


TECAR Therapy Associated with High-Intensity Laser Therapy (Hilt) and Manual Therapy in the Treatment of Muscle Disorders: A Literature Review on the Theorised Effects Supporting Their Use

 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
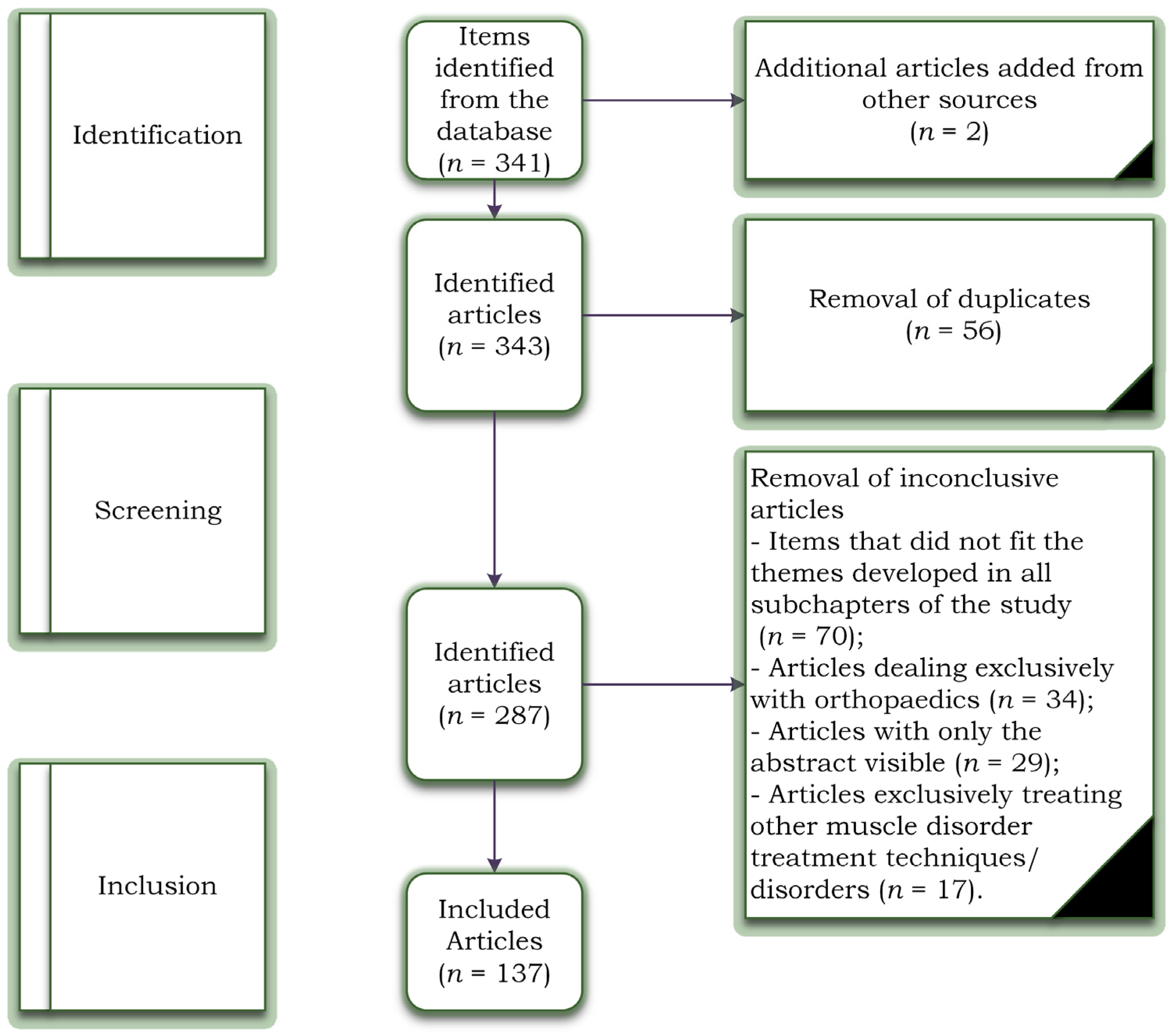
2. Materials and Methods
- (a)
- PubMed: (TECAR therapy) OR (HILT Therapy) OR (Manual Therapy) OR (Muscle disorders) AND (Treatment) AND (High-frequency) OR (Electric stimulation) AND (Laser treatment) OR (Muscle pain) AND (Back) AND (Knee) OR (Therapeutic effect) OR (Ultrasound Therapy) OR (Mobilisation) OR (Physical Rehabilitation) OR (knee joint effusion) OR (elastography) OR (Hydrotherapy) OR (Electromyographic activity) OR (Musculoskeletal pain) OR (therapeutic ultrasound) OR (Pain intensity evaluation) OR (Massage therapy) OR (Capacitive and Resistive Electric Transfer).
- (b)
- Scopus: (Therapeutic effect) OR (Ultrasound Therapy) OR (Mobilisation) OR (Physical Rehabilitation) OR (knee joint effusion) OR (elastography) OR (Hydrotherapy) OR (Electromyographic activity) OR (Musculoskeletal pain) OR (Therapeutic ultrasound) OR (Pain intensity evaluation) OR (TECAR therapy) OR (HILT therapy) OR (Manual Therapy) OR (Muscle disorders) AND (Massage therapy) OR (Capacitive and Resistive Electric Transfer).
- (c)
- Web of Science: (Muscle pain) AND (Back) AND (Knee) OR (Therapeutic effect) OR (Ultrasound Therapy) OR (Mobilisation) OR (Physical Rehabilitation) OR (knee joint effusion) OR (elastography) (TECAR therapy) OR (HILT Therapy) OR (therapeutic ultrasound) OR (Pain intensity evaluation) OR (Massage therapy) OR (Manual Therapy) OR (Muscle disorders) AND (Treatment) AND (High-frequency) OR (Electric stimulation) AND (Laser treatment) OR (Capacitive and Resistive Electric Transfer).
3. Manual Therapy vs. TECAR vs. HILT Therapy
4. The Benefits of Manual Therapy in the Treatment of Muscle Diseases
5. The Benefits of HILT Therapy in the Treatment of Muscle Disorders
- Thyroid disorders: The thyroid is known to be sensitive to light, and although it has not yet been found to harm the thyroid gland, caution and careful dosing are recommended when using the laser [62].
