
Effect of Algorithmic Music Listening on Cardiac Autonomic Nervous System Activity: An Exploratory, Randomized Crossover Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
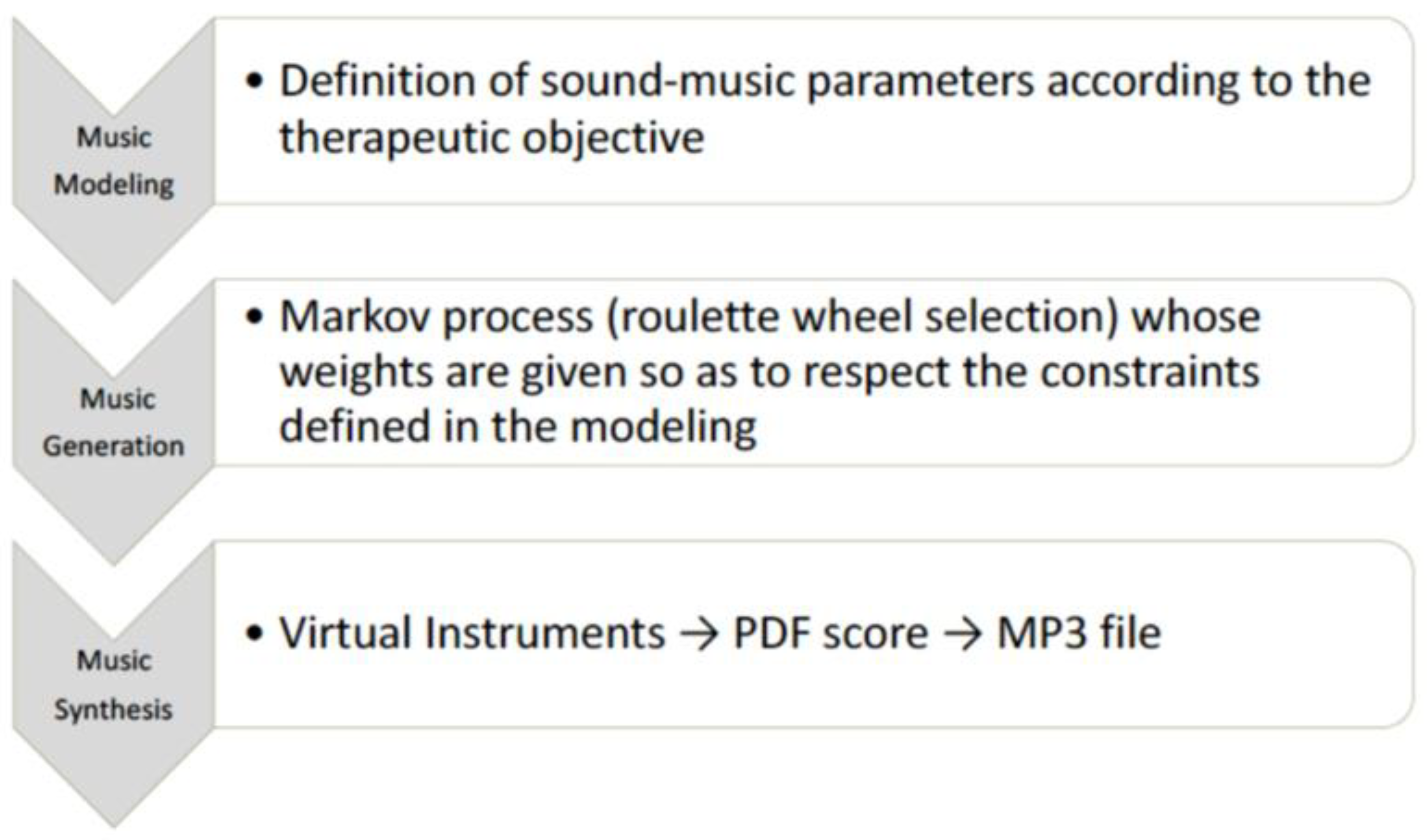
2.2. Music Intervention
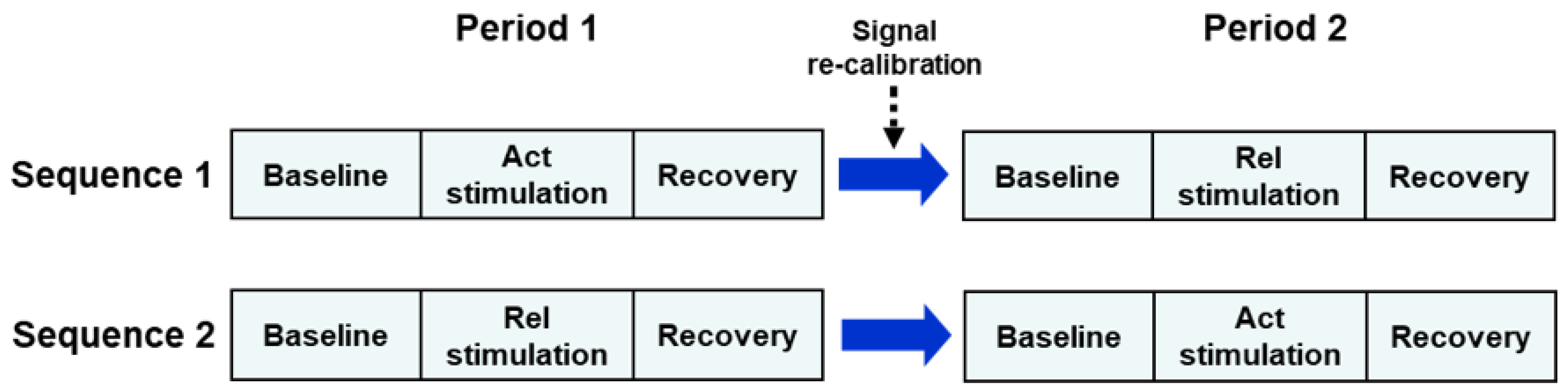
2.3. Experimental Protocol
2.4. Signal Analysis and Measurement of Autonomic Indices
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Interpretation of Changes in Cardiovascular Variability Indices
4.2. Study Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raglio, A.; Oasi, O. Music and health: What interventions for what results? Front. Psychol. 2015, 2, 230. [Google Scholar] [CrossRef] [PubMed]
- Boso, M.; Politi, P.; Barale, F.; Enzo, E. Neurophysiology and neurobiology of the musical experience. Funct. Neurol. 2006, 21, 187–191. [Google Scholar] [PubMed]
- Koelsch, S. A neuroscientific perspective on music therapy. Ann. N. Y. Acad. Sci. 2009, 1169, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Koelsch, S. Brain correlates of music-evoked emotions. Nat. Rev. Neurosci. 2014, 15, 170–180. [Google Scholar] [CrossRef]
- Chanda, M.L.; Levitin, D.J. The neurochemistry of music. Trends Cogn. Sci. 2013, 17, 179–193. [Google Scholar] [CrossRef]
- Raglio, A.; De Maria, B.; Perego, F.; Galizia, G.; Gallotta, M.; Imbriani, C.; Porta, A.; Vecchia, L.A.D. Effects of Algorithmic Music on the Cardiovascular Neural Control. J. Pers. Med. 2021, 11, 1084. [Google Scholar] [CrossRef]
- Orini, M.; Al-Amodi, F.; Koelsch, S.; Bailón, R. The Effect of Emotional Valence on Ventricular Repolarization Dynamics Is Mediated by Heart Rate Variability: A Study of QT Variability and Music-Induced Emotions. Front. Physiol. 2019, 10, 1465. [Google Scholar] [CrossRef]
- Koelsch, S.; Jäncke, L. Music and the heart. Eur. Heart J. 2015, 36, 3043–3049. [Google Scholar] [CrossRef]
- Loomba, R.S.; Arora, R.; Shah, P.H.; Chandrasekar, S.; Molnar, J. Effects of music on systolic blood pressure, diastolic blood pressure, and heart rate: A meta-analysis. Indian Heart J. 2012, 64, 309–313. [Google Scholar] [CrossRef]
- Raglio, A.; Oasi, O.; Gianotti, M.; Manzoni, V.; Bolis, S.; Ubezio, M.C.; Gentile, S.; Villani, D.; Stramba-Badiale, M. Effects of Music Therapy on Psychological Symptoms and Heart Rate Variability in Patients with Dementia. A Pilot Study. Curr. Aging Sci. 2010, 3, 242–246. [Google Scholar] [CrossRef]
- Okada, K.; Kurita, A.; Takase, B.; Otsuka, T.; Kodani, E.; Kusama, Y.; Atarashi, H.; Mizuno, K. Effects of music therapy on autonomic nervous system activity, incidence of heart failure events, and plasma cytokine and catecholamine levels in elderly patients with cerebrovascular disease and dementia. Int. Heart J. 2009, 50, 95–110. [Google Scholar] [CrossRef] [PubMed]
