
Complications and Implant Survival of Total Knee Arthroplasty in People with Hemophilia

 ,
,  , and
, and
Abstract
1. Introduction
2. Methods
3. Results
3.1. Published Series
3.2. Venous Thromboembolism (VTE)
3.3. Arterial Pseudoaneurysms
3.4. Case Reports
3.4.1. Intraoperative Popliteal Artery Injury
3.4.2. Brucella Infection
3.4.3. Postoperative Flexion Contracture
3.5. Is Drain after TKA Necessary?
3.6. Special Scenarios
3.6.1. Computer-Navigated TKA
3.6.2. Robot-Assisted TKA
3.6.3. TKA in Patients with Inhibitors
3.6.4. Simultaneous Bilateral TKA
3.6.5. Medicare Beneficiaries with a Diagnosis of Hemophilia
3.6.6. TKA for a Stiff Knee of PWH
3.7. Comparative Studies
3.7.1. Continuous Infusion versus Bolus Injection
3.7.2. Hemophilia versus Non-Hemophilia
3.7.3. Hemophilia versus Osteoarthritis and Rheumatoid Arthritis
3.8. Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mortazavi, S.J.; Bagheri, N.; Farhoud, A.; Hadi Kalantar, S.; Ghadimi, E. Total knee arthroplasty in patients with hemophilia: What do we know? Arch. Bone Jt. Surg. 2020, 8, 470–478. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C.; De la Corte-Rodriguez, H.; Alvarez-Roman, T.; Gomez-Cardero, P.; Encinas-Ullan, C.A.; Jimenez-Yuste, V. Total knee arthroplasty in hemophilia: Lessons learned and projections of what’s next for hemophilic knee joint health. Expert Rev. Hematol. 2022, 15, 65–82. [Google Scholar] [CrossRef]
- Jimenez-Yuste, V.; Rodriguez-Merchan, E.C.; Matsushita, T.; Holme, P.A. Concomitant use of bypassing agents with emicizumab for people with haemophilia A and inhibitors undergoing surgery. Haemophilia 2021, 27, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Hermans, C.; Apte, S.; Santagostino, E. Invasive procedures in patients with haemophilia: Review of low-dose protocols and experience with extended half-life FVIII and FIX concentrates and non-replacement therapies. Haemophilia 2021, 27 (Suppl. 3), 46–52. [Google Scholar] [CrossRef] [PubMed]
- Valentino, L.A.; Cooper, D.L.; Goldstein, B. Surgical Experience with rFVIIa (NovoSeven) in congenital haemophilia A and B patients with inhibitors to factors VIII or IX. Haemophilia 2011, 17, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Escobar, M.; Maahs, J.; Hellman, E.; Donkin, J.; Forsyth, A.; Hroma, N.; Young, G.; Valentino, L.A.; Tachdjian, R.; Cooper, D.L.; et al. Multidisciplinary management of patients with haemophilia with inhibitors undergoing surgery in the United States: Perspectives and best practices derived from experienced treatment centres. Haemophilia 2012, 18, 971–981. [Google Scholar] [CrossRef]