- Clotting problems: Laser therapy affects blood clotting, so its use for patients with such problems should be consulted with a specialist or even replaced with another procedure [63].
- Children: Although there is no contraindication to the use of the laser for children, its dose should be adjusted according to weight [64].
6. The Benefits of TECAR Therapy in the Treatment of Muscle Diseases
7. Manual Therapy–TECAR–HILT Therapy: Recommendations in the Treatment of Muscle Diseases
8. Manual Therapy–TECAR–HILT Therapy: Methods of Use in the Treatment of Muscle Diseases
9. Manual Therapy–TECAR–HILT Therapy: Contraindications
10. Limitations of the Study
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nas, K.; Yazmalar, L.; Şah, V.; Aydin, A.; Öneş, K. Rehabilitation of spinal cord injuries. World J. Orthop. 2015, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Jesus, T.S.; Landry, M.D.; Hoenig, H. Global need for physical rehabilitation: Systematic analysis from the global burden of disease study. Int. J. Environ. Res. Public Health 2019, 16, 980. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, M.M.; Wang, J.; Haarbauer-Krupa, J.; Yeates, K.O.; Durbin, D.; Zonfrillo, M.R.; Jaffe, K.M.; Temkin, N.; Tulsky, D.; Bertisch, H.; et al. Unmet rehabilitation needs after hospitalisation for traumatic brain injury. Pediatrics 2018, 141, e20172859. [Google Scholar] [CrossRef] [PubMed]
- Kamenov, K.; Mills, J.A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.; Wallace, S.; Kuper, H. A systematic review of access to rehabilitation for people with disabilities in low- and middle-income countries. Int. J. Environ. Res. Public Health 2018, 15, 2165. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef]
- Logerstedt, D.; Arundale, A.; Lynch, A.; Snyder-Mackler, L. A conceptual framework for a sports knee injury performance profle (SKIPP) and return to activity criteria (RTAC). Braz. J. Phys. Ther. 2015, 19, 340–359. [Google Scholar] [CrossRef][Green Version]
- Alessandrino, F.; Balconi, G. Complications of muscle injuries. J. Ultrasound. 2013, 16, 215–222. [Google Scholar] [CrossRef][Green Version]
- Wong, K.; Sun, F.; Trudel, G.; Sebastiani, P.; Laneuville, O. Temporal gene expression profiling of the rat knee joint capsule during immobilisation-induced joint contractures. BMC Musculoskelet. Disord. 2015, 16, 125. [Google Scholar] [CrossRef]
- Lynch, A.D.; Logerstedt, D.S.; Axe, M.J.; Snyder-Mackler, L. Quadriceps activation failure after anterior cruciate ligament rupture is not mediated by knee joint effusion. J. Orthop. Sports Phys. Ther. 2012, 42, 502–510. [Google Scholar] [CrossRef]
- Frontera, W.R.; Ochala, J. Skeletal muscle: A brief review of structure and function. Calcif. Tissue Int. 2015, 96, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Shieh, P.B. Muscular dystrophies and other genetic myopathies. Neurol. Clin. 2013, 31, 1009–1029. [Google Scholar] [CrossRef]
- Mueller-Wohlfahrt, H.W.; Haensel, L.; Mithoefer, K.; Ekstrand, J.; English, B.; McNally, S.; Orchard, J.; van Dijk, C.N.; Kerkhoffs, G.M.; Schamasch, P.; et al. Terminology and classification of muscle injuries in sport: The Munich consensus statement. Br. J. Sports Med. 2013, 47, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Branco, P.; Alonso, J.M. Muscle injury is the principal injury type and hamstring muscle injury is the first injury diagnosis during top-level international athletics championships between 2007 and 2015. Br. J. Sports Med. 2016, 50, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Bordoni, B.; Sugumar, K.; Varacallo, M. Muscle Cramps; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Hotfiel, T.; Carl, H.D.; Swoboda, B.; Heinrich, M.; Heiß, R.; Grim, C.; Engelhardt, M. Current conservative treatment and management strategies of skeletal muscle injuries. Z. Orthop. Und Unf. 2016, 154, 245–253. [Google Scholar]
- Delos, D.; Maak, T.G.; Rodeo, S.A. Muscle injuries in athletes: Enhancing recovery through scientific understanding and novel therapies. Sports Health 2013, 5, 346–352. [Google Scholar] [CrossRef]
- Yanagisawa, O.; Niitsu, M.; Kurihara, T.; Fukubayashi, T. Evaluation of human muscle hardness after dynamic exercise with ultrasound real-time tissue elastography: A feasibility study. Clin. Radiol. 2011, 66, 815–819. [Google Scholar] [CrossRef]
- Ghasemi, M.; Bagheri, H.; Olyaei, G.; Talebian, S.; Shadmehr, A.; Jalaei, S.; Kalantari, K.K. Effects of cyclic static stretch on fatigue recovery of triceps surae in female basketball players. Biol. Sport 2013, 30, 97–102. [Google Scholar] [CrossRef]
- Castro-Sánchez, A.M.; Matarán-Peñarrocha, G.A.; Lara-Palomo, I.; Saavedra-Hernández, M.; Arroyo-Morales, M.; Moreno-Lorenzo, C. Hydrotherapy for the treatment of pain in people with multiple sclerosis: A randomised controlled trial. Evid. Based Complement. Altern. Med. 2012, 2012, 473963. [Google Scholar] [CrossRef]
- Elias, G.P.; Varley, M.C.; Wyckelsma, V.L.; McKenna, M.J.; Minahan, C.L.; Aughey, R.J. Effects of water immersion on post training recovery in Australian footballers. Int. J. Sports Physiol. Perform. 2012, 7, 357–366. [Google Scholar] [CrossRef]