- Robb, S.L.; Burns, D.S.; Carpenter, J.S. Reporting guidelines for music-based interventions. J. Health Psychol. 2011, 16, 393. [Google Scholar] [CrossRef] [PubMed]
- Maestri, R.; Pinna, G.D. POLYAN: A computer program for polyparametric analysis of cardio-respiratory variability signals. Comput. Methods Programs Biomed. 1998, 56, 37–48. [Google Scholar] [CrossRef]
- Pinna, G.D.; Maestri, R.; Raczak, G.; La Rovere, M.T. Measuring baroreflex sensitivity from the gain function between arterial pressure and heart period. Clin. Sci. 2002, 103, 81–88. [Google Scholar] [CrossRef]
- La Rovere, M.T.; Pinna, G.D.; Maestri, R.; Mortara, A.; Capomolla, S.; Febo, O.; Ferrari, R.; Franchini, M.; Gnemmi, M.; Opasich, C.; et al. Short-term heart rate variability strongly predicts sudden cardiac death in chronic heart failure patients. Circulation 2003, 107, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Pinna, G.D.; Maestri, R.; Capomolla, S.; Febo, O.; Robbi, E.; Cobelli, F.; La Rovere, M.T. Applicability and clinical relevance of the transfer function method in the assessment of baroreflex sensitivity in heart failure patients. J. Am. Coll. Cardiol. 2005, 46, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Pinna, G.D.; Maestri, R.; Torunski, A.; Danilowicz-Szymanowicz, L.; Szwoch, M.; La Rovere, M.T.; Raczak, G. Heart rate variability measures: A fresh look at reliability. Clin. Sci. 2007, 113, 131–140. [Google Scholar] [CrossRef]
- La Rovere, M.T.; Maestri, R.; Robbi, E.; Caporotondi, A.; Guazzotti, G.; Febo, O.; Pinna, G.D. Comparison of the prognostic values of invasive and noninvasive assessments of baroreflex sensitivity in heart failure. J. Hypertens. 2011, 29, 1546–1552. [Google Scholar] [CrossRef]
- Raglio, A.; Vico, F. Music and technology: The curative algorithm. Front. Psychol. 2017, 8, 2055. [Google Scholar] [CrossRef]
- Zatorre, R.J. Why Do We Love Music? In Cerebrum: The Dana Forum on Brain Science; Dana Foundation: New York, NY, USA, 2018. [Google Scholar]
- Raglio, A.; Baiardi, P.; Vizzari, G.; Imbriani, M.; Castelli, M.; Manzoni, S.; Vico, F.; Manzoni, L. Algorithmic Music for Therapy: Effectiveness and Perspectives. Appl. Sci. 2021, 11, 8833. [Google Scholar] [CrossRef]
- Sihvonen, A.J.; Pitkäniemi, A.; Särkämö, T.; Soinila, S. Isn’t There Room for Music in Chronic Pain Management? J. Pain 2022, 23, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Requena, G.; Sánchez, C.; Corzo-Higueras, J.L.; Reyes-Alvarado, S.; Rivas-Ruiz, F.; Vico, F.; Raglio, A. Melomics music medicine (M3) to lessen pain perception during pediatric prick test procedure. Pediatr. Allergy Immunol. 2014, 25, 721–724. [Google Scholar] [CrossRef]
