
Please Don’t Compliment Me! Fear of Positive Evaluation and Emotion Regulation—Implications for Adolescents’ Social Anxiety


Abstract
1. Introduction
1.1. Fear of Evaluation
1.2. Emotion Regulation
1.3. Do Evaluation Fears Mediate the Link between Social Anxiety and Emotion Regulation?
1.4. The Current Study
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.3.1. Social Anxiety
2.3.2. Fear of Evaluation
2.3.3. Emotion Regulation
2.3.4. Control Variables
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Measurement Model
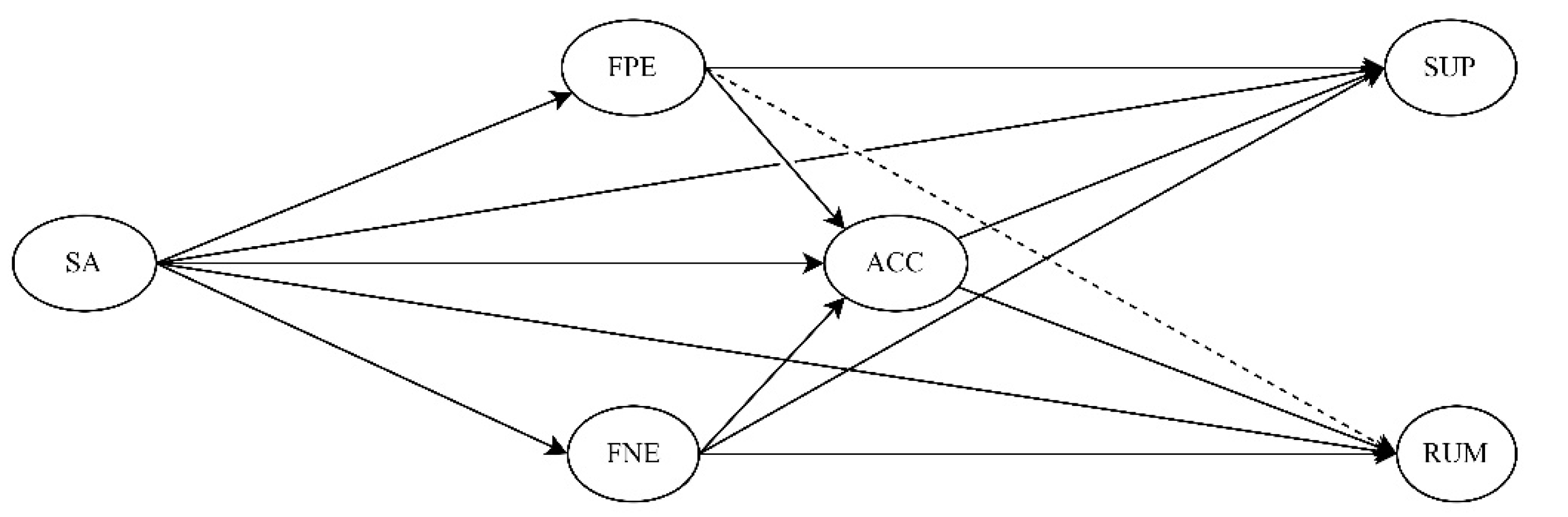
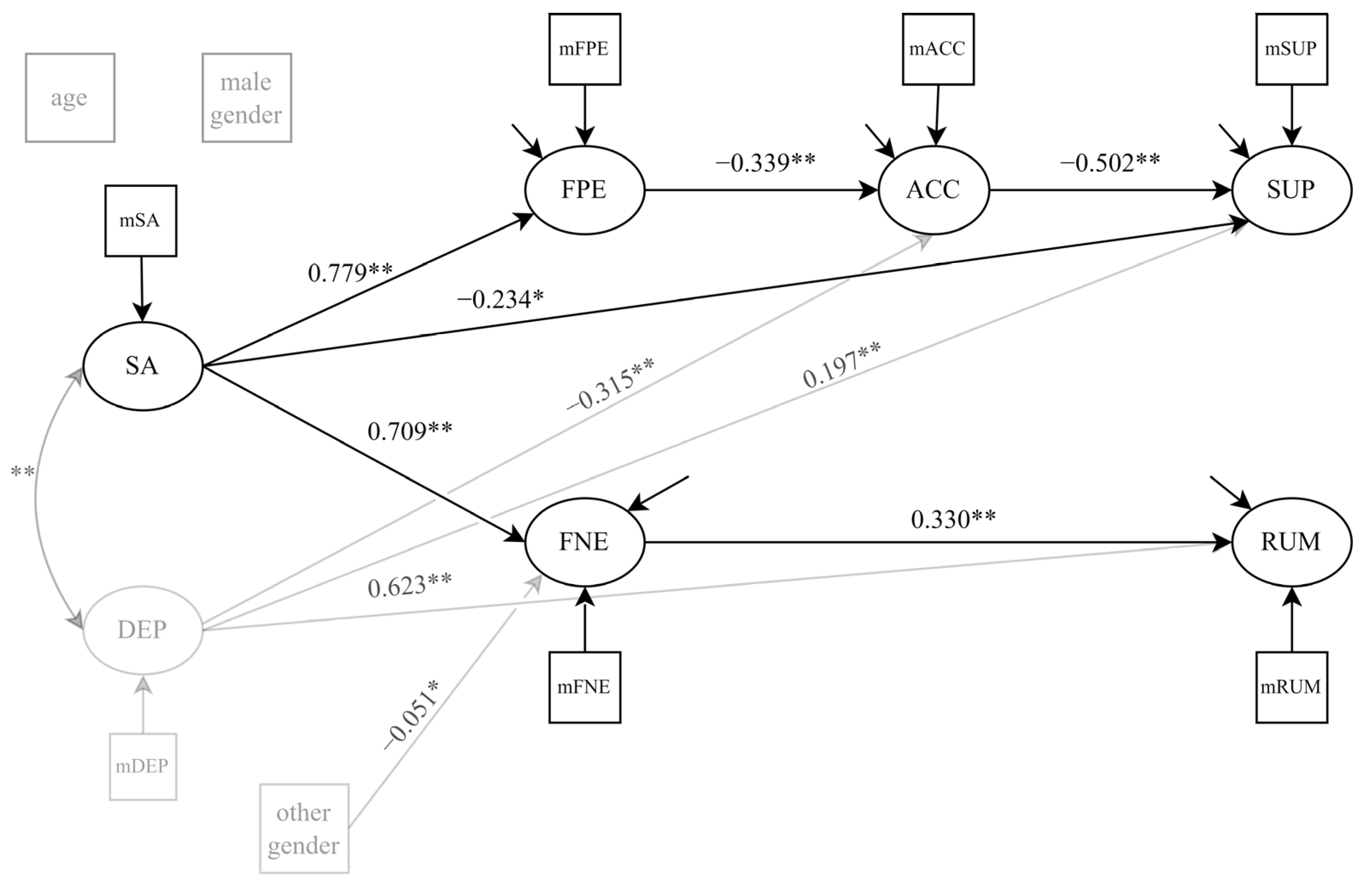
3.3. Structural Model
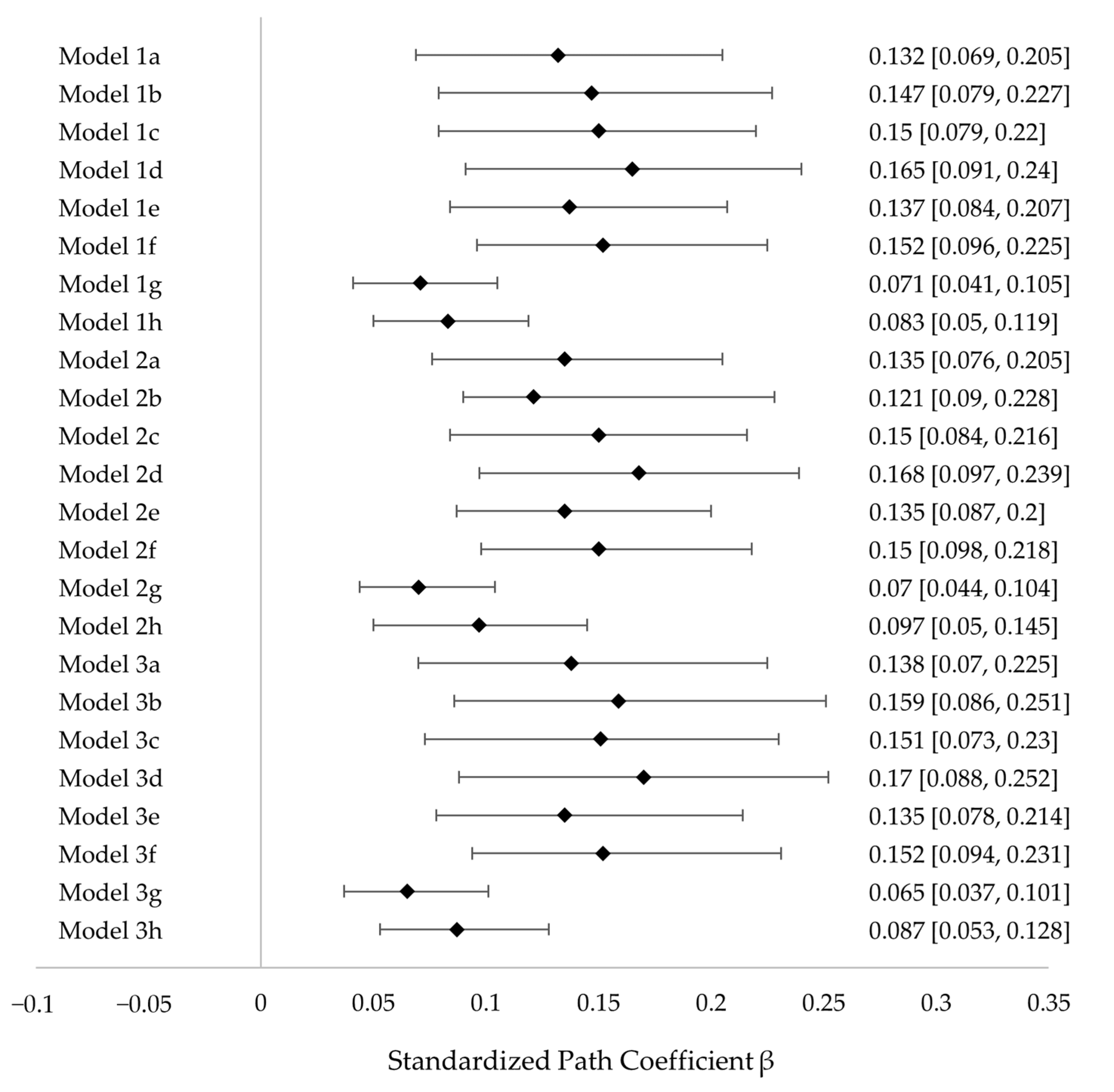
3.4. Multiverse Analyses
4. Discussion
4.1. Practical Implications
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ollendick, T.H.; Benoit, K.E.; Grills-Taquechell, A.E. Social Anxiety Disorder in Children and Adolescents. In The Wiley Blackwell Handbook of Social Anxiety Disorder; Weeks, J.W., Ed.; Wiley Blackwell: Chichester, UK, 2014; pp. 181–200. ISBN 978-1-118-65389-0. [Google Scholar]
- Scaini, S.; Belotti, R.; Ogliari, A.; Battaglia, M. A Comprehensive Meta-Analysis of Cognitive-Behavioral Interventions for Social Anxiety Disorder in Children and Adolescents. J. Anxiety Disord. 2016, 42, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H. Twelve-month and Lifetime Prevalence and Lifetime Morbid Risk of Anxiety and Mood Disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Bruce, S.E.; Yonkers, K.A.; Otto, M.W.; Eisen, J.L.; Weisberg, R.B.; Pagano, M.; Shea, M.T.; Keller, M.B. Influence of Psychiatric Comorbidity on Recovery and Recurrence in Generalized Anxiety Disorder, Social Phobia, and Panic Disorder: A 12-Year Prospective Study. Am. J. Psychiatry 2005, 162, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Spence, S.H.; Rapee, R.M. The Etiology of Social Anxiety Disorder: An Evidence-Based Model. Behav. Res. Ther. 2016, 86, 50–67. [Google Scholar] [CrossRef]
- Heimberg, R.G.; Magee, L. Social Anxiety Disorder. In Clinical Handbook of Psychological Disorders: A Step-by-Step Treatment Manual; Barlow, D.H., Ed.; The Guilford Press: New York, NY, USA, 2014; pp. 114–154. ISBN 978-1-4625-4704-3. [Google Scholar]
- Knappe, S.; Beesdo-Baum, K.; Fehm, L.; Stein, M.B.; Lieb, R.; Wittchen, H.-U. Social Fear and Social Phobia Types among Community Youth: Differential Clinical Features and Vulnerability Factors. J. Psychiatr. Res. 2011, 45, 111–120. [Google Scholar] [CrossRef]
- Knappe, S.; Sasagawa, S.; Creswell, C. Developmental Epidemiology of Social Anxiety and Social Phobia in Adolescents. In Social Anxiety and Phobia in Adolescents; Ranta, K., La Greca, A.M., Garcia-Lopez, L.-J., Marttunen, M., Eds.; Springer International Publishing: Cham, Switzerland, 2015; pp. 39–70. ISBN 978-3-319-16703-9. [Google Scholar]
- Yap, M.B.H.; Allen, N.B.; Sheeber, L. Using an Emotion Regulation Framework to Understand the Role of Temperament and Family Processes in Risk for Adolescent Depressive Disorders. Clin. Child. Fam. Psychol. Rev. 2007, 10, 180–196. [Google Scholar] [CrossRef]
- Westenberg, P.M.; Gullone, E.; Bokhorst, C.L.; Heyne, D.A.; King, N.J. Social Evaluation Fear in Childhood and Adolescence: Normative Developmental Course and Continuity of Individual Differences. Br. J. Dev. Psychol. 2007, 25, 471–483. [Google Scholar] [CrossRef]
- Riediger, M.; Klipker, K. Emotion Regulation in Adolescence. In Handbook of Emotion Regulation; Gross, J.J., Ed.; The Guilford Press: New York, NY, USA, 2014; pp. 187–202. ISBN 978-1-4625-2073-2. [Google Scholar]
- Michiel Westenberg, P.; Drewes, M.J.; Goedhart, A.W.; Siebelink, B.M.; Treffers, P.D.A. A Developmental Analysis of Self-Reported Fears in Late Childhood through Mid-Adolescence: Social-Evaluative Fears on the Rise? J. Child. Psychol. Psychiatry 2004, 45, 481–495. [Google Scholar] [CrossRef]
- Schmitz, J.; Asbrand, J. Soziale Angststörung Im Kindes—Und Jugendalter; Kolhammer Verlag: Stuttgart, Germany, 2020; ISBN 978-3-17-035130-1. [Google Scholar]