- Leeder, J.; Gissane, C.; van Someren, K.; Gregson, W.; Howatson, G. Cold water immersion and recovery from strenuous exercise: A meta-analysis. Br. J. Sports Med. 2012, 46, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Osti, R.; Pari, C.; Salvatori, G.; Massari, L. Tri-length laser therapy associated to TECAR therapy in the treatment of low-back pain in adults: A preliminary report of a prospective case series. Lasers Med. Sci. 2015, 30, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Pereira, W.M.; Ferreira, L.A.; Rossi, L.P.; Kerpers, I.I.; Grecco, S.L.A.; de Paula, A.R.J.; Oliveira, C.S. Influence of heat on fatigue and electromyographic activity of the biceps brachii muscle. J. Bodyw. Mov. Ther. 2011, 15, 478–484. [Google Scholar] [CrossRef]
- Hayashi, K.; Arai, Y.C.; Ikemoto, T.; Nishihara, M.; Suzuki, S.; Hirakawa, T.; Matsuo, S.; Kobayashi, M.; Haruta, M.; Kawabata, Y.; et al. Predictive factors for the outcome of multidisciplinary treatments in chronic low back pain at the first multidisciplinary pain center of Japan. J. Phys. Ther. Sci. 2015, 27, 2901–2905. [Google Scholar] [CrossRef] [PubMed]
- Alayat, M.S.; Atya, A.M.; Ali, M.M.; Shosha, T.M. Long-term effect of high-intensity laser therapy in the treatment of patients with chronic low back pain: A randomised blinded placebo-controlled trial. Lasers Med. Sci. 2014, 29, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Pillastrini, P.; Gardenghi, I.; Bonetti, F.; Capra, F.; Guccione, A.; Mugnai, R.; Violante, F.S. An updated overview of clinical guidelines for chronic low back pain management in primary care. Jt. Bone Spine 2012, 79, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Bule, M.L.; Paíno, C.L.; Trillo, M.Á.; Úbeda, A. Electric stimulation at 448 kHz promotes proliferation of human mesenchymal stem cells. Cell Physiol. Biochem. 2014, 34, 1741–1755. [Google Scholar] [CrossRef]
- Kato, S.; Saitoh, Y.; Miwa, N. Repressive effects of a capacitive-resistive electric transfer (CRet) hyperthermic apparatus combined with provitamin C on intracellular lipid-droplets formation in adipocytes. Int. J. Hyperth. 2013, 29, 30–37. [Google Scholar] [CrossRef]
- Cheng, H.; Huang, Y.; Yue, H.; Fan, Y. Electrical Stimulation Promotes Stem Cell Neural Differentiation in Tissue Engineering. Stem Cells Int. 2021, 2021, 6697574. [Google Scholar] [CrossRef]
- Oostendorp, R.A.B. Credibility of manual therapy is at stake “Where do we go from here?”. J. Man Manip. Ther. 2018, 26, 189–192. [Google Scholar] [CrossRef]
- Reid, D.; Cook, C.; Sizer, P.S. Is orthopedic manipulative physical therapy not fashionable anymore? Lessons learned from 2016 IFOMPT meeting and future directions. J. Man Manip. Ther. 2017, 25, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Babatunde, O.O.; Jordan, J.L.; Van der Windt, D.A.; Hill, J.C.; Foster, N.E.; Protheroe, J. Effective treatment options for musculoskeletal pain in primary care: A systematic overview of current evidence. PLoS ONE 2017, 12, e0178621. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.J.; Choi, J.; Lee, S.; Jeon, C.; Lee, K. The effects of high intensity laser therapy on pain and function in patients with knee osteoarthritis. J. Phys. Ther. Sci. 2016, 28, 3197–3199. [Google Scholar] [CrossRef] [PubMed]
- Conforti, M.; Fachinetti, G.P. High power laser therapy treatment compared to simple segmental physical rehabilitation in whiplash injuries (1° and 2° grade of the Quebec Task Force classification) involving muscles and ligaments. Muscles Ligaments Tendons J. 2013, 3, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, K.; Fekrazad, R.; Raoufi, Z. The effects of photo-biomodulation therapy on post-surgical pain. J. Lasers Med. Sci. 2019, 10, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Thabet, A.A.E.; Elsodany, A.M.; Battecha, K.H.; Alshehri, M.A.; Refaat, B. High-intensity laser therapy versus pulsed electromagnetic field in the treatment of primary dysmenorrhea. J. Phys. Ther. Sci. 2017, 29, 1742–1748. [Google Scholar] [CrossRef]
- Thabet, A.A.E.; Mahran, H.G.; Ebid, A.A.; Alshehri, M.A. Effect of pulsed high intensity laser therapy on delayed caesarean section healing in diabetic women. J. Phys. Ther. Sci. 2018, 30, 570–575. [Google Scholar] [CrossRef]
- Pekyavas, N.O.; Baltaci, G. Short-term effects of high-intensity laser therapy, manual therapy, and Kinesio taping in patients with subacromial impingement syndrome. Lasers Med. Sci. 2016, 31, 1133–1141. [Google Scholar] [CrossRef]
- Ordahan, B.; Karahan, A.Y.; Kaydok, E. The effect of high-intensity versus low-level laser therapy in the management of plantar fasciitis: A randomised clinical trial. Lasers Med. Sci. 2018, 33, 1363–1369. [Google Scholar] [CrossRef]
- Taradaj, J.; Rajfur, K.; Shay, B.; Rajfur, J.; Ptaszkowski, K.; Walewicz, K.; Dymarek, R.; Sopel, M.; Rosińczuk, J. Photo-biomodulation using high—Or low-level laser irradiations in patients with lumbar disc degenerative changes: Disappointing outcomes and remarks. Clin. Interv. Aging 2018, 13, 1445–1455. [Google Scholar] [CrossRef]
- Song, H.J.; Seo, H.J.; Lee, Y.; Kim, S.K. Effectiveness of high-intensity laser therapy in the treatment of musculoskeletal disorders: A systematic review and meta-analysis of randomised controlled trials. Medicine 2018, 97, e13126. [Google Scholar] [CrossRef] [PubMed]
- Thoomes, E.J.; Scholten-Peeters, W.; Koes, B.; Falla, D.; Verhagen, A.P.; Clin, J. The effectiveness of conservative treatment for patients with cervical radiculopathy: A systematic review. Pain 2013, 29, 1073–1086. [Google Scholar] [CrossRef] [PubMed]
