
Fighting Fatigue in Systemic Lupus Erythematosus: Experience of Dehydroepiandrosterone on Clinical Parameters and Patient-Reported Outcomes


Abstract
:1. Introduction
2. Methods
2.1. Data Source, Patients, and Study Design
2.2. Assessments
2.3. Laboratory Analyses
2.4. Statistics
2.5. Ethics Approvals
3. Results
3.1. Baseline Differences between Patient Groups
3.2. Disease Activity and Organ Damage
3.3. Background Medication
3.4. DHEA Exposure and Safety
3.5. Longitudinal Effects on PROMs among DHEA-Treated Patients
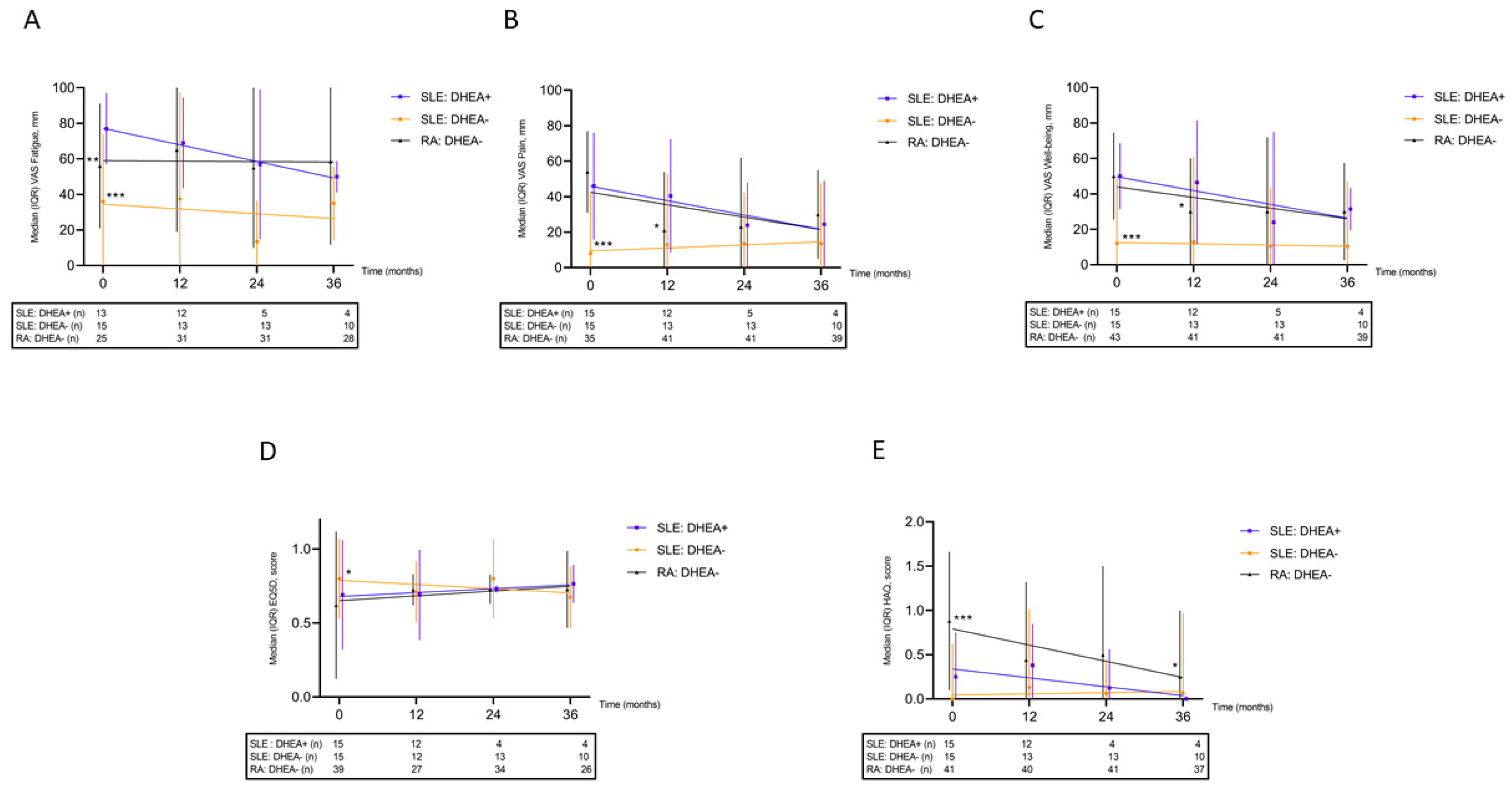
3.6. Effects on PROMs between the Patient Groups
3.7. Effects on Laboratory Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barber, M.R.W.; Drenkard, C.; Falasinnu, T.; Hoi, A.; Mak, A.; Kow, N.Y.; Svenungsson, E.; Peterson, J.; Clarke, A.E.; Ramsey-Goldman, R. Global epidemiology of systemic lupus erythematosus. Nat. Rev. Rheumatol. 2021, 17, 515–532. [Google Scholar] [CrossRef]
- Kaul, A.; Gordon, C.; Crow, M.K.; Touma, Z.; Urowitz, M.B.; van Vollenhoven, R.; Ruiz-Irastorza, G.; Hughes, G. Systemic lupus erythematosus. Nat. Rev. Dis. Primers 2016, 2, 16039. [Google Scholar] [CrossRef]
- Arnaud, L.; Gavand, P.E.; Voll, R.; Schwarting, A.; Maurier, F.; Blaison, G.; Magy-Bertrand, N.; Pennaforte, J.L.; Peter, H.H.; Kieffer, P.; et al. Predictors of fatigue and severe fatigue in a large international cohort of patients with systemic lupus erythematosus and a systematic review of the literature. Rheumatology 2019, 58, 987–996. [Google Scholar] [CrossRef]
- Baker, K.; Pope, J. Employment and work disability in systemic lupus erythematosus: A systematic review. Rheumatology 2009, 48, 281–284. [Google Scholar] [CrossRef]
- Jönsen, A.; Hjalte, F.; Willim, M.; Carlsson, K.S.; Sjöwall, C.; Svenungsson, E.; Leonard, D.; Bengtsson, C.; Rantapää-Dahlqvist, S.; Pettersson, S.; et al. Direct and indirect costs for systemic lupus erythematosus in Sweden. A nationwide health economic study based on five defined cohorts. Semin Arthritis Rheum. 2016, 45, 684–690. [Google Scholar] [CrossRef]
- Nguyen, M.H.; Huang, F.F.; O’Neill, S.G. Patient-Reported Outcomes for Quality of Life in SLE: Essential in Clinical Trials and Ready for Routine Care. J. Clin. Med. 2021, 10, 3754. [Google Scholar] [CrossRef]
- Dey, M.; Parodis, I.; Nikiphorou, E. Fatigue in Systemic Lupus Erythematosus and Rheumatoid Arthritis: A Comparison of Mechanisms, Measures and Management. J. Clin. Med. 2021, 10, 3566. [Google Scholar] [CrossRef]
