
Dermoscopy and Trichoscopy in Dermatomyositis—A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
3. Results
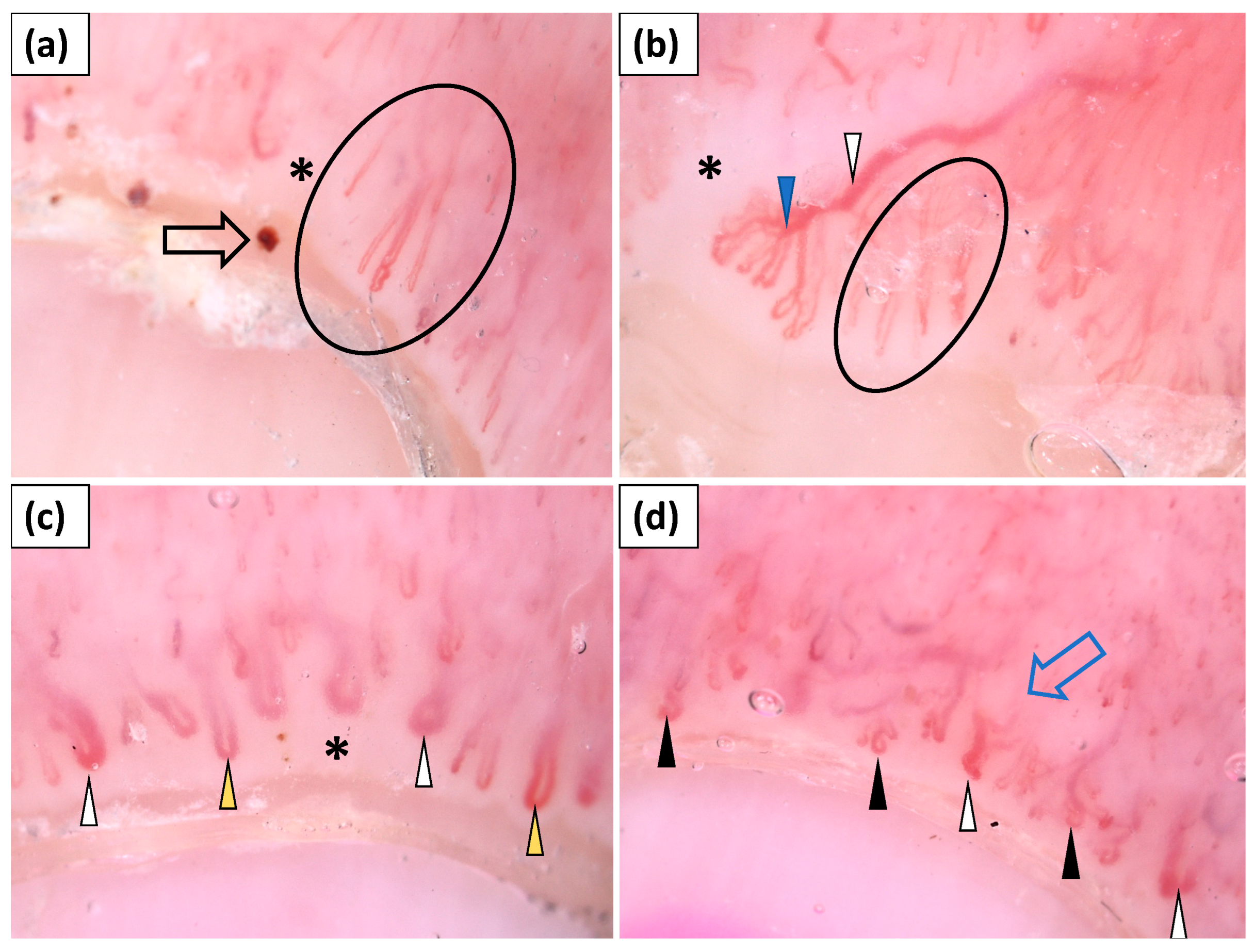
3.1. Capillaroscopy
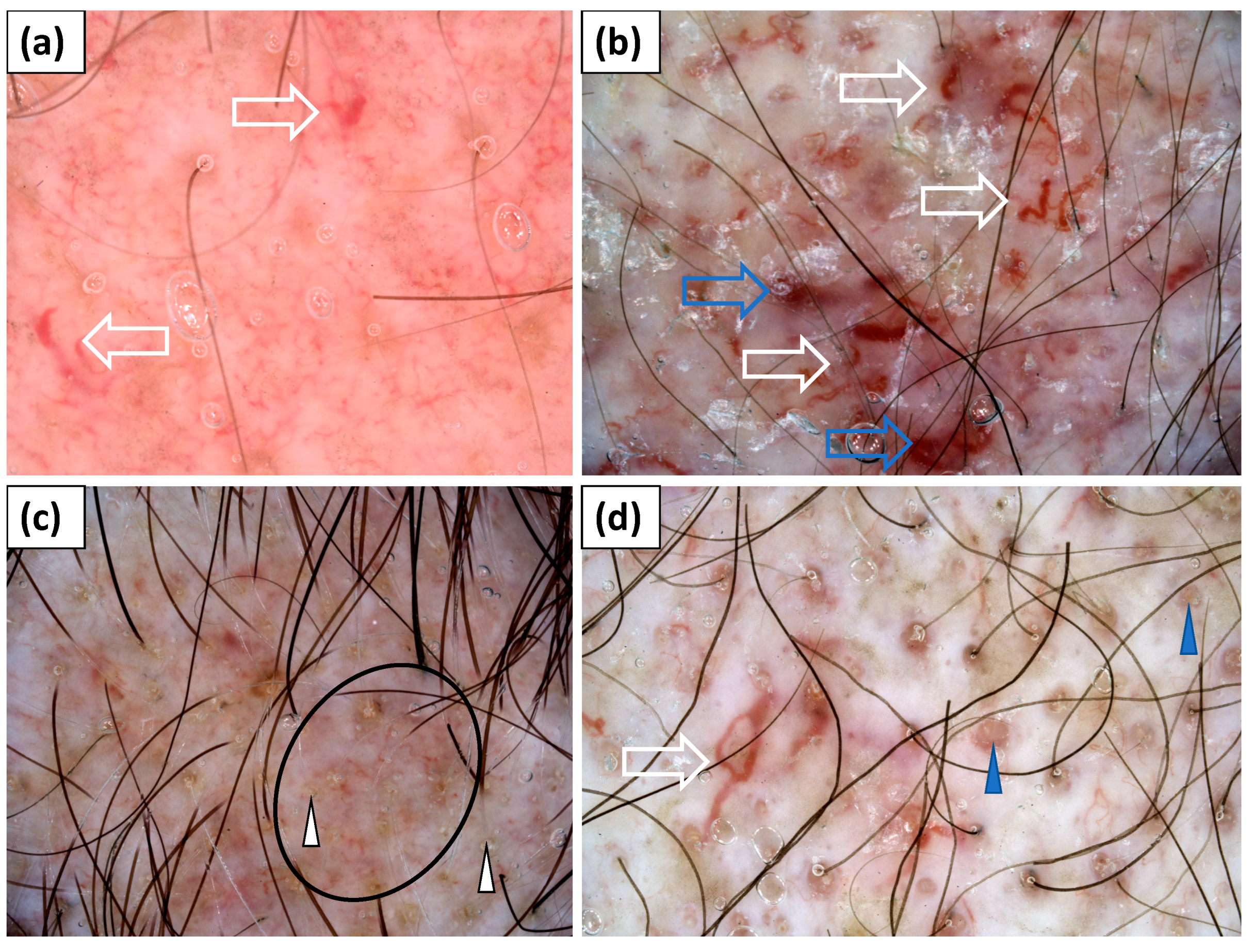
3.2. Trichoscopy
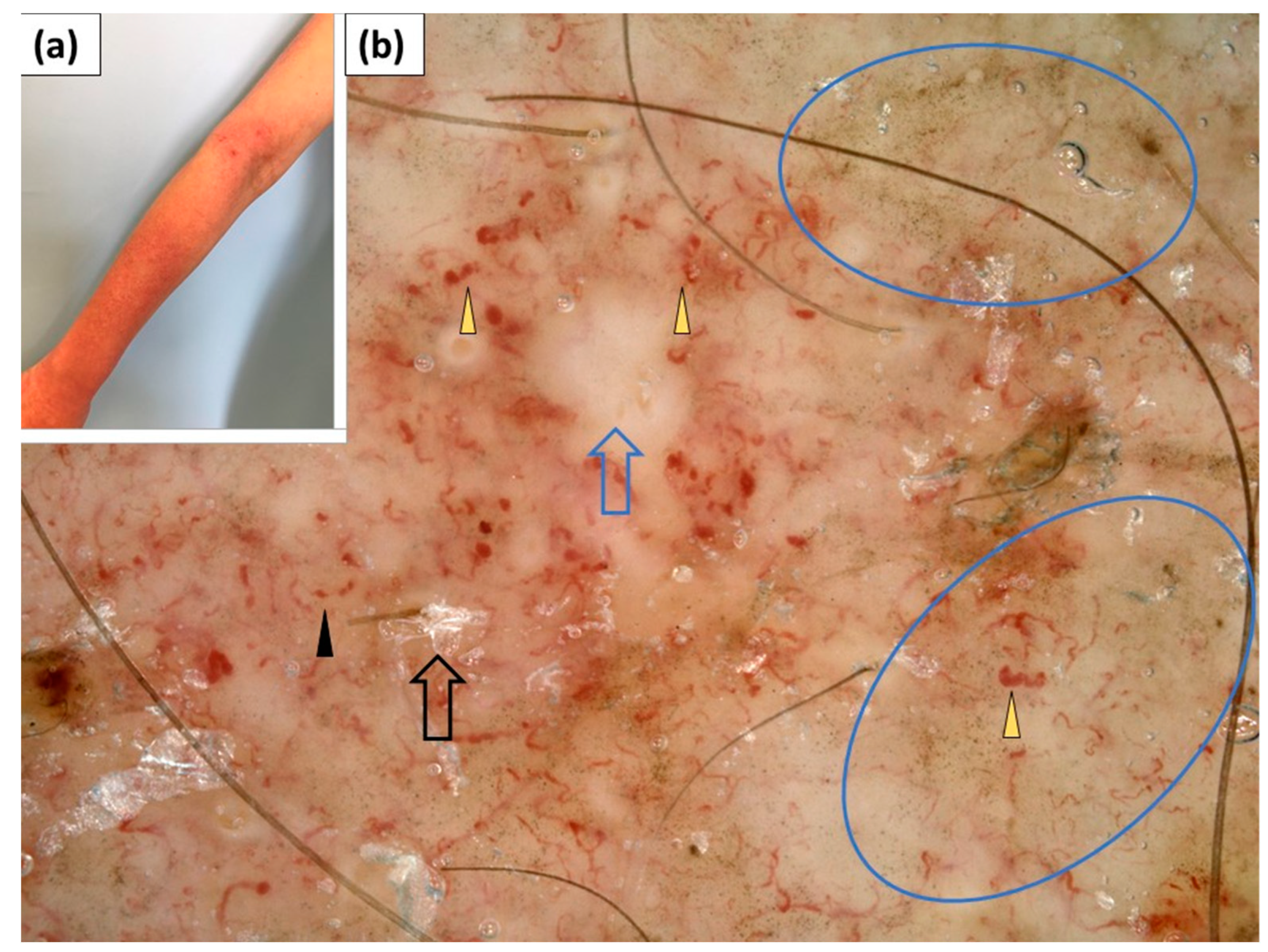
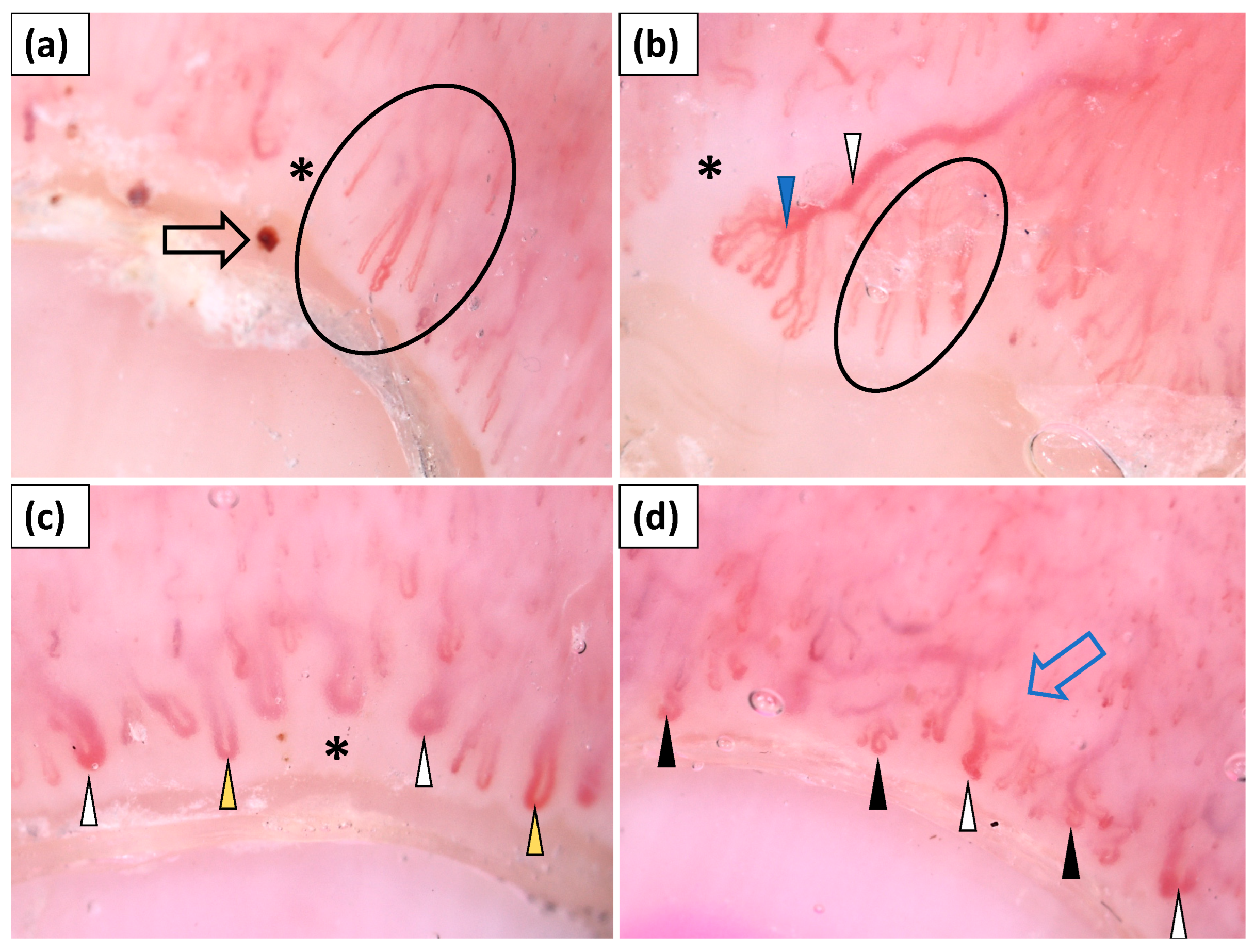
3.3. Dermoscopy of Gottron’s Papules
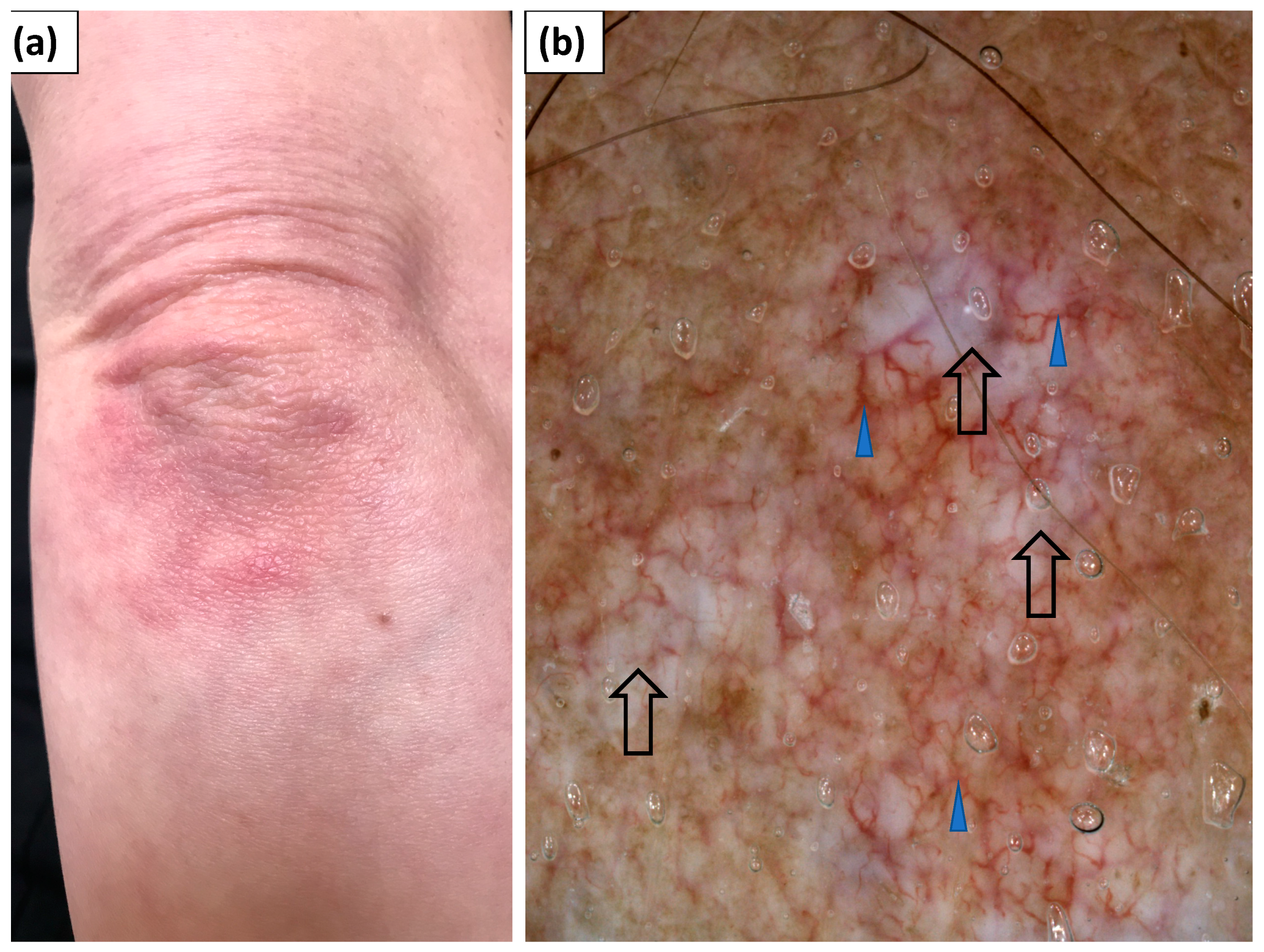
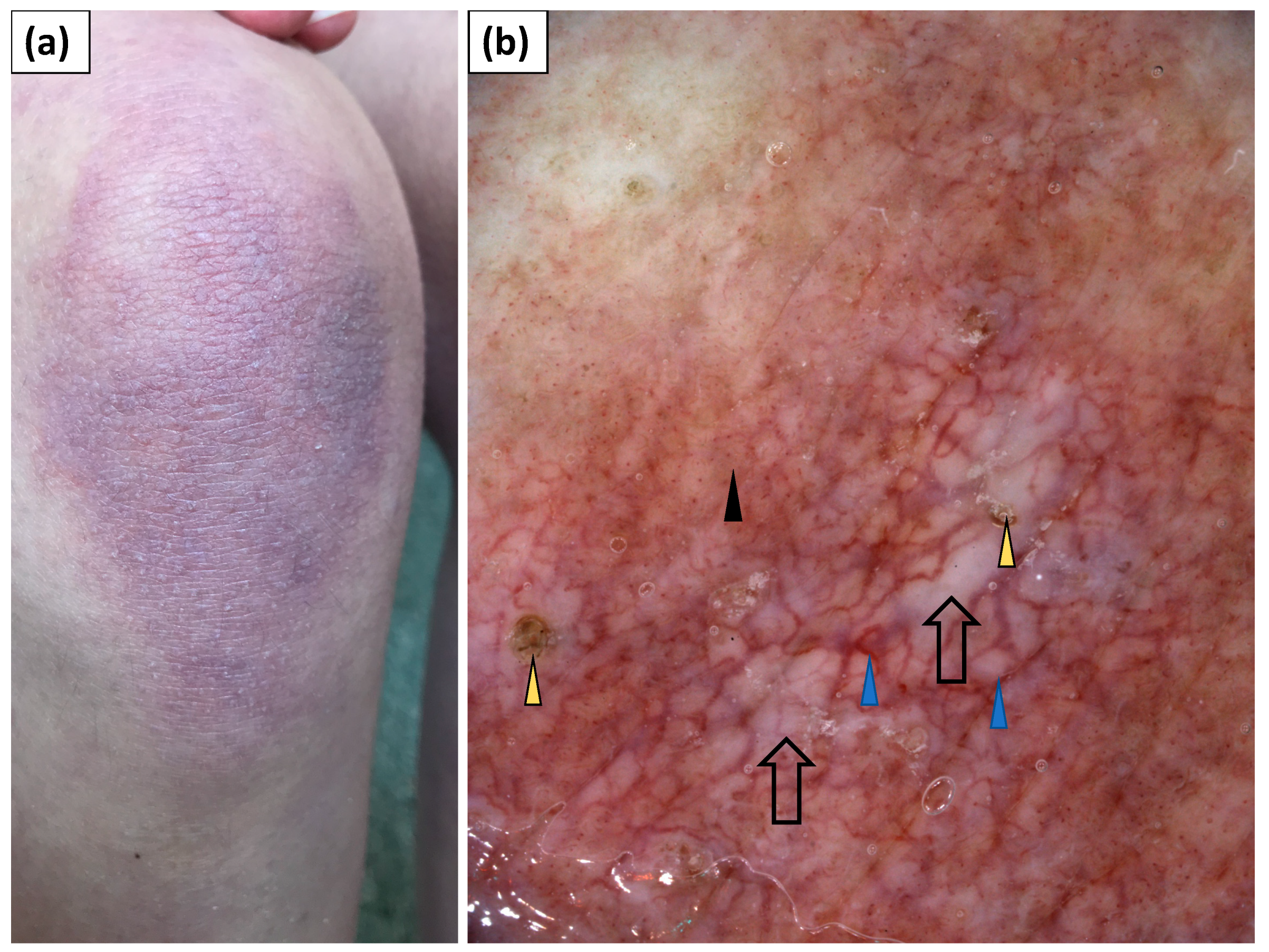
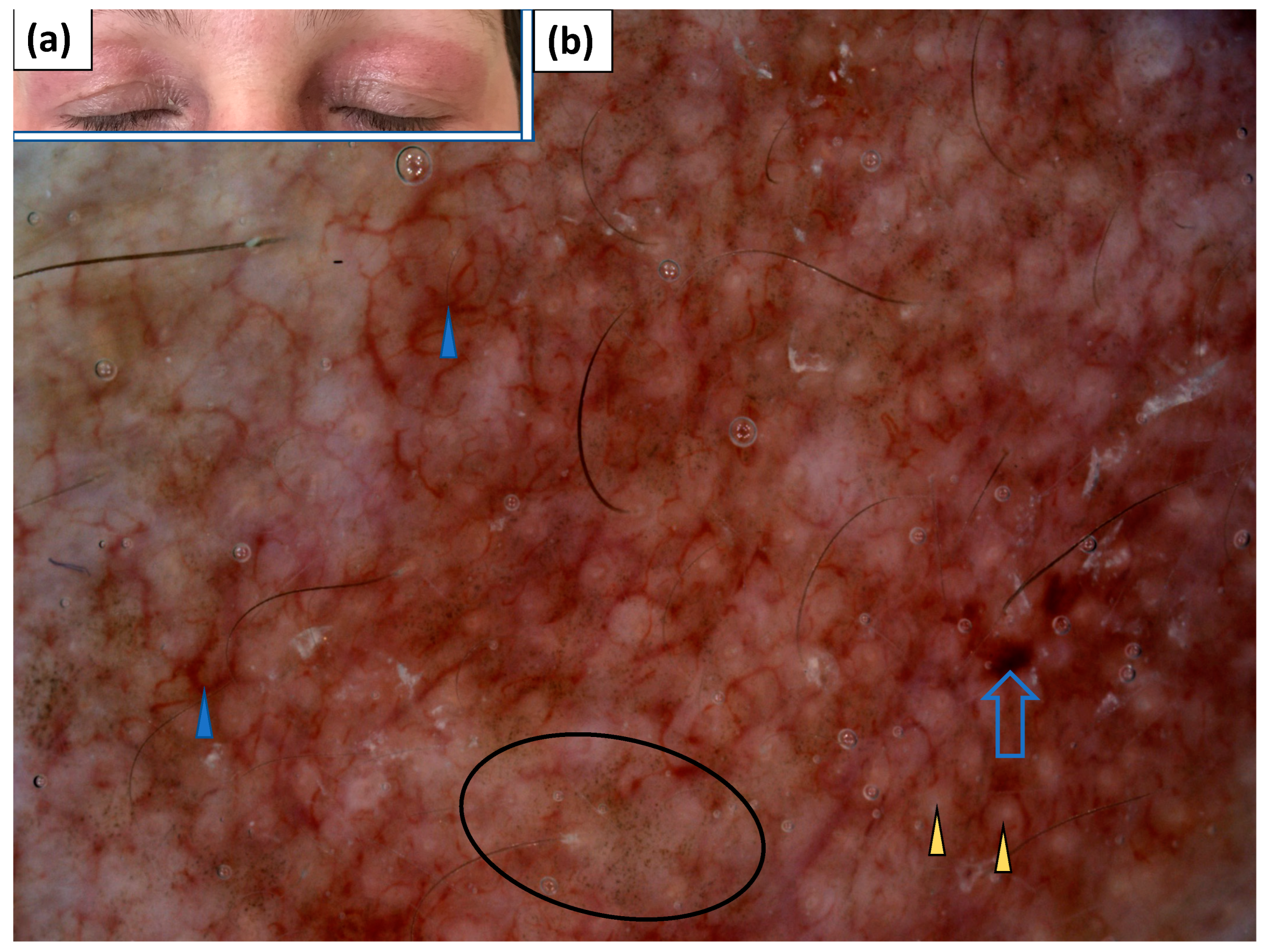
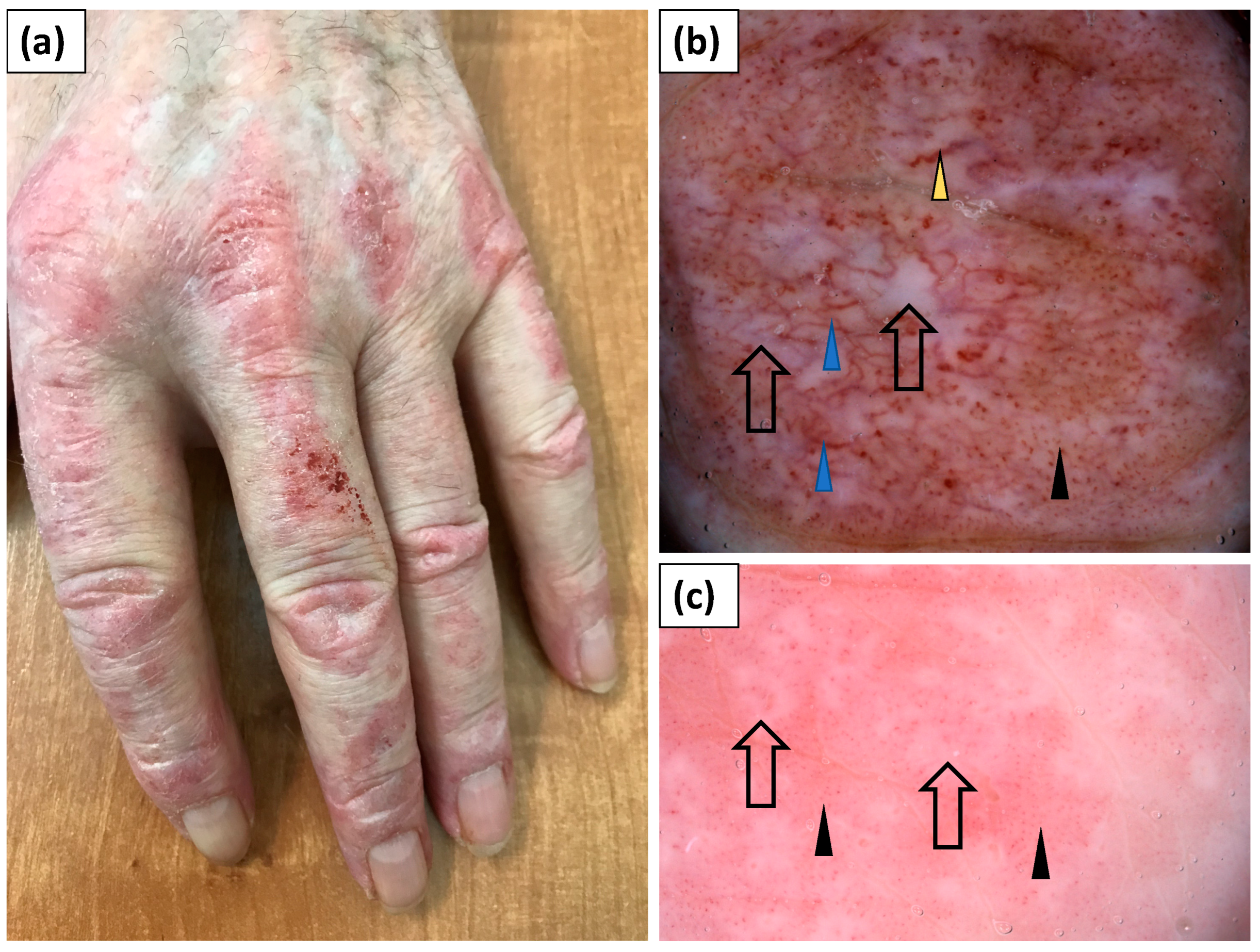
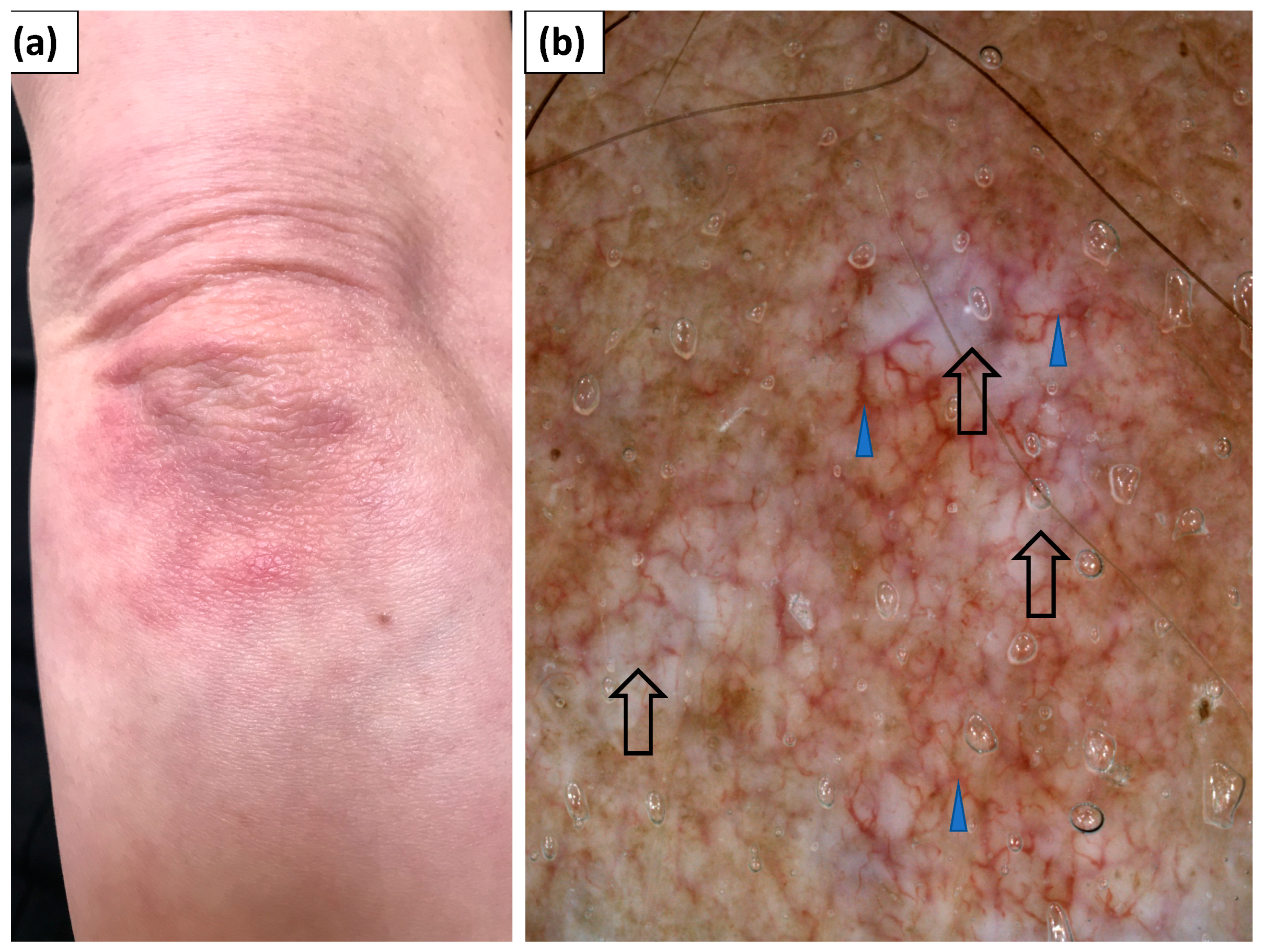
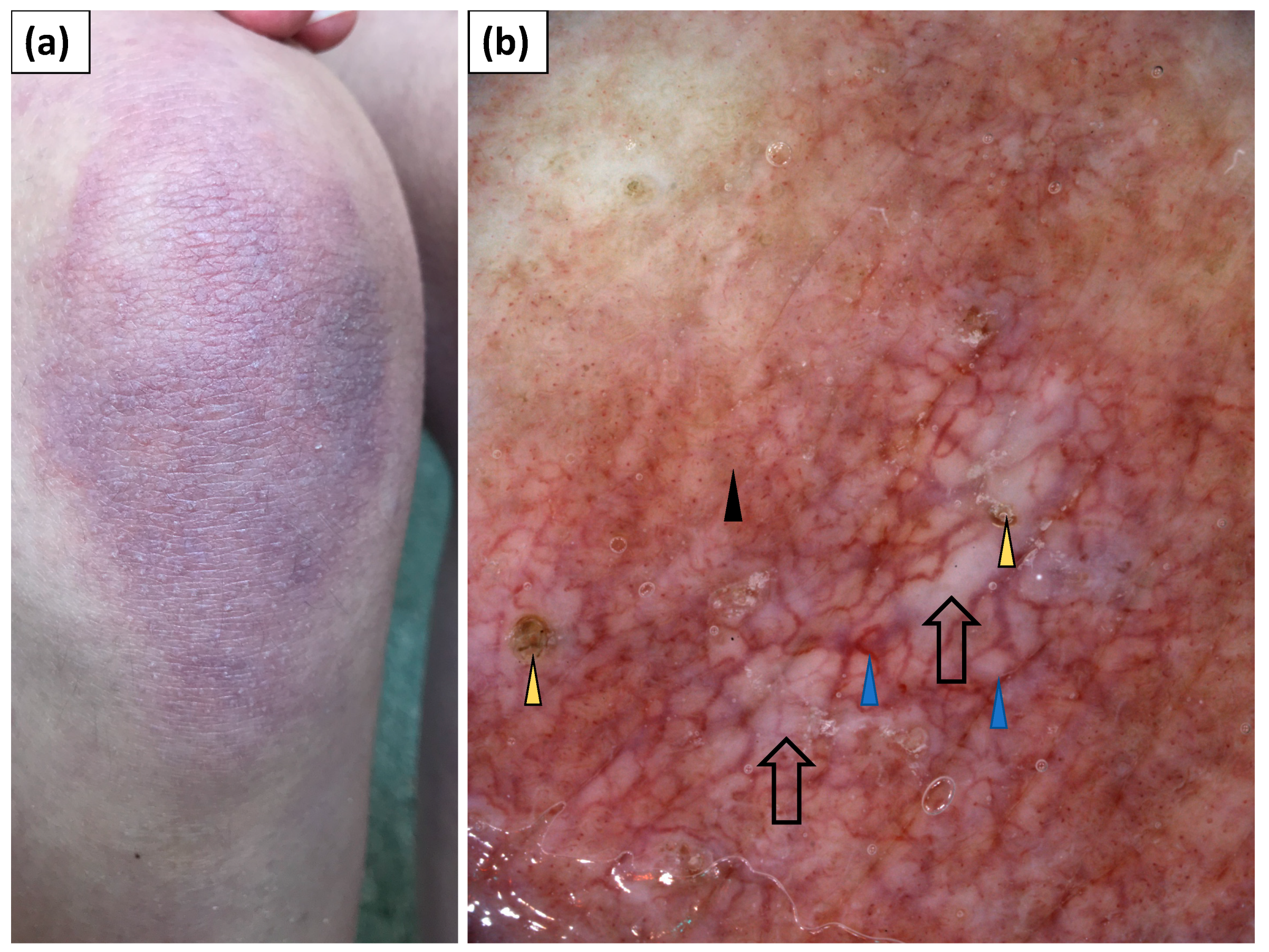
3.4. Dermoscopy of Gottron’s Sign
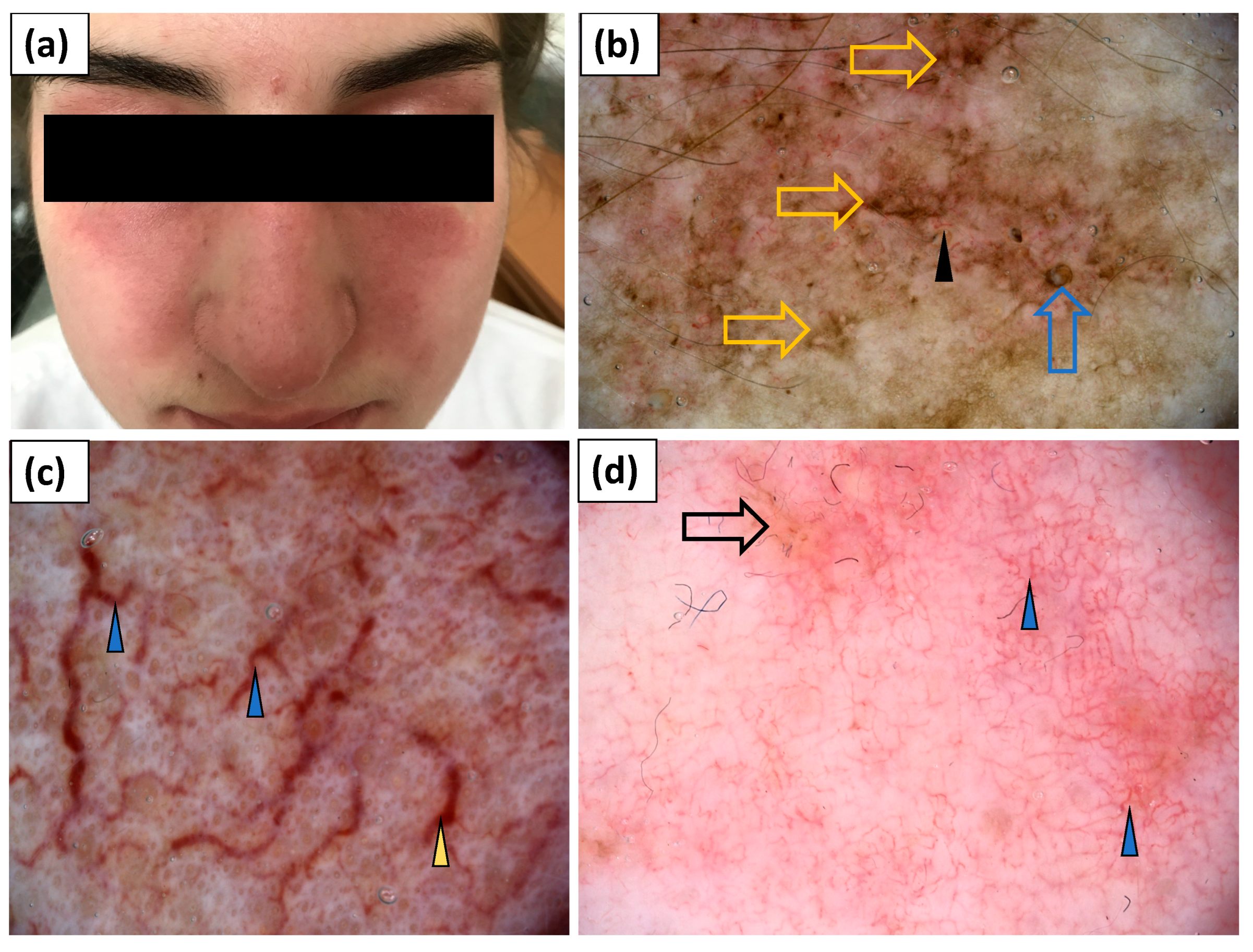
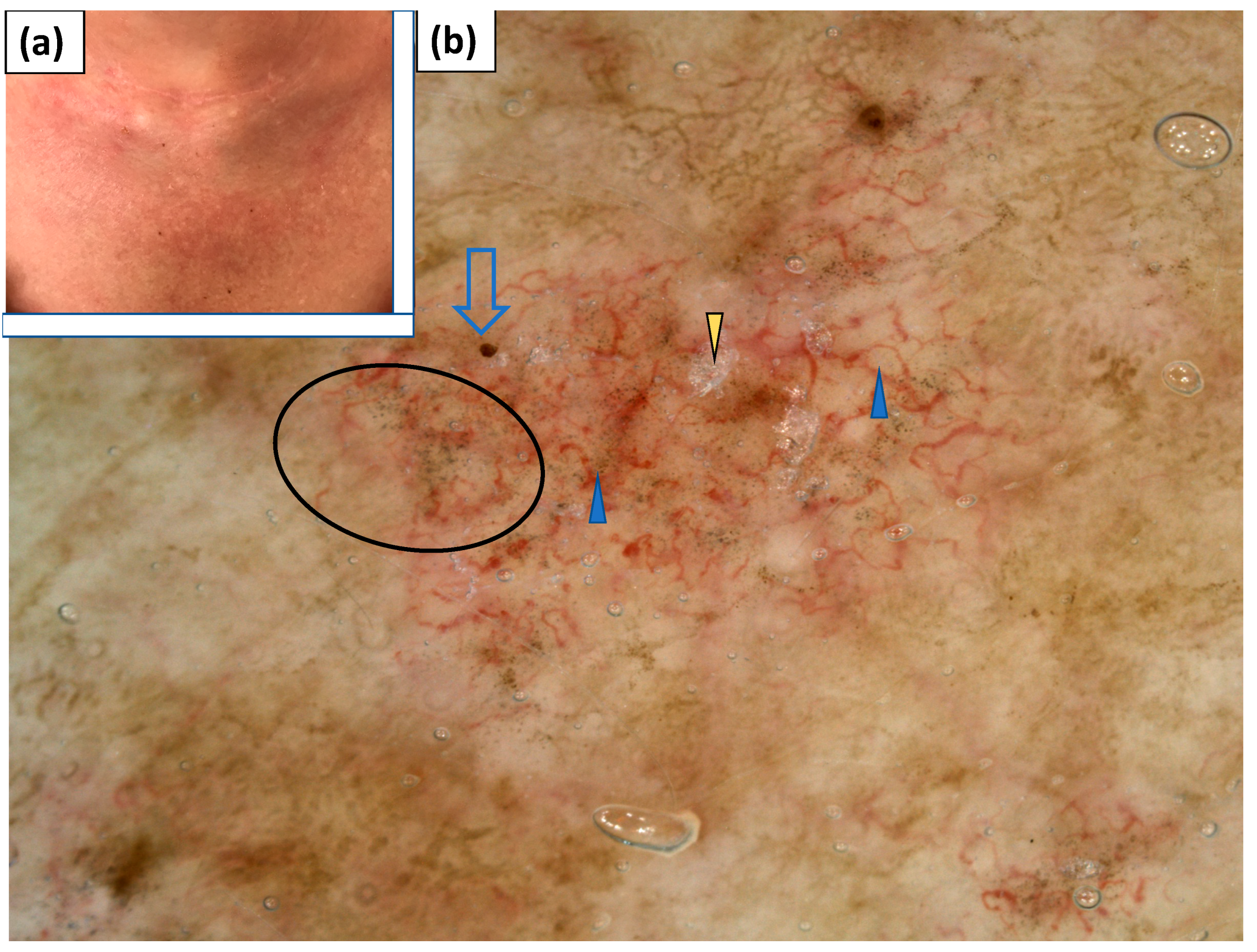
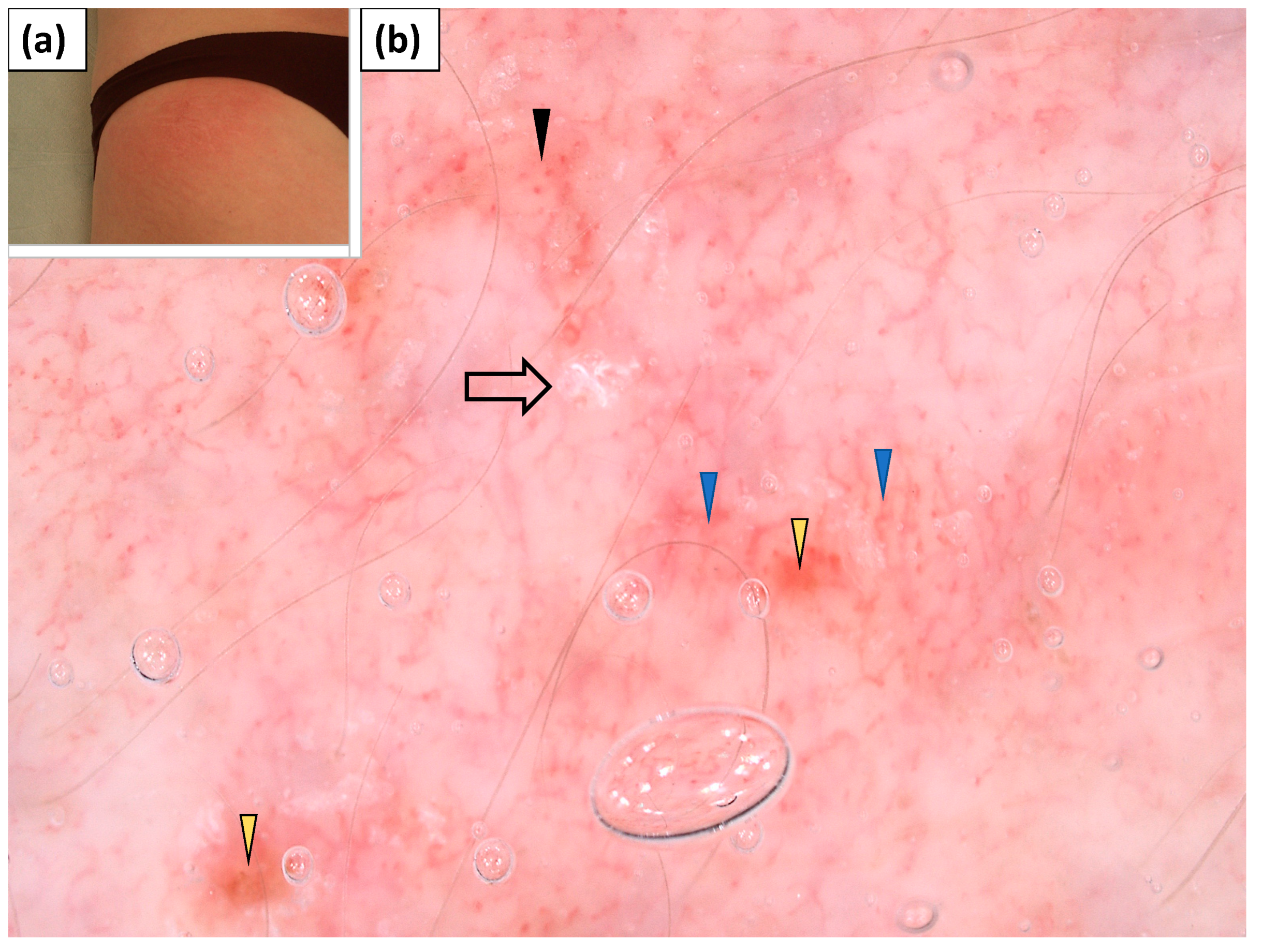
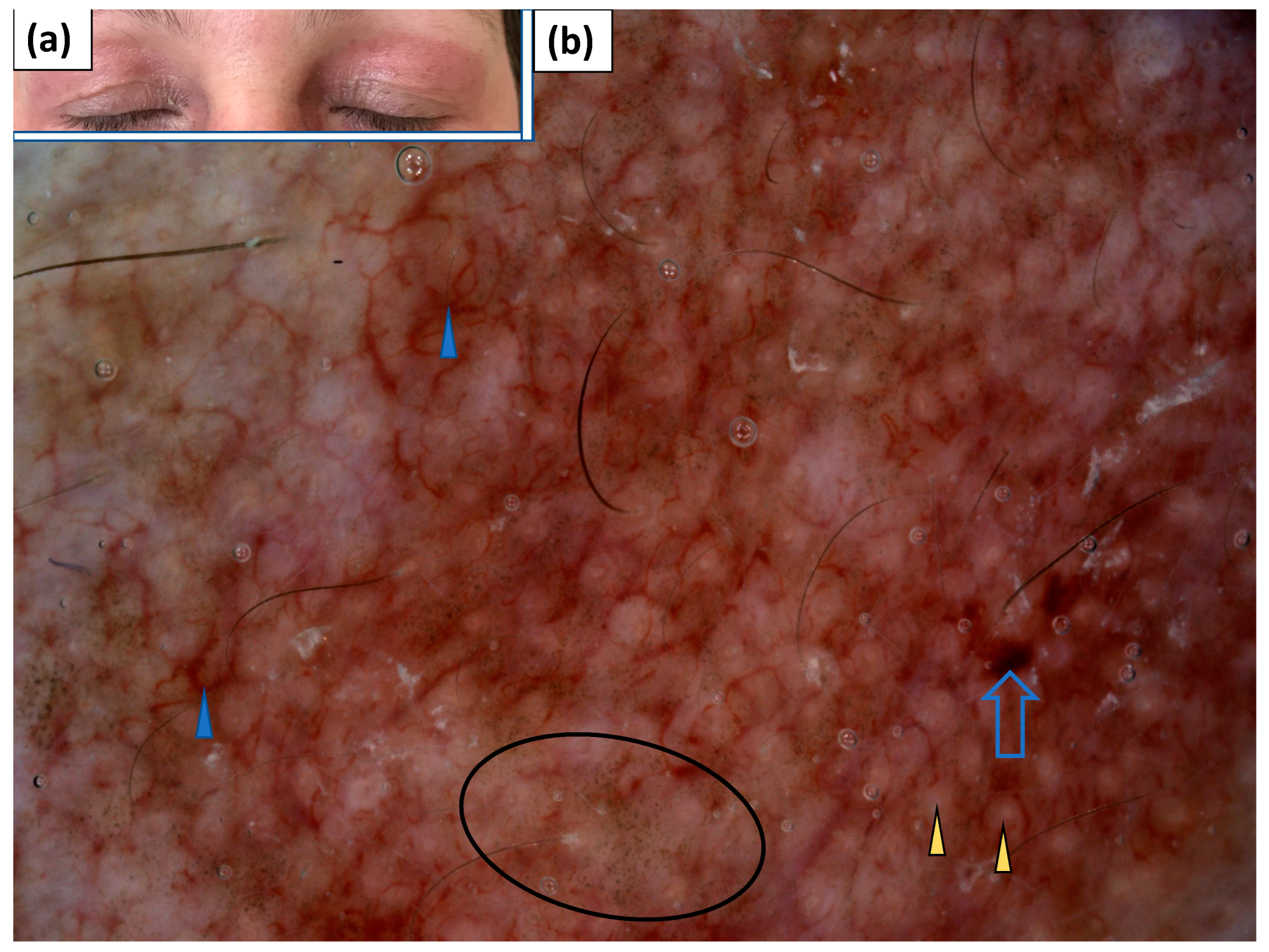
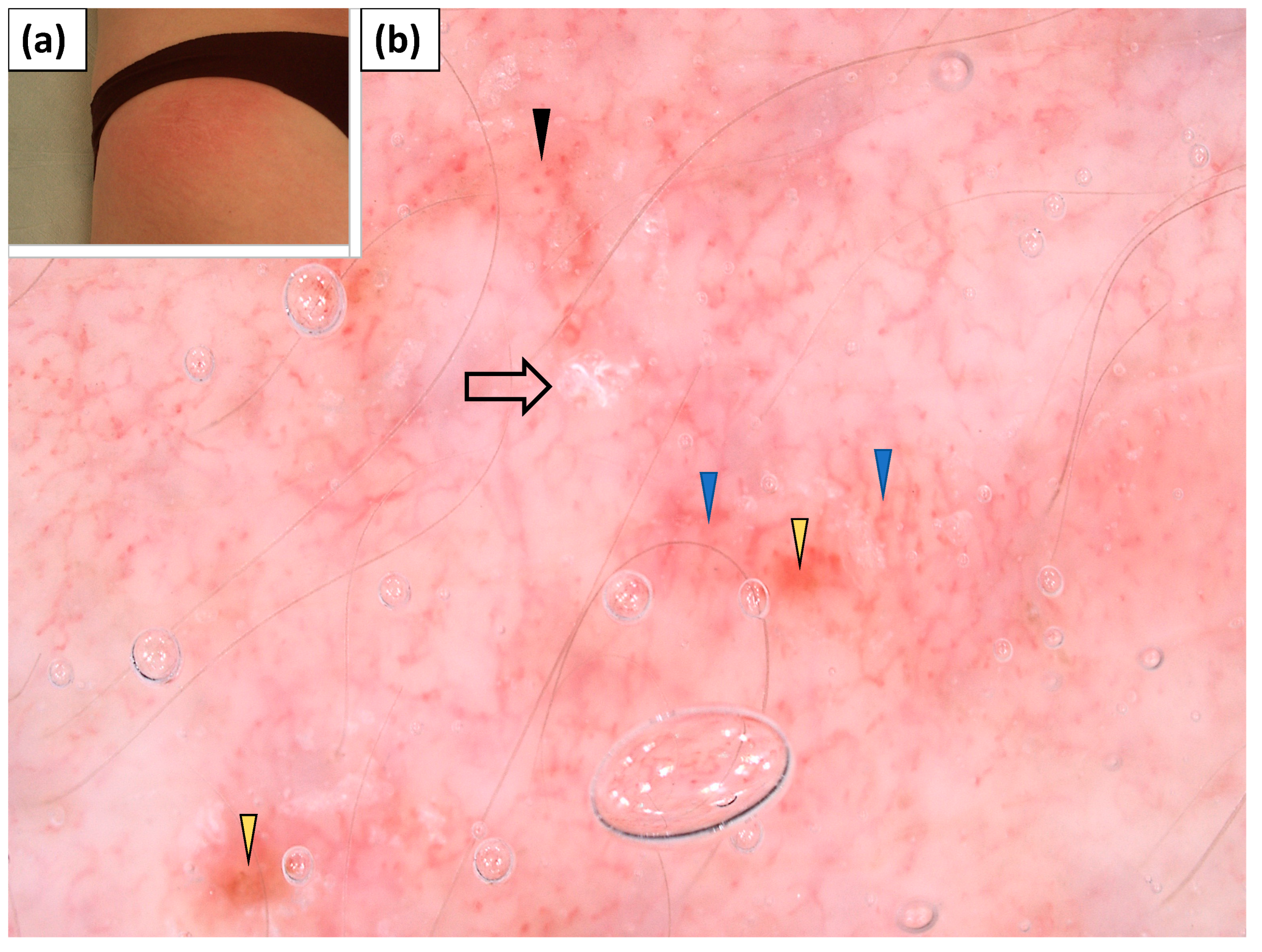
3.5. Dermoscopy of Other Cutaneous Lesions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sontheimer, R.D. Dermatomyositis: An overview of recent progress with emphasis on dermatologic aspects. Dermatol. Clin. 2002, 20, 387–408. [Google Scholar] [CrossRef]
- Mainetti, C.; Beretta-Piccoli, B.T.; Selmi, C. Cutaneous Manifestations of Dermatomyositis: A Comprehensive Review. Clin. Rev. Allergy Immunol. 2017, 53, 337–356. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, A.L.; Bressan, A.L.; Vasconcelos, B.N.; Gripp, A.C. Skin manifestations associated with systemic diseases—Part 1. An. Bras. Dermatol. 2021, 96, 655–671. [Google Scholar] [CrossRef] [PubMed]
- Reich, A.; Lis-Święty, A.; Krasowska, D.; Maj, J.; Wojas-Pelc, W.A.; Rudnicka, L. Dermatomyositis. Diagnostic and therapeutic recommendations of the Polish Dermatological Society. Dermatol. Rev. Przegl. Dermatol. 2021, 108, 85–104. [Google Scholar] [CrossRef]