- Kheshie, A.R.; Alayat, M.S.; Ali, M.M. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: A randomised controlled trial. Lasers Med. Sci. 2014, 29, 1371–1376. [Google Scholar] [CrossRef] [PubMed]
- Yıldırıım, M.A.; Uçar, D.; Öneş, K. Comparison of therapeutic duration of therapeutic ultrasound in patients with knee osteoarthritis. J. Phys. Ther. Sci. 2015, 27, 3667–3670. [Google Scholar] [CrossRef] [PubMed]
- Boyraz, I.; Yildiz, A.; Koc, B.; Sarman, H. Comparison of high-intensity laser therapy and ultrasound treatment in the patients with lumbar discopathy. Biomed. Res. Int. 2015, 2015, 304328. [Google Scholar] [CrossRef]
- Zielińska, P.; Nicpoń, J.; Kiełbowicz, Z.; Soroko, M.; Dudek, K.; Zaborski, D. Effects of high intensity laser therapy in the treatment of tendon and ligament injuries in performance horses. Animals 2020, 10, 1327. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, K.; Laakso, E.L.; Salari, A.; Hasannejad, A.; Fekrazad, R.; Aris, A. The beneficial effects of high-intensity laser therapy and co-interventions on musculoskeletal pain management: A systematic review. J. Lasers Med. Sci. 2020, 11, 81–90. [Google Scholar] [CrossRef]
- Abdelbasset, W.K.; Nambi, G.; Alsubaie, S.F.; Abodonya, A.M.; Saleh, A.K.; Ataalla, N.N.; Ibrahim, A.A.; Tantawy, S.A.; Kamel, D.M.; Verma, A.; et al. A randomised comparative study between high-intensity and low-level laser therapy in the treatment of chronic nonspecific low back pain. Evid. Based Complement. Altern. Med. 2020, 2020, 1350281. [Google Scholar] [CrossRef]
- Pellegrino, R.; Paolucci, T.; Brindisino, F.; Mondardini, P.; Di Iorio, A.; Moretti, A.; Iolascon, G. Effectiveness of High-Intensity Laser Therapy Plus Ultrasound-Guided Peritendinous Hyaluronic Acid Compared to Therapeutic Exercise for Patients with Lateral Elbow Tendinopathy. J. Clin. Med. 2022, 11, 5492. [Google Scholar] [CrossRef]
- Alayat, M.S.; El Soudany, A.M.; El Fiky, A.A. Efficacy of high—And low-level laser therapy in the treatment of Bell’s palsy: A randomised double-blind placebo-controlled trial. Lasers Med. Sci. 2014, 29, 335–342. [Google Scholar] [CrossRef]
- Alayat, M.S.; El Soudany, A.M.; Ali, M.E. Efficacy of multiwave locked system laser on pain and function in patients with chronic neck pain: A randomised placebo-controlled trial. Photomed. Laser Surg. 2017, 35, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Alayat, M.S.; Aly, T.H.A.; Elsayed, A.E.M.; Fadil, A.S.M. Efficacy of pulsed Nd:YAG laser in the treatment of patients with knee osteoarthritis: A randomised controlled trial. Lasers Med. Sci. 2017, 32, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Thabet, A.A.E.; Alshehri, M.A. Effect of pulsed high-intensity laser therapy on pain, adhesions, and quality of life in women having endometriosis: A randomized controlled trial. Photomed. Laser Surg. 2018, 36, 363–369. [Google Scholar] [CrossRef]
- Tkocz, P.; Matusz, T.; Kosowski, Ł.; Walewicz, K.; Argier, Ł.; Kuszewski, M.; Hagner-Derengowska, M.; Ptaszkowski, K.; Dymarek, R.; Taradaj, J. A Randomised-Controlled Clinical Study Examining the Effect of High-Intensity Laser Therapy (HILT) on the Management of Painful Calcaneal Spur with Plantar Fasciitis. J. Clin. Med. 2021, 10, 4891. [Google Scholar] [CrossRef] [PubMed]
- Alayat, M.S.M.; Abdel-Kafy, E.M.; Elsoudany, A.M.; Helal, O.F.; Alshehri, M.A. Efficacy of high intensity laser therapy in the treatment of male with osteopenia or osteoporosis: A randomised placebo-controlled trial. J. Phys. Ther. Sci. 2017, 29, 1675–1679. [Google Scholar] [CrossRef]
- Ebid, A.A.; El-Kafy, E.M.; Alayat, M.S. Effect of pulsed Nd:YAG laser in the treatment of neuropathic foot ulcers in children with spina bifida: A randomised controlled study. Photomed. Laser Surg. 2013, 31, 565–570. [Google Scholar] [CrossRef]
- Wyszynska, J.; Bal-Bochenska, M. Efficacy of high-intensity laser therapy in treating knee osteoarthritis: A first systematic review. Photomed. Laser Surg. 2018, 36, 343–353. [Google Scholar] [CrossRef]
- Cotler, H.; Chow, R.T.; Hamblin, M.R.; Carroll, J. The use of low-level laser therapy (LLLT) for musculoskeletal pain. MOJ Orthop. Rheumatol. 2015, 2, 00068. [Google Scholar] [CrossRef] [PubMed]
- Tortorici, S.; Messina, P.; Scardina, G.A. Effectiveness of low-level laser therapy on pain intensity after lower third molar extraction. Int. J. Clin. Dent. 2019, 12, 357–367. [Google Scholar]
- Chow, R.; Armati, P.; Laakso, E.L.; Bjordal, J.M.; Baxter, G.D. Inhibitory effects of laser irradiation on peripheral mammalian nerves and relevance to analgesic effects: A systematic review. Photomed. Laser Surg. 2011, 29, 365–381. [Google Scholar] [CrossRef]
- Holanda, V.M.; Chavantes, M.C.; Wu, X.; Anders, J.J. The mechanistic basis for photo-biomodulation therapy of neuropathic pain by near infrared laser light. Lasers Surg. Med. 2017, 49, 516–524. [Google Scholar] [PubMed]
- Ketz, A.K.; Byrnes, K.R.; Grunberg, N.E. Characterization of macrophage/microglial activation and effect of photo-biomodulation in the spared nerve injury model of neuropathic pain. Pain Med. 2017, 18, 932–946. [Google Scholar]