- Tench, C.M.; McCurdie, I.; White, P.D.; D’Cruz, D.P. The prevalence and associations of fatigue in systemic lupus erythematosus. Rheumatology 2000, 39, 1249–1254. [Google Scholar] [CrossRef]
- Da Costa, D.; Dritsa, M.; Bernatsky, S.; Pineau, C.; Ménard, H.A.; Dasgupta, K.; Keschani, A.; Rippen, N.; Clarke, A.E. Dimensions of fatigue in systemic lupus erythematosus: Relationship to disease status and behavioral and psychosocial factors. J. Rheumatol. 2006, 33, 1282–1288. [Google Scholar]
- Sawalha, A.H.; Kovats, S. Dehydroepiandrosterone in systemic lupus erythematosus. Curr. Rheumatol. Rep. 2008, 10, 286–291. [Google Scholar] [CrossRef]
- Lucas, J.A.; Ahmed, S.A.; Casey, M.L.; MacDonald, P.C. Prevention of autoantibody formation and prolonged survival in New Zealand black/New Zealand white F1 mice fed dehydroisoandrosterone. J. Clin. Investig. 1985, 75, 2091–2093. [Google Scholar] [CrossRef] [Green Version]
- Norton, S.D.; Harrison, L.L.; Yowell, R.; Araneo, B.A. Administration of dehydroepiandrosterone sulfate retards onset but not progression of autoimmune disease in NZB/W mice. Autoimmunity 1997, 26, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Poynter, M.E.; Daynes, R.A. Peroxisome proliferator-activated receptor alpha activation modulates cellular redox status, represses nuclear factor-kappaB signaling, and reduces inflammatory cytokine production in aging. J. Biol. Chem. 1998, 273, 32833–32841. [Google Scholar] [CrossRef] [PubMed]
- Lahita, R.G.; Bradlow, H.L.; Ginzler, E.; Pang, S.; New, M. Low plasma androgens in women with systemic lupus erythematosus. Arthritis Rheum. 1987, 30, 241–248. [Google Scholar] [CrossRef]
- Hedman, M.; Nilsson, E.; de la Torre, B. Low sulpho-conjugated steroid hormone levels in systemic lupus erythematosus (SLE). Clin. Exp. Rheumatol. 1989, 7, 583–588. [Google Scholar] [PubMed]
- van Vollenhoven, R.F.; Engleman, E.G.; McGuire, J.L. Dehydroepiandrosterone in systemic lupus erythematosus. Results of a double-blind, placebo-controlled, randomized clinical trial. Arthritis Rheum. 1995, 38, 1826–1831. [Google Scholar] [CrossRef]
- van Vollenhoven, R.F.; Park, J.L.; Genovese, M.C.; West, J.P.; McGuire, J.L. A double-blind, placebo-controlled, clinical trial of dehydroepiandrosterone in severe systemic lupus erythematosus. Lupus 1999, 8, 181–187. [Google Scholar] [CrossRef]
- Chang, D.M.; Lan, J.L.; Lin, H.Y.; Luo, S.F. Dehydroepiandrosterone treatment of women with mild-to-moderate systemic lupus erythematosus: A multicenter randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2002, 46, 2924–2927. [Google Scholar] [CrossRef]