- Żychowska, M.; Pięta, K.; Rudy, I.; Skubisz, A.; Reich, A. Dermoscopic Features of Lichen Amyloidosis in Caucasians—A Case Series and Literature Review. Medicina 2021, 57, 1027. [Google Scholar] [CrossRef] [PubMed]
- Zychowska, M.; Zychowska, M. Dermoscopy of discoid lupus erythematosus—A systematic review of the literature. Int. J. Dermatol. 2021, 60, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Sontheimer, R.D. A portable digital microphotography unit for rapid documentation of periungual nailfold capillary changes in autoimmune connective tissue diseases. J. Rheumatol. 2004, 31, 539–544. [Google Scholar] [PubMed]
- Hasegawa, M. Dermoscopy findings of nail fold capillaries in connective tissue diseases. J. Dermatol. 2011, 38, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuka, T. Dermoscopic detection of nail fold capillary abnormality in patients with systemic sclerosis. J. Dermatol. 2012, 39, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Chanprapaph, K.; Fakprapai, W.; Limtong, P.; Suchonwanit, P. Nailfold capillaroscopy with USB digital microscopy in connective tissue disease: A comparative study of 245 patients and healthy controls. Front Med. 2021, 8, 683900. [Google Scholar] [CrossRef] [PubMed]
- Jasso-Olivares, J.C.; Tosti, A.; Miteva, M.; Domínguez-Cherit, J.; Díaz-González, J.M. Clinical and Dermoscopic Features of the Scalp in 31 Patients with Dermatomyositis. Ski. Appendage Disord. 2017, 3, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Golińska, J.; Sar-Pomian, M.; Sławińska, M.; Sobjanek, M.; Sokołowska-Wojdyło, M.; Rudnicka, L. Trichoscopy may enhance the differential diagnosis of erythroderma. Clin. Exp. Dermatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Gonzalez, J.M.; Vega-Memije, M.E.; Mosqueda-Taylor, A.; García-Edgar, V.N.; Cuevas-Gonzalez, J.C. Dermoscopic patterns of filiform papillae of the tongue in patients with and without connective tissue autoimmune diseases. Int. J. Dermatol. 2018, 57, 938–942. [Google Scholar] [CrossRef] [PubMed]