- Raglio, A.; Bellandi, D.; Gianotti, M.; Zanacchi, E.; Gnesi, M.; Monti, M.C.; Montomoli, C.; Vico, F.; Imbriani, C.; Giorgi, I.; et al. Daily music listening to reduce work-related stress: A randomized controlled pilot trial. J. Public Health 2020, 42, e81–e87. [Google Scholar] [CrossRef] [PubMed]
- Raglio, A.; Oddone, E.; Meaglia, I.; Monti, M.C.; Gnesi, M.; Gontero, G.; Imbriani, C.; Ivaldi, G.B. Conventional and Algorithmic Music Listening before Radiotherapy Treatment: A Randomized Controlled Pilot Study. Brain Sci. 2021, 11, 1618. [Google Scholar] [CrossRef] [PubMed]
- Pinna, G.D.; Maestri, R.; Di Cesare, A. Application of time series spectral analysis theory: Analysis of cardiovascular variability signals. Med. Biol. Eng. Comput. 1996, 34, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Task force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Rosenblueth, A.; Simeone, F. The interrelations of vagal and accelerator effects on the cardiac rate. Am. J. Physiol. 1934, 110, 42–55. [Google Scholar] [CrossRef]
- Bigger, J.T., Jr.; Fleiss, J.L.; Steinman, R.C.; Rolnitzky, L.M.; Kleiger, R.E.; Rottman, J.N. Correlations among time and frequency domain measures of heart period variability two weeks after acute myocardial infarction. Am. J. Cardiol. 1992, 69, 891–898. [Google Scholar] [CrossRef]
- Ramaekers, D.; Ector, H.; Aubert, A.E.; Rubens, A.; Van de Werf, F. Heart rate variability and heart rate in healthy volunteers. Is the female autonomic nervous system cardioprotective? Eur. Heart J. 1998, 19, 1334–1341. [Google Scholar] [CrossRef]
- Gouveia, S.; Scotto, M.G.; Pinna, G.D.; Maestri, R.; La Rovere, M.T.; Ferreira, P.J. Spontaneous baroreceptor reflex sensitivity for risk stratification of heart failure patients: Optimal cut-off and age effects. Clin. Sci. 2015, 129, 1163–1172. [Google Scholar] [CrossRef][Green Version]
- Pinna, G.D.; Porta, A.; Maestri, R.; De Maria, B.; Dalla Vecchia, L.A.; La Rovere, M.T. Different estimation methods of spontaneous baroreflex sensitivity have different predictive value in heart failure patients. J. Hypertens. 2017, 35, 1666–1675. [Google Scholar] [CrossRef] [PubMed]
- Van de Vooren, H.; Gademan, M.G.; Swenne, C.A.; Tenvoorde, B.J.; Schalij, M.J.; Van der Wall, E.E. Baroreflex Sensitivity, Blood Pressure Buffering and Resonance: What are the Links? Computer Simulation of Healthy Subjects and Heart Failure Patients. J. Appl. Physiol. 2007, 102, 1348–1356. [Google Scholar] [CrossRef] [PubMed]