- Escobar, M.A.; Brewer, A.; Caviglia, H.; Forsyth, A.; Jimenez-Yuste, V.; Laudenbach, L.; Lobet, S.; McLaughlin, P.; Oyesiku, J.O.O.; Rodriguez-Merchan, E.C.; et al. Recommendations on multidisciplinary management of elective surgery in people with haemophilia. Haemophilia 2018, 24, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Ueyama, H.; Kanemoto, N.; Minoda, Y.; Yamamoto, N.; Taniguchi, Y.; Nakamura, H. No difference in postoperative knee flexion and patient joint awareness between cruciate-substituting and cruciate-retaining medial pivot total knee prostheses: A 10-year follow-pp study. J. Arthroplast. 2022, 37, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Park, J.W.; Jang, Y.S. 20-year minimum outcomes and survival rate of high-flexion versus standard total knee arthroplasty. J. Arthroplast. 2021, 36, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Feng, B.; Du, Y.; Wang, Y.; Bian, Y.; Weng, X. Complications of total knee arthroplasty in patients with haemophilia compared with osteoarthritis and rheumatoid arthritis: A 20-year single-surgeon cohort. Haemophilia 2020, 26, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Figgie, M.P.; Goldberg, V.M.; Figgie, H.E., 3rd; Heiple, K.G.; Sobel, M. Total knee arthroplasty for the treatment of chronic hemophilic arthropathy. Clin. Orthop. Relat. Res. 1989, 248, 98–107. [Google Scholar]
- Kjærsgaard-Andersen, P.; Christiansen, S.E.; Ingerslev, J.; Sneppen, O. Total knee arthroplasty in classic hemophilia. Clin. Orthop. Relat. Res. 1990, 256, 137–146. [Google Scholar] [CrossRef]
- Legroux-Gérot, I.; Strouk, G.; Parquet, A.; Goodemand, J.; Gougeon, F.; Duquesnoy, B. Total knee arthroplasty in hemophilic arthropathy. Jt. Bone Spine 2003, 70, 22–32. [Google Scholar] [CrossRef]
- Sheth, D.S.; Oldfield, D.; Ambrose, C.; Clyburn, T. Total knee arthroplasty in hemophilic arthropathy. J. Arthroplast. 2004, 19, 56–60. [Google Scholar] [CrossRef]
- Innocenti, M.; Civinini, R.; Carulli, C.; Villano, M.; Linari, S.; Morfini, M. A modular total knee arthroplasty in haemophilic arthropathy. Knee 2007, 14, 264–268. [Google Scholar] [CrossRef]
- Chiang, C.C.; Chen, P.Q.; Shen, M.C.; Tsai, W. Total knee arthroplasty for severe haemophilic arthropathy: Long-term experience in Taiwan. Haemophilia 2008, 14, 828–834. [Google Scholar] [CrossRef]