- Namiki, T.; Hashimoto, T.; Hanafusa, T.; Miura, K.; Yokozeki, H. Case of dermatomyositis with Gottron papules and mechanic’s hand: Dermoscopic features. J. Dermatol. 2018, 45, e19–e20. [Google Scholar] [CrossRef] [PubMed]
- Sławińska, M.; Sokołowska-Wojdyło, M.; Sobjanek, M.; Golińska, J.; Nowicki, R.; Rudnicka, L. The significance of dermoscopy and trichoscopy in differentiation of erythroderma due to various dermatological disorders. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Errichetti, E.; Zalaudek, I.; Kittler, H.; Apalla, Z.; Argenziano, G.; Bakos, R.; Blum, A.; Braun, R.P.; Ioannides, D.; Lacarrubba, F.; et al. Standardization of dermoscopic terminology and basic dermoscopy parameters to evaluate in general dermatology (non-neoplastic dermatoses): An expert consensus on behalf of the International Dermoscopy Society. Br. J. Dermatol. 2020, 182, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Chanprapaph, K.; Limtong, P.; Ngamjanyaporn, P.; Suchonwanit, P. Trichoscopic Signs in Dermatomyositis, Systemic Lupus Erythematosus, and Systemic Sclerosis: A Comparative Study of 150 Patients. Dermatology 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chojer, P.; Mahajan, B.B. Nail fold dermoscopy in collagen vascular disorders: A cross-sectional study. Indian J. Dermatol. Venereol. Leprol. 2019, 85, 439. [Google Scholar] [CrossRef] [PubMed]