- Pinna, G.D. Assessing baroreflex sensitivity by the transfer function method: What are we really measuring? J. Appl. Physiol. 2007, 102, 1310–1311. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, L.; Leuzzi, S.; Radaelli, A.; Passino, C.; Johnston, J.A.; Sleight, P. Low-frequency spontaneous fluctuations of R-R interval and blood pressure in conscious humans: A baroreceptor or central phenomenon? Clin. Sci. 1994, 87, 649–654. [Google Scholar] [CrossRef]
- Sleight, P.; La Rovere, M.T.; Mortara, A.; Pinna, G.; Maestri, R.; Leuzzi, S.; Bianchini, B.; Tavazzi, L.; Bernardi, L. Physiology and pathophysiology of heart rate and blood pressure variability in humans: Is power spectral analysis largely an index of baroreflex gain? Clin. Sci. 1995, 88, 103–109. [Google Scholar] [CrossRef]
- Cevese, A.; Gulli, G.; Polati, E.; Gottin, L.; Grasso, R. Baroreflex and oscillation of heart period at 0.1 Hz studied by alpha-blockade and cross-spectral analysis in healthy humans. J. Physiol. 2001, 531, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Bentho, O.; Park, M.Y.; Sharabi, Y. Low-frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp. Physiol. 2011, 96, 1255–1261. [Google Scholar] [CrossRef]
- Malliani, A.; Pagani, M.; Lombardi, F.; Cerutti, S. Cardiovascular neural regulation explored in the frequency domain. Circulation 1991, 84, 482–492. [Google Scholar] [CrossRef]
- Eckberg, D. Sympathovagal balance: A critical appraisal. Circulation 1997, 96, 3224–3232. [Google Scholar] [CrossRef]
- Goldberger, J.J. Sympathovagal balance: How should we measure it? Am. J. Physiol. 1999, 276, H1273–H1280. [Google Scholar] [CrossRef]
- Bootsma, M.; Swenne, C.A.; Janssen, M.J.; Cats, V.M.; Schalij, M.J. Heart rate variability and sympathovagal balance: Pharmacological validation. Neth. Heart J. 2003, 11, 250–259. [Google Scholar] [PubMed]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef]
- Reyes del Paso, G.A.; Langewitz, W.; Mulder, L.J.; van Roon, A.; Duschek, S. The utility of low frequency heart rate variability as an index of sympathetic cardiac tone: A review with emphasis on a reanalysis of previous studies. Psychophysiology 2013, 50, 477–487. [Google Scholar] [CrossRef]
- Hole, J.; Hirsch, M.; Ball, E.; Meads, C. Music as an aid for postoperative recovery in adults: A systematic review and meta-analysis. Lancet 2015, 386, 1630. [Google Scholar] [CrossRef]
- Opdahl, A.; Ambale Venkatesh, B.; Fernandes, V.R.S.; Wu, C.O.; Nasir, K.; Choi, E.Y.; Almeida, A.L.C.; Rosen, B.; Carvalho, B.; Edvardsen, T.; et al. Resting heart rate as predictor for left ventricular dysfunction and heart failure: MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 2014, 63, 1182–1189. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Rel Baseline | Rel Stimulation | Act Baseline | Act Stimulation |
