manikin on the floor | ||||||
| Wang, 2013 [31] | 20/20 (100%) | 20/20 (100%) | p = 1 | 24.0 +/- 6.70 | 29.0 +/- 6.30 | p = 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Schuppen, H.; Wojciechowicz, K.; Hollmann, M.W.; Preckel, B. Tracheal Intubation during Advanced Life Support Using Direct Laryngoscopy versus Glidescope® Videolaryngoscopy by Clinicians with Limited Intubation Experience: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 6291. https://doi.org/10.3390/jcm11216291
van Schuppen H, Wojciechowicz K, Hollmann MW, Preckel B. Tracheal Intubation during Advanced Life Support Using Direct Laryngoscopy versus Glidescope® Videolaryngoscopy by Clinicians with Limited Intubation Experience: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(21):6291. https://doi.org/10.3390/jcm11216291
Chicago/Turabian Stylevan Schuppen, Hans, Kamil Wojciechowicz, Markus W. Hollmann, and Benedikt Preckel. 2022. "Tracheal Intubation during Advanced Life Support Using Direct Laryngoscopy versus Glidescope® Videolaryngoscopy by Clinicians with Limited Intubation Experience: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 21: 6291. https://doi.org/10.3390/jcm11216291
APA Stylevan Schuppen, H., Wojciechowicz, K., Hollmann, M. W., & Preckel, B. (2022). Tracheal Intubation during Advanced Life Support Using Direct Laryngoscopy versus Glidescope® Videolaryngoscopy by Clinicians with Limited Intubation Experience: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(21), 6291. https://doi.org/10.3390/jcm11216291