- Apalla, Z.; Papadimitriou, I.; Iordanidis, D.; Errichetti, E.; Kyrgidis, A.; Rakowska, A.; Sotiruou, E.; Vakirlis, E.; Bakirtzi, A.; Liopyris, K.; et al. The dermoscopic spectrum of cuta-neous lupus erythematosus: A retrospective analysis by clinical subtype with clinicopathological correlation. Dermatol. Ther. 2020, 33, e14514. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | |
|---|---|
| Gender, n (%) | |
| Male | 5 (33.3) |
| female | 10 (66.7) |
| Age, years | |
| Mean ± SD | 48.7 ± 19.4 |
| range | 18–87 |
| Time since first symptoms, months | |
| Mean ± SD | 17.3 ± 26.0 |
| range | 1–96 |
| Time since diagnosis, years | |
| Mean ± SD | 1.13 ± 2.3 |
| range | 0–8 |
| Muscle involvement, n (%) | 9 (60.0) |
| Hair loss, n (%) | 8 (53.3) |
| Associated malignancy, n (%) | 1 (6.7) |
| Nailfold Capillaroscopic Findings | P1 | P2 | P3 | P4 | P5 | P6 | P7 | P8 | P9 | P10 | P11 | P12 | P13 | P14 | P15 | Total (% of Cases with Abnormal Capillaroscopy/% of All Cases)) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tortuous vessels | - | - | + | + | + | + | - | - | - | - | + | + | + | + | - | 8 (72.7/53.3) |
| “bushy” capillaries | - | - | - | + | + | - | - | - | - | - | + | - | + | + | - | 5 (45.5/33.3) |
| Elongated capillaries | - | - | + | + | + | + | - | + | - | - | + | + | + | + | + | 10 (90.9/66.7) |
| Dilated capillaries | - | - | + | + | + | + | - | - | - | - | + | + | + | + | - | 8 (72.7/53.3) |
| Giant capillaries | - | - | - | - | + | - | - | - | - | - | + | - | + | + | - | 4 (36.4/26.7) |
| Subpapillary plexus | - | - | - | + | + | + | - | - | - | - | + | + | + | + | + | 8 (72.7/53.3) |
| Hemorrhages | + | - | - | + | + | + | - | + | - | - | + | - | + | - | + | 8 (72.7/53.3) |
| Disorganized vessel architecture | - | - | + | + | + | + | - | - | - | - | + | + | + | + | + | 9 (81.8/60.0) |
| Avascular areas | - | - | + | + | + | + | - | - | - | - | + | + | + | + | + | 9 (81.8/60.0) |