- Clark, D.M.; Wells, A. A Cognitive Model of Social Phobia. In Social Phobia: Diagnosis, Assessment, and Treatment; Heimberg, R.G., Liebowitz, M.R., Hope, D.A., Schneier, F.R., Eds.; The Guilford Press: New York, NY, USA, 1995; pp. 69–93. ISBN 978-1-57230-012-5. [Google Scholar]
- Rapee, R.M.; Heimberg, R.G. A Cognitive-Behavioral Model of Anxiety in Social Phobia. Behav. Res. Ther. 1997, 35, 741–756. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- WHO. International Classification of Diseases; 11th Revision; World Health Organization: Geneva, Switzerland, 2018.
- Alden, L.E.; Taylor, C.T.; Mellings, T.M.J.B.; Laposa, J.M. Social Anxiety and the Interpretation of Positive Social Events. J. Anxiety Disord. 2008, 22, 577–590. [Google Scholar] [CrossRef]
- Aderka, I.M.; Hofmann, S.G.; Nickerson, A.; Hermesh, H.; Gilboa-Schechtman, E.; Marom, S. Functional Impairment in Social Anxiety Disorder. J. Anxiety Disord. 2012, 26, 393–400. [Google Scholar] [CrossRef]
- Fredrick, J.W.; Luebbe, A.M. Fear of Positive Evaluation and Social Anxiety: A Systematic Review of Trait-Based Findings. J. Affect. Disord. 2020, 265, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Weeks, J.W.; Heimberg, R.G.; Rodebaugh, T.L.; Norton, P.J. Exploring the Relationship between Fear of Positive Evaluation and Social Anxiety. J. Anxiety Disord. 2008, 22, 386–400. [Google Scholar] [CrossRef] [PubMed]
- Weeks, J.W.; Heimberg, R.G.; Rodebaugh, T.L. The Fear of Positive Evaluation Scale: Assessing a Proposed Cognitive Component of Social Anxiety. J. Anxiety Disord. 2008, 22, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Weeks, J.W.; Howell, A.N. Fear of Positive Evaluation. The Neglected Fear Domain in Social Anxiety. In The Wiley Blackwell Handbook of Social Anxiety Disorder; Weeks, J.W., Ed.; Wiley Blackwell: Chichester, UK, 2014; pp. 433–453. ISBN 978-1-118-65389-0. [Google Scholar]
- Weeks, J.W.; Jakatdar, T.A.; Heimberg, R.G. Comparing and Contrasting Fears of Positive and Negative Evaluation as Facets of Social Anxiety. J. Soc. Clin. Psychol. 2010, 29, 68–94. [Google Scholar] [CrossRef]
- Gilboa-Schechtman, E.; Shachar, I.; Sahar, Y. Positivity Impairment as a Broad-Based Feature of Social Anxiety. In The Wiley Blackwell Handbook of Social Anxiety Disorder; Weeks, J.W., Ed.; Wiley Blackwell: Chichester, UK, 2014; pp. 409–432. ISBN 978-1-118-65389-0. [Google Scholar]
- Weeks, J.W.; Howell, A.N. The Bivalent Fear of Evaluation Model of Social Anxiety: Further Integrating Findings on Fears of Positive and Negative Evaluation. Cogn. Behav. Ther. 2012, 41, 83–95. [Google Scholar] [CrossRef]
- Weeks, J.W.; Zoccola, P.M. “Having the Heart to Be Evaluated”: The Differential Effects of Fears of Positive and Negative Evaluation on Emotional and Cardiovascular Responses to Social Threat. J. Anxiety Disord. 2015, 36, 115–126. [Google Scholar] [CrossRef]
- Reichenberger, J.; Blechert, J. Malaise with Praise: A Narrative Review of 10 Years of Research on the Concept of Fear of Positive Evaluation in Social Anxiety. Depress. Anxiety 2018, 35, 1228–1238. [Google Scholar] [CrossRef]
- Gilbert, P. Evolution and Social Anxiety. Psychiatr. Clin. N. Am. 2001, 24, 723–751. [Google Scholar] [CrossRef]
- Reichenberger, J.; Wiggert, N.; Wilhelm, F.H.; Liedlgruber, M.; Voderholzer, U.; Hillert, A.; Timmer, B.; Blechert, J. Fear of Negative and Positive Evaluation and Reactivity to Social-Evaluative Videos in Social Anxiety Disorder. Behav. Res. Ther. 2019, 116, 140–148. [Google Scholar] [CrossRef]
- Gross, J.J. The Emerging Field of Emotion Regulation: An Integrative Review. Rev. Gen. Psychol. 1998, 2, 271–299. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion Regulation: Current Status and Future Prospects. Psychol. Inq. 2015, 26, 1–26. [Google Scholar] [CrossRef]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-Regulation Strategies across Psychopathology: A Meta-Analytic Review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Heimberg, R.G.; Brozovich, F.A.; Rapee, R.M. A Cognitive-Behavioral Model of Social Anxiety Disorder. In Social Anxiety: Clinical, Developmental, and Social Perspectives; Hofmann, S.G., Di Bartolo, P.M., Eds.; Academic Press: London, UK, 2014; pp. 705–728. ISBN 978-0-12-394427-6. [Google Scholar]