- Petri, M.A.; Mease, P.J.; Merrill, J.T.; Lahita, R.G.; Iannini, M.J.; Yocum, D.E.; Ginzler, E.M.; Katz, R.S.; Gluck, O.S.; Genovese, M.C.; et al. Effects of prasterone on disease activity and symptoms in women with active systemic lupus erythematosus. Arthritis Rheum. 2004, 50, 2858–2868. [Google Scholar] [CrossRef]
- Ziegelasch, M.; Boman, A.; Martinsson, K.; Thyberg, I.; Jacobs, C.; Nyhäll-Wåhlin, B.M.; Svärd, A.; Berglin, E.; Rantapää-Dahlqvist, S.; Skogh, T.; et al. Anti-cyclic citrullinated peptide antibodies are associated with radiographic damage but not disease activity in early rheumatoid arthritis diagnosed in 2006–2011. Scand. J. Rheumatol. 2020, 49, 434–442. [Google Scholar] [CrossRef]
- Ziegelasch, M.; van Delft, M.A.; Wallin, P.; Skogh, T.; Magro-Checa, C.; Steup-Beekman, G.M.; Trouw, L.A.; Kastbom, A.; Sjöwall, C. Antibodies against carbamylated proteins and cyclic citrullinated peptides in systemic lupus erythematosus: Results from two well-defined European cohorts. Arthritis Res. Ther. 2016, 18, 289. [Google Scholar] [CrossRef] [Green Version]
- Tan, E.M.; Cohen, A.S.; Fries, J.F.; Masi, A.T.; McShane, D.J.; Rothfield, N.F.; Schaller, J.G.; Talal, N.; Winchester, R.J. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982, 25, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Ighe, A.; Dahlström, Ö.; Skogh, T.; Sjöwall, C. Application of the 2012 Systemic Lupus International Collaborating Clinics classification criteria to patients in a regional Swedish systemic lupus erythematosus register. Arthritis Res. Ther. 2015, 17, 3. [Google Scholar] [CrossRef] [PubMed]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Ekdahl, C.; Eberhardt, K.; Andersson, S.I.; Svensson, B. Assessing disability in patients with rheumatoid arthritis. Use of a Swedish version of the Stanford Health Assessment Questionnaire. Scand. J. Rheumatol. 1988, 17, 263–271. [Google Scholar] [CrossRef]
- Dolan, P. Modeling valuations for EuroQol health states. Med. Care 1997, 35, 1095–1108. [Google Scholar] [CrossRef]
- Heijke, R.; Björk, M.; Thyberg, I.; Kastbom, A.; McDonald, L.; Sjöwall, C. Comparing longitudinal patient-reported outcome measures between Swedish patients with recent-onset systemic lupus erythematosus and early rheumatoid arthritis. Clin. Rheumatol. 2022, 41, 1561–1568. [Google Scholar] [CrossRef]
- Griffiths, B.; Mosca, M.; Gordon, C. Assessment of patients with systemic lupus erythematosus and the use of lupus disease activity indices. Best. Pract. Res. Clin. Rheumatol. 2005, 19, 685–708. [Google Scholar] [CrossRef]