| Trichoscopic Features | P1 | P2 | P3 | P4 | P5 | P6 | P7 | P8 | P9 | P10 | P11 | P12 | P13 | P14 | P15 | Total (% of All Cases) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Follicular openings | ||||||||||||||||
| Absence of openings | - | - | - | + | + | + | + | - | + | - | - | - | - | - | - | 5 (33.3) |
| White dots | - | - | - | - | - | - | + | - | - | - | - | - | - | - | - | 1 (6.7) |
| Yellow dots | - | + | + | + | + | + | - | + | - | + | + | + | - | - | - | 9 (60.0) |
| Red follicular dots | - | - | - | - | + | - | - | - | - | - | - | - | - | - | - | 1 (6.7) |
| Dilated follicles | - | + | - | - | + | - | - | + | - | - | + | - | - | - | - | 4 (26.7) |
| Hair shafts | ||||||||||||||||
| Hair diameter diversity | - | + | - | + | + | + | - | + | + | + | + | + | - | - | - | 9 (60.0) |
| Pili torti | - | - | - | - | + | - | - | - | - | - | - | - | - | - | - | 1 (6.7) |
| Perifollicular surface | ||||||||||||||||
| Scaling | - | + | - | - | - | - | + | - | - | - | - | - | + | - | - | 3 (20.0) |
| Erythema | - | - | + | - | + | - | + | - | + | - | + | - | - | - | - | 5 (33.3) |
| Pigmentation | - | - | + | - | - | + | + | - | + | - | + | + | - | - | - | 6 (40.0) |
| White halo | - | - | - | - | - | + | - | - | - | - | - | - | - | - | - | 1 (6.7) |
| Interfollicular surface | ||||||||||||||||
| White structureless areas | - | - | - | - | + | + | + | - | - | - | - | - | - | - | - | 3 (20.0) |
| Pink structureless areas | - | - | - | + | - | + | - | - | - | - | - | - | - | - | - | 2 (13.3) |
| White scales | - | - | - | - | + | - | - | - | - | - | - | - | + | - | + | 3 (20.0) |
| Yellow scales | - | + | - | - | + | - | - | - | - | - | - | - | + | - | - | 3 (20.0) |