- Dryman, M.T.; Heimberg, R.G. Emotion Regulation in Social Anxiety and Depression: A Systematic Review of Expressive Suppression and Cognitive Reappraisal. Clin. Psychol. Rev. 2018, 65, 17–42. [Google Scholar] [CrossRef]
- Jazaieri, H.; Morrison, A.S.; Goldin, P.R.; Gross, J.J. The Role of Emotion and Emotion Regulation in Social Anxiety Disorder. Curr. Psychiatry Rep. 2015, 17, 531. [Google Scholar] [CrossRef]
- Brozovich, F.; Heimberg, R.G. An Analysis of Post-Event Processing in Social Anxiety Disorder. Clin. Psychol. Rev. 2008, 28, 891–903. [Google Scholar] [CrossRef]
- Mennin, D.S.; McLaughlin, K.A.; Flanagan, T.J. Emotion Regulation Deficits in Generalized Anxiety Disorder, Social Anxiety Disorder, and Their Co-Occurrence. J. Anxiety Disord. 2009, 23, 866–871. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Kashdan, T.B. The Affective Style Questionnaire: Development and Psychometric Properties. J. Psychopathol. Behav. Assess. 2010, 32, 255–263. [Google Scholar] [CrossRef]
- Zawadzki, M.J. Rumination Is Independently Associated with Poor Psychological Health: Comparing Emotion Regulation Strategies. Psychol. Health 2015, 30, 1146–1163. [Google Scholar] [CrossRef]
- Blalock, D.V.; Kashdan, T.B.; Farmer, A.S. Trait and Daily Emotion Regulation in Social Anxiety Disorder. Cogn. Ther. Res. 2016, 40, 416–425. [Google Scholar] [CrossRef]
- Farmer, A.S.; Kashdan, T.B. Social Anxiety and Emotion Regulation in Daily Life: Spillover Effects on Positive and Negative Social Events. Cogn. Behav. Ther. 2012, 41, 152–162. [Google Scholar] [CrossRef]
- Spokas, M.; Luterek, J.A.; Heimberg, R.G. Social Anxiety and Emotional Suppression: The Mediating Role of Beliefs. J. Behav. Ther. Exp. Psychiatry 2009, 40, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Wirtz, C.M.; Hofmann, S.G.; Riper, H.; Berking, M. Emotion Regulation Predicts Anxiety over a Five-Year Interval: A Cross-Lagged Panel Analysis. Depress. Anxiety 2014, 31, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Turk, C.L.; Heimberg, R.G.; Luterek, J.A.; Mennin, D.S.; Fresco, D.M. Emotion Dysregulation in Generalized Anxiety Disorder: A Comparison with Social Anxiety Disorder. Cogn. Ther. Res. 2005, 29, 89–106. [Google Scholar] [CrossRef]
- Goldin, P.R.; Jazaieri, H.; Gross, J.J. Emotion Regulation in Social Anxiety Disorder. In Social Anxiety: Clinical, Developmental, and Social Perspectives; Academic Press: London, UK, 2014; pp. 511–529. ISBN 978-0-12-394427-6. [Google Scholar]
- Ehring, T. Thinking Too Much: Rumination and Psychopathology. World Psychiatry 2021, 20, 441–442. [Google Scholar] [CrossRef]
- Fehm, L.; Schneider, G.; Hoyer, J. Is Post-Event Processing Specific for Social Anxiety? J. Behav. Ther. Exp. Psychiatry 2007, 38, 11–22. [Google Scholar] [CrossRef]
- Everaert, J.; Bronstein, M.V.; Castro, A.A.; Cannon, T.D.; Joormann, J. When Negative Interpretations Persist, Positive Emotions Don’t! Inflexible Negative Interpretations Encourage Depression and Social Anxiety by Dampening Positive Emotions. Behav. Res. Ther. 2020, 124, 103510. [Google Scholar] [CrossRef]
- Zou, J.B.; Abbott, M.J. Self-Perception and Rumination in Social Anxiety. Behav. Res. Ther. 2012, 50, 250–257. [Google Scholar] [CrossRef]
- Brozovich, F.A.; Heimberg, R.G. Mental Imagery and Post-Event Processing in Anticipation of a Speech Performance among Socially Anxious Individuals. Behav. Ther. 2013, 44, 701–716. [Google Scholar] [CrossRef]
- Penney, E.S.; Abbott, M.J. Anticipatory and Post-Event Rumination in Social Anxiety Disorder: A Review of the Theoretical and Empirical Literature. Behav. Chang. 2014, 31, 79–101. [Google Scholar] [CrossRef]
- Mennin, D.S.; Holaway, R.M.; Fresco, D.M.; Moore, M.T.; Heimberg, R.G. Delineating Components of Emotion and Its Dysregulation in Anxiety and Mood Psychopathology. Behav. Ther. 2007, 38, 284–302. [Google Scholar] [CrossRef] [PubMed]