- Gladman, D.; Ginzler, E.; Goldsmith, C.; Fortin, P.; Liang, M.; Urowitz, M.; Bacon, P.; Bombardieri, S.; Hanly, J.; Hay, E.; et al. The development and initial validation of the Systemic Lupus International Collaborating Clinics/American College of Rheumatology damage index for systemic lupus erythematosus. Arthritis Rheum. 1996, 39, 363–369. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Nordmark, G.; Bengtsson, C.; Larsson, A.; Karlsson, F.A.; Sturfelt, G.; Rönnblom, L. Effects of dehydroepiandrosterone supplement on health-related quality of life in glucocorticoid treated female patients with systemic lupus erythematosus. Autoimmunity 2005, 38, 531–540. [Google Scholar] [CrossRef]
- Björk, M.; Dahlström, Ö.; Wetterö, J.; Sjöwall, C. Quality of life and acquired organ damage are intimately related to activity limitations in patients with systemic lupus erythematosus. BMC Musculoskelet. Disord. 2015, 16, 188. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Background Characteristics | Median Value (Range) [IQR] or % | ||
|---|---|---|---|
| SLE: DHEA+ (n = 15) | SLE: DHEA− (n = 15) | RA: DHEA− (n = 45) | |
| Females, n (%) | 14 (93.3) | 14 (93.3) | 42 (93.3) |
| Caucasian ethnicity, n (%) | 14 (93.3) | 14 (93.3) | N/A |
| Age at disease onset (years) | 42 (12–76) [20] | 43 (15–55) [21] | 49 (20–76) [19] |
| Age at baseline (years) | 51 (24–76) [19.5] | 46 (21–71) [13.5] | 50 (21–76) [19] |
| Disease duration at baseline (years) | 9 (0–31) [17] | 4 (0–19) [8.5] | 1 (0–5) [1] |
| SLEDAI-2K (score) | 0 (0–4) [1] | 2 (0–15) [4] | N/A |
| Physician’s global assessment (0–4) | 0 (0–1) [0] | 0 (0–2) [0] | N/A |
| BMI at baseline (kg/m2) | 27.6 (19.2–40.4) [5.2] | 24.5 (19.9–35.8) [6] | N/A |
| SDI at baseline (score) | 0 (0–2) [1] | 0 (0–4) [1] | N/A |
| ACR criteria fulfilled, n | 5 (3–7) | 4 (3–7) | N/A |
| 1982 ACR criteria, n (%) | |||
| Malar rash | 7 (46.7) | 8 (53.3) | N/A |
| Discoid rash | 12 (80) | 7 (46.7) | N/A |
| Photosensitivity | 1 (6.7) | 1 (6.7) | N/A |
| Oral ulcers | 3 (20) | 0 (0) | N/A |
| Arthritis | 11 (73.3) | 13 (86.7) | N/A |
| Serositis | 4 (26.7) | 5 (33.3) | N/A |
| Renal disorder | 6 (40) | 6 (40) | N/A |
| Neurological disorder | 1 (6.7) | 1 (6.7) | N/A |
| Hematological disorder | 9 (60) | 6 (40) | N/A |
| Immunological disorder | 7 (46.7) | 8 (53.3) | N/A |
| Anti-nuclear antibody | 15 (100) | 15 (100) | N/A |