- Massin, P.; Lautridou, C.; Cappelli, M.; Petit, A.; Odri, G.; Ducellier, F.; Sabatier, C.; Hulet, C.; Canciani, J.; Letenneur, J.; et al. Total knee arthroplasty with limitations of flexion. Orthop. Traumatol. Surg. Res. 2009, 95 (Suppl. 1), S1–S6. [Google Scholar] [CrossRef][Green Version]
- Feng, B.; Weng, X.S.; Lin, J.; Qian, W.W.; Wei, W.; Sheng, L.; Zhai, J.-L.; Bian, Y.-Y.; Qiu, G.-X. Outcome of total knee arthroplasty combined patelloplasty for end-stage type A hemophilic arthropathy. Knee 2012, 19, 107–111. [Google Scholar] [CrossRef]
- Westberg, M.; Paus, A.C.; Holme, P.A.; Tjønnfjord, G.E. Haemophilic arthropathy: Long-term outcomes in 107 primary total knee arthroplasties. Knee 2014, 21, 147–150. [Google Scholar] [CrossRef]
- Strauss, A.C.; Schmolders, J.; Friedrich, M.J.; Pflugmacher, R.; Müller, M.; Goldmann, G.; Oldenburg, J.; Pennekamp, P.H. Outcome after total knee arthroplasty in haemophilic patients with stiff knees. Haemophilia 2015, 21, e300–e305. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C. Total knee arthroplasty in hemophilic arthropathy. Am. J. Orthop. 2015, 44, E503–E507. [Google Scholar] [PubMed]
- Ernstbrunner, L.; Hingsammer, A.; Catanzaro, S.; Sutter, R.; Brand, B.; Wieser, K.; Fucentese, S.F. Long-term results of total knee arthroplasty in haemophilic patients: An 18-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3431–3438. [Google Scholar] [CrossRef] [PubMed]
- Szmyd, J.; Jaworski, J.M.; Kaminski, P. Outcomes of total knee arthroplasty in patients with bleeding disorders. Ortop. Traumatol. Rehabil. 2017, 19, 361–371. [Google Scholar] [CrossRef] [PubMed]
- Song, S.J.; Bae, J.K.; Park, C.H.; Yoo, M.C.; Bae, D.K.; Kim, K.I. Mid-term outcomes and complications of total knee arthroplasty in haemophilic arthropathy: A review of consecutive 131 knees between 2006 and 2015 in a single institute. Haemophilia 2018, 24, 299–306. [Google Scholar] [CrossRef]
- Santos Silva, M.; Rodrigues-Pinto, R.; Rodrigues, C.; Morais, S.; Costa e Castro, J. Long-term results of total knee arthroplasty in hemophilic arthropathy. J. Orthop. Surg. 2019, 27, 2309499019834337. [Google Scholar] [CrossRef]
- Oyarzun, A.; Barrientos, C.; Barahona, M.; Martinez, A.; Soto-Arellano, V.; Courtin, C.; Cruz-Montecinos, C. Knee haemophilic arthropathy care in Chile: Midterm outcomes and complications after total knee arthroplasty. Haemophilia 2020, 26, e179–e186. [Google Scholar] [CrossRef]