- Rusch, S.; Westermann, S.; Lincoln, T.M. Specificity of Emotion Regulation Deficits in Social Anxiety: An Internet Study. Psychol. Psychother 2012, 85, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Kashdan, T.B.; Farmer, A.S.; Adams, L.M.; Ferssizidis, P.; McKnight, P.E.; Nezlek, J.B. Distinguishing Healthy Adults from People with Social Anxiety Disorder: Evidence for the Value of Experiential Avoidance and Positive Emotions in Everyday Social Interactions. J. Abnorm. Psychol. 2013, 122, 645–655. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, P.M.; Hyett, M.P.; Ehring, T.; Johnson, S.L.; Samtani, S.; Anderson, R.; Moulds, M.L. Transdiagnostic Assessment of Repetitive Negative Thinking and Responses to Positive Affect: Structure and Predictive Utility for Depression, Anxiety, and Mania Symptoms. J. Affect. Disord. 2018, 232, 375–384. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Vine, V.; Gilbert, K.E. Emotions and Rumination. In Handbook of Psychology of Emotions; Mohiyeddini, C., Eysenck, M., Bauer, S., Eds.; Nova: London, UK, 2013; ISBN 978-1-62808-053-7. [Google Scholar]
- Schneider, R.L.; Arch, J.J.; Landy, L.N.; Hankin, B.L. The Longitudinal Effect of Emotion Regulation Strategies on Anxiety Levels in Children and Adolescen. J. Clin. Child. Adolesc. Psychol. 2016, 47, 978–991. [Google Scholar] [CrossRef]
- Young, K.; Sandman, C.; Craske, M. Positive and Negative Emotion Regulation in Adolescence: Links to Anxiety and Depression. Brain Sci. 2019, 9, 76. [Google Scholar] [CrossRef]
- Mathews, B.L.; Kerns, K.A.; Ciesla, J.A. Specificity of Emotion Regulation Difficulties Related to Anxiety in Early Adolescence. J. Adolesc. 2014, 37, 1089–1097. [Google Scholar] [CrossRef]
- Klemanski, D.H.; Curtiss, J.; McLaughlin, K.A.; Nolen-Hoeksema, S. Emotion Regulation and the Transdiagnostic Role of Repetitive Negative Thinking in Adolescents with Social Anxiety and Depression. Cogn. Ther. Res. 2017, 41, 206–219. [Google Scholar] [CrossRef]
- Gómez, O.; Roldán, R.; Ortega-Ruiz, R.; Garcia-Lopez, L. Social Anxiety and Psychosocial Adjustment in Adolescents: Relation with Peer Victimization, Self-Esteem and Emotion Regulation. Child Indic. Res. 2018, 11, 1719–1736. [Google Scholar] [CrossRef]
- Schmitz, J.; Krämer, M.; Tuschen-Caffier, B. Negative Post-Event Processing and Decreased Self-Appraisals of Performance Following Social Stress in Childhood Social Anxiety: An Experimental Study. Behav. Res. Ther. 2011, 49, 789–795. [Google Scholar] [CrossRef]
- Kley, H.; Tuschen-Caffier, B.; Heinrichs, N. Safety Behaviors, Self-Focused Attention and Negative Thinking in Children with Social Anxiety Disorder, Socially Anxious and Non-Anxious Children. J. Behav. Ther. Exp. Psychiatry 2012, 43, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Hodson, K.J.; McManus, F.V.; Clark, D.M.; Doll, H. Can Clark and Wells’ (1995) Cognitive Model of Social Phobia Be Applied to Young People? Behav. Cogn. Psychother. 2008, 36, 449–461. [Google Scholar] [CrossRef]
- Sackl-Pammer, P.; Jahn, R.; Özlü-Erkilic, Z.; Pollak, E.; Ohmann, S.; Schwarzenberg, J.; Plener, P.; Akkaya-Kalayci, T. Social Anxiety Disorder and Emotion Regulation Problems in Adolescents. Child Adolesc. Psychiatry Ment. Health 2019, 13, 37. [Google Scholar] [CrossRef] [PubMed]
- Kashdan, T.B.; Collins, R.L. Social Anxiety and the Experience of Positive Emotion and Anger in Everyday Life: An Ecological Momentary Assessment Approach. Anxiety Stress Coping 2010, 23, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Blanco, I.; Joormann, J. Examining Facets of Depression and Social Anxiety: The Relation among Lack of Positive Affect, Negative Cognitions, and Emotion Dysregulation. Span. J. Psychol. 2017, 20, E51. [Google Scholar] [CrossRef] [PubMed]
- Kashdan, T.B.; Steger, M.F. Expanding the Topography of Social Anxiety: An Experience-Sampling Assessment of Positive Emotions, Positive Events, and Emotion Suppression. Psychol. Sci. 2006, 17, 120–128. [Google Scholar] [CrossRef]
- Storozuk, A.; Ashley, M.; Delage, V.; Maloney, E.A. Got Bots? Practical Recommendations to Protect Online Survey Data from Bot Attacks. Quant. Meth. Psych 2020, 16, 472–481. [Google Scholar] [CrossRef]