| Honeycomb pigment pattern | - | - | - | - | - | + | + | + | + | - | + | + | - | - | - | 6 (40.0) |
| Hemorrhages | - | + | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 (6.7) |
| Erosions | - | + | - | - | - | - | - | - | - | - | - | - | - | - | - | 1 (6.7) |
| Vessel morphology | ||||||||||||||||
| Dotted | - | - | - | + | - | + | - | - | - | - | + | + | - | - | - | 4 (26.7) |
| Linear | - | + | - | + | + | + | - | + | - | - | + | + | + | - | + | 9 (60.0) |
| Thin linear branched | - | + | - | + | + | + | + | + | + | + | + | + | + | - | + | 12 (80.0) |
| Thick linear branched | - | + | - | + | + | - | - | + | - | - | + | - | - | - | + | 6 (40.0) |
| Linear curved | - | - | - | + | + | + | - | + | - | - | + | + | + | - | + | 8 (53.3) |
| Polymorphous | - | - | - | + | + | + | - | + | - | - | + | + | + | - | + | 8 (53.3) |
| Lake-like structures | - | - | - | - | + | - | - | - | - | - | - | + | - | - | - | 2 (13.3) |
| Dermoscopic Features | Gottron’s Papules n = 13 | Gottron’s Sign (Elbows) n = 12 | Gottron’s Sign (Knees) n = 5 | Heliotrope n = 3 | Face n = 7 | V-Neck Sign n = 2 | Holster Sign n = 1 | Forearms n = 4 |
|---|---|---|---|---|---|---|---|---|
| Morphology of vessels, n (%) | ||||||||
| Dotted | 12 (92.3) | 10 (83.3) | 5 (100.0) | 0 (0.0) | 0 (0.0) | 1 (50.0) | 1 (100.0) | 3 (75.0) |
| Linear | 7 (53.9) | 8 (66.7) | 3 (60.0) | 0 (0.0) | 5 (71.4) | 1 (50.0) | 0 (0.0) | 4 (100.0) |
| Linear with branches | 6 (46.2) | 5 (41.7) | 3 (60.0) | 3 (100.0) | 5 (71.4) | 2 (100.0) | 1 (100.0) | 1 (25.0) |
| Linear curved | 4 (30.8) | 3 (25.0) | 0 (0.0) | 0 (0.0) | 3 (42.9) | 2 (100.0) | 0 (0.0) | 2 (50.0) |
| Polymorphic | 10 (76.9) | 10 (83.3) | 4 (80.0) | 0 (0.0) | 5 (71.4) | 2 (100.0) | 1 (100.0) | 4 (100.0) |
| Distribution of vessels, n (%) | ||||||||