- Thabet, A.A.; Ebid, A.A.; El-Boshy, M.E.; Almuwallad, A.O.; Hudaimoor, E.A.; Alsaeedi, F.E.; Alsubhi, R.H.; Almatrook, R.H.; Aljifry, R.F.; Alotaibi, S.H.; et al. Pulsed high-intensity laser therapy versus low level laser therapy in the management of primary dysmenorrhea. J. Phys. Ther. Sci. 2021, 33, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.K.; Masaracchio, M.; Brismée, J.-M. The future of orthopedic manual therapy: What are we missing? J. Man Manip. Ther. 2017, 25, 169–171. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Coronado, R.A.; Bialosky, J.E. Manual physical therapy for chronic pain: The complex whole is greater than the sum of its parts. J. Man Manip. Ther. 2017, 25, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Duñabeitia, I.; Arrieta, H.; Torres-Unda, J.; Gil, J.; Santos-Concejero, J.; Gil, S.M.; Irazusta, J.; Bidaurrazaga-Letona, I. Effects of a capacitive-resistive electric transfer therapy on physiological and biomechanical parameters in recreational runners: A randomised controlled crossover trial. Phys. Ther. Sport 2018, 32, 227–234. [Google Scholar] [CrossRef]
- Diego, I.M.A.; Fernández-Carnero, J.; Val, S.L.; Cano-de-la-Cuerda, R.; Calvo-Lobo, C.; Piédrola, R.M.; Oliva, L.C.L.; Rueda, F.M. Analgesic effects of a capacitive-resistive monopolar radiofrequency in patients with myofascial chronic neck pain: A pilot randomised controlled trial. Rev. Assoc. Med. Bras. 2019, 65, 156–164. [Google Scholar] [CrossRef]
- Rodríguez-Sanz, J.; López-De-Celis, C.; Hidalgo-García, C.; Canet-Vintró, M.; Fanlo-Mazas, P.; Pérez-Bellmunt, A. Temperature and current flow effects of different electrode placement in shoulder capacitive-resistive electric transfer applications: A cadaveric study. BMC Musculoskelet. Disord. 2021, 22, 139. [Google Scholar] [CrossRef]
- Sousa, L.D.S.-D.; Sanchez, C.T.; Maté-Muñoz, J.L.; Hernández-Lougedo, J.; Barba, M.; Lozano-Estevan, M.D.C.; Garnacho-Castaño, M.V.; García-Fernández, P. Application of Capacitive-Resistive Electric Transfer in Physiotherapeutic Clinical Practice and Sports. Int. J. Environ. Res. Public Health 2021, 18, 12446. [Google Scholar] [CrossRef]
- Beltrame, R.; Ronconi, G.; Ferrara, P.E.; Salgovic, L.; Vercelli, S.; Solaro, C.; Ferriero, G. Capacitive and resistive electric transfer therapy in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2020, 43, 291–298. [Google Scholar] [CrossRef]
- Nakamura, M.; Sato, S.; Kiyono, R.; Yahata, K.; Yoshida, R.; Kasahara, K.; Konrad, A. The Effect of Capacitive and Resistive Electric Transfer Intervention on Delayed-Onset Muscle Soreness Induced by Eccentric Exercise. Int. J. Environ. Res. Public Health 2022, 19, 5723. [Google Scholar] [CrossRef] [PubMed]
- López-De-Celis, C.; Hidalgo-García, C.; Pérez-Bellmunt, A.; Fanlo-Mazas, P.; González-Rueda, V.; Tricás-Moreno, J.M.; Ortiz, S.; Rodríguez-Sanz, J. Thermal and non-thermal effects off capacitive-resistive electric transfer application on the Achilles tendon and musculotendinous junction of the gastrocnemius muscle: A cadaveric study. BMC Musculoskelet. Disord. 2020, 21, 46. [Google Scholar] [CrossRef]
- Ostrowski, J.; Herb, C.C.; Scifers, J.; Gonzalez, T.; Jennings, A.; Breton, D. Comparison of muscle temperature increases produced by moist hot pack and ThermoStim probe. J. Sport Rehabil. 2019, 28, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Pizarro, S. Transferencia eléctrica capacitiva y resistiva para mitigar el dolor [Capacitive and resistive electrical transfer for pain mitigation]. Rehabilitacion 2020, 54, 221–222. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, Y.; Hasegawa, S.; Yokota, Y.; Nishiguchi, S.; Fukutani, N.; Shirooka, H.; Tasaka, S.; Matsushita, T.; Matsubara, K.; Nakayama, Y.; et al. Effect of capacitive and resistive electric transfer on haemoglobin saturation and tissue temperature. Int. J. Hyperth. 2017, 33, 696–702. [Google Scholar] [CrossRef]
- Hernández-Bule, M.L.; Trillo, M.Á.; Úbeda, A. Molecular mechanisms underlying antiproliferative and differentiating responses of hepatocarcinoma cells to subthermal electric stimulation. PLoS ONE 2014, 9, e84636. [Google Scholar] [CrossRef]
- Chen, C.; Bai, X.; Ding, Y.; Lee, I.S. Electrical stimulation as a novel tool for regulating cell behavior in tissue engineering. Biomater. Res. 2019, 23, 25. [Google Scholar] [CrossRef]
- Paolucci, T.; Pezzi, L.; Centra, M.A.; Porreca, A.; Barbato, C.; Bellomo, R.G.; Saggini, R. Effects of capacitive and resistive electric transfer therapy in patients with painful shoulder impingement syndrome: A comparative study. J. Int. Med. Res. 2020, 48, 300060519883090. [Google Scholar] [CrossRef]
- Bito, T.; Tashiro, Y.; Suzuki, Y.; Kajiwara, Y.; Zeidan, H.; Kawagoe, M.; Sonoda, T.; Nakayama, Y.; Yokota, Y.; Shimoura, K.; et al. Acute effects of capacitive and resistive electric transfer (CRet) on the Achilles tendon. Electromagn. Biol. Med. 2019, 38, 48–54. [Google Scholar] [CrossRef]
- Wostyn, V. La Tecarthérapie Appliquée a la Kinésithérapie: Evaluation de Leffet Antalgique Immédiat; Institut de Formation on Masso-Kinésithérapie: Reims, France, 2015. [Google Scholar]
- Clijsen, R.; Leoni, D.; Schneebeli, A.; Cescon, C.; Soldini, E.; Li, L.; Barbero, M. Does the application of TECAR therapy affect temperature and perfusion of skin and muscle microcirculation? A pilot feasibility study on healthy subjects. J. Altern. Complement. Med. 2020, 26, 147–153. [Google Scholar] [CrossRef]