- Tabachnik, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson: London, UK, 2013; ISBN 978-0-13-752654-3. [Google Scholar]
- Leiner, D.J. SoSci Survey; Version 3.1.06; SoSci Survey GmbH: Munich, Germany, 2019. [Google Scholar]
- Connor, K.M.; Davidson, J.R.T.; Churchill, L.E.; Sherwood, A.; Weisler, R.H.; Foa, E. Psychometric Properties of the Social Phobia Inventory (SPIN): New Self-Rating Scale. Br. J. Psychiatry 2000, 176, 379–386. [Google Scholar] [CrossRef]
- Von Consbruch, K.; Stangier, U.; Heidenrich, T. Skalen Zur Sozialen Angststörung. Soziale-Phobie-Inventar (SPIN), Soziale-Interaktions-Angst-Skala (SIAS), Liebowitz-Soziale-Angst-Skala, 1st ed.; Hogrefe Verlag: Göttingen, Germany, 2016. [Google Scholar]
- Schwarz, M.; Reichenberger, J.; Schwitalla, M.; König, D.; Wilhelm, F.H.; Voderholzer, U.; Hillert, A.; Blechert, J. Furcht vor positiver sozialer Bewertung: Übersetzung und Validierung einer deutschsprachigen Version der FPES. Diagnostica 2016, 62, 157–168. [Google Scholar] [CrossRef]
- Leary, M.R. A Brief Version of the Fear of Negative Evaluation Scale. Pers. Soc. Psychol. Bull. 1983, 9, 371–375. [Google Scholar] [CrossRef]
- Reichenberger, J.; Schwarz, M.; König, D.; Wilhelm, F.H.; Voderholzer, U.; Hillert, A.; Blechert, J. Angst vor negativer sozialer Bewertung: Übersetzung und Validierung der Furcht vor negativer Evaluation–Kurzskala (FNE-K). Diagnostica 2016, 62, 169–181. [Google Scholar] [CrossRef]
- Graser, J.; Heimlich, C.; Kelava, A.; Hofmann, S.G.; Stangier, U.; Schreiber, F. Erfassung der Emotionsregulation bei Jugendlichen anhand des “Affective Style Questionnaire—Youth (ASQ-Y)”. Diagnostica 2019, 65, 49–59. [Google Scholar] [CrossRef]
- Ehring, T.; Zetsche, U.; Weidacker, K.; Wahl, K.; Schönfeld, S.; Ehlers, A. The Perseverative Thinking Questionnaire (PTQ): Validation of a Content-Independent Measure of Repetitive Negative Thinking. J. Behav. Ther. Exp. Psychiatry 2011, 42, 225–232. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Gräfe, K.; Zipfel, S.; Herzog, W.; Löwe, B. Screening psychischer Störungen mit dem “Gesundheitsfragebogen für Patienten (PHQ-D)”. Diagnostica 2004, 50, 171–181. [Google Scholar] [CrossRef]
- Epkins, C.; Heckler, D. Integrating Etiological Models of Social Anxiety and Depression in Youth: Evidence for a Cumulative Interpersonal Risk Model. Clin. Child. Fam. Psychol. Rev. 2011, 14, 329–376. [Google Scholar] [CrossRef]
- Ranta, K.; Kaltiala-Heino, R.; Koivisto, A.-M.; Tuomisto, M.T.; Pelkonen, M.; Marttunen, M. Age and Gender Differences in Social Anxiety Symptoms during Adolescence: The Social Phobia Inventory (SPIN) as a Measure. Psychiatry Res. 2007, 153, 261–270. [Google Scholar] [CrossRef]
- Sanchis-Sanchis, A.; Grau, M.D.; Moliner, A.-R.; Morales-Murillo, C.P. Effects of Age and Gender in Emotion Regulation of Children and Adolescents. Front. Psychol. 2020, 11, 946. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows; Version 27.0; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Maydeu-Olivares, A. Maximum Likelihood Estimation of Structural Equation Models for Continuous Data: Standard Errors and Goodness of Fit. Struct. Equ. Model. 2017, 24, 383–394. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Lai, K. Estimating Standardized SEM Parameters Given Nonnormal Data and Incorrect Model: Methods and Comparison. Struct. Equ. Model. 2018, 25, 600–620. [Google Scholar] [CrossRef]
- Hoyle, R.H. Handbook of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2012; ISBN 978-1-4625-1679-7. [Google Scholar]
- Trizano-Hermosilla, I.; Alvarado, J.M. Best Alternatives to Cronbach’s Alpha Reliability in Realistic Conditions: Congeneric and Asymmetrical Measurements. Front. Psychol. 2016, 7, 769. [Google Scholar] [CrossRef] [PubMed]
- Hayduk, L.A.; Littvay, L. Should Researchers Use Single Indicators, Best Indicators, or Multiple Indicators in Structural Equation Models? BMC Med. Res. Methodol. 2012, 12, 159. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; Guilford Press: New York, NY, USA, 2006; ISBN 978-1-4625-1536-3. [Google Scholar]