| Uniform | 0 (0.0) | 1 (8.3) | 1 (20.0) | 2 (66.7) | 2 (28.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Clustered | 0 (0.0) | 2 (16.7) | 0 (0.0) | 0 (0.0) | 1 (14.3) | 1 (50.0) | 0 (0.0) | 0 (0.0) |
| Peripheral | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Unspecific | 13 (100.0) | 9 (75.0) | 4 (80.0) | 1 (33.3) | 4 (57.1) | 2 (100.0) | 1 (100.0) | 4 (100.0) |
| Color of scales, n (%) | ||||||||
| White | 10 (76.9) | 10 (83.3) | 4 (80.0) | 1 (33.3) | 1 (14.3) | 2 (100.0) | 1 (100.0) | 3 (75.0) |
| Yellow | 1 (7.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 2 (50.0) |
| Distribution of scales, n (%) | ||||||||
| Diffuse | 1 (7.7) | 0 (0.0) | 1 (20.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Central | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Peripheral | 0 (0.0) | 2 (16.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Patchy | 9 (69.2) | 9 (8.3) | 3 (60.0) | 1 (33.3) | 1 (14.3) | 2 (100.0) | 1 (100.0) | 4 (100.0) |
| Follicular findings, n (%) | ||||||||
| Follicular plugs | 5 (38.5) | 1 (8.3) | 2 (40.0) | 0 (0.0) | 2 (28.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Follicular red dots | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (33.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Perifollicular pigmentation | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Morphologies/colors, n (%) | ||||||||
| White structureless areas | 6 (46.2) | 5 (41.7) | 2 (40.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 1 (25.0) |
| Pink structureless areas | 10 (76.9) | 4 (33.3) | 3 (60.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 2 (50.0) |
| Yellow structureless areas | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 1 (25.0) |