- López-de-Celis, C.; Rodríguez-Sanz, J.; Hidalgo-García, C.; Cedeño-Bermúdez, S.A.; Zegarra-Chávez, D.; Fanlo-Mazas, P.; Pérez-Bellmunt, A. Thermal and Current Flow Effects of a Capacitive-Resistive Electric Transfer Application Protocol on Chronic Elbow Tendinopathy. A Cadaveric Study. Int. J. Environ. Res. Public Health 2021, 18, 1012. [Google Scholar] [CrossRef] [PubMed]
- Masiero, S.; Pignataro, A.; Piran, G.; Duso, M.; Mimche, P.; Ermani, M.; Del Felice, A. Short-wave diathermy in the clinical management of musculoskeletal disorders: A pilot observational study. Int. J. Biometeorol. 2020, 64, 981–988. [Google Scholar] [CrossRef]
- Ozen, S.; Doganci, E.B.; Ozyuvali, A.; Yalcin, A.P. Effectiveness of continuous versus pulsed short-wave diathermy in the management of knee osteoarthritis: A randomised pilot study. Casp. J. Intern Med. 2019, 10, 431–438. [Google Scholar]
- Koller, T. Mechanosensitive Aspects of Cell Biology in Manual Scar Therapy for Deep Dermal Defects. Int. J. Mol. Sci. 2020, 21, 2055. [Google Scholar] [CrossRef] [PubMed]
- Kumaran, B.; Watson, T. Thermal build-up, decay and retention responses to local therapeutic application of 448 kHz capacitive resistive monopolar radiofrequency: A prospective randomised crossover study in healthy adults. Int. J. Hyperth. 2015, 31, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Priego-Quesada, J.I.; De la Fuente, C.; Kunzler, M.R.; Perez-Soriano, P.; Hervás-Marín, D.; Carpes, F.P. Relationship between Skin Temperature, Electrical Manifestations of Muscle Fatigue, and Exercise-Induced Delayed Onset Muscle Soreness for Dynamic Contractions: A Preliminary Study. Int. J. Environ. Res. Public Health 2020, 17, 6817. [Google Scholar] [CrossRef]
- Notarnicola, A.; Maccagnano, G.; Gallone, M.F.; Covelli, I.; Tafuri, S.; Moretti, B. Short term efficacy of capacitive resistive diathermy therapy in patients with low back pain: A prospective randomised controlled trial. J. Biol. Regul. Homeost. Agents 2017, 31, 509–515. [Google Scholar] [PubMed]
- Yokota, Y.; Tashiro, Y.; Suzuki, Y. Effect of capacitive and resistive electric transfer on tissue temperature, muscle flexibility and blood circulation. J. Nov. Physiother. 2017, 30, 719–725. [Google Scholar] [CrossRef]
- Niajalili, M.; Sedaghat, M.; Reazasoltani, A.; Akbarzade Baghban, A.R.; Naimi, S.S. Effect of Capacitive Tecar Therapy on Foot Pain and Tactile Sensation in Patients with Type 2 Diabetes. Arch. Rehab. 2020, 21, 304–319. [Google Scholar] [CrossRef]
- Du, J.; Zhen, G.; Chen, H.; Zhang, S.; Qing, L.; Yang, X.; Lee, G.; Mao, H.Q.; Jia, X. Optimal electrical stimulation boosts stem cell therapy in nerve regeneration. Biomaterials 2018, 181, 347–359. [Google Scholar] [CrossRef]
- Zaretsky, D.V.; Romanovsky, A.A.; Zaretskaia, M.V.; Molkov, Y.I. Tissue oxidative metabolism can increase the difference between local temperature and arterial blood temperature by up to 1.3 °C: Implications for brain, brown adipose tissue, and muscle physiology. Temperature 2018, 5, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Ganzit, G.P.; Stefanini, L.; Stesina, G. TECAR Therapy in the Treatment of Acute and Chronic Pathologies in Sports; FMSI (Italian Sports Medicine Federation)-CONI Institute of Sports Medicine: Torino, Italy, 2015. [Google Scholar]
- Robinson, S.E.; Buono, M.J. Effect of continuous-wave ultrasound on blood flow in skeletal muscle. Phys. Ther. 1995, 75, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Meng, S.; Rouabhia, M.; Zhang, Z. Electrical Stimulation and Cellular Behaviors in Electric Field in Biomedical Research. Materials 2021, 15, 165. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Bule, M.L.; Martínez, M.A.; Trillo, M.Á.; Martínez, L.; Toledano-Macías, E.; Úbeda, A. Response of human cancer cells to simultaneous treatment with sorafenib and radiofrequency current. Oncol. Lett. 2021, 22, 807. [Google Scholar] [CrossRef]
- Yokota, Y.; Sonoda, T.; Tashiro, Y.; Suzuki, Y.; Kajiwara, Y.; Zeidan, H.; Nakayama, Y.; Kawagoe, M.; Shimoura, K.; Tatsumi, M.; et al. Effect of capacitive and resistive electric transfer on changes in muscle flexibility and lumbopelvic alignment after fatiguing exercise. J. Phys. Ther. Sci. 2018, 30, 719–725. [Google Scholar] [CrossRef]
- Castellani, J.W.; Zambraski, E.J.; Sawka, M.N.; Urso, M.L. Does high muscle temperature accentuate skeletal muscle injury from eccentric exercise? Physiol. Rep. 2016, 4, e12777. [Google Scholar] [CrossRef][Green Version]
- Giombini, A.; Di Cesare, A.; Casciello, G.; Sorrenti, D.; Dragoni, S.; Gabriele, P. Hyperthermia at 434 MHz in the treatment of overuse sport tendinopathies: A randomised controlled clinical trial. Int. J. Sports Med. 2002, 23, 207–211. [Google Scholar] [CrossRef]
- Hawkes, A.R.; Draper, D.O.; Johnson, A.W.; Diede, M.T.; Rigby, J.H. Heating capacity of rebound shortwave diathermy and moist hot packs at superficial depths. J. Athl. Train. 2013, 48, 471–476. [Google Scholar] [CrossRef]
- Berteau, J.P. Knee Pain from Osteoarthritis: Pathogenesis, Risk Factors, and Recent Evidence on Physical Therapy Interventions. J. Clin. Med. 2022, 11, 3252. [Google Scholar] [CrossRef]
- Naruseviciute, D.; Raimondas, K. The effect of high-intensity versus low-level laser therapy in the management of plantar fasciitis: Randomised participant blind controlled trial. Clin. Rehabil. 2020, 34, 1072–1082. [Google Scholar] [CrossRef]