- Bae, J.K.; Kim, K.I.; Lee, S.H.; Yoo, M.C. Mid-to long-term survival of total knee arthroplasty in hemophilic arthropathy. J. Clin. Med. 2020, 9, 3247. [Google Scholar] [CrossRef]
- Kleiboer, B.; Layer, M.A.; Cafuir, L.A.; Cuker, A.; Escobar, M.; Eyster, M.E.; Kraut, E.; Leavitt, A.D.; Lentz, S.R.; Quon, D.; et al. Postoperative bleeding complications in patients with hemophilia undergoing major orthopedic surgery: A prospective multicenter observational study. J. Thromb. Haemost. 2022, 20, 857–865. [Google Scholar] [CrossRef]
- Wang, R.; Wang, Z.; Gu, Y.; Zhang, J.; Wang, P.; Tong, P.; Lv, S. Total knee arthroplasty in patients with haemophilic arthropathy is effective and safe according to the outcomes at a mid-term follow-up. J. Orthop. Traumatol. 2022, 23, 31. [Google Scholar] [CrossRef]
- Chen, C.F.; Yu, Y.B.; Tsai, S.W.; Chiu, J.W.; Hsiao, L.T.; Gau, J.P.; Hsu, H.C. Total knee replacement for patients with severe hemophilic arthropathy in Taiwan: A nationwide population-based retrospective study. J. Chin. Med. Assoc. 2022, 85, 228–232. [Google Scholar] [CrossRef]
- Peng, H.-M.; Wang, L.-C.; Zhai, J.-L.; Jiang, C.; Weng, X.-S.; Feng, B.; Gao, N. Incidence of symptomatic venous thromboembolism in patients with hemophilia undergoing hip and knee joint replacement without chemoprophylaxis: A retrospective study. Orthop. Surg. 2019, 11, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Merchan, E.C.; Jimenez-Yuste, V.; Gomez-Cardero, P.; Rodriguez, T. Severe postoperative haemarthrosis following a total knee replacement in a haemophiliac patient caused by a pseudoaneurysm: Early treatment with arterial embolization. Haemophilia 2014, 20, e86–e89. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Merchan, E.C. Enormous articular hemorrhage following arthroscopy, total joint replacement and other surgical operations in hemophilic patients due to arterial pseudoaneurysms: Diagnosis and treatment. Arch. Bone Jt. Surg. 2021, 9, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Xiao, K.; Shao, J.; Fan, Y.; Weng, X. Open repair of intraoperative popliteal artery injury during total knee arthroplasty in a patient with severe hemophilia A: A case report and literature review. Medicine 2017, 96, e8791. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.M.J.; Sobhan, M.R.; Mazoochy, H. Brucella arthritis following total knee arthroplasty in a patient with hemophilia: A case report. Arch. Bone Jt. Surg. 2017, 5, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Liawrungrueang, W.; Tangtrakulwanich, B.; Yuenyongviwat, V. Soft tissue releasing and serial casting for management of flexion contracture after primary total knee arthroplasty in a patient with hemophilia. Int. J. Surg. Case Rep. 2021, 83, 105995. [Google Scholar] [CrossRef]