| Red dots/globules | 5 (38.5) | 2 (16.7) | 1 (20.0) | 0 (0.0) | 0 (0.0) | 1 (100.0) | 0 (0.0) | 1 (25.0) |
| Brown globules | 0 (0.0) | 0 (0.0) | 1 (20.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Yellow globules | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (100.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Grey dots | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (33.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (25.0) |
| Specific clues, n (%) | ||||||||
| Stellate brown structures | 1 (7.7) | 1 (8.3) | 0 (0.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Speckled brown pigmentation | 0 (0.0) | 3 (25.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Yellowish crust | 0 (0.0) | 0 (0.0) | 1 (20.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Erosion | 0 (0.0) | 0 (0.0) | 1 (20.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 3 (75.0) |
| “sticky fiber” sign | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (14.3) | 0 (0.0) | 0 (0.0) | 1 (25.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żychowska, M.; Reich, A. Dermoscopy and Trichoscopy in Dermatomyositis—A Cross-Sectional Study. J. Clin. Med. 2022, 11, 375. https://doi.org/10.3390/jcm11020375
Żychowska M, Reich A. Dermoscopy and Trichoscopy in Dermatomyositis—A Cross-Sectional Study. Journal of Clinical Medicine. 2022; 11(2):375. https://doi.org/10.3390/jcm11020375
Chicago/Turabian StyleŻychowska, Magdalena, and Adam Reich. 2022. "Dermoscopy and Trichoscopy in Dermatomyositis—A Cross-Sectional Study" Journal of Clinical Medicine 11, no. 2: 375. https://doi.org/10.3390/jcm11020375
APA StyleŻychowska, M., & Reich, A. (2022). Dermoscopy and Trichoscopy in Dermatomyositis—A Cross-Sectional Study. Journal of Clinical Medicine, 11(2), 375. https://doi.org/10.3390/jcm11020375