- Mamais, I.; Konstantinos, P.; Demetris, L.; Demetrios, S. Effectiveness of low-level laser therapy (LLLT) in the treatment of Lateral elbow tendinopathy (L.E.T.): An umbrella review effectiveness of LLLT in the treatment of L.E.T.: Umbrella review. Laser Ther. 2018, 27, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Starzec-Proserpio, M.; Grigol Bardin, M.; Fradette, J.; Tu, L.M.; Bérubè-Lauzière, Y.; Paré, J.; Carroll, M.-S.; Morin, M. High-Intensity Laser Therapy (HILT) as an Emerging Treatment for Vulvodynia and Chronic Musculoskeletal Pain Disorders: A Systematic Review of Treatment Efficacy. J. Clin. Med. 2022, 11, 3701. [Google Scholar] [CrossRef] [PubMed]
- Dunning, J.R.; Butts, R.; Mourad, F.; Young, I.; Fernandez-de-Las Peñas, C.; Hagins, M.; Stanislawski, T.; Donley, J.; Buck, D.; Hooks, T.R.; et al. Upper cervical and upper thoracic manipulation versus mobilisation and exercise in patients with cervicogenic headache: A multi-center randomised clinical trial. BMC Musculoskelet. Dis. 2016, 17, 64. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.K.; Gilden, B. A non-operative approach to the management of chronic exertional compartment syndrome in a triathlete: A case report. Int. J. Sports Phys. Ther. 2016, 11, 1160–1176. [Google Scholar]
- Rajasekaran, S.; Hall, M.M. Nonoperative management of chronic exertional compartment syndrome: A systematic review. Curr. Sports Med. Rep. 2016, 15, 191–198. [Google Scholar] [CrossRef]
- Masaracchio, M.; Cleland, J.A.; Hellman, M.; Hagins, M. Short-term combined effects of thoracic spine thrust manipulation and cervical spine nonthrust manipulation in individuals with mechanical neck pain: A randomised clinical trial. J. Orthop. Sports Phys. Ther. 2013, 43, 118–127. [Google Scholar] [CrossRef]
- Takasaki, H.; Hall, T.; Jull, G. Immediate and short-term effects of mulligan’s mobilisation with movement on knee pain and disability associated with knee osteoarthritis—A prospective case series. Physiother. Theory Pract. 2013, 29, 87–95. [Google Scholar] [CrossRef]
- Delitto, A.; George, S.Z.; Van Dillen, L.; Whitman, J.M.; Sowa, G.; Shekelle, P.; Denninger, T.R.; Godges, J.J. Low back pain. J. Orthop. Sports Phys. Ther. 2012, 42, A1–A57. [Google Scholar] [CrossRef]
- Santuzzi, C.H.; Buss, H.F.; Pedrosa, D.F.; Freire, M.O.; Nogueira, B.V.; Gonçalves, W.L. Combined use of low-level laser therapy and cyclooxygenase-2 selective inhibition on skin incisional wound reepithelialisation in mice: A preclinical study. Bras. Dermatol. 2011, 86, 278–283. [Google Scholar] [CrossRef]
- Hernández-Bule, M.L.; Medel, E.; Colastra, C.; Roldán, R.; Úbeda, A. Response of neuroblastoma cells to RF currents as a function of the signal frequency. BMC Cancer 2019, 19, 889. [Google Scholar] [CrossRef]
- Cheng, H.; Huang, Y.; Chen, W.; Che, J.; Liu, T.; Na, J.; Wang, R.; Fan, Y. Cyclic Strain and Electrical Co-stimulation Improve Neural Differentiation of Marrow-Derived Mesenchymal Stem Cells. Front. Cell Dev. Biol. 2021, 9, 624755. [Google Scholar] [CrossRef] [PubMed]
- Shadrin, I.Y.; Khodabukus, A.; Bursac, N. Striated muscle function, regeneration, and repair. Cell Mol. Life Sci. 2016, 73, 4175–4202. [Google Scholar] [CrossRef] [PubMed]
- Brozovich, F.V.; Nicholson, C.J.; Degen, C.V.; Gao, Y.Z.; Aggarwal, M.; Morgan, K.G. Mechanisms of vascular smooth muscle contraction and the basis for pharmacologic treatment of smooth muscle disorders. Pharmacol. Rev. 2016, 68, 476–532. [Google Scholar] [CrossRef] [PubMed]
- McLoon, L.K.; Vicente, A.; Fitzpatrick, K.R.; Lindström, M.; Domellöf, F.P. Composition, architecture, and functional implications of the connective tissue network of the extraocular muscles. Investig. Ophthalmol. Vis. Sci. 2018, 59, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Tantawy, S.A.; Abdelbasset, W.K.; Kamel, D.M.; Alrawaili, S.M. A randomised controlled trial comparing helium-neon laser therapy and infrared laser therapy in patients with diabetic foot ulcer. Lasers Med. Sci. 2018, 33, 1901–1906. [Google Scholar] [CrossRef]
- Tantawy, S.A.; Abdelbasset, W.K.; Kamel, D.M.; Alrawaili, S.M.; Alsubaie, S.F. Laser photo-biomodulation is more effective than ultrasound therapy in patients with chronic nonspecific low back pain: A comparative study. Lasers Med. Sci. 2019, 34, 793–800. [Google Scholar] [CrossRef]
- Kaydok, E.; Ordahan, B.; Solum, S.; Karahan, A.Y. Short-term Efficacy Comparison of High-intensity and Low-intensity Laser Therapy in the Treatment of Lateral Epicondylitis: A Randomized Double-blind Clinical Study. Arch. Rheumatol. 2019, 35, 60–67. [Google Scholar] [CrossRef]
- Furlan, A.D.; Yazdi, F.; Tsertsvadze, A.; Gross, A.; Van Tulder, M.; Santaguida, L.; Gagnier, J.; Ammendolia, C.; Dryden, T.; Doucette, S.; et al. A systematic review and meta-analysis of efficacy, cost-effectiveness, and safety of selected complementary and alternative medicine for neck and low-back pain. Evid. Based Complement. Altern. Med. 2012, 2012, 953139. [Google Scholar] [CrossRef]
- Alayat, M.S.M.; Mohamed, A.A.; Helal, O.F.; Khaled, O.A. Efficacy of high-intensity laser therapy in the treatment of chronic neck pain: A randomised double-blind placebo-control trial. Lasers Med. Sci. 2016, 31, 687–694. [Google Scholar] [CrossRef]