- Simmons, J.P.; Nelson, L.D.; Simonsohn, U. False-Positive Psychology: Undisclosed Flexibility in Data Collection and Analysis Allows Presenting Anything as Significant. Psychol. Sci. 2011, 22, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Steegen, S.; Tuerlinckx, F.; Gelman, A.; Vanpaemel, W. Increasing Transparency through a Multiverse Analysis. Perspect. Psychol. Sci. 2016, 11, 702–712. [Google Scholar] [CrossRef]
- Akinwande, M.O.; Dikko, H.G.; Samson, A. Variance Inflation Factor: As a Condition for the Inclusion of Suppressor Variable(s) in Regression Analysis. Open J. Stat. 2015, 5, 754–767. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Chmielewski, M.; Kotov, R. The Value of Suppressor Effects in Explicating the Construct Validity of Symptom Measures. Psychol. Assess. 2013, 25, 929. [Google Scholar] [CrossRef]
- Paulhus, D.L.; Robins, R.W.; Trzesniewski, K.H.; Tracy, J.L. Two Replicable Suppressor Situations in Personality Research. Multivar. Behav. Res. 2004, 39, 303–328. [Google Scholar] [CrossRef]
- Hofmann, S.G. Interpersonal Emotion Regulation Model of Mood and Anxiety Disorders. Cogn. Ther. Res. 2014, 38, 483–492. [Google Scholar] [CrossRef]
- Jose, P.E.; Wilkins, H.; Spendelow, J.S. Does Social Anxiety Predict Rumination and Co-Rumination Among Adolescents? J. Clin. Child. Adolesc. Psychol. 2012, 41, 86–91. [Google Scholar] [CrossRef]
- Carpenter, J.K.; Andrews, L.A.; Witcraft, S.M.; Powers, M.B.; Smits, J.A.J.; Hofmann, S.G. Cognitive Behavioral Therapy for Anxiety and Related Disorders: A Meta-analysis of Randomized Placebo-controlled Trials. Depress. Anxiety 2018, 35, 502–514. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.L.; Rapee, R.M.; Lyneham, H.J.; McLellan, L.F.; Wuthrich, V.M.; Schniering, C.A. Comparing Outcomes for Children with Different Anxiety Disorders Following Cognitive Behavioural Therapy. Behav. Res. Ther. 2015, 72, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Weeks, J.W.; Wilmer, M.T.; Potter, C.M.; Waldron, E.M.; Versella, M.; Kaplan, S.C.; Jensen, D.; Heimberg, R.G. Targeting Fear of Positive Evaluation in Patients with Social Anxiety Disorder via a Brief Cognitive Behavioural Therapy Protocol: A Proof-of-Principle Study. Behav. Cogn. Psychother. 2020, 48, 745–750. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: The Process and Practice of Mindful Change, 2nd ed.; The Guilford Press: New York, NY, USA, 2012; ISBN 978-1-4625-2894-3. [Google Scholar]
- Herbert, J.D.; Forman, E.M.; Kaye, J.L.; Gershkovich, M.; Goetter, E.; Yuen, E.K.; Glassman, L.; Goldstein, S.; Hitchcock, P.; Tronieri, J.S.; et al. Randomized Controlled Trial of Acceptance and Commitment Therapy versus Traditional Cognitive Behavior Therapy for Social Anxiety Disorder: Symptomatic and Behavioral Outcomes. J. Context. Behav. Sci. 2018, 9, 88–96. [Google Scholar] [CrossRef]
- Niles, A.N.; Burklund, L.J.; Arch, J.J.; Lieberman, M.D.; Saxbe, D.; Craske, M.G. Cognitive Mediators of Treatment for Social Anxiety Disorder: Comparing Acceptance and Commitment Therapy and Cognitive-Behavioral Therapy. Behav. Ther. 2014, 45, 664–677. [Google Scholar] [CrossRef]
- Gross, J.T.; Cassidy, J. Expressive Suppression of Negative Emotions in Children and Adolescents: Theory, Data, and a Guide for Future Research. Dev. Psychol. 2019, 55, 1938–1950. [Google Scholar] [CrossRef]
- Wolniewicz, C.A.; Tiamiyu, M.F.; Weeks, J.W.; Elhai, J.D. Problematic Smartphone Use and Relations with Negative Affect, Fear of Missing out, and Fear of Negative and Positive Evaluation. Psychiatry Res. 2018, 262, 618–623. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Conditional Process Analysis: Concepts, Computation, and Advances in the Modeling of the Contingencies of Mechanisms. Am. Behav. Sci. 2020, 64, 19–54. [Google Scholar] [CrossRef]
- Aldao, A.; Sheppes, G.; Gross, J.J. Emotion Regulation Flexibility. Cogn. Ther. Res. 2015, 39, 263–278. [Google Scholar] [CrossRef]
- Kobylińska, D.; Kusev, P. Flexible Emotion Regulation: How Situational Demands and Individual Differences Influence the Effectiveness of Regulatory Strategies. Front. Psychol. 2019, 10, 72. [Google Scholar] [CrossRef]