- Haghpanah, B.; Mortazavi, S.M.J.; Kaseb, M.H.; Ebrahiminasab, S.M. Drain after total knee arthroplasty in patients with hemophilia: A necessary practice? Haemophilia 2016, 22, 88. [Google Scholar]
- Mortazavi, S.M.J.; Firoozabadi, M.A.; Najafi, A.; Mansouri, P. Evaluation of outcomes of suction drainage in patients with haemophilic arthropathy undergoing total knee arthroplasty. Haemophilia 2017, 23, e310–e315. [Google Scholar] [CrossRef]
- Cho, K.Y.; Kim, K.I.; Khurana, S.; Cho, S.W.; Kang, D.G. Computer-navigated total knee arthroplasty in haemophilic arthropathy. Haemophilia 2013, 19, 259–266. [Google Scholar] [CrossRef]
- Kim, K.I.; Kim, D.K.; Juh, H.S.; Khurana, S.; Rhyu, K.H. Robot-assisted total knee arthroplasty in haemophilic arthropathy. Haemophilia 2016, 22, 446–452. [Google Scholar] [CrossRef]
- Carulli, C.; Innocenti, M.; Linari, S.; Morfini, M.; Castaman, G.; Innocenti, M. Joint replacement for the management of haemophilic arthropathy in patients with inhibitors: A long-term experience at a single Haemophilia centre. Haemophilia 2021, 27, e93–e101. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Zhao, Y.; Feng, B.; Zhai, J.; Bian, Y.; Qiu, G.; Weng, X. Simultaneous bilateral total knee arthroplasty in patients with end-stage hemophilic arthropathy: A mean follow-up of 6 years. Sci. Rep. 2018, 8, 1608. [Google Scholar] [CrossRef] [PubMed]
- Rosas, S.; Buller, L.T.; Plate, J.; Higuera, C.; Barsoum, W.K.; Emory, C. Total knee arthroplasty among Medicare beneficiaries with hemophilia A and B is associated with increased complications and higher costs. J. Knee Surg. 2021, 34, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Ono, K.; Hirose, J.; Noguchi, M.; Asano, K.; Yasuda, M.; Takedani, H. Extension contracture stiff knee in haemophilia: Surgical timing and procedure for total knee arthroplasty. Mod. Rheumatol. 2022, roac067. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.S.; Shin, W.J.; Kim, K.I. Comparison of continuous infusion versus bolus injection of factor concentrates for blood management after total knee arthroplasty in patients with hemophilia. BMC Musculoskelet. Disord. 2017, 18, 356. [Google Scholar] [CrossRef] [PubMed]