|---|---|---|---|---|
| HR, bpm | 73.4 ± 2.2 | 72.2 ± 2.1 | 73.5 ± 2.1 | 73.3 ± 2.1 |
| SDNN, ms | 42.8 ± 2.6 | 40.9 ± 2.5 | 44.7 ± 3.2 | 40.3 ± 2.8 |
| RMSSD, ms | 30.8 ± 2.2 | 33.0 ± 2.3 | 35.0 ± 3.4 | 30.3 ± 2.7 |
| pNN50, % | 11.7 ± 2.6 | 14.1 ± 2.6 | 12.6 ± 2.7 | 11.1 ± 2.5 |
| LFpower, ms2 | 559 ± 87 | 644 ± 108 | 712 ± 144 | 512 ± 105 |
| LFNUr, N.U. | 51.7 ± 4.4 | 50.5 ± 4.2 | 53.9 ± 4.7 | 53.2 ± 4.1 |
| HFpower, ms2 | 443 ± 65 | 519 ± 59 | 479 ± 90 | 408 ± 62 |
| LF/HF, A.U. | 1.51 ± 0.26 | 1.37 ± 0.22 | 1.78 ± 0.34 | 1.51 ± 0.22 |
| BRS, ms/mm Hg | 6.0 ± 0.6 | 7.0 ± 0.7 | 6.3 ± 0.6 | 5.9 ± 0.5 |
| Variable | Rel Effect | Act Effect | p Carryover | p Period | p Treatment |
|---|---|---|---|---|---|
| HR, bpm | −1.2 ± 0.4 †† | −0.2 ± 0.3 | 0.63 | 0.36 | 0.018 |
| SDNN, ms | −1.9 ± 1.4 | −4.4 ± 1.9 † | 1.0 | 0.82 | 0.31 |
| RMSSD, ms | 2.2 ± 1.0 † | −4.7 ± 1.7 †† | 0.87 | 0.53 | 0.0002 |
| pNN50, % | 2.4 ± 1.1 † | −1.5 ± 0.8 | 0.95 | 0.61 | 0.010 |
| LFpower, ms2 | 85 ± 50 * | −201 ± 88 * | 0.72 | 0.47 | 0.015 |
| LFNU, N.U. | −1.2 ± 2.7 | −0.7 ± 2.6 | 0.97 | 0.88 | 0.89 |
| HFpower, ms2 | 76 ± 50 * | −72 ± 54 | 0.69 | 0.78 | 0.05 |
| LF/HF, A.U. | −0.14 ± 0.23 | −0.27 ± 0.21 | 0.40 | 0.85 | 0.72 |
| BRS, ms/mm Hg | 1.0 ± 0.4 † | −0.4 ± 0.4 | 0.73 | 0.48 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raglio, A.; Maestri, R.; Robbi, E.; Pierobon, A.; La Rovere, M.T.; Pinna, G.D. Effect of Algorithmic Music Listening on Cardiac Autonomic Nervous System Activity: An Exploratory, Randomized Crossover Study. J. Clin. Med. 2022, 11, 5738. https://doi.org/10.3390/jcm11195738
Raglio A, Maestri R, Robbi E, Pierobon A, La Rovere MT, Pinna GD. Effect of Algorithmic Music Listening on Cardiac Autonomic Nervous System Activity: An Exploratory, Randomized Crossover Study. Journal of Clinical Medicine. 2022; 11(19):5738. https://doi.org/10.3390/jcm11195738
Chicago/Turabian StyleRaglio, Alfredo, Roberto Maestri, Elena Robbi, Antonia Pierobon, Maria Teresa La Rovere, and Gian Domenico Pinna. 2022. "Effect of Algorithmic Music Listening on Cardiac Autonomic Nervous System Activity: An Exploratory, Randomized Crossover Study" Journal of Clinical Medicine 11, no. 19: 5738. https://doi.org/10.3390/jcm11195738
APA StyleRaglio, A., Maestri, R., Robbi, E., Pierobon, A., La Rovere, M. T., & Pinna, G. D. (2022). Effect of Algorithmic Music Listening on Cardiac Autonomic Nervous System Activity: An Exploratory, Randomized Crossover Study. Journal of Clinical Medicine, 11(19), 5738. https://doi.org/10.3390/jcm11195738