- Ranta, K.; Kaltiala-Heino, R.; Rantanen, P.; Tuomisto, M.T.; Marttunen, M. Screening Social Phobia in Adolescents from General Population: The Validity of the Social Phobia Inventory (SPIN) against a Clinical Interview. Eur. Psychiatry 2007, 22, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Richardson, L.P.; McCauley, E.; Grossman, D.C.; McCarty, C.A.; Richards, J.; Russo, J.E.; Rockhill, C.; Katon, W. Evaluation of the Patient Health Questionnaire-9 Item for Detecting Major Depression Among Adolescents. Pediatrics 2010, 126, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Wagner, G.; Zeiler, M.; Waldherr, K.; Philipp, J.; Truttmann, S.; Dür, W.; Treasure, J.L.; Karwautz, A.F.K. Mental Health Problems in Austrian Adolescents: A Nationwide, Two-Stage Epidemiological Study Applying DSM-5 Criteria. Eur. Child Adolesc. Psychiatry 2017, 26, 1483–1499. [Google Scholar] [CrossRef] [PubMed]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-Analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | n | % |
|---|---|---|
| Gender | ||
| Male | 65 | 10.0 |
| Female | 554 | 85.6 |
| Other | 28 | 4.3 |
| Residency | ||
| Austria | 251 | 38.8 |
| Germany | 394 | 60.9 |
| Italy | 2 | 0.3 |
| First Language | ||
| German | 579 | 89.5 |
| Other | 68 | 10.5 |
| Current Household (Living Together) | ||
| Both Parents | 434 | 67.1 |
| Mother | 141 | 21.8 |
| Father | 22 | 3.4 |
| Other | 50 | 7.7 |
| Current Education | ||
| Middle School | 4 | 0.6 |
| High School | 547 | 84.8 |
| Vocational School | 31 | 4.8 |
| Special Needs School | 6 | 0.9 |
| Other | 57 | 8.8 |
| Psychotherapy | ||
| Yes | 165 | 25.5 |
| No | 482 | 74.5 |
| Physical Disability | ||
| Yes | 61 | 9.4 |
| No | 586 | 90.6 |
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. | SA | 1.99 | 0.87 | - | |||||
| 2. | FNE | 2.73 | 0.92 | 0.664 ** | - | ||||
| 3. | FPE | 3.98 | 2.08 | 0.698 ** | 0.496 ** | - | |||
| 4. | RUM | 2.64 | 0.70 | 0.561 ** | 0.571 ** | 0.449 ** | - | ||
| 5. | SUP | 3.49 | 0.79 | 0.231 ** | 0.192 ** | 0.264 ** | 0.254 ** | - | |
| 6. | ACC | 3.21 | 0.88 | −0.389 ** | −0.250 ** | −0.409 ** | −0.298 ** | −0.471 ** | - |
| 7. | DEP | 1.53 | 0.71 | 0.611 ** | 0.467 ** | 0.475 ** | 0.673 ** | 0.322 ** | −0.404 ** |
| Questionnaire | RMSEA | CFI | TLI | SRMR | McDonald’s ω |
|---|---|---|---|---|---|
| SPIN | 0.074 [0.067, 0.080] | 0.920 | 0.905 | 0.050 | 0.929 |
| FPES | 0.066 [0.050, 0.083] | 0.971 | 0.955 | 0.030 | 0.868 |
| BFNE | 0.070 [0.060, 0.079] | 0.957 | 0.944 | 0.032 | 0.945 |
| ASQ–Y: Acceptance | 0.068 [0.060, 0.076] | 0.922 | 0.902 | 0.063 | 0.835 |
| ASQ–Y: Suppression | 0.833 | ||||
| PTQ | 0.066 [0.059, 0.074] | 0.931 | 0.917 | 0.043 | 0.922 |
| PHQ-9 | 0.073 [0.059, 0.086] | 0.953 | 0.937 | 0.036 | 0.871 |
| Direct Effects | b | BC 95% CI | β | BC 95% CI | p | R2 |
|---|---|---|---|---|---|---|
| Fear of Positive Evaluation | 0.608 | |||||
| SA | 1.786 | [1.655, 1.906] | 0.779 | [0.732, 0.817] | <0.001 | |
| Gender (F vs. M) | 0.100 | [−0.244, 0.468] | 0.015 | [−0.037, 0.070] | 0.580 | |
| Gender (F vs. O) | −0.016 | [−0.512, 0.445] | −0.002 | [−0.052, 0.046] | 0.948 | |
| Age | 0.082 | [−0.040, 0.205] | 0.039 | [−0.019, 0.097] | 0.184 | |
| Fear of Negative Evaluation | 0.508 | |||||
| SA | 0.732 | [0.676, 0.794] | 0.709 | [0.667, 0.749] | <0.001 | |
| Gender (F vs. M) | -0.128 | [−0.324, 0.060] | −0.043 | [−0.108, 0.021] | 0.193 | |
| Gender (F vs. O) | −0.222 | [−0.436, −0.001] | −0.051 | [−0.099, 0.000] | 0.048 | |
| Age | 0.019 | [−0.035, 0.072] | 0.021 | [−0.038, 0.077] | 0.479 | |
| Acceptance | 0.303 | |||||
| SA | −0.014 | [−0.210, 0.168] | −0.015 | [−0.220, 0.180] | 0.880 | |
| FPE | −0.138 | [−0.199, −0.073] | −0.339 | [−0.490, −0.176] | <0.001 | |
| FNE | 0.063 | [−0.040, 0.170] | 0.070 | [−0.044, 0.188] | 0.243 | |
| Depression | −0.373 | [−0.510, −0.234] | −0.315 | [−0.429, −0.197] | <0.001 | |
| Gender (F vs. M) | −0.101 | [−0.298, 0.091] | −0.037 | [−0.111, 0.034] | 0.309 | |
| Gender (F vs. O) | −0.180 | [−0.450, 0.122] | −0.045 | [−0.114, 0.030] | 0.216 | |
| Age | 0.032 | [−0.033, 0.098] | 0.038 | [−0.038, 0.116] | 0.331 | |