- Sikkema, T.; Boerboom, A.L.; Meijer, K. A comparison between the complications and long-term outcome of hip and knee replacement therapy in patients with and without haemophilia; a controlled retrospective cohort study. Haemophilia 2011, 17, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.H.; Chung, C.H.; Chen, Y.C.; Cooper, A.M.; Chien, W.C.; Pan, R.Y. Does hemophilia increase risk of adverse outcomes following total hip and knee arthroplasty? A propensity score–matched analysis of a nationwide, population-based study. J. Arthroplast. 2019, 34, 2329–2336.e1. [Google Scholar] [CrossRef]
- Moore, M.F.; Tobase, P.; Allen, D.D. Meta-analysis: Outcomes of total knee arthroplasty in the haemophilia population. Haemophilia 2016, 22, e275–e285. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C.; Encinas-Ullan, C.A.; Gomez-Cardero, P. Intra-articular tranexamic acid in primary total knee arthroplasty decreases the rate of post-operative blood transfusions in people with hemophilia: A retrospective case-control study. HSS J. Musculoskelet. J. Hosp. Spéc. Surg. 2020, 16, 218–221. [Google Scholar] [CrossRef]
- Mohan, K.; Broderick, J.M.; Raftery, N.; McAuley, N.F.; McCarthy, T.; Hogan, N. Perioperative haematological outcomes following total knee arthroplasty in haemophiliacs. J. Orthop. Surg. 2021, 29, 23094990211033999. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, J.H.; Kim, K.I. Risk factors for increased perioperative blood loss during total knee arthroplasty in patients with haemophilia. Haemophilia 2022, 28, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.W.; Park, C.H.; Bae, D.K.; Song, S.J. How much preoperative flexion contracture is a predictor for residual flexion contracture after total knee arthroplasty in hemophilic arthropathy and rheumatoid arthritis? Knee Surg. Relat. Res. 2022, 34, 20. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Hosseini, F.; Squire, S.; Jackson, S.; Sun, H.L. Trends of outcomes and healthcare utilization following orthopaedic procedures in adults with haemophilia: A 3-decade retrospective review. Haemophilia 2022, 28, 151–157. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors [Reference] | Year | Number of TKAs/Patients | Average Age (Years) | Average Follow-Up | Complications | TKA Survival Rate |
|---|---|---|---|---|---|---|
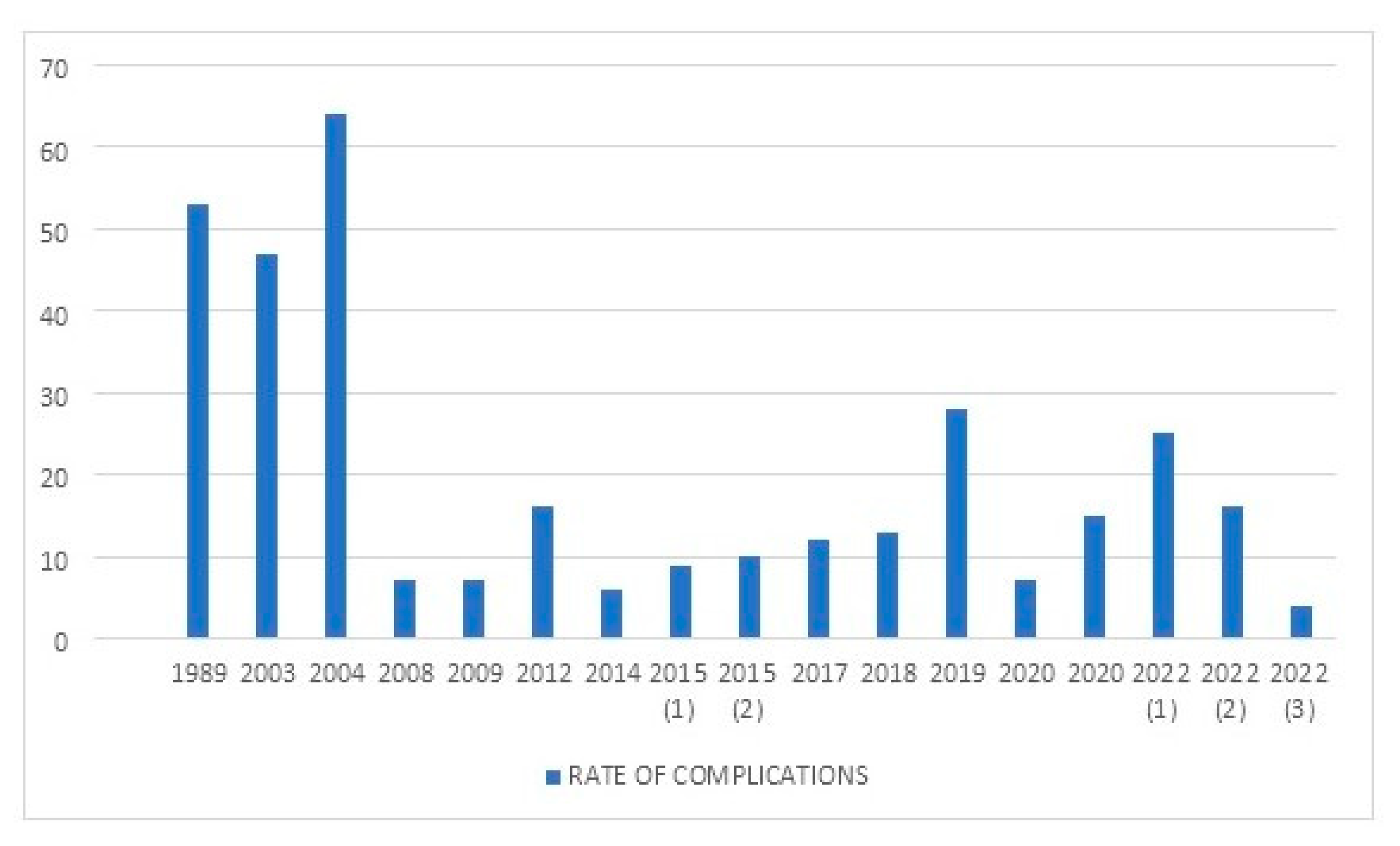
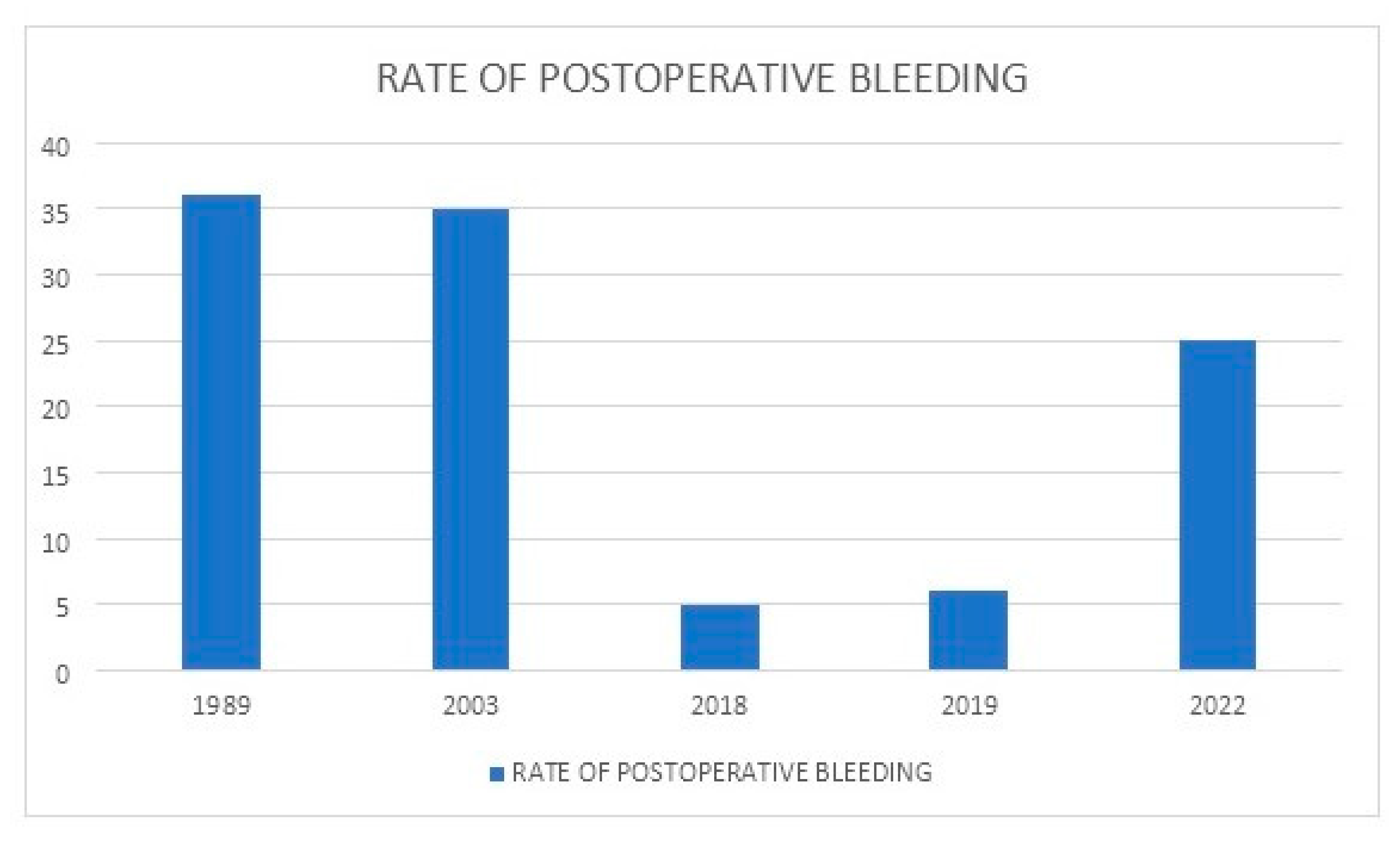
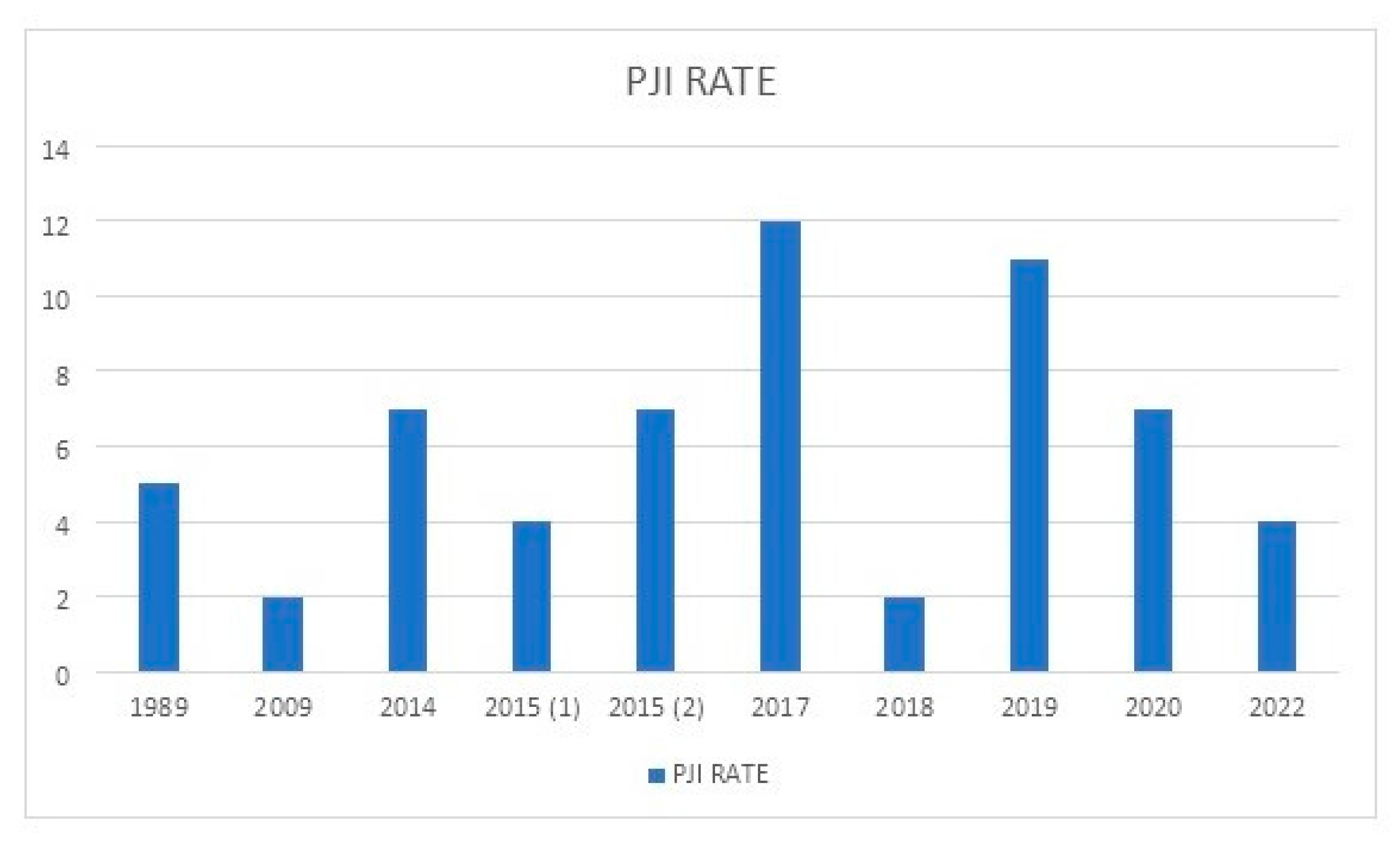