- Glazov, G.; Yelland, M.; Emery, J. Low-level laser therapy for chronic non-specific low back pain: A meta-analysis of randomised controlled trials. Acupunct. Med. 2016, 34, 328–341. [Google Scholar] [CrossRef]
- Huang, Z.; Ma, J.; Chen, J.; Shen, B.; Pei, F.; Kraus, V.B. The effectiveness of low-level laser therapy for nonspecific chronic low back pain: A systematic review and meta-analysis. Arthritis Res. Ther. 2015, 17, 360. [Google Scholar] [CrossRef]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the N.R.S., VAS, V.R.S., and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.P.; Fu, T.S.; Liu, C.Y.; Hung, C.I. Psychometric evaluation of the oswestry disability index in patients with chronic low back pain: Factor and mokken analyses. Health Qual. Life Outcomes 2017, 15, 192. [Google Scholar] [CrossRef] [PubMed]
- Kholoosy, L.; Elyaspour, D.; Akhgari, M.R.; Razzaghi, Z.; Khodamardi, Z.; Bayat, M. Evaluation of the therapeutic effect of low-level laser in controlling low back pain: A randomised controlled trial. J. Lasers Med. Sci. 2020, 11, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Dommerholt, J.; Hooks, T.; Finnegan, M.; Grieve, R. A critical overview of the current myofascial pain literature—March 2016. J. Bodyw. Mov. Ther. 2016, 20, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.L.K.; Matsutani, L.A.; Marques, A.P. Effectiveness of different styles of massage therapy in fibromyalgia: A systematic review and meta-analysis. Man Ther. 2015, 20, 257–264. [Google Scholar] [CrossRef]
- Castro-Sánchez, A.M.; Matarán-Pe-arrocha, G.A.; Granero-Molina, J.; Aguilera-Manrique, G.; Quesada-Rubio, J.M.; Moreno-Lorenzo, C. Benefits of massage-myofascial release therapy on pain, anxiety, quality of sleep, depression, and quality of life in patients with fibromyalgia. Evid. Based Complement. Altern. Med. 2011, 20, 257–264. [Google Scholar] [CrossRef]
- Castro-Sánchez, A.M.; Matarán-Pe-arrocha, G.A.; Arroyo-Morales, M.; Saavedra-Hernández, M.; Fernández-Sola, C.; Moreno-Lorenzo, C. Effects of myofascial release techniques on pain, physical function, and postural stability in patients with fibromyalgia: A randomised controlled trial. Clin. Rehabil. 2011, 25, 800–813. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, J.H.; Yoon, H.B. Immediate effects of high-frequency diathermy on muscle architecture and flexibility in subjects with gastrocnemius tightness. Phys. Ther. Korea 2020, 27, 133–139. [Google Scholar] [CrossRef]
- Henderson, C.A.; Gomez, C.G.; Novak, S.M.; Mi-Mi, L.; Gregorio, C.C. Overview of the muscle cytoskeleton. Compr. Physiol. 2017, 18, 891–944. [Google Scholar]
- Shamrock, A.G.; Varacallo, M. Achilles Tendon Rupture; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Arnedo, F.; Andrew, A.; Till, L.; Sendrós, S.; Hellín, S. Radiofrecuencia Monopolar Capacitiva/Resistiva 448 kHz (Indiba Activ Therapy) en el Tratamiento Rehabilitador de Lesiones de la Musculatura Isquitibial Derivada de la Práctica Deportiva: XIV Congreso Nacional de la Federación Española de Medicina del Deporte; Santander: Boadilla del Monte, Spain, 2012; Volume XXIX, p. 915. [Google Scholar]
- Ezzati, K.; Laakso, E.L.; Saberi, A.; Chabok, S.Y.; Nasiri, E.; Eghbali, B.B. A comparative study of the dose-dependent effects of low level and high intensity photo-biomodulation (laser) therapy on pain and electrophysiological parameters in patients with carpal tunnel syndrome: A randomised controlled trial. Eur. J. Phys. Rehabil. Med. 2019, 56, 733–740. [Google Scholar] [CrossRef] [PubMed]
- El-Shamy, S.M.; Alayat, M.S.M.; Abdelgalil, A.A.; Alshehri, M.A. Long-term effect of pulsed nd: YAG laser in the treatment of children with juvenile rheumatoid arthritis: A randomized controlled trial. Photomed. Laser Surg. 2018, 36, 445–451. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szabo, D.A.; Neagu, N.; Teodorescu, S.; Predescu, C.; Sopa, I.S.; Panait, L. TECAR Therapy Associated with High-Intensity Laser Therapy (Hilt) and Manual Therapy in the Treatment of Muscle Disorders: A Literature Review on the Theorised Effects Supporting Their Use. J. Clin. Med. 2022, 11, 6149. https://doi.org/10.3390/jcm11206149
Szabo DA, Neagu N, Teodorescu S, Predescu C, Sopa IS, Panait L. TECAR Therapy Associated with High-Intensity Laser Therapy (Hilt) and Manual Therapy in the Treatment of Muscle Disorders: A Literature Review on the Theorised Effects Supporting Their Use. Journal of Clinical Medicine. 2022; 11(20):6149. https://doi.org/10.3390/jcm11206149
Chicago/Turabian StyleSzabo, Dan Alexandru, Nicolae Neagu, Silvia Teodorescu, Corina Predescu, Ioan Sabin Sopa, and Loredana Panait. 2022. "TECAR Therapy Associated with High-Intensity Laser Therapy (Hilt) and Manual Therapy in the Treatment of Muscle Disorders: A Literature Review on the Theorised Effects Supporting Their Use" Journal of Clinical Medicine 11, no. 20: 6149. https://doi.org/10.3390/jcm11206149
APA StyleSzabo, D. A., Neagu, N., Teodorescu, S., Predescu, C., Sopa, I. S., & Panait, L. (2022). TECAR Therapy Associated with High-Intensity Laser Therapy (Hilt) and Manual Therapy in the Treatment of Muscle Disorders: A Literature Review on the Theorised Effects Supporting Their Use. Journal of Clinical Medicine, 11(20), 6149. https://doi.org/10.3390/jcm11206149