| Suppression | 0.346 | |||||
| SA | −0.198 | [−0.366, −0.031] | −0.234 | [−0.429, −0.038] | 0.018 | |
| FPE | 0.035 | [−0.022, 0.095] | 0.096 | [−0.060, 0.258] | 0.239 | |
| FNE | 0.071 | [−0.030, 0.172] | 0.087 | [−0.037, 0.210] | 0.166 | |
| Acceptance | −0.454 | [−0.549, −0.359] | −0.502 | [−0.599, −0.402] | <0.001 | |
| Depression | 0.211 | [0.076, 0.347] | 0.197 | [0.071, 0.325] | 0.002 | |
| Gender (F vs. M) | −0.084 | [−0.270, 0.107] | −0.034 | [−0.113, 0.044] | 0.379 | |
| Gender (F vs. O) | 0.142 | [−0.126, 0.392] | 0.040 | [−0.034, 0.110] | 0.280 | |
| Age | −0.025 | [−0.078, 0.026] | −0.033 | [−0.101, 0.034] | 0.336 | |
| Rumination | 0.634 | |||||
| SA | −0.065 | [−0.177, 0.051] | −0.082 | [−0.221, 0.064] | 0.259 | |
| FPE | 0.023 | [−0.017, 0.064] | 0.066 | [−0.049, 0.185] | 0.268 | |
| FNE | 0.254 | [0.186, 0.321] | 0.330 | [0.242, 0.417] | <0.001 | |
| Acceptance | 0.034 | [−0.034, 0.105] | 0.040 | [−0.039, 0.122] | 0.331 | |
| Depression | 0.629 | [0.528, 0.726] | 0.623 | [0.531, 0.706] | <0.001 | |
| Gender (F vs. M) | −0.047 | [−0.182, 0.080] | -0.021 | [−0.080, 0.034] | 0.481 | |
| Gender (F vs. O) | 0.016 | [−0.193, 0.236] | 0.005 | [−0.055, 0.068] | 0.882 | |
| Age | 0.036 | [−0.002, 0.076] | 0.050 | [−0.003, 0.107] | 0.079 |
| Total and Indirect Effects | b | BC 95% CI | β | BC 95% CI | p |
|---|---|---|---|---|---|
| Acceptance | |||||
| Total Effect | −0.214 | [−0.323, −0.100] | −0.230 | [−0.345, −0.107] | <0.001 |
| Total Indirect Effect | −0.200 | [−0.344, −0.054] | −0.214 | [−0.370, −0.058] | 0.006 |
| 1. SA → FPE → ACC | −0.246 | [−0.361, −0.130] | −0.264 | [−0.387, −0.138] | <0.001 |
| 2. SA → FNE → ACC | 0.046 | [−0.029, 0.125] | 0.050 | [−0.032, 0.135] | 0.245 |
| Suppression | |||||
| Total Effect | 0.015 | [−0.101, 0.126] | 0.018 | [−0.121, 0.149] | 0.798 |
| Total Indirect Effect | 0.212 | [0.079, 0.346] | 0.252 | [0.095, 0.409] | 0.002 |
| 1. SA → FPE → SUP | 0.063 | [−0.038, 0.171] | 0.075 | [−0.046, 0.202] | 0.241 |
| 2. SA → FNE → SUP | 0.052 | [−0.021, 0.127] | 0.062 | [−0.026, 0.151] | 0.168 |
| 3. SA → ACC → SUP | 0.007 | [−0.077, 0.097] | 0.008 | [−0.091, 0.114] | 0.881 |
| 4. SA → FPE → ACC → SUP | 0.112 | [0.058, 0.176] | 0.132 | [0.069, 0.206] | <0.001 |
| 5. SA → FNE → ACC → SUP | −0.021 | [−0.059, 0.013] | −0.025 | [−0.070,0.014] | 0.248 |
| Rumination | |||||
| Total Effect | 0.155 | [0.082, 0.226] | 0.194 | [0.102, 0.284] | <0.001 |
| Total Indirect | 0.220 | [0.133, 0.305] | 0.276 | [0.166, 0.379] | <0.001 |
| 1. SA → FPE → RUM | 0.041 | [−0.030, 0.115] | 0.052 | [−0.037, 0.145] | 0.269 |
| 2. SA → FNE → RUM | 0.186 | [0.134, 0.239] | 0.234 | [0.170, 0.297] | <0.001 |
| 3. SA → ACC → RUM | 0.000 | [−0.015, 0.006] | −0.001 | [−0.019, 0.008] | 0.917 |
| 4. SA → FPE → ACC → RUM | −0.008 | [−0.030, 0.007] | −0.011 | [−0.038, 0.009] | 0.360 |
| 5. SA → FNE → ACC → RUM | 0.002 | [−0.001, 0.011] | 0.002 | [−0.001, 0.014] | 0.532 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsarpalis-Fragkoulidis, A.; van Eickels, R.L.; Zemp, M. Please Don’t Compliment Me! Fear of Positive Evaluation and Emotion Regulation—Implications for Adolescents’ Social Anxiety. J. Clin. Med. 2022, 11, 5979. https://doi.org/10.3390/jcm11205979
Tsarpalis-Fragkoulidis A, van Eickels RL, Zemp M. Please Don’t Compliment Me! Fear of Positive Evaluation and Emotion Regulation—Implications for Adolescents’ Social Anxiety. Journal of Clinical Medicine. 2022; 11(20):5979. https://doi.org/10.3390/jcm11205979
Chicago/Turabian StyleTsarpalis-Fragkoulidis, Achilleas, Rahel Lea van Eickels, and Martina Zemp. 2022. "Please Don’t Compliment Me! Fear of Positive Evaluation and Emotion Regulation—Implications for Adolescents’ Social Anxiety" Journal of Clinical Medicine 11, no. 20: 5979. https://doi.org/10.3390/jcm11205979
APA StyleTsarpalis-Fragkoulidis, A., van Eickels, R. L., & Zemp, M. (2022). Please Don’t Compliment Me! Fear of Positive Evaluation and Emotion Regulation—Implications for Adolescents’ Social Anxiety. Journal of Clinical Medicine, 11(20), 5979. https://doi.org/10.3390/jcm11205979