| Figgie et al. [11] | 1989 | 19/NA | NA | 9.5 years | RATE OF COMPLICATIONS: 52,6% (10/19: 1 PJI, 6 superficial skin necroses, 3 nerve palsies, 7 postoperative bleedings, 1 transfusion reaction). | NA |
| Kjaersgaard-Andersen et al. [12] | 1990 | 13/19 | 38 | 3.6 years | NA | NA |
| Legroux-Gérot et al. [13] | 2003 | 17/12 | 39 | 4.5 years | RATE OF COMPLICATIONS: 47% (recurrent hemarthrosis in 6 patients and development of an anticoagulant in 2 patients). | NA |
| Sheth et al. [14] | 2004 | 14/9 | NA | 6.4 years | RATE OF COMPLICATIONS: 64.3% (9/14). | NA |
| Innocenti et al. [15] | 2007 | 24/20 | 36 | 4.4 years | NA | NA |
| Chiang et al. [16] | 2008 | 35/26 | 34.2 | 6.8 years | RATE OF COMPLICATIONS: 7% (3 patients underwent MUA because of an inadequate ROM; 3 PJIs). | NA |
| Massin et al. [17] | 2009 | 128/NA | NA | NA | RATE OF COMPLICATIONS: 7% (3 skin necroses, 2 PJIs, 2 femoral fractures, 1 rupture of patellar tendon, 1 sciatic nerve palsy). | NA |
| Feng et al. [18] | 2012 | 25/19 | NA | 3.4 years | RATE OF COMPLICATIONS: 16% (4 patients complained mild but endurable anterior knee pain). | NA |
| Westberg et al. [19] | 2014 | 107/74 | NA | 11.2 years | RATE OF COMPLICATIONS: 6.5% (PJI in 7 knees). | FIVE-YEAR: 92%. TEN-YEAR: 88%. With component removal for any reason as the end point. |
| Strauss et al. [20] | 2015 | 23/21 | NA | 8.3 years | RATE OF COMPLICATIONS: 8.7% (1 late PJI, and 1 aseptic implant loosening; 9 patients who required VY-quadricepsplasty for knee exposure developed a mean postoperative extensor lag of 7°). | NA |
| Rodriguez-Merchan [21] | 2015 | 88/74 | 38.2 | 8 years | RATE OF COMPLICATIONS: 10% (PJI 6.8%; aseptic loosening 2.2%). | 92% (with implant removal for any reason regarded as final endpoint). |
| Ernstbrunner et al. [22] | 2017 | 43/30 | 58 | 18 years | RATE OF COMPLICATIONS: 12% (5 hematogenous PJIs). | 20-YEAR: 59% (with revision for any reason as the endpoint). 20-YEAR: 82% (with infection as the endpoint). |
| Szmyd et al. [23] | 2017 | 40/35 | 36.7 | 1.6 years | NA | NA |
| Song et al. [24] | 2018 | 131/NA | 41 | 6.8 years | RATE OF COMPLICATIONS: 13% (7 hemarthroses, 1 medial collateral ligament injury, 2 stiffness, 3 PJIs, 4 periprosthetic fractures). | NA |
| Santos Silva et al. [25] | 2019 | 18/15 | NA | 11.3 years | RATE OF COMPLICATIONS: 27.8% (2 PJIs, 2 prosthesis stiffness, 1 recurrent hemarthrosis). | 10-YEAR: 94.3% (with prosthesis removal as end point). |