| Sex | Age at Start (years) | DHEA Exposure (months) | DHEA Concentration, Baseline (μmol/L) | DHEA Concentration, Percent of Lower Reference Limit (%) | Initial Daily DHEA Dose (mg) | Concomitant DMARDs | Steroid Dose at DHEA Initiation (mg) | Change in Steroid Dose at Last Follow Up (mg) | Cause of Cessation |
|---|---|---|---|---|---|---|---|---|---|
| F | 57 | 8 | 0.38 | 75 | 50 | HCQ | 0 | 0 | Treatment ongoing |
| F | 47 | 4 | N/A | N/A | 50 | MMF | 7.5 | 0 | Without specification * |
| F | 54 | 4 | 0.55 | 57 | 200 | HCQ | 0 | 0 | Lack of efficacy * |
| F | 50 | 6 | 0.38 | 40 | 50 | HCQ | 2.5 | 0 | Lack of efficacy |
| M | 43 | 81 | N/A | N/A | 50 | HCQ, MTX | 5 | +2.5 | Treatment ongoing |
| F | 56 | 3 | N/A | N/A | 50 | None | 7.5 | −2.5 | Acne, scaly hair * |
| F | 31 | 12 | 0.54 | 20 | 25 | HCQ, AZA | 2.5 | 0 | Lack of efficacy |
| F | 37 | 14 | 2.2 | 140 | 25 | HCQ | 0 | 0 | Without specification |
| F | 27 | 30 | 2.7 | 100 | 25 | HCQ, MMF | 2.5 | 0 | Treatment ongoing |
| F | 61 | 9 | 0.22 | 43 | 50 | AZA | 5 | 0 | Lack of efficacy |
| F | 47 | 69 | 0.35 | 36 | 25 | HCQ | 0 | 0 | Acne, fear of thrombosis |
| F | 58 | 17 | 0.44 | 86 | 50 | HCQ, MMF | 5 | −5 | Treatment ongoing |
| F | 76 | 36 | 0.14 | 42 | 200 | HCQ | 5 | +2.5 | Treatment ongoing |
| F | 23 | 16 | 2.7 | 68 | 50 | HCQ | 5 | −5 | Treatment ongoing |
| F | 50 | 10 | 0.43 | 45 | 25 | HCQ | 5 | 0 | Lack of efficacy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skoglund, O.; Walhelm, T.; Thyberg, I.; Eriksson, P.; Sjöwall, C. Fighting Fatigue in Systemic Lupus Erythematosus: Experience of Dehydroepiandrosterone on Clinical Parameters and Patient-Reported Outcomes. J. Clin. Med. 2022, 11, 5300. https://doi.org/10.3390/jcm11185300
Skoglund O, Walhelm T, Thyberg I, Eriksson P, Sjöwall C. Fighting Fatigue in Systemic Lupus Erythematosus: Experience of Dehydroepiandrosterone on Clinical Parameters and Patient-Reported Outcomes. Journal of Clinical Medicine. 2022; 11(18):5300. https://doi.org/10.3390/jcm11185300
Chicago/Turabian StyleSkoglund, Oliver, Tomas Walhelm, Ingrid Thyberg, Per Eriksson, and Christopher Sjöwall. 2022. "Fighting Fatigue in Systemic Lupus Erythematosus: Experience of Dehydroepiandrosterone on Clinical Parameters and Patient-Reported Outcomes" Journal of Clinical Medicine 11, no. 18: 5300. https://doi.org/10.3390/jcm11185300
APA StyleSkoglund, O., Walhelm, T., Thyberg, I., Eriksson, P., & Sjöwall, C. (2022). Fighting Fatigue in Systemic Lupus Erythematosus: Experience of Dehydroepiandrosterone on Clinical Parameters and Patient-Reported Outcomes. Journal of Clinical Medicine, 11(18), 5300. https://doi.org/10.3390/jcm11185300