| Oyarzun et al. [26] | 2020 | 41/22 | NA | NS | RATE OF COMPLICATIONS: 6.6% (6 PJIs). | 5-YEAR: 92% |
| Bae et al. [27] | 2020 | 78/56 | 38.7 | 10.2 years | RATE OF COMPLICATIONS: 15.4%. | 10-YEAR: 97.1%. 13-YEAR: 93.2%. |
| Kleiboer et al. [28] | 2022 | 98/NA | NA | NA | RATE OF COMPLICATIONS: 25% (major bleeding). | NA |
| Wang et al. [29] | 2022 | 32/28 | NA | 5.1 years | RATE OF COMPLICATIONS: 15.6%. | NA |
| Chen et al. [30] | 2022 | 103/75 | 32.3 | 6.5 years | RATE OF COMPLICATIONS: 3.9% (PJI). | 10-YEAR: 88.6%. |
| Complications |
|---|
| Postoperative bleeding |
| Early hematoma |
| Arterial pseudoaneurysm |
| Periprosthetic joint infection (PJI) |
| Superficial skin necrosis |
| Inadequate range of motion (ROM): postoperative extensor lag, stiffness, postoperative flexion contracture |
| Periprosthetic fracture |
| Nerve palsy |
| Popliteal artery injury |
| Rupture of the patellar tendon |
| Medial collateral ligament (MCL) injury |
| Heterotopic ossification |
| Deep vein thrombosis (DVT) |
| Pulmonary embolism |
| Transfusion reaction |
| Acquired immunodeficiency syndrome (AIDS) |
| Development of an inhibitor |
| Mild but endurable anterior knee pain |
| Aseptic loosening |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez-Merchan, E.C.; De la Corte-Rodriguez, H.; Alvarez-Roman, T.; Gomez-Cardero, P.; Encinas-Ullan, C.A.; Jimenez-Yuste, V. Complications and Implant Survival of Total Knee Arthroplasty in People with Hemophilia. J. Clin. Med. 2022, 11, 6244. https://doi.org/10.3390/jcm11216244
Rodriguez-Merchan EC, De la Corte-Rodriguez H, Alvarez-Roman T, Gomez-Cardero P, Encinas-Ullan CA, Jimenez-Yuste V. Complications and Implant Survival of Total Knee Arthroplasty in People with Hemophilia. Journal of Clinical Medicine. 2022; 11(21):6244. https://doi.org/10.3390/jcm11216244
Chicago/Turabian StyleRodriguez-Merchan, Emerito Carlos, Hortensia De la Corte-Rodriguez, Teresa Alvarez-Roman, Primitivo Gomez-Cardero, Carlos A. Encinas-Ullan, and Victor Jimenez-Yuste. 2022. "Complications and Implant Survival of Total Knee Arthroplasty in People with Hemophilia" Journal of Clinical Medicine 11, no. 21: 6244. https://doi.org/10.3390/jcm11216244
APA StyleRodriguez-Merchan, E. C., De la Corte-Rodriguez, H., Alvarez-Roman, T., Gomez-Cardero, P., Encinas-Ullan, C. A., & Jimenez-Yuste, V. (2022). Complications and Implant Survival of Total Knee Arthroplasty in People with Hemophilia. Journal of Clinical Medicine, 11(21), 6244. https://doi.org/10.3390/